Embed Size (px)
Citation preview

1
CDPH Updates
November 7, 2018
Welcome
Robyn ThomasonCalifornia Hospital Association

2
Continuing Education
Continuing education will be offered for this program for compliance, health care executives, legal, nursing and risk managers.
Full attendance and completion of the online evaluation and attestation of attendance are required to receive CEs for this webinar. CEs are complimentary and available for the registrant only.
Faculty & Facilitator
Debby Rogers, RN, MS, FAEN is CHA’s vice president of clinical performance and transformation. Ms. Rogers provides leadership in developing policy on clinical performance issues related to quality and quality measurement, case management, licensing and certification, and electronic health records. She is a masters prepared registered nurse with expertise in the regulatory and legislative processes.

3
Program Overview
Faculty
Cari Lee, Pharm.D., has been a consultant with the California Department of Public Health (CDPH) for over 11 years and is currently the Chief Pharmaceutical Consultant for the Licensing and Certification Program of CDPH. She oversees the Pharmaceutical Consultant Unit and is responsible for program and policy matters related to the provision of pharmaceutical services in all licensed health care facilities. Prior to joining CDPH, Dr. Lee had worked as an ambulatory care clinical pharmacist for a northern California medical center.

4
Faculty
Lori Schaumleffel, RN, BSN, PHN, CIC, is currently the HAI Performance Coordinator for the California Department of Public Health (CDPH) in the Healthcare Associated Infection (HAI) Program. She has worked in Infection Prevention and Employee Health for 16 years, earned a bachelor’s degree in nursing, is a licensed registered and public health nurse, and is certified in infection prevention and control. In addition Ms. Schaumleffel has a background in Emergency Medicine and Adult Critical Care.
Medication Deficiencies
Cari Lee, Pharm.D., Pharmaceutical Consultant Unit Chief, California Department of Public Health

5
Updates on Hospital RelicensingSurveys & Review of Clinical Findings
Cari Lee, Pharm.D.Chief Pharmaceutical Consultant Center for Healthcare Quality
GACH Relicensing Survey 2017-2018
March 1, 2017 to February 28, 2018 106 GACH relicensing surveys were completed Total number of regulatory violations cited: 1248 64% of the violations constitute the top 10 findings

6
GACH Relicensing Survey 2017-2018 (cont.)
Regulation Grouping Count Percent Ranking
Pharmaceutical Service General Requirements 362 29% 1
Infection Control Program 116 9% 2
Nursing Service Policies and Procedures 79 6% 3
Planning and Implementing Patient Care 76 6% 4
Patients' Rights 43 3% 5
GACH Relicensing Survey 2017-2018 (cont.)
Regulation Grouping Count Percent Ranking
Nursing Service Staff 30 2% 6
Dietetic Service General Requirements 27 2% 7
General Safety and Maintenance 27 2% 8
Surgical Service General Requirements 23 2% 9
Basic Emergency Medical Service, Physician on Duty 17 1% 10

7
GACH Relicensing Survey 2017-2018 (cont.)Regulation Description Count
Total Count 1248Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(c)(1) 78Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(g)(2) 59Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(q)(9) 56Nursing Service Policies and Procedures. / T22 DIV5 CH1 ART3-70213(a) 54Infection Control Program / T22 DIV5 CH1 ART7-70739(a) 40Infection Control Program / T22 DIV5 CH1 ART7-70739(a)(1) 36Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(r) 29Planning and Implementing Patient Care / T22 DIV5 CH1 ART3-70215(b) 28Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(q)(6) 26Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(f)(2) 23
CCR Title 22 Section 70263(c)(1)Development and implementation of P&P for safe and effective
systems for procurement, storage, distribution, dispensing and use of drugs
Common findings: Fentanyl transdermal P&P not followed Second independent check for high alert meds not performed High alert medication storage and handling Ambiguous orders, orders not clarified SDV/ MDV ADC overrides/access

8
CCR Title 22 Section 70263(g)(2)
Medications and treatments shall be administered as ordered
Common findings: Medications not titrated as ordered (heparin drips, insulin
drips, norepinephrine) Pain medications not administered according to pain scale Omission, wrong dose
CCR Title 22 Section 70263(q)(9)
Expired, contaminated or deteriorated drugs available for patient use
Common findings: Light sensitive meds not protected from light Expired, improperly stored meds available Expired meds in crash carts

9
CCR Title 22 Section 70213(a)
Nursing P&P development and implementation
Common findings: PCA monitoring (RR, sedation, pain) Pain assessment Propofol titration (RASS) Medication administration techniques (slow IV push,
rotating injection sites) Monitoring (BG, aPTT/Anti-Xa) Physician notification
CCR Title 22 Section 70263(r) Quality control procedures for all repackaged and compounded drugs in the
hospital
Common findings: BUD assignment inconsistent with sterile compounding area design Certification report not reviewed and acted upon Differential pressure not monitored appropriately CSP used as stock solution Bedside admixing of medium risk CSPs HD compounding Staff competency

10
CCR Title 22 Section 70263(q)(6)
Medication storage at appropriate temperatures
Common findings: Refrigerator temperatures not monitored properly Freezer temperature settings not appropriate for
specific meds Remote temperature monitoring system and
responsibilities
CCR Title 22 Section 70263(f)(2)
Emergency medication properly sealed, content list
Common findings: Content not matching list Ampules without filter needles Other emergency meds deficiencies: MH training
and MH supplies access for ED staff

11
High Risk Medication Clinical Record Review
Heparin DripInsulin DripPCAFentanyl TransdermalNarcoticsPropofolOther High Risk Medications
Clinical Case #1
Patient AK was a 74 year old male admitted to the hospital for elective surgery with no history of prior narcotic use. PACU order: Fentanyl 25 mcg IV Push q 3 min prn PACU pain
(1st choice) Hydromorphone 0.5 mg IV push q 3 min prn PACU pain
(2nd choice if 1st choice not effective)

12
Clinical Case #1 (cont.)Patient AK’s MAR:
4:25pm Hydromorphone 0.5mg IV pushFentanyl 25mcg IV push
4:35pm Fentanyl 25mcg IV push4:37pm Fentanyl 25mcg IV push4:38pm Fentanyl 25mcg IV push4:40pm Fentanyl 25mcg IV push
Hydromorphone 0.5mg IV push4:55pm Fentanyl 25mcg IV push4:56pm Fentanyl 25mcg IV push
Clinical Case #1 (cont.)Including narcotics given in OR, Patient AK received a total of
225mcg of fentanyl and 5.5mg of hydromorphone over 71minutes
At 6:20pm AK was transferred to the floor. Vital signs: BP 144/64 HR 61 RR 19 O2 91%
At 6:50, AK was found unresponsive. Code blue was called.AK suffered diffused anoxic injury of the brain. Life support was
withdrawn 7 days later and the patient expired.

13
Clinical Case #1 (cont.)
What went wrong: Medication orders not carried out as prescribed 1st choice and 2nd choice given togetherMedications given more frequent than prescribed
Uncontrolled pain not reported to MD Drop in O2 saturation not noted Were the orders reasonable? How about access to meds? Was the preprinted order clear?
Clinical Case #1 (cont.)
Chart Review: Were medications administered as ordered (dose, frequency,
selection of drug)? Was the patient monitored appropriately? Documentation in accordance with P&P? MAR and wastage consistent with ADC dispensing record?

14
Clinical Case #2
Patient KC was admitted to the hospital through the ED for significant lower quadrant abdominal pain, N/V.
KC received:
12:45pm Hydromorphone 1mg IV3:45am Hydromorphone 1mg IV9:22am Hydromorphone 2mg IV
12:27pm Hydromorphone 2mg IV 12:54pm Hydromorphone 2mg IV
Clinical Case #2 (cont.)
New order for Hydromorphone 4mg IV q 2hr prn pain was written at 12:46pm
5:35pm Hydromorphone 4mg IV8:02pm Hydromorphone 4mg IV
10:07pm Hydromorphone 4mg IV
KC received a total of 20mg of hydromorphone in 24 hrsAt 2:56 am, KC was found unresponsive and was pronounced
dead at 3:15 am

15
Clinical Case #2 (cont.)
“I don’t know why that didn’t strike me [as a high dose] at that time.”
Hospital P&P required hourly rounds between 0600 to 2200 and every 2-hr rounds between midnight and 0600
No documentation of assessment of pain, sedation, RR and BP when hydromorphone was administered at 8:02pm and 10:07pm
Last assessment was performed between 11pm to 12am, 3.5 hours before the patient was found unresponsive
Clinical Case #2 (cont.)
How did it happen? Hydromorphone dose:Opioid naive: 0.2 to 1 mg every 2 to 3 hours as needed;
Critically ill patients (off-label dosing): 0.2 to 0.6 mg every 1 to 2 hours as needed or 0.5 mg every 3 hours as needed

16
Clinical Case #2 (cont.)
What a retrospective chart review would identify?
Were hydromorphone orders reasonable? Was the medication administered as ordered? Was monitoring performed effectively and in accordance
with P&P?
Clinical Case #3
Patient CT was admitted to hospital for DVT Heparin drip at 18 units/kg/hr was ordered with a goal aPTT of 62
to 100 secondsBaseline aPTT 30.2 secondsHeparin 1467units/hr was started at 7:00pmAt 3:21 am, critical aPTT of >200 seconds was reportedHeparin was held for 2 hours and then increased to 1850 units/hr
with a bolus dose of 3000 units

17
Clinical Case #3 (cont.)
At 1:16 pm, a critical aPTT of >200 was reported Heparin was again held for 2 hours and then increased to
2000 units/hr with a bolus dose of 1000 units At 2:45am, a critical aPTT of >200 was reported Heparin was held for 2 hours. A repeat aPTT at 6:30 am was
>200. Heparin was d/c’ed.
Clinical Case #3 (cont.) What happened? Why did staff keep increasing CT’s heparin infusion
rate and administered bolus doses when critical aPTT was reported?

18
Clinical Case #3 (cont.) Heparin drip protocol was confusing – when critical aPTT was
reported, protocol directed nursing staff to hold the drip for 2 hours and to repeat aPTT. When it was time to resume the drip, staff used the aPTT reported when heparin was on hold to make adjustments.
CT was fortunately not harmed but the potential for more than minimum harm existed with the extended period of over-anticoagulation. A non-IJ administrative penalty was issued.
Hospital was unaware of the incident. It was discovered during survey as part of random chart review.
Clinical Case #3 (cont.) What a retrospective chart review would identify?
Was the heparin protocol followed appropriately? Was aPTT monitored appropriately? Was MD notified when critical aPTT was reported? Was second independent check performed? Does the heparin protocol make sense? Was documentation easy to follow?

19
Clinical Case #4 MK was a 1.87kg preterm baby. Enoxaparin 1.1mg/kg SQ q12hr
was ordered for thrombus in descending aorta. Anti-Xa goal 0.5 to 0.7 u/ml. Calculated dose was 2mg.
Pediatric pharmacy miscalculated and prepared 3 doses of Enoxaparin 20mg/0.2ml (10X)
MK received 3 doses of enoxaparin at 10X the prescribed doseAnti-Xa was 1.92 after the 2nd dose but 3rd dose was already
administered
Clinical Case #4 (cont.)
MK received 2 doses of protamine to reverse the over-anticoagulation effect from the enoxaparin overdoseMAR showed 2nd independent check was carried out but
all six nurses involved missed the calculation errorP&P indicated each nurse should independently calculate
and verify the doseInterviews revealed that nurses did not verify the dose by
calculation independently

20
Clinical Case #5
Patient BG was prescribed Norco 5 one to two tablets every 4 hours as needed for moderate to severe pain (4/10, with 10 being the most severe pain). The physician order further indicated for the first administration to start with one tablet, assess response after 30 minutes and then give another tablet if needed. If patient receives both tablets then next administration, two tablets can be given.
BG received two (2) tablets of Norco 5 as his first dose for a pain score of "4”
Clinical Case #5 (cont.)
BG was found unresponsive 5 hours later. Rapid response team was called. BG received 2 doses of naloxone to reverse the opioid effect.
Hospital was unaware of the error even naloxone was administered. Error was discovered during survey as part of the random chart review.
An non-IJ administrative penalty was issued

21
Clinical Case #5 (cont.)
What a retrospective chart review would identify?
Was the range order appropriate? Pain scale of 4/10 for moderate to severe pain? Was the ADR reported and investigated?
Other Clinical Findings
Pump Programming errors (including PCA)Infusion pump malfunction (free flow)Wrong concentration errors (heparinized saline vs
premixed)Medication labeling error (Norepinephrine given
instead of oxytocin in L&D)Insulin drip on NPOPCA by proxy

22
How to prevent these from happening in your hospital?
Now that you have learned about others’ mistakes, it’s time to…
Be your own surveyorIdentify high risk medications and populations in your
organizationConduct periodic chart reviews to identify irregularitiesPeriodic audit of adherence to medication safety P&P
Medication Error Reduction Plan
California Health and Safety Code 1339.63 (e) (5):“Include a system or process to proactively identify actual or potential medication-related errors. The system or process shall include concurrent and retrospective review of clinical care.
Putting the pieces together, your organization will build a stronger Medication Error Reduction Plan to enhance medication safety.

23
CDPH Updates on Hospital Relicensing Survey Findings
Infection Prevention
Lori Schaumleffel, RN, BSN, PHN, CIC, Infection Prevention Liaison, California Department of Public Health

24
Preventing Health Care-Associated Infections:Do You Know if Your Health Care Providers are Doing
the Most Important Things Consistently?
WebinarCalifornia Hospital Association
November 7, 2018
CALIFORNIA DEPARTMENT OF PUBLIC HEALTH
Lori Schaumleffel, RN, BSN, PHN, CICHAI Performance Coordinator
Health Care-Associated Infections ProgramCenter for Health Care Quality
• Describe CDPH Health Care-Associated Infections (HAI) Program• Review evidence-based practices known to prevent HAI• Describe observed gaps in infection prevention practices• Review recommendations for monitoring adherence to core/basic infection
prevention care practices• Discuss how to establish a facility-wide adherence monitoring program• Review CDPH adherence monitoring tools
Objectives

25
CDPH Center for Health Care Quality Health Care-Associated Infections Program
• 2006 law required CDPH to create a program to oversee the prevention, surveillance, and reporting of HAI in California general acute care hospitals (Health & Safety Code 1288.8)
• HAI Program launched in December 2009
• 2008 law established hospital HAI reporting requirements (Health & Safety Code 1288.55)
• California requires more HAI data reporting than any other state
California HAI Public Reporting Laws• General acute care hospitals required to report 5 HAI types
• Central line associated bloodstream infections (CLABSI)• Methicillin-resistant S. aureus bloodstream infections (MRSA BSI)• Vancomycin-resistant Enterococcus bloodstream infections (VRE BSI)• C. difficile infections (CDI)• Surgical site infections (SSI) following 28 procedure types
• Data risk adjusted using National Healthcare Safety Network (NHSN) protocols, definitions, and reporting system
• CDPH must publish hospital HAI data annually
Health and Safety Code section 1288.55

26
• Content
• 18-page narrative report with 5 appendices (38 pages total)
• Detailed 2-page HAI summary profile for each hospital
• “My Hospital’s Infections” map with ability to perform side by side comparisons for 2-3 hospitals
• Infection-specific data tables published on California Health and Human Services Open Data Portal
HAI in California Hospitals Annual Report, 2017
• In 2015, HAI Advisory Committee recommended that CDPH adopt national HAI prevention goals for California hospitals
• 2020 CLABSI and MRSA BSI goal, SIR <0.50
• Considered on track in 2018 if SIR 0.70 or lower
• 2020 CDI and SSI goal, SIR <0.70
• Considered on track in 2018 if SIR 0.82 or lower
Tracking Progress to 2020 HAI Reduction Goals

27
HAI Prevention – What really works? • Evidence-based practice recommendations are based on science
• If studied systematically, does a practice result in reduced infection rates?
• Best sources for evidence-based HAI prevention practice recommendations • Centers for Disease Control and Prevention (CDC)• Healthcare Infection Control Practices Advisory Committee (HICPAC)• Infectious Diseases Society of America (IDSA) / Society for Healthcare
Epidemiology of America (SHEA)
53
54
• Standard precautions• Hand hygiene• Environmental cleaning and
disinfection• Injection safety, medication safety• Assess risk, use PPE appropriately• Minimize potential exposures• Clean and reprocess reusable
medical equipment • Transmission-based precautions as
necessary
• Visible, tangible leadership support for infection control
• Infection prevention trainingfor all HCP
• Patient, family, caregiver HAI prevention education
• Performance monitoringand feedback
• Early, prompt removal of invasive devices
• Occupational health
Core Infection Prevention Practices
For Use in All Health Care Settings at All Times

28
Are Core Infection Prevention Care Practices Performed Routinely?
Sample Findings from CDPH HAI Program Liaison IP Observations
55
HEALTH CARE-ASSOCIATED INFECTIONS PROGRAM
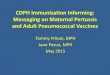
Hand Hygiene Adherence Monitoring
61%0
500
1000
1500
2000
2500
Hand Hygiene Rate - Includes All Opportunities
158 Acute Care Facilities, 2015-2018 (N=2195)
Successful Missed Missed
56
# O
bser
vatio
ns

29
57
• Test only symptomatic patients
• Do not repeat testing within 7 days of same diarrhea episode
• Do not test for cure
• Initiate institutional criteria for optimal CDI testing
-OR-• Perform toxin-test as
part of multi-step algorithm
Reducing CDI Rate/SIR: The Most Important Things
Improve CDI Surveillance – Improve Diagnosis/Treatment
Preventing CDI: The MOST Important Things
58
• Isolate patients with diarrhea pending CDI confirmation
• Lab alert system for immediate notification of positive CDI tests
• Contact precautions for duration of diarrhea plus 48 hours• Private room, dedicated toilet• Gloves/gown to enter room• Remove gloves, perform hand
hygiene prior to room exit• Hand hygiene before/after patient
contact & after glove removal• Patient hand hygiene
• Disposable equipment • Sporicidal disinfectant for cleaning reusable
equipment• Sporicidal disinfectant for terminal cleaning• Quality cleaning, daily & terminal• CDI-targeted antimicrobial stewardship
program• Improve overall prescribing, stop
unnecessary antibiotics• Restrict high-risk antibiotics based on
local epidemiology• Stop inciting antibiotic
Prevent C. difficile Acquisition / Reduce Antimicrobial Exposure

30
Are CDI Prevention Care Practices Performed Routinely?
59
HEALTH CARE-ASSOCIATED INFECTIONS PROGRAM
Contact Precautions Adherence Monitoring
99% 97% 99% 51%0
100
200
300
400
500
PPE available atContact
Precautions RoomEntry
ContactPrecautions SignClear and Visible
Patient in SingleRoom OR Cohorted
Correctly
Hand HygieneBefore Entering
ContactPrecautions Room
158 Acute Care Facilities, 2015-2018
Successful Missed
60
# Ob
serv
atio
ns

31
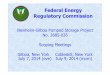
HEALTH CARE-ASSOCIATED INFECTIONS PROGRAM
Environmental Cleaning Adherence Monitoring
96% 66% 91% 91% 63%0
100
200
300
Solution mixed tomanufacturerinstructions
Contact time -manufacturerinstructions
New cleansaturated cloth
used in each room
Proper PPE High touch objectscleaned daily-
w/EPA disinfectant
158 Acute Care Facilities, 2015-2018
Successful Missed
61
# Ob
serv
atio
ns
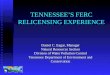
HEALTH CARE-ASSOCIATED INFECTIONS PROGRAM
Antibiotic Stewardship Adherence Monitoring
55% 45% 69% 88% 60% 44%0
20
40
60
80
100
120
140
Indication for useon antibiotic
orders
Antibioticreviewed at 48
hours forappropriateness
Antibioticreviewed with
new/recurrent CDIdiagnosis
Antibiotic usemonitored at unit-
or hospital-level
ASP interventionstarget CDI
ASP tracks CDI asan outcome
158 Acute Care Facilities, 2015-2018
Successful Missed
62
# Ob
serv
atio
ns

32
Preventing CLABSI: The MOST Important Things63
• Provide list of indications for central line
• Education of HCP inserting or caring for central line
• Bathe ICU patients with CHG daily• Adhere to infection prevention
practices at insertion (CLIP)• Use all-inclusive catheter cart/kit• Use Ultrasound guidance for insertion• Use alcoholic CHG skin prep• Ensure appropriate nurse patient ratio
• Disinfect hub before accessing central line
• Remove nonessential catheters• Change transparent dressings and site
care with CHG every 5-7 days or if soiled
• Replace administration sets not used for blood product or lipids no longer than every 4 days (96 hours)
• Use antimicrobial ointment for hemodialysis catheter insertion sites
• Perform CLABSI surveillance
Prevent Early- and Late-Onset CLABSI
Are CLABSI Prevention Care Practices Performed Routinely?
64

33
HEALTH CARE-ASSOCIATED INFECTIONS PROGRAM
63% 75% 84% 81% 29%0
10
20
30
40
50
Review Line NeedDaily with Primary
Provider
MaintenanceBundle
Investiages CLABSICause Factors
Protector Caps onPorts
Uses AntimicrobialCatheters
46 Acute Care Facilities, 2016-2018
Successful Missed
CLABSI Practices Adherence Monitoring
65
# Ob
serv
atio
ns
CLABSI Practice Observations
66
39 Hospitals with High CLABSI Rates, 2016-2017 # Observations Adherence Line Insertion 12 90% Line Maintenance 39 Insertion Date Documented 83% Hand Hygiene Before/After Even if Gloves Worn 78% Clean, Dry, Intact Dressing 92% Avoid Femoral Site 95% CHG Sponge at Insertion Site 95% Daily CHG Bath if Hospital Policy 63%

34
Preventing SSI: The MOST Important Things67
• Prophylactic antibiotics• Right drug, right dose, right time • No doses after incision closed
• Alcohol-based skin prep• Blood glucose control, all patients • Normothermia, all patients• Increased Fi02, if normal function• Pre-night shower or bath • Treat other infections• Smoking cessation at least 30 days
• No hair removal; if must, clippers • Maintain positive pressure
ventilation• Hand hygiene • Surgical attire worn entire time
including mask and head cover (covering all head and facial hair)
• Clean and disinfect all surfaces between cases
• Flash sterilization only if emergency • Sterile dressing for 24-48 hours
Prevent the Devastating Effects of Deep/Organ Space SSI
Are SSI Prevention Care Practices Performed Routinely?
68

35
SSI Prevention Practice Observations
69
41 Hospitals with High SSI Rates, 2016-2017 # Observations Adherence 62 Operating Rooms 641 72% OR Clean 69% Appropriate Surgical Attire 48% Timely, Appropriate Antibiotic Administration 94% Alcohol-Based Skin Prep 91% Door Closed to Maintain Positive Air Pressure 72% Safe Injection Practices Observed 72% Hand Hygiene Adherence 48%
70
Facility-wide Adherence Monitoring Program

36
Adherence Monitoring Program Checklist• Initiate meeting for ongoing participation and support
• Include chief-level executives and multidisciplinary team members• Establish as a hospital-wide program• Develop the hospital Adherence Monitoring Program policy
• Include all patient care departments• Decide where and how often to be performed• Compile adherence monitoring tools to be used*• Decide how feedback of results will be delivered to staff
• Develop formal training for staff performing adherence monitoring• Hold a kick-off event to inform staff of program• Develop a plan for feedback and remediation of identified practice gaps• Develop a plan to celebrate successes
71
CDPH Adherence Monitoring Tools
All HAI / Core• Hand hygiene• Safe injection practices• Blood glucose meter• Environmental cleaning and
disinfection• Device reprocessing• High level disinfection of reusable
devices
72
CDI• Contact precautions• CDI-targeted ASP practices (coming soon)CLABSI• Central line insertion practices central line
maintenance• Central line access and dressing changesSSI• OR observations• Sterilization of reusable devices

37
Monitoring Hand Hygiene73
Monitoring Contact Precautions
74
2 2
2 2
2 2
1 2
2 2
0 2
2 2
1411 79

38
Summary
Hospitals need to know the gaps to correct the gaps
Every care giver needs to own HAI, know how to prevent them, and practice consistently
HAI can only be prevented if every HCP adheres to evidence-based practices
75
Updates and Clarifications
Debby Rogers, RN, MS, FAEN, Vice President, Clinical Performance & Transformation, California Hospital Association

39
Outline
• Centralized Applications Branch Update
• Performance Metrics
• Program Flexibility
• Sterile Compounding Requirements
• Top Deficiencies & GACH Relicensing Survey
• Title 22 Updates
• CDPH Provider and Consumer Engagement Expectations
• Problem Resolution
• Immediate Jeopardy/Enforcement Actions
• Plans of Correction
• Emergency Food Supply Requirements
• CDPH Referrals to Accrediting Organizations
• Use of Licensed Space
• Recent Legislation
• Tubing Connectors77
78
Centralized Applications Branch
• Centralized Applications Unit becomes a Branch
• Increased staffing • Increased training• Specialization of CAB staff (e.g. analysts with
training in hospital applications)

40
Hospital/Acute Psychiatric Hospital Application Volume
79
0
50
100
150
200
250
300
350
400
450
500
Q4 Q1 Q2 Q3 Q4
FY 2016-17 FY 2017-18
Acute Psychiatric Hospital and General Acute Care HospitalAll Applications Type
Application Received
Application Completed
Application Completed within 100 days ofreceipt
Hospital/Acute Psychiatric Hospital Application Pending Review
80
0
100
200
300
400
500
600
Q4 Q1 Q2 Q3 Q4
FY 2016-17 FY 2017-18
Acute Psychiatric Hospital and General Acute Care HospitalAll Applications Type
Application Pending CAU Review by the End ofthe Selected Period, regardless of Receipt Date
Application Pending Provider Review by the Endof the Selected Period, regardless of ReceiptDate

41
Median Age of Hospital/Acute Psychiatric Hospital Applications
81
0
20
40
60
80
100
120
140
160
180
Q4 Q1 Q2 Q3 Q4
FY 2016-17 FY 2017-18
Median Age of Open Applications for All Applications Type
CAB Contact Information
Completed Applications are sent to:California Department of Public Health Licensing and Certification Program Centralized Applications BranchPO Box 997377, MS 3207Sacramento, CA 95899-7377(916) [email protected]
Application Status or Questions [email protected].• Name of Facility or Agency• License or Facility/Agency # (if you already have one)• Address• Facility or Provider Type• Date documentation sent• Contact Number
82

42
83
CDPH Performance Metrics
https://www.cdph.ca.gov/Programs/CHCQ/LCP/Pages/CHCQPerformanceMetrics.aspx
84
Non-Long-term Care Facility Complaints and Entity Reported Events

43
85
All Facilities Letters
https://www.cdph.ca.gov/Programs/CHCQ/LCP/Pages/LNCAFL.aspx
Program Flexibility (AFL 18-19)
• Must demonstrate its ability to meet related statutory requirements found in the Health and Safety Code
• All flexes are reviewed on a case-by-case basis
• Submit CDPH form 5000 to the local CDPH district office including:o Each regulation for which the facility is requesting flex
o Explanation of the alternative concept, methods, procedure, etc. proposed to use
o Supporting evidence of how the flex will meet the intent of the regulation
o Representative signature
• The District Office should review and respond within 60 days
• All approved program flexibility will specify an expiration date and are subject to specific terms and conditions
• CDPH will review all flexes during the tri-annual relicensing survey
86

44
Posting Program Flex
• Title 22 requires posting all program flexibilities next to the hospital license
• Many hospitals have multiple program flexes, thus making posting all impractical
• If hospitals want to keep program flexes in a central location, the hospital must request and receive a program flex from CDPH
• This flex request should include where the flexes will be kept, how an individual viewing the posting of the current license would know these flexes have been granted, and any additional information requested by the District Office
87
Sterile Compounding Pharmacy Requirements
• The California Board of Pharmacy (BoP), the Office of Statewide Health Planning and Development and the CDPH Licensing and Certification Program all have requirements for hospitals performing sterile compounding
• All Facilities Letter 18-20 provides information for hospitals related to requirements for new or remodeled pharmacy clean rooms and use of mobile sterile compounding units in general acute care hospitals. Hospitals must obtain CDPH approval for:
• All new or remodeled pharmacy clean rooms under the hospital’s license.
• Program flexibility approval — to temporarily use mobile sterile compounding units.
• CDPH advises hospitals to submit applications to the Centralized Applications Branch 120 days prior to the anticipated completion of the new or remodeled pharmacy, and to clearly mark that the application is for sterile compounding
• CDPH advises contacting the CDPH Pharmacy Consultant Unit at [email protected] 90 days prior to anticipated completion
88

45
General Acute Care Relicensing Survey
• The GACH Relicensing Survey was implemented on March 1, 2016 and merged California’s licensing regulations and statue requirements with elements of the former stand-alone Medication Error Reduction Plan (MERP) survey and Patient Safety Licensing Survey (PSLS) into one survey process
• CDPH resources available:• Relicensing Survey Overview • Process Guidance• Regulations with Survey Procedures• General Entrance List • Pharmacy Entrance List• Survey Activity Schedule• Medication Pass Worksheet• Relicensing Evaluation Form
https://www.cdph.ca.gov/Programs/CHCQ/LCP/Pages/GeneralAcuteCareRelicensingSurvey.aspx
89
Top Deficiencies from Relicensing Surveys 2017-2018
GACH Relicensure - Deficiency Cited From 03/01/2017 - 02/28/2018Regulation Description Count
Total 1248Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(c)(1) 78Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(g)(2) 59Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(q)(9) 56Nursing Service Policies and Procedures. / T22 DIV5 CH1 ART3-70213(a) 54Infection Control Program / T22 DIV5 CH1 ART7-70739(a) 40Infection Control Program / T22 DIV5 CH1 ART7-70739(a)(1) 36Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(r) 29Planning and Implementing Patient Care / T22 DIV5 CH1 ART3-70215(b) 28Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(q)(6) 26Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(f)(2) 23General Safety and Maintenance / T22 DIV5 CH1 ART8-70837(a) 22Surgical Service General Requirements / T22 DIV5 CH1 ART3-70223(b)(2) 19Planning and Implementing Patient Care / T22 DIV5 CH1 ART3-70215(a)(2) 15Annual Review / 1339.63 (e) (2) 13Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(f)(1) 13Planning and Implementing Patient Care / T22 DIV5 CH1 ART3-70215(c) 13Infection Control Program / T22 DIV5 CH1 ART7-70739(b) 11Multidisciplinary Process / 1339.63 (e)(6) 10Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(f) 10Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(q)(8) 10Planning and Implementing Patient Care / T22 DIV5 CH1 ART3-70215(a)(1) 9Basic Emergency Medical Service, Physician on / T22 DIV5 CH1 ART6-70413(a) 8Nursing Service Policies and Procedures. / T22 DIV5 CH1 ART3-70213(b) 8Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(g) 8Space Conversion / T22 DIV5 CH1 ART8-70805 8
90

46
91
GACH Relicensure - Deficiency Cited From 03/01/2017 - 02/28/2018Regulation Description Count
Total 1248Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(c)(1) 78Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(g)(2) 59Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(q)(9) 56Nursing Service Policies and Procedures. / T22 DIV5 CH1 ART3-70213(a) 54Infection Control Program / T22 DIV5 CH1 ART7-70739(a) 40Infection Control Program / T22 DIV5 CH1 ART7-70739(a)(1) 36Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(r) 29Planning and Implementing Patient Care / T22 DIV5 CH1 ART3-70215(b) 28Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(q)(6) 26Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(f)(2) 23General Safety and Maintenance / T22 DIV5 CH1 ART8-70837(a) 22Surgical Service General Requirements / T22 DIV5 CH1 ART3-70223(b)(2) 19Planning and Implementing Patient Care / T22 DIV5 CH1 ART3-70215(a)(2) 15Annual Review / 1339.63 (e) (2) 13Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(f)(1) 13Planning and Implementing Patient Care / T22 DIV5 CH1 ART3-70215(c) 13Infection Control Program / T22 DIV5 CH1 ART7-70739(b) 11Multidisciplinary Process / 1339.63 (e)(6) 10Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(f) 10Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(q)(8) 10Planning and Implementing Patient Care / T22 DIV5 CH1 ART3-70215(a)(1) 9Basic Emergency Medical Service, Physician on / T22 DIV5 CH1 ART6-70413(a) 8Nursing Service Policies and Procedures. / T22 DIV5 CH1 ART3-70213(b) 8Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(g) 8Space Conversion / T22 DIV5 CH1 ART8-70805 8
Top Deficiencies from Relicensing Surveys 2017-2018 (cont.)
92
GACH Relicensure - Deficiency Cited From 03/01/2017 - 02/28/2018Regulation Description Count
Total 1248Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(c)(1) 78Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(g)(2) 59Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(q)(9) 56Nursing Service Policies and Procedures. / T22 DIV5 CH1 ART3-70213(a) 54Infection Control Program / T22 DIV5 CH1 ART7-70739(a) 40Infection Control Program / T22 DIV5 CH1 ART7-70739(a)(1) 36Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(r) 29Planning and Implementing Patient Care / T22 DIV5 CH1 ART3-70215(b) 28Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(q)(6) 26Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(f)(2) 23General Safety and Maintenance / T22 DIV5 CH1 ART8-70837(a) 22Surgical Service General Requirements / T22 DIV5 CH1 ART3-70223(b)(2) 19Planning and Implementing Patient Care / T22 DIV5 CH1 ART3-70215(a)(2) 15Annual Review / 1339.63 (e) (2) 13Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(f)(1) 13Planning and Implementing Patient Care / T22 DIV5 CH1 ART3-70215(c) 13Infection Control Program / T22 DIV5 CH1 ART7-70739(b) 11Multidisciplinary Process / 1339.63 (e)(6) 10Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(f) 10Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(q)(8) 10Planning and Implementing Patient Care / T22 DIV5 CH1 ART3-70215(a)(1) 9Basic Emergency Medical Service, Physician on / T22 DIV5 CH1 ART6-70413(a) 8Nursing Service Policies and Procedures. / T22 DIV5 CH1 ART3-70213(b) 8Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(g) 8Space Conversion / T22 DIV5 CH1 ART8-70805 8
Top Deficiencies from Relicensing Surveys 2017-2018 (cont.)

47
93
GACH Relicensure - Deficiency Cited From 03/01/2017 - 02/28/2018Regulation Description Count
Total 1248Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(c)(1) 78Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(g)(2) 59Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(q)(9) 56Nursing Service Policies and Procedures. / T22 DIV5 CH1 ART3-70213(a) 54Infection Control Program / T22 DIV5 CH1 ART7-70739(a) 40Infection Control Program / T22 DIV5 CH1 ART7-70739(a)(1) 36Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(r) 29Planning and Implementing Patient Care / T22 DIV5 CH1 ART3-70215(b) 28Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(q)(6) 26Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(f)(2) 23General Safety and Maintenance / T22 DIV5 CH1 ART8-70837(a) 22Surgical Service General Requirements / T22 DIV5 CH1 ART3-70223(b)(2) 19Planning and Implementing Patient Care / T22 DIV5 CH1 ART3-70215(a)(2) 15Annual Review / 1339.63 (e) (2) 13Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(f)(1) 13Planning and Implementing Patient Care / T22 DIV5 CH1 ART3-70215(c) 13Infection Control Program / T22 DIV5 CH1 ART7-70739(b) 11Multidisciplinary Process / 1339.63 (e)(6) 10Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(f) 10Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(q)(8) 10Planning and Implementing Patient Care / T22 DIV5 CH1 ART3-70215(a)(1) 9Basic Emergency Medical Service, Physician on / T22 DIV5 CH1 ART6-70413(a) 8Nursing Service Policies and Procedures. / T22 DIV5 CH1 ART3-70213(b) 8Pharmaceutical Service General Requirements / T22 DIV5 CH1 ART3-70263(g) 8Space Conversion / T22 DIV5 CH1 ART8-70805 8
Top Deficiencies from Relicensing Surveys 2017-2018 (cont.)
Title 22 Update Work
• AFL 18-22, which applies to hospital cardiovascular surgery service and cardiac catheterization laboratory service regulations
• AFL 18-23, which applies to hospital surgical service regulations
• AFL 18-24, which applies to hospital anesthesia service regulations
• AFL 18-30, which applies to hospital administration regulations
• AFL 18-31, which applies to hospital employee/personnel records requirements
• AFL 18-32, which applies to hospital license, supplemental service approval and special permit regulations
• AFL 18-33, which applies to hospital medical records regulations
• AFL 18-34, which applies to hospital medical service regulations
• AFL 18-35, which applies to hospital records and reporting regulations
• AFL 18-36, which applies to small and rural hospital regulations
• AFL 18-40, which applies to hospital infection control and physical plant regulations
• AFL 18-42, which applies to change of ownership regulations94

48
CDPH Provider and Consumer Engagement Expectations
• Professional conduct, which includes demonstrating mutual respect and cooperation between staff, consumers and providers
• Staff will be trained and knowledgeable in conducting surveys and investigations and will adhere to the principles of investigation
• Surveys will be conducted in an unbiased and nondiscriminatory manner in accordance with program policies and procedures
• Upon entering the facility, the CDPH survey team leader will introduce the team, discussion expectations, outline the survey process, provide a checklist of documents, and more
https://www.calhospital.org/sites/main/files/file-attachments/pacee_3.16.18.pdf?_cldee=ZHJvZ2Vyc0BjYWxob3NwaXRhbC5vcmc%3d&recipientid=contact-6a8c1358e6c3e51180cd2c44fd7ff449-82e91ff195b341aeb55e56bb8068721c&utm_source=ClickDimensions&utm_medium=email&utm_campaign=CHA%20News%20Campaign&esid=af43e046-886a-e811-812a-00155d0ca412
95
Problem Resolution and Escalation Process
Strive to resolve problems at the lowest level possible starting with the District Office supervisor. If there is no resolution to the issue, contact:
• District Manager or District Administrator
• Field Operations Branch Chief
• Chief of Field Operations
96

49
Immediate Jeopardy/Enforcement Actions
• CHA’s Sortable IJ Catalog: https://www.calhospital.org/general-information/catalog-cdph-immediate-jeopardy-administrative-penalties-1
• CDPH IJs - https://www.cdph.ca.gov/Programs/CHCQ/LCP/Pages/Hospital-Administrative-Penalties-by-Year.aspx
• CDPH state enforcement information is under each hospital –https://www.cdph.ca.gov/programs/chcq/lcp/calhealthfind/Pages/Home.aspx
97
Plan of Correction
• CDPH, and CMS, allow facilities to stable the plan of correction to 2567 (AFL 17-23)
• CDPH states three elements are required for State Survey Plan of Correction (POC):
• Corrective action to be taken for each individual affected by the deficient practice, including any system changes that must be made
• The position of the person who will monitor the corrective action and the frequency of monitoring
• Dates each corrective action will be completed
• CDPH Goal: have providers complete the POC within 10 calendar days from date of the issuance of the 2567 but there are times when the deadline cannot be met. The POC does not have to be fully implemented at the time the POC is due back to CDPH.
98

50
CDPH Referrals to Accrediting Organizations AFL (18.05.1)
• CDPH developed a process for referring low and medium non-immediate jeopardy entity-reported incidents (ERIs) to accrediting organizations
• Hospitals are advise to continue to report ERIs to their District Office for triage and prioritization
• If the District Office determines that the ERI is eligible for referral to an accrediting organization it will inform the entity that it may contact the applicable accrediting organization for further action on the ERI
• CDPH will investigate all events triaged as immediate jeopardy (IJ), non-IJ high priority events and all state requirements (e.g. adverse events)
This AFL supersedes ALFs 17.11 and 18.05.
99
Use of Licensed Space
• HSC 1251. “License” means a basic permit to operate a health facility with an authorized number and classification of beds. A license shall not be transferable.
• HSC 1256.1. A general acute care hospital shall not hold itself out directly or indirectly by any sign, brochure, or advertisement as providing any service or services that require a supplemental or special service unless that general acute care hospital has first obtained a supplemental or special service approval from the State Department of Public Health to operate that service.
• Title 22 70105 Application RequiredA verified application shall be forwarded to the Department whenever any of the following circumstances occur:
• Construction of a new or replacement facility or addition to an existing facility
• Increase or decrease of licensed bed capacity
• Added service or change from one service to another
• Change of ownership
• Change of name of hospital
• Change of license category
• Change of location of the hospital
• Change of bed classification
Title 22 70805 Space Conversion
Spaces approved for specific uses at the time of licensure shall not be converted to other uses without the written approval of the Department.
100

51
Recently Signed Legislation
• SB 1138 (Skinner) – Plant-Based Meals
• SB 1152 (Hernandez) – Discharge of Homeless Patients
• AB 2798 (Maienschein) – CDPH Centralized Applications Unit Timelines
• AB 2679 (O’Donnell) – Laundry Processing Standards
• SB 1288 (Leyva) – Nurse Staffing Ratio Penalties– Vetoed
• AB 940 (Weber) – SNF Initiated Transfer – 2016
• AB 3032 (Frazier) & AB 2193 (Maienschein) – Maternal Mental Health Conditions
101
Construction/Multi-Stages Projects: CDPH Pre-Meeting
Consider contacting CDPH District Office and Centralized Applications Branch to discuss multi-staged projects
102

52
Tubing Connector Prohibition
• The law prohibiting hospitals from using tubing “connectors that would fit into a connector other than the type it was intended for” for intravenous, epidural and enteral feeding connectors went into effect in 2016
• The law requires hospitals to develop, implement and comply with a patient safety plan to improve patients’ health and safety and reduce preventable patient safety events (HSC 1279.6). Patient safety plans must include measures to prevent adverse events associated with misconnecting IV, enteral feeding and epidural lines (HSC 1279.7)
• Review the patient safety plan to ensure that prevention of adverse events associated with these misconnections is adequately addressed, and perform a risk analysis addressing the availability of connectors and identifying methods to mitigate risk. The plan may include an assessment of the sustained availability of connectors that meet the legal standard, staff training, etc.
103
Parkinson’s Disease Reporting
• A new state law requires health care providers diagnosing or treating Parkinson’s disease patients to report each case to CDPH as of July 1, 2018
• CDPH revised Parkinson’s Disease Registry Implementation Guide requires only certain providers (medical doctor, doctor of osteopathy, physician's assistant or nurse practitioner) to report cases/treatment of Parkinson’s disease
• A webinar is planned for November 16th
• Providers can submit case data using the manual data entry portal using CalREDIEAuthorization form. Or submit data electronically
• Questions should be directed to [email protected]
https://www.cdph.ca.gov/Programs/CCDPHP/DCDIC/CDSRB/Pages/California-Parkinson%27s-Disease-Registry.aspx 104

53
Observation Status Patients
• Observation status must be ordered by the provider
• Observation services can be provided in ED, inpatient unit(s) and an observation unit
• Observation units must meet OSHPD building requirements and provide 1:4 staffing ratios
105
CHA Licensing Manual
106
The California Hospital Survey Manual can help hospitals prepare for the survey process, and explains who the surveyors are and how they conduct their surveys. It covers the different types of surveys and possible outcomes
To order:https://www.calhospital.org/survey-manual

54
Questions
Online questions:Type your question in the Q & A box, press enter
Phone questions:To ask a question, press *1
Thank You
Cari Lee, Pharm.D.Pharmaceutical Consultant Unit ChiefCalifornia Department of Public [email protected]
Debby Rogers, RN, MS, FAENVice President, Clinical Performance & TransformationCalifornia Hospital [email protected]
Lori Schaumleffel, RN, BSN, PHN, CICInfection Prevention LiaisonCalifornia Department of Public [email protected]

55
Upcoming Programs
Behavioral Health Care Symposium & Emergency Services ForumDecember 10-12, 2018Mission Inn Hotel and Spa and Riverside Convention Center
Day 1: Focus is on behavioral health care policy and pressing issues. Day 2: This blended format is designed for both behavioral health care providers and ED professionals.Day 3: Emphasis is solely on emergency medical care services issues and innovative practices to create future-focused ED care systems.
Visit the conference webpages for more information:www.calhospital.org/behavioral-symposiumwww.calhospital.org/emergency-services-forum
Thank You and Evaluation
Thank you for participating in today’s webinar. An online evaluation will be sent to you shortly.
For education questions, contact Robyn Thomason at (916) 552-7514 or [email protected].