Embed Size (px)
Citation preview
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 1 of 26
CDDFT Policy
Reference Number POL/N&G/0015
Title Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients).
Version number 2.2
Document Type Policy
Original policy date October 2011
Date approved 23rd February 2012
Effective date 27th February 2012
Approving body Quality and Healthcare Governance Committee
Originating Directorate Nursing and Service Transformation
Scope Trust-wide
Last review date February 2012
Next review date October 2014
Reviewing body VTE Group
Document Owner Clinical Effectiveness Lead
Equality impact assessed
Yes
Date superseded N/A
Status Approved
Confidentiality Unrestricted
Keywords Venous thromboembolism, VTE, deep vein thrombosis, DVT, pulmonary embolism, PE, assessment, prophylaxis, low molecular weight heparin(LMWH), anti-embolic stockings, flowtrons
Approval
Signature of Chairman of Approving Body
Name / job title of Chairman of approving Body:
Diane Murphy Chair of Quality and Healthcare Governance Committee
Signed paper copy held at (location): Library Services DMH
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 2 of 25
Contents
Section Page
1. Introduction 4
2. Scope 4
3. Purpose 4
4. Definitions 4
5. Duties 4
6. Procedure to follow if DVT is suspected 4
6.1 Signs and symptoms 4
6.2 Risk factors to consider in history taking 5
6.3 Wells‘ scoring system 5
6.4 D-dimer testing 6
7 Management of DVT 6
8 Procedure to follow if PE is suspected 7
8.1 Signs and symptoms 7
8.2 Use of CPTA and VQ imaging of investigation of possible acute pulmonary embolism
7
8.2.1 Clinical 7
8.2.2 D-dimer 8
8.2.3 Requesting chest imaging 8
8.2.4 Imaging of non-massive PE 8
8.2.5 Imaging of massive PE 9
8.2.6 Imaging in pregnancy 9
9 Management of PE 9
10 Management on discharge 9
11 Root Cause Analysis 9
12 Monitoring 10
13 References and sources of information 10
14 Associated documents 11
15 Equality Impact Assessment 12
Appendices
Appendix 1 Flow chart for DVT diagnosis 18
Appendix 2 Anticoagulation record sheet 19
Appendix 3 Imaging pathway for PE 21
Appendix 4 Checklist for requesting CPTA and VQ investigation in suspected PE.
22
Appendix 5 Flowchart for management of confirmed PE 23
Appendix 6 Contraindications to LMWH 24
Appendix 7 Root Cause Analysis Tool 25
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 3 of 25
Document Control Information
Version control table
Date of issue Version number Status
June 2011 1.0 Superseded
September 2011 1.1 Superseded
October 2011 2.0 Superseded
January 2012 2.1 Superseded
23rd February 2012 2.2 Approved
Table of revisions
Date Section Revision Author
September 2011
Various sections
Revision of versions 1.0 –working draft documents taking into account peer comments
Helen Rutter – Clinical Effectiveness Lead
October 2011
Various sections
Revision of versions 1.1 –working draft documents taking into account peer comments
Helen Rutter – Clinical Effectiveness Lead
January 2012
11 Added to incorporate the Root Cause Analysis process for VTE episodes
Helen Rutter - Clinical Effectiveness Lead
February 2012
Monitoring Monitoring mechanisms made more specific. Helen Rutter - Clinical Effectiveness Lead
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 4 of 25
1. Introduction Venous thromboembolism (VTE), in either the form of deep vein thrombosis (DVT) or pulmonary embolism (PE) has been identified as being one of the main causes of morbidity and mortality in medical and surgical patients. Both present with a large range of clinical symptoms ranging from asymptomatic DVT to life threatening, acute PE. VTE has a high mortality when untreated but treatment also carries risks, principally haemorrhage. Therefore, accurate confirmation of diagnosis is essential in all patients, usually by imaging. In addition, the duration of treatment with antithrombotics requires individual and careful consideration of the balance of benefits (reduced risk of long term complications and recurrent thrombosis) and risks (principally haemorrhage)1.
2. Scope
This policy applies to all patients who are either admitted with or develop symptoms of either DVT or PE whist an in-patient within the Trust.
Adherence to this policy is the responsibility of all Trust employees
Obstetric patients will be treated in line with policy MATG14 ‗Management of DVT and pulmonary embolism during pregnancy and the puerperium‘ and EMG19 ‗Management of massive PE‘
The recommendations in this policy must be implemented taking into account the patient‘s individual clinical situation and the clinical judgement of the clinician in charge of their care.
Guidance on assessment and prophylaxis is in POL/N&G/0013 Policy for Venous Thromboembolism (VTE) risk assessment and prophylaxis in adult patients admitted to hospital
3. Purpose To ensure safe, standardised, evidence based approach to the diagnosis and treatment of patients who are either admitted with or develop symptoms of either DVT or PE whist an in-patient within the County Durham and Darlington NHS Foundation Trust.
4. Definitions For the purpose of this policy the following definitions stand. VTE: Venous thromboembolism PE: Pulmonary embolism DVT: Deep vein thrombosis LMWH: Low molecular weight heparin CPTA: Computed tomographic pulmonary angiography CXR: Chest x-ray
5. Duties
Medical Director. The Medical Director has overall clinical responsibility and will report issues as they arise to the Board
VTE Group. The VTE Group is responsible for overseeing the development and implementation of the guidelines for the diagnosis, treatment and management of VTE.
Clinical Directors. Clinical Directors are responsible for implementation within Care Group.
Medical staff. Medical staff are responsible for carrying out appropriate diagnostics and prescribing appropriate treatment.
Nursing staff. Ward nursing staff are responsible delivering treatment, medication and care as prescribed by medical staff.
6. Procedure to follow if DVT is suspected 6.1 Signs and symptoms
In patients presenting with the following symptoms, investigation for the presence of DVT should be considered.
Calf pain and tenderness
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 5 of 25
Swelling, sometimes with pitting oedema
Localised skin warmth
Erythema
Dilated superficial veins There are a range of conditions which also cause pain and/or swelling of the lower limb hence can be confused with the presence of a DVT. These include superficial thrombophlebitis, post thrombotic syndrome, chronic venous insufficiency, venous obstruction, cellulitis, Baker‘s cyst, torn gastrocnemius muscle, fracture, haematoma, acute arterial ischaemia, lymphoedema and hypoproteinemia. 2,3
6.2 Risk factors to consider in history taking The following factors should be taken in to account when taking the initial patient history
Active cancer or cancer treatment
Age >60
Dehydration
Known thrombophilias
Obesity (BMI >30 kg/m2)
One or more significant medical comorbidities (e.g. heart disease; metabolic, endocrine or respiratory pathologies; acute infectious diseases; inflammatory conditions)
Personal history or first-degree relative with a history of VTE
Use of hormone replacement therapy
Use of oestrogen-containing contraceptive therapy
Varicose veins with phlebitis
Pregnancy or < 6 weeks post partum (see NICE guidance for specific risk factors)
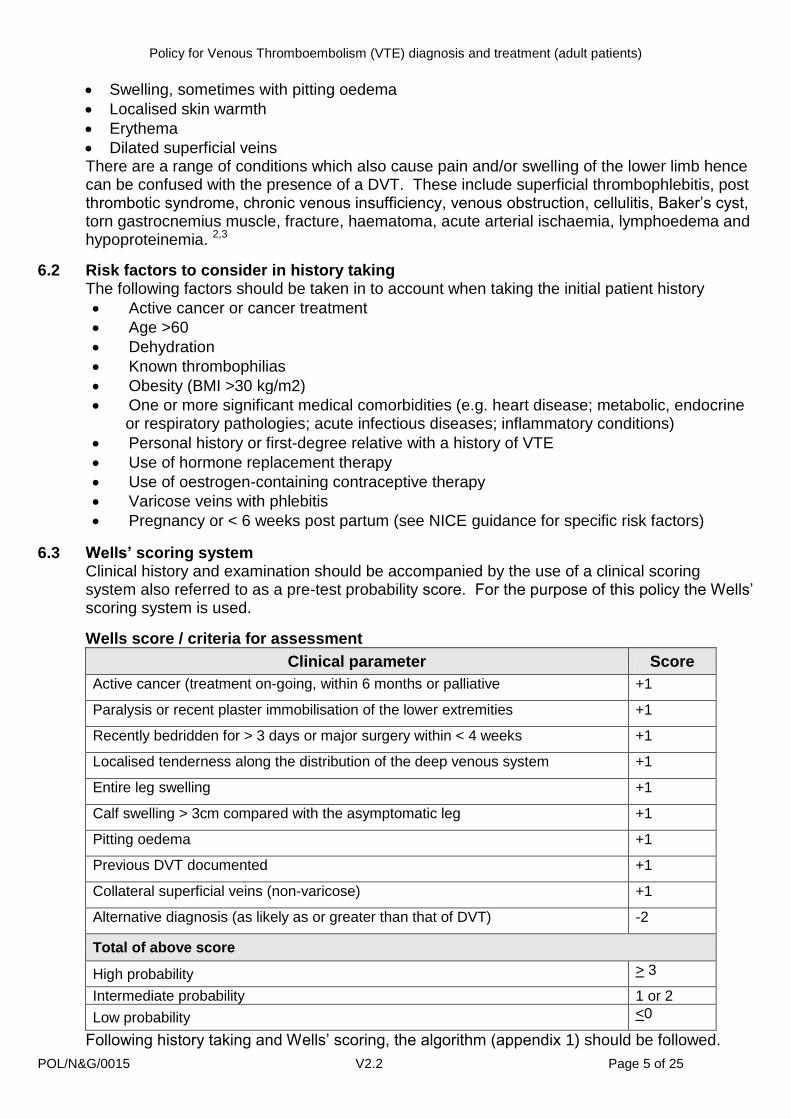
6.3 Wells’ scoring system Clinical history and examination should be accompanied by the use of a clinical scoring system also referred to as a pre-test probability score. For the purpose of this policy the Wells‘ scoring system is used.
Wells score / criteria for assessment
Clinical parameter Score
Active cancer (treatment on-going, within 6 months or palliative +1
Paralysis or recent plaster immobilisation of the lower extremities +1
Recently bedridden for > 3 days or major surgery within < 4 weeks +1
Localised tenderness along the distribution of the deep venous system +1
Entire leg swelling +1
Calf swelling > 3cm compared with the asymptomatic leg +1
Pitting oedema +1
Previous DVT documented +1
Collateral superficial veins (non-varicose) +1
Alternative diagnosis (as likely as or greater than that of DVT) -2
Total of above score
High probability > 3
Intermediate probability 1 or 2
Low probability <0
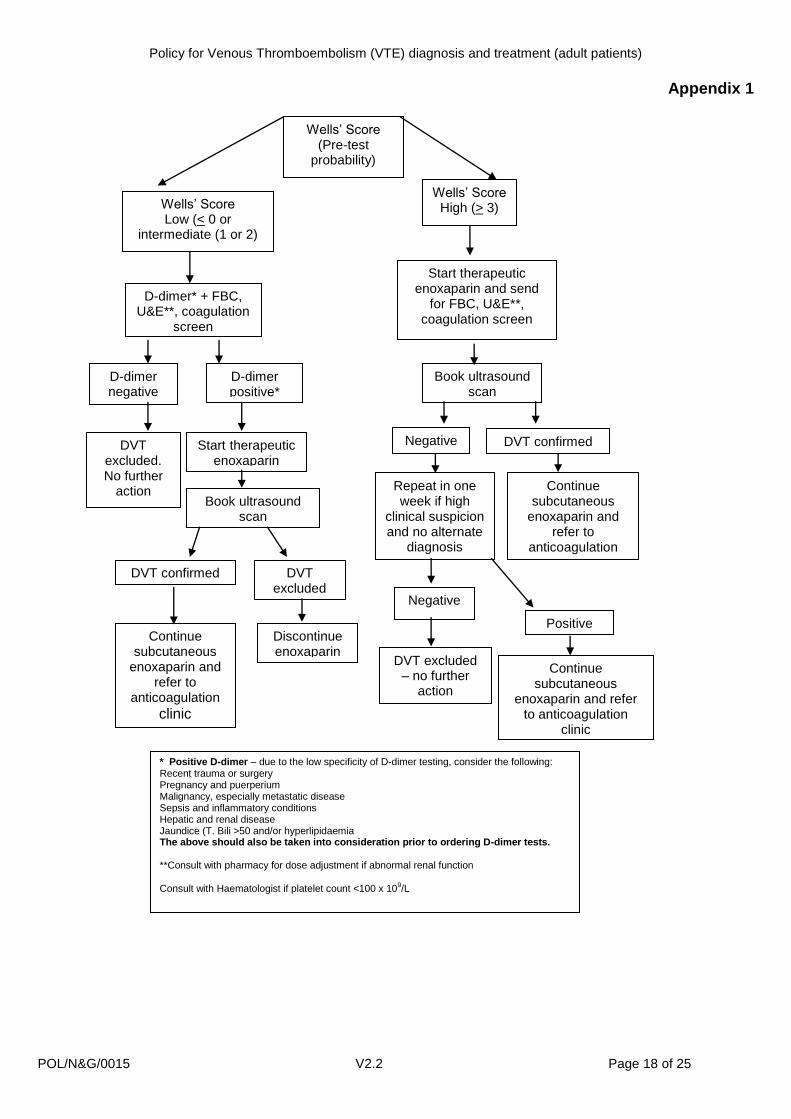
Following history taking and Wells‘ scoring, the algorithm (appendix 1) should be followed.
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 6 of 25
6.4 D-dimer testing A negative D-dimer test is valuable in excluding VTE in patients with low/ intermediate probability (Wells‘ score).
Although a positive D-dimer test has very high sensitivity (close to 100%) in patients with VTE, the test has low specificity (less than 40%), meaning that there are a multitude of other causes that can result is raised D-dimer test in absence of VTE. Many of these latter causes are themselves risk factors for developing VTE. They include: 1- Recent trauma/ Surgery (up to few weeks). 2- Pregnancy and puerperium*. 3- Malignancy especially metastatic disease. 4- Sepsis and inflammatory conditions. 5- Hepatic and Renal diseases.
In addition, false positive (raised) D-dimer can be seen in patients with Jaundice (T.Bili >50), and/ or Hyperlipidaemia.
It is critically important that the above is taken into consideration when requesting/ interpreting results of D-dimer test.
* D-dimer is not a recommended investigation in pregnancy since a negative result has a low sensitivity, i.e. does not reliably exclude VTE in pregnancy.
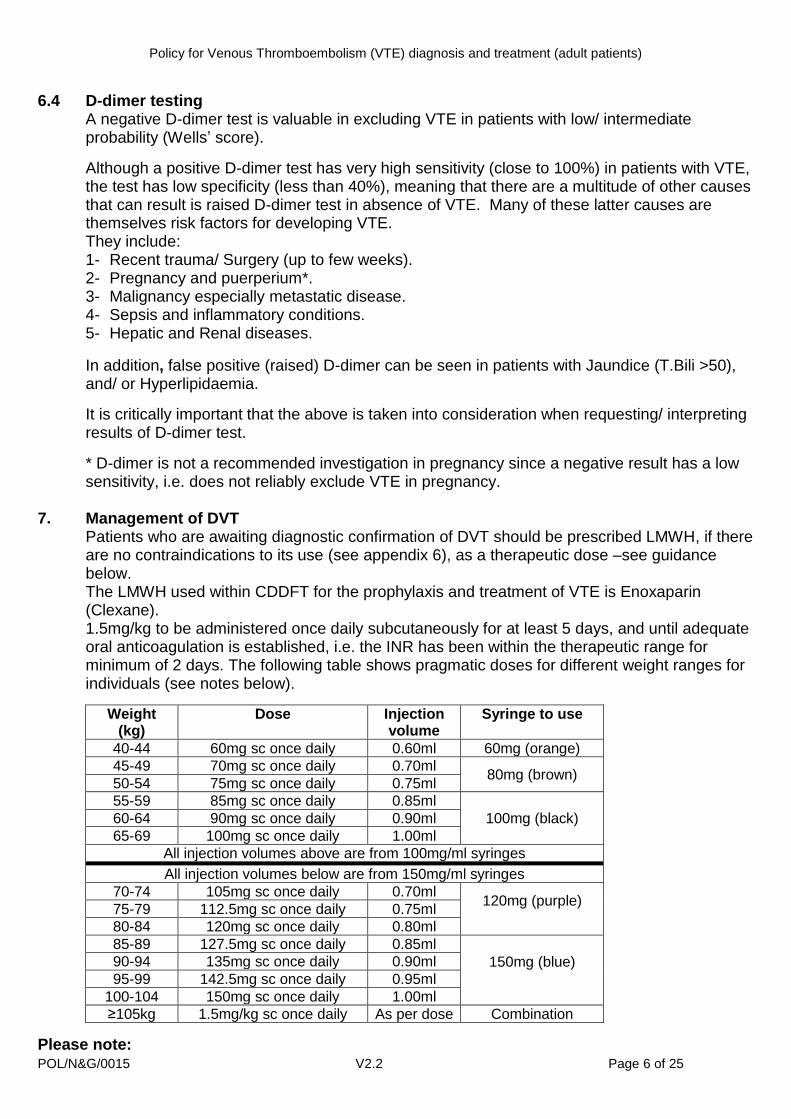
7. Management of DVT Patients who are awaiting diagnostic confirmation of DVT should be prescribed LMWH, if there are no contraindications to its use (see appendix 6), as a therapeutic dose –see guidance below. The LMWH used within CDDFT for the prophylaxis and treatment of VTE is Enoxaparin (Clexane). 1.5mg/kg to be administered once daily subcutaneously for at least 5 days, and until adequate oral anticoagulation is established, i.e. the INR has been within the therapeutic range for minimum of 2 days. The following table shows pragmatic doses for different weight ranges for individuals (see notes below).
Weight (kg)
Dose Injection volume
Syringe to use
40-44 60mg sc once daily 0.60ml 60mg (orange)
45-49 70mg sc once daily 0.70ml 80mg (brown)
50-54 75mg sc once daily 0.75ml
55-59 85mg sc once daily 0.85ml
100mg (black) 60-64 90mg sc once daily 0.90ml
65-69 100mg sc once daily 1.00ml
All injection volumes above are from 100mg/ml syringes
All injection volumes below are from 150mg/ml syringes
70-74 105mg sc once daily 0.70ml 120mg (purple)
75-79 112.5mg sc once daily 0.75ml
80-84 120mg sc once daily 0.80ml
85-89 127.5mg sc once daily 0.85ml
150mg (blue)
90-94 135mg sc once daily 0.90ml
95-99 142.5mg sc once daily 0.95ml
100-104 150mg sc once daily 1.00ml
≥105kg 1.5mg/kg sc once daily As per dose Combination
Please note:
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 7 of 25
Patients with severe renal impairment (creatinine clearance < 30ml/min) should be administered 1mg/kg once daily subcutaneously
There is no maximum dose; in patients of above 105kg, calculations should be based on 1.5mg/kg
If patient is admitted on anticoagulant therapy, refer to Anticoagulant record sheet (appendix 2) for dosage guidance
If patient is admitted on antiplatelet agents on admission, review must be made by the appropriate physician and discontinued as instructed
Patients with a true allergy to LMWH should be managed with alternative parenteral anticoagulants, e.g. Hirudins or Heparinoids. Contact pharmacy for advice regarding the most suitable agent
For warfarin guidance and INR ranges see appendix 2 - Anticoagulant record sheet. Please note:
Warfarin is contraindicated in pregnancy and the guidelines referred to in section 2 should be consulted.
Oncology patients should not be commenced on warfarin without oncologists review. 8. Procedure to follow if PE is suspected 8.1 Signs and symptoms
In patients presenting with the following symptoms, investigation for the presence of PE should be considered in the differential diagnosis -
Dyspnoea
Tachypnoea
Pleuritic chest pain
Cough
Haemoptysis
Cyanosis
Collapse
Circulatory instability
8.2 Use of CTPA and VQ imaging of investigation of possible acute pulmonary embolism Recommendations based on BTS guidelines 2003 with input from the European Association of Nuclear Medicine Guidelines 2009 for V/Q SPECT scintigraphy4,5
8.2.1 Clinical
All patients with possible PE should have clinical probability assessed and documented (as per PIOPED II recommendations). See Section 6.3. Wells‘ scoring system.
As an alternative to the Wells‘ scoring system, the following system (BTS 2003) can be used. Patient has clinical features compatible with PE—namely, breathlessness and/or tachypnoea, with or without pleuritic chest pain and/or haemoptysis. Two other factors are sought: (a) the absence of another reasonable clinical explanation, and (b) the presence of a major risk factor. Where (a) and (b) are both true the probability is high; if only one is true the probability is intermediate; and if neither is true the probability is low.
An alternative clinical explanation should always be considered at presentation and sought when PE is excluded
High clinical probability may proceed to chest imaging without d-dimer
CXR mandatory within 24 hours
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 8 of 25
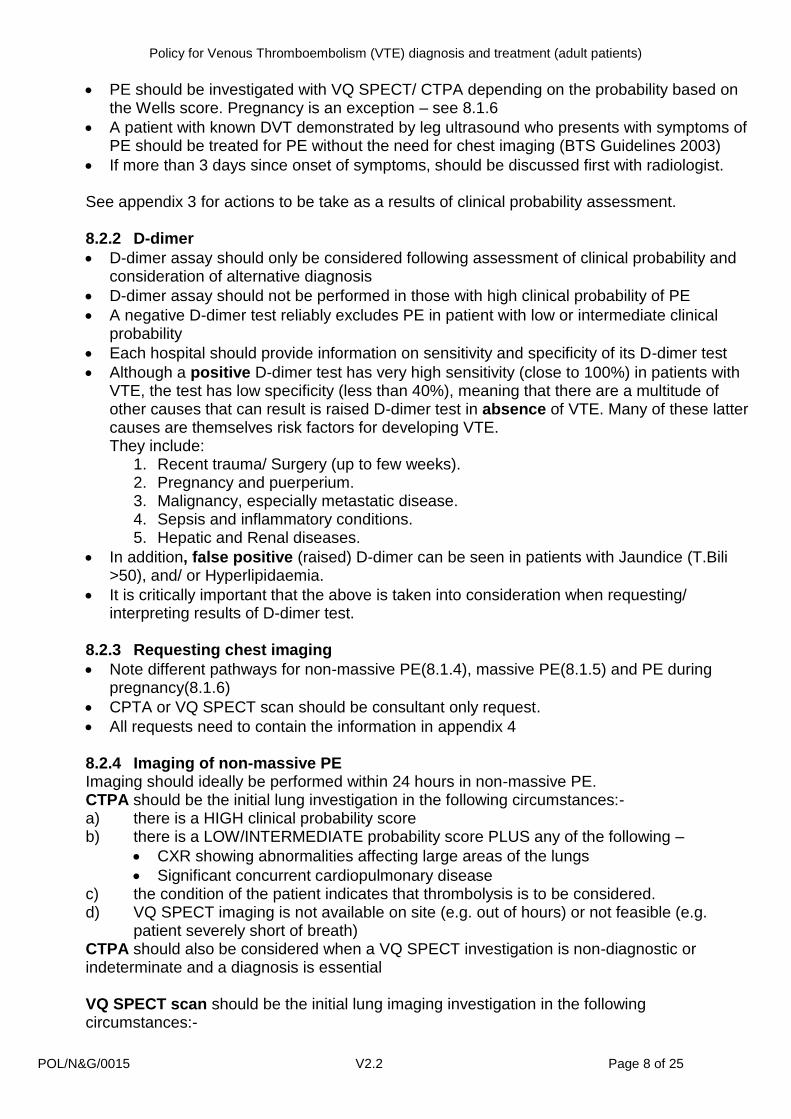
PE should be investigated with VQ SPECT/ CTPA depending on the probability based on the Wells score. Pregnancy is an exception – see 8.1.6
A patient with known DVT demonstrated by leg ultrasound who presents with symptoms of PE should be treated for PE without the need for chest imaging (BTS Guidelines 2003)
If more than 3 days since onset of symptoms, should be discussed first with radiologist. See appendix 3 for actions to be take as a results of clinical probability assessment. 8.2.2 D-dimer
D-dimer assay should only be considered following assessment of clinical probability and consideration of alternative diagnosis
D-dimer assay should not be performed in those with high clinical probability of PE
A negative D-dimer test reliably excludes PE in patient with low or intermediate clinical probability
Each hospital should provide information on sensitivity and specificity of its D-dimer test
Although a positive D-dimer test has very high sensitivity (close to 100%) in patients with VTE, the test has low specificity (less than 40%), meaning that there are a multitude of other causes that can result is raised D-dimer test in absence of VTE. Many of these latter causes are themselves risk factors for developing VTE. They include:
1. Recent trauma/ Surgery (up to few weeks). 2. Pregnancy and puerperium. 3. Malignancy, especially metastatic disease. 4. Sepsis and inflammatory conditions. 5. Hepatic and Renal diseases.
In addition, false positive (raised) D-dimer can be seen in patients with Jaundice (T.Bili >50), and/ or Hyperlipidaemia.
It is critically important that the above is taken into consideration when requesting/ interpreting results of D-dimer test.
8.2.3 Requesting chest imaging
Note different pathways for non-massive PE(8.1.4), massive PE(8.1.5) and PE during pregnancy(8.1.6)
CPTA or VQ SPECT scan should be consultant only request.
All requests need to contain the information in appendix 4 8.2.4 Imaging of non-massive PE Imaging should ideally be performed within 24 hours in non-massive PE. CTPA should be the initial lung investigation in the following circumstances:- a) there is a HIGH clinical probability score b) there is a LOW/INTERMEDIATE probability score PLUS any of the following –
CXR showing abnormalities affecting large areas of the lungs
Significant concurrent cardiopulmonary disease c) the condition of the patient indicates that thrombolysis is to be considered. d) VQ SPECT imaging is not available on site (e.g. out of hours) or not feasible (e.g.
patient severely short of breath) CTPA should also be considered when a VQ SPECT investigation is non-diagnostic or indeterminate and a diagnosis is essential VQ SPECT scan should be the initial lung imaging investigation in the following circumstances:-
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 9 of 25
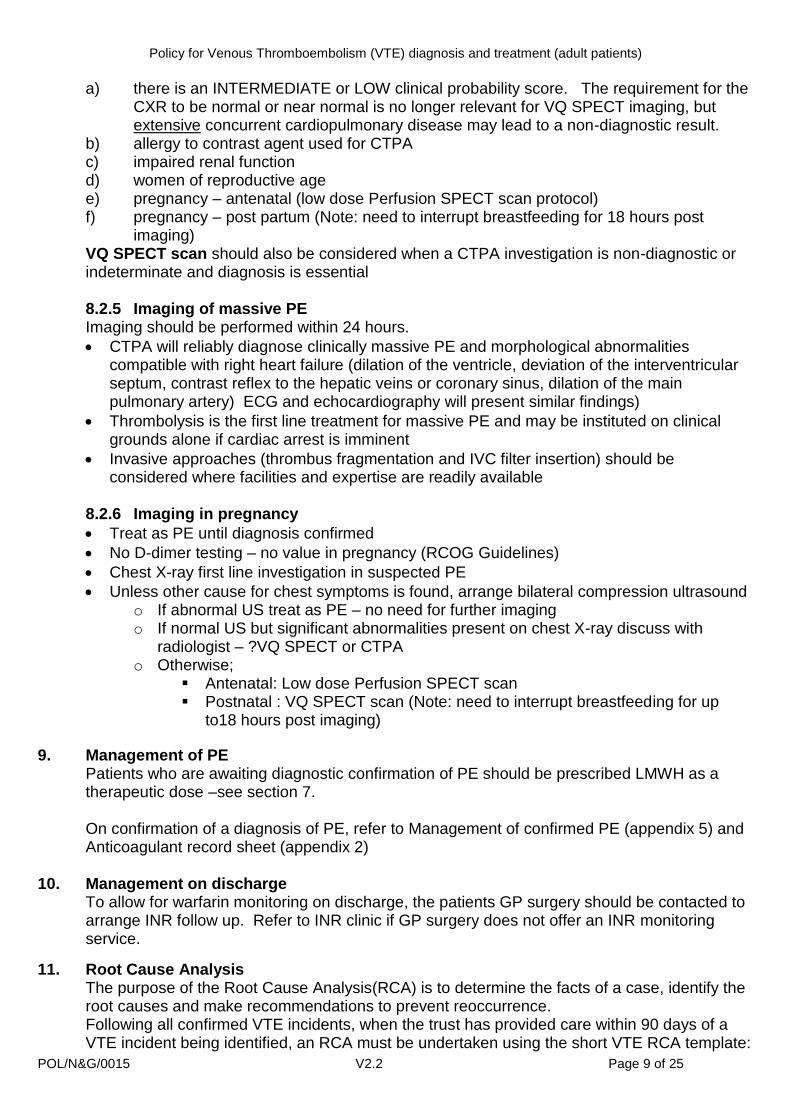
a) there is an INTERMEDIATE or LOW clinical probability score. The requirement for the CXR to be normal or near normal is no longer relevant for VQ SPECT imaging, but extensive concurrent cardiopulmonary disease may lead to a non-diagnostic result.
b) allergy to contrast agent used for CTPA c) impaired renal function d) women of reproductive age e) pregnancy – antenatal (low dose Perfusion SPECT scan protocol) f) pregnancy – post partum (Note: need to interrupt breastfeeding for 18 hours post
imaging) VQ SPECT scan should also be considered when a CTPA investigation is non-diagnostic or indeterminate and diagnosis is essential 8.2.5 Imaging of massive PE Imaging should be performed within 24 hours.
CTPA will reliably diagnose clinically massive PE and morphological abnormalities compatible with right heart failure (dilation of the ventricle, deviation of the interventricular septum, contrast reflex to the hepatic veins or coronary sinus, dilation of the main pulmonary artery) ECG and echocardiography will present similar findings)
Thrombolysis is the first line treatment for massive PE and may be instituted on clinical grounds alone if cardiac arrest is imminent
Invasive approaches (thrombus fragmentation and IVC filter insertion) should be considered where facilities and expertise are readily available
8.2.6 Imaging in pregnancy
Treat as PE until diagnosis confirmed
No D-dimer testing – no value in pregnancy (RCOG Guidelines)
Chest X-ray first line investigation in suspected PE
Unless other cause for chest symptoms is found, arrange bilateral compression ultrasound o If abnormal US treat as PE – no need for further imaging o If normal US but significant abnormalities present on chest X-ray discuss with
radiologist – ?VQ SPECT or CTPA o Otherwise;
Antenatal: Low dose Perfusion SPECT scan Postnatal : VQ SPECT scan (Note: need to interrupt breastfeeding for up
to18 hours post imaging)
9. Management of PE Patients who are awaiting diagnostic confirmation of PE should be prescribed LMWH as a therapeutic dose –see section 7. On confirmation of a diagnosis of PE, refer to Management of confirmed PE (appendix 5) and Anticoagulant record sheet (appendix 2)
10. Management on discharge
To allow for warfarin monitoring on discharge, the patients GP surgery should be contacted to arrange INR follow up. Refer to INR clinic if GP surgery does not offer an INR monitoring service.
11. Root Cause Analysis The purpose of the Root Cause Analysis(RCA) is to determine the facts of a case, identify the root causes and make recommendations to prevent reoccurrence. Following all confirmed VTE incidents, when the trust has provided care within 90 days of a VTE incident being identified, an RCA must be undertaken using the short VTE RCA template:
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 10 of 25
This is available at http://intranet/Directorates/CorporateDirectorates/NursingDirector/ClinGov/PatSafety/Root%20Cause%20Analysis/Forms/AllItems.aspx or see appendix
Consultants and teams have the responsibility to complete this work within 30 working days of the VTE event being recognised. Competed RCA‘s are to be sent to [email protected] or [email protected] in the Patient Safety Team.
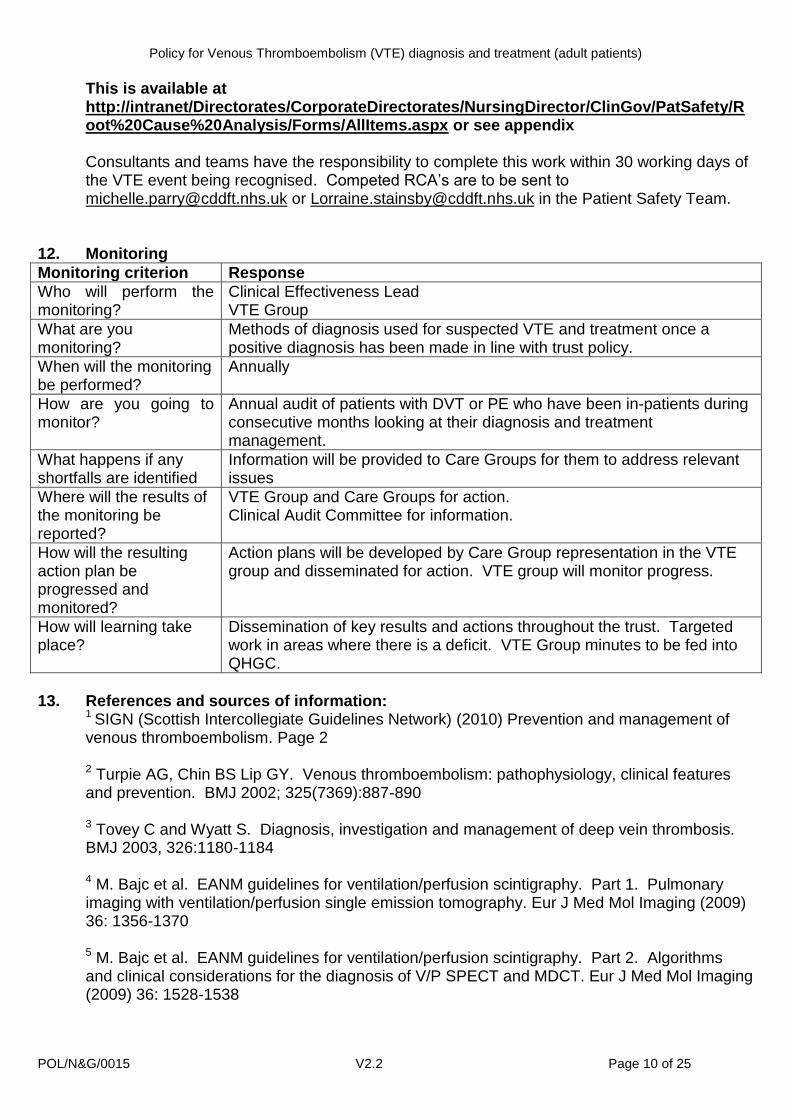
12. Monitoring
Monitoring criterion Response
Who will perform the monitoring?
Clinical Effectiveness Lead VTE Group
What are you monitoring?
Methods of diagnosis used for suspected VTE and treatment once a positive diagnosis has been made in line with trust policy.
When will the monitoring be performed?
Annually
How are you going to monitor?
Annual audit of patients with DVT or PE who have been in-patients during consecutive months looking at their diagnosis and treatment management.
What happens if any shortfalls are identified
Information will be provided to Care Groups for them to address relevant issues
Where will the results of the monitoring be reported?
VTE Group and Care Groups for action. Clinical Audit Committee for information.
How will the resulting action plan be progressed and monitored?
Action plans will be developed by Care Group representation in the VTE group and disseminated for action. VTE group will monitor progress.
How will learning take place?
Dissemination of key results and actions throughout the trust. Targeted work in areas where there is a deficit. VTE Group minutes to be fed into QHGC.
13. References and sources of information:
1 SIGN (Scottish Intercollegiate Guidelines Network) (2010) Prevention and management of venous thromboembolism. Page 2 2 Turpie AG, Chin BS Lip GY. Venous thromboembolism: pathophysiology, clinical features and prevention. BMJ 2002; 325(7369):887-890 3 Tovey C and Wyatt S. Diagnosis, investigation and management of deep vein thrombosis. BMJ 2003, 326:1180-1184 4 M. Bajc et al. EANM guidelines for ventilation/perfusion scintigraphy. Part 1. Pulmonary imaging with ventilation/perfusion single emission tomography. Eur J Med Mol Imaging (2009) 36: 1356-1370
5 M. Bajc et al. EANM guidelines for ventilation/perfusion scintigraphy. Part 2. Algorithms and clinical considerations for the diagnosis of V/P SPECT and MDCT. Eur J Med Mol Imaging (2009) 36: 1528-1538
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 11 of 25
14. Associated documents
Policy for the Development and Management of Policy and Guidance Documents
Clinical Audit
Policy for Venous Thromboembolism (VTE) risk assessment and prophylaxis in adult patients admitted to hospital
Incident Management policy
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 12 of 25
14. Equality Impact Assessment
Equality Analysis / Impact Assessment
Full Assessment Form v2/2011
Division/Department:
Patient Safety and Governance
Title of policy, procedure, decision, project, function or service:
Policy for Venous Thromboembolism (VTE) diagnosis and treatment
Lead person responsible:
Helen Rutter. Clinical Effectiveness Lead
People involved with completing this:
Helen Rutter. Clinical Effectiveness Lead Denise Kirkup. Clinical Audit, Effectiveness and Governance Manager
Type of policy, procedure, decision, project, function or service: Existing New/proposed
Changed
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 13 of 25
Step 1 – Scoping your analysis
What is the aim of your policy, procedure, project, decision, function or service and how does it relate to equality?
The policy describes the process for diagnosing a suspected deep vein thrombosis or pulmonary embolism and the appropriate treatment if confirmed..
Who is the policy, procedure, project, decision, function or service going to benefit and how?
Guidance for staff on diagnosis and treatment. Benefit for patients for in providing staff with this guidance.
What outcomes do you want to achieve?
Correct diagnosis and treatment of deep vein thrombosis or pulmonary embolism.
What barriers are there to achieving these outcomes?
Staff awareness and implementation of the policy.
How will you put your policy, procedure, project, decision, function or service into practice?
Implementation of policy via VTE Group, governance forums and via the intranet.
Does this policy link, align or conflict with any other policy, procedure, project, decision, function or service?
Yes, Policy for Venous Thromboembolism (VTE) risk assessment and prophylaxis in adult
patients admitted to hospital
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 14 of 25
Step 2 – Collecting your information
What existing information / data do you have?
Annual audit and Root Cause Analysis
Who have you consulted with?
VTE Group members, Pharmacy, radiology and appropriate staff within Care Groups
What are the gaps and how do you plan to collect what is missing?
No gaps identified.
Step 3 – What is the impact?
Using the information from Step 2 explain if there is an impact or potential for impact on staff or people in the community with characteristics protected under the Equality Act 2010? Ethnicity or Race
None
Sex/Gender
None
Age
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 15 of 25
None.
Disability
None.
Religion or Belief
None.
Sexual Orientation
None
Marriage and Civil Partnership
None
Pregnancy and Maternity
Specific guidance is available for obstetric patients.
Gender Reassignment
None.
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 16 of 25
Other socially excluded groups or communities e.g. rural community, socially excluded, carers, areas of deprivation, low literacy skills
None.
Step 4 – What are the differences?
Are any groups affected in a different way to others as a result of the policy, procedure, project, decision, function or service?
No
Does your policy, procedure, project, decision, function or service discriminate against anyone with characteristics protected under the Equality Act? Yes No If yes, explain the justification for this. If it cannot be justified, how are you going to change it to remove or mitigate the affect?
Not applicable.
Step 5 – Make a decision based on steps 2 - 4
If you are in a position to introduce the policy, procedure, project, decision, function or service? Clearly show how this has been decided.
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 17 of 25
Agreed, approved and implemented with agreement of the VTE Group and Quality and Healthcare Governance Committee.
If you are in a position to introduce the policy, procedure, project, decision, function or service, but still have information to collect, changes to make or actions to complete to ensure all people affected have been covered please list:
N/A
How are you going to monitor this policy, procedure, project or service, how often and who will be responsible?
Monitoring as described in section 12.
Step 6 – Completion and central collation
Once completed this Equality Analysis form must be attached to any documentation to which it relates and must be forwarded to Jillian Wilkins, Equality and Diversity Lead. [email protected]
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 18 of 25
Appendix 1
Wells‘ Score (Pre-test
probability)
Wells‘ Score Low (< 0 or
intermediate (1 or 2)
Wells‘ Score High (> 3)
D-dimer* + FBC, U&E**, coagulation
screen
D-dimer negative
D-dimer positive*
Start therapeutic enoxaparin
Book ultrasound scan
DVT excluded. No further
action
DVT confirmed DVT excluded
Continue subcutaneous
enoxaparin and refer to
anticoagulation clinic
Discontinue enoxaparin
Book ultrasound scan
Start therapeutic enoxaparin and send
for FBC, U&E**, coagulation screen
Negative DVT confirmed
Repeat in one week if high
clinical suspicion and no alternate
diagnosis
Continue subcutaneous
enoxaparin and refer to
anticoagulation clinic
Negative
DVT excluded – no further
action
Positive
Continue subcutaneous
enoxaparin and refer to anticoagulation
clinic
* Positive D-dimer – due to the low specificity of D-dimer testing, consider the following: Recent trauma or surgery Pregnancy and puerperium Malignancy, especially metastatic disease Sepsis and inflammatory conditions Hepatic and renal disease Jaundice (T. Bili >50 and/or hyperlipidaemia The above should also be taken into consideration prior to ordering D-dimer tests. **Consult with pharmacy for dose adjustment if abnormal renal function
Consult with Haematologist if platelet count <100 x 109/L
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 19 of 25
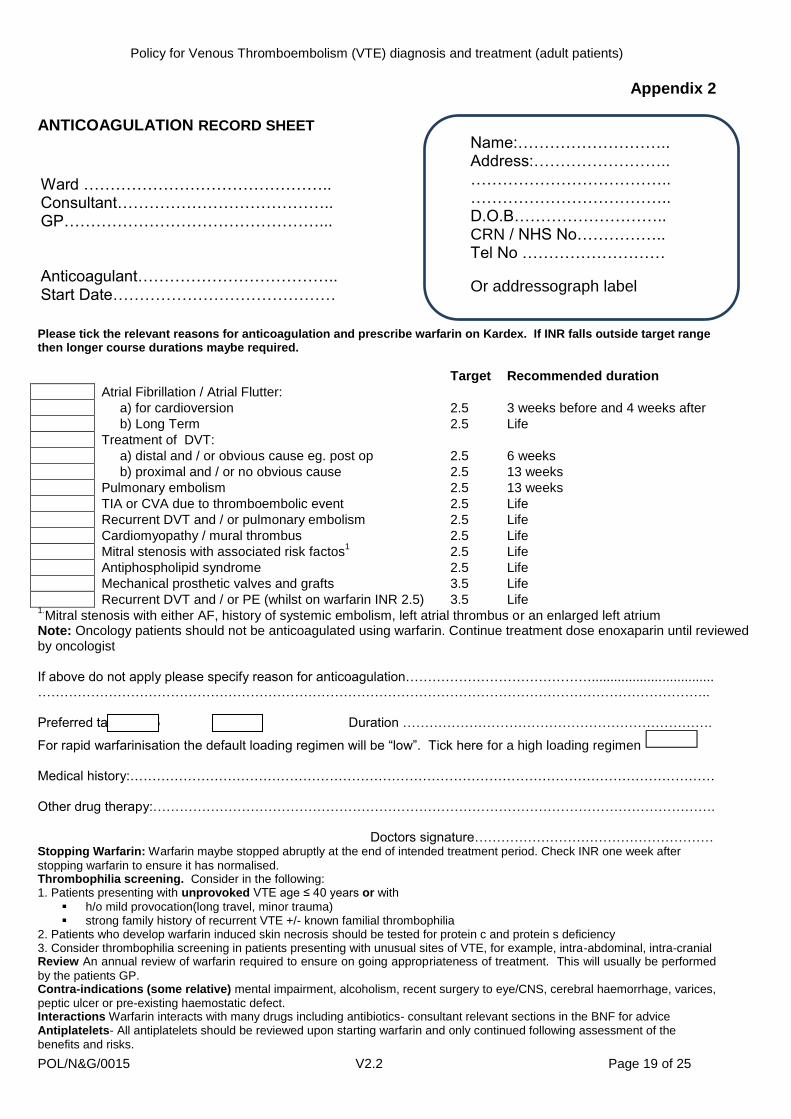
Appendix 2 ANTICOAGULATION RECORD SHEET Request for continuation of anticoagulant Please tick the relevant reasons for anticoagulation and prescribe warfarin on Kardex. If INR falls outside target range then longer course durations maybe required.
Target Recommended duration
Atrial Fibrillation / Atrial Flutter:
a) for cardioversion 2.5 3 weeks before and 4 weeks after
b) Long Term 2.5 Life
Treatment of DVT:
a) distal and / or obvious cause eg. post op 2.5 6 weeks
b) proximal and / or no obvious cause 2.5 13 weeks
Pulmonary embolism 2.5 13 weeks
TIA or CVA due to thromboembolic event 2.5 Life
Recurrent DVT and / or pulmonary embolism 2.5 Life
Cardiomyopathy / mural thrombus 2.5 Life
Mitral stenosis with associated risk factos1 2.5 Life
Antiphospholipid syndrome 2.5 Life
Mechanical prosthetic valves and grafts 3.5 Life
Recurrent DVT and / or PE (whilst on warfarin INR 2.5) 3.5 Life 1.Mitral stenosis with either AF, history of systemic embolism, left atrial thrombus or an enlarged left atrium
Note: Oncology patients should not be anticoagulated using warfarin. Continue treatment dose enoxaparin until reviewed by oncologist If above do not apply please specify reason for anticoagulation……………………………………................................. …………………………………………………………………………………………………………………………………….. Preferred target 2.5 3.5 Duration …………………………………………………………….
For rapid warfarinisation the default loading regimen will be ―low‖. Tick here for a high loading regimen Medical history:…………………………………………………………………………………………………………………… Other drug therapy:………………………………………………………………………………………………………………. Doctors signature……………………………………………… Stopping Warfarin: Warfarin maybe stopped abruptly at the end of intended treatment period. Check INR one week after
stopping warfarin to ensure it has normalised. Thrombophilia screening. Consider in the following: 1. Patients presenting with unprovoked VTE age ≤ 40 years or with
h/o mild provocation(long travel, minor trauma) strong family history of recurrent VTE +/- known familial thrombophilia
2. Patients who develop warfarin induced skin necrosis should be tested for protein c and protein s deficiency 3. Consider thrombophilia screening in patients presenting with unusual sites of VTE, for example, intra-abdominal, intra-cranial Review An annual review of warfarin required to ensure on going appropriateness of treatment. This will usually be performed
by the patients GP. Contra-indications (some relative) mental impairment, alcoholism, recent surgery to eye/CNS, cerebral haemorrhage, varices,
peptic ulcer or pre-existing haemostatic defect. Interactions Warfarin interacts with many drugs including antibiotics- consultant relevant sections in the BNF for advice Antiplatelets- All antiplatelets should be reviewed upon starting warfarin and only continued following assessment of the
benefits and risks.
Name:……………………….. Address:…………………….. ……………………………….. ……………………………….. D.O.B……………………….. CRN / NHS No…………….. Tel No ………………………
Or addressograph label
Ward ……………………………………….. Consultant………………………………….. GP…………………………………………... Anticoagulant……………………………….. Start Date……………………………………
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 20 of 25
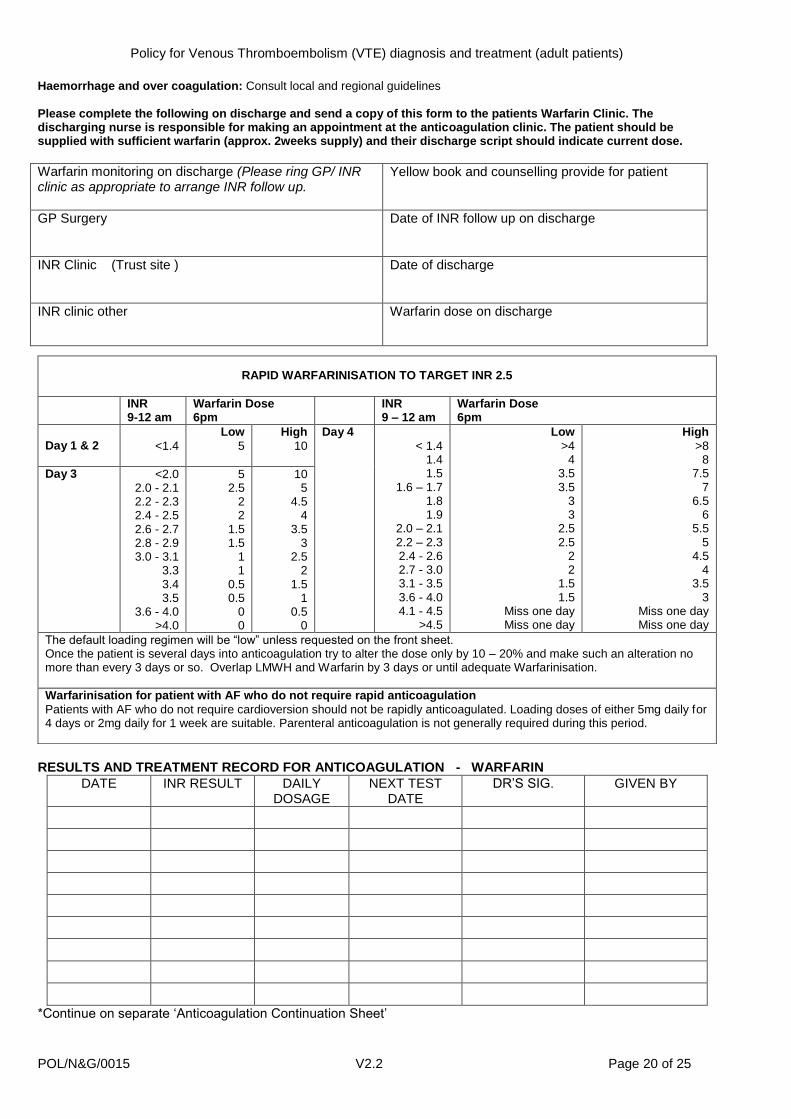
Haemorrhage and over coagulation: Consult local and regional guidelines Please complete the following on discharge and send a copy of this form to the patients Warfarin Clinic. The discharging nurse is responsible for making an appointment at the anticoagulation clinic. The patient should be supplied with sufficient warfarin (approx. 2weeks supply) and their discharge script should indicate current dose.
Warfarin monitoring on discharge (Please ring GP/ INR clinic as appropriate to arrange INR follow up.
Yellow book and counselling provide for patient
GP Surgery
Date of INR follow up on discharge
INR Clinic (Trust site )
Date of discharge
INR clinic other Warfarin dose on discharge
RESULTS AND TREATMENT RECORD FOR ANTICOAGULATION - WARFARIN
DATE INR RESULT DAILY DOSAGE
NEXT TEST DATE
DR‘S SIG. GIVEN BY
*Continue on separate ‗Anticoagulation Continuation Sheet‘
RAPID WARFARINISATION TO TARGET INR 2.5
INR 9-12 am
Warfarin Dose 6pm
INR 9 – 12 am
Warfarin Dose 6pm
Day 1 & 2
<1.4
Low
5
High
10
Day 4 < 1.4
1.4 1.5
1.6 – 1.7 1.8 1.9
2.0 – 2.1 2.2 – 2.3 2.4 - 2.6 2.7 - 3.0 3.1 - 3.5 3.6 - 4.0 4.1 - 4.5
>4.5
Low
>4 4
3.5 3.5
3 3
2.5 2.5
2 2
1.5 1.5
Miss one day Miss one day
High
>8 8
7.5 7
6.5 6
5.5 5
4.5 4
3.5 3
Miss one day Miss one day
Day 3 <2.0 2.0 - 2.1 2.2 - 2.3 2.4 - 2.5 2.6 - 2.7 2.8 - 2.9 3.0 - 3.1
3.3 3.4 3.5
3.6 - 4.0 >4.0
5 2.5
2 2
1.5 1.5
1 1
0.5 0.5
0 0
10 5
4.5 4
3.5 3
2.5 2
1.5 1
0.5 0
The default loading regimen will be ―low‖ unless requested on the front sheet. Once the patient is several days into anticoagulation try to alter the dose only by 10 – 20% and make such an alteration no more than every 3 days or so. Overlap LMWH and Warfarin by 3 days or until adequate Warfarinisation.
Warfarinisation for patient with AF who do not require rapid anticoagulation
Patients with AF who do not require cardioversion should not be rapidly anticoagulated. Loading doses of either 5mg daily for 4 days or 2mg daily for 1 week are suitable. Parenteral anticoagulation is not generally required during this period.
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 21 of 25
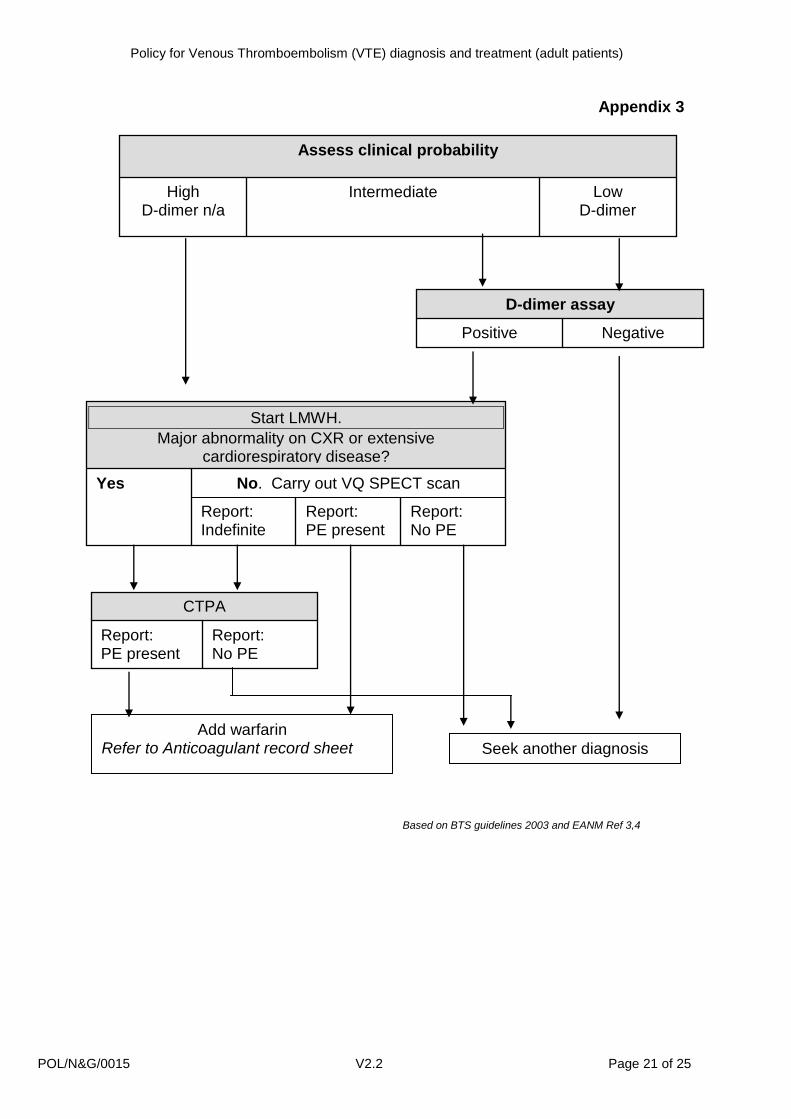
Appendix 3
Low D-dimer
Intermediate High D-dimer n/a
Assess clinical probability
Negative Positive
D-dimer assay
Report: No PE
Report: PE present
Report: Indefinite
No. Carry out VQ SPECT scan Yes
Start LMWH.
Major abnormality on CXR or extensive cardiorespiratory disease?
Report: No PE
Report: PE present
CTPA
Add warfarin Refer to Anticoagulant record sheet Seek another diagnosis
Based on BTS guidelines 2003 and EANM Ref 3,4
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 22 of 25
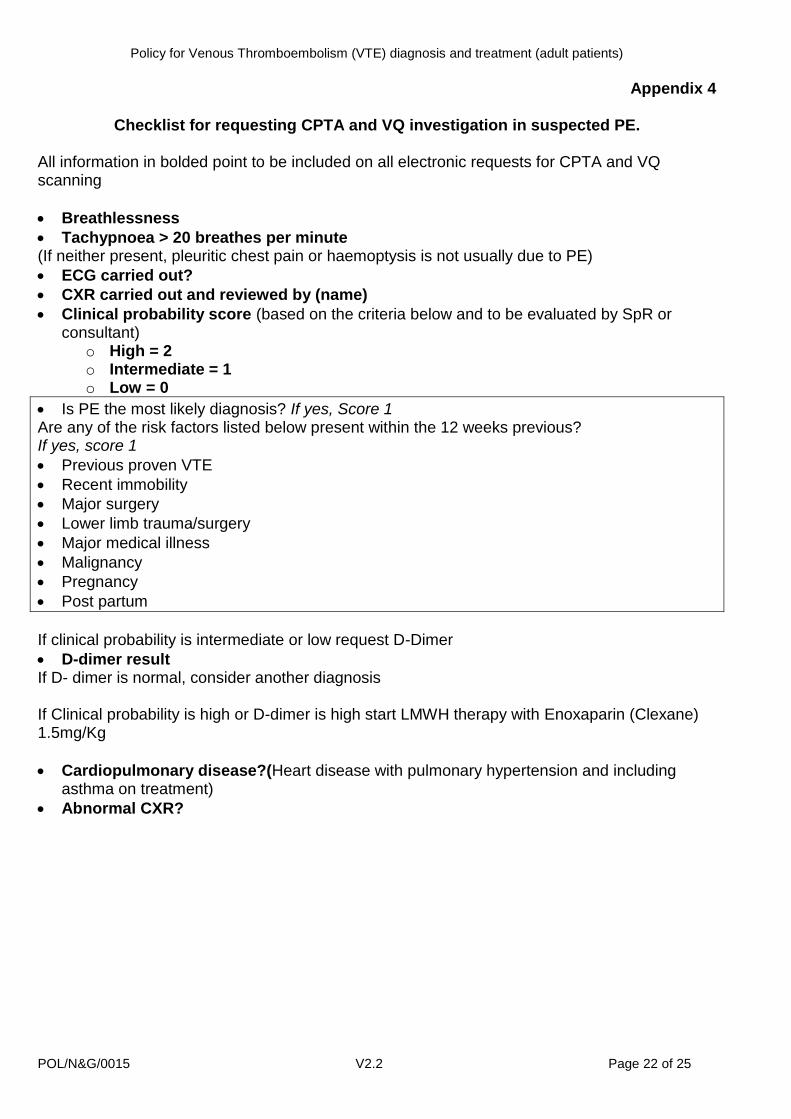
Appendix 4
Checklist for requesting CPTA and VQ investigation in suspected PE. All information in bolded point to be included on all electronic requests for CPTA and VQ scanning
Breathlessness
Tachypnoea > 20 breathes per minute (If neither present, pleuritic chest pain or haemoptysis is not usually due to PE)
ECG carried out?
CXR carried out and reviewed by (name)
Clinical probability score (based on the criteria below and to be evaluated by SpR or consultant)
o High = 2 o Intermediate = 1 o Low = 0
Is PE the most likely diagnosis? If yes, Score 1 Are any of the risk factors listed below present within the 12 weeks previous? If yes, score 1
Previous proven VTE
Recent immobility
Major surgery
Lower limb trauma/surgery
Major medical illness
Malignancy
Pregnancy
Post partum
If clinical probability is intermediate or low request D-Dimer
D-dimer result If D- dimer is normal, consider another diagnosis If Clinical probability is high or D-dimer is high start LMWH therapy with Enoxaparin (Clexane) 1.5mg/Kg
Cardiopulmonary disease?(Heart disease with pulmonary hypertension and including asthma on treatment)
Abnormal CXR?
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 23 of 25
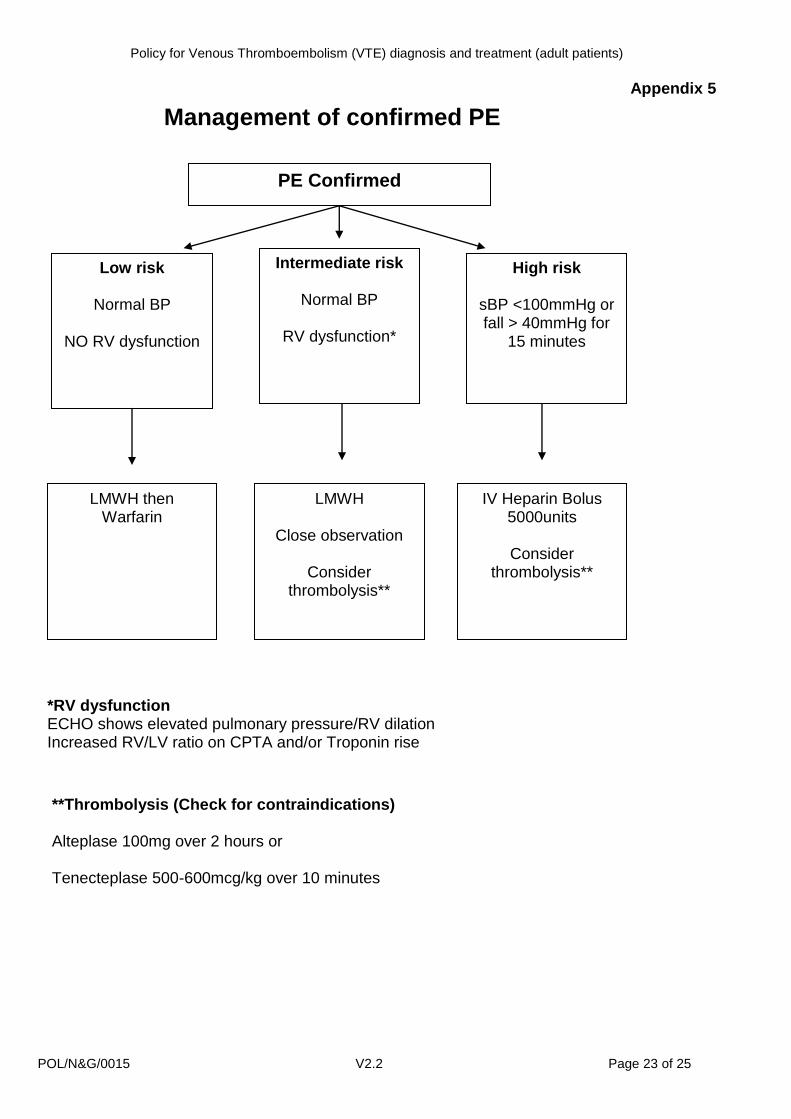
Appendix 5
Management of confirmed PE
PE Confirmed
Low risk
Normal BP
NO RV dysfunction
Intermediate risk
Normal BP
RV dysfunction*
High risk
sBP <100mmHg or fall > 40mmHg for
15 minutes
IV Heparin Bolus 5000units
Consider
thrombolysis**
LMWH
Close observation
Consider thrombolysis**
LMWH then Warfarin
*RV dysfunction ECHO shows elevated pulmonary pressure/RV dilation Increased RV/LV ratio on CPTA and/or Troponin rise
**Thrombolysis (Check for contraindications) Alteplase 100mg over 2 hours or Tenecteplase 500-600mcg/kg over 10 minutes
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 24 of 25
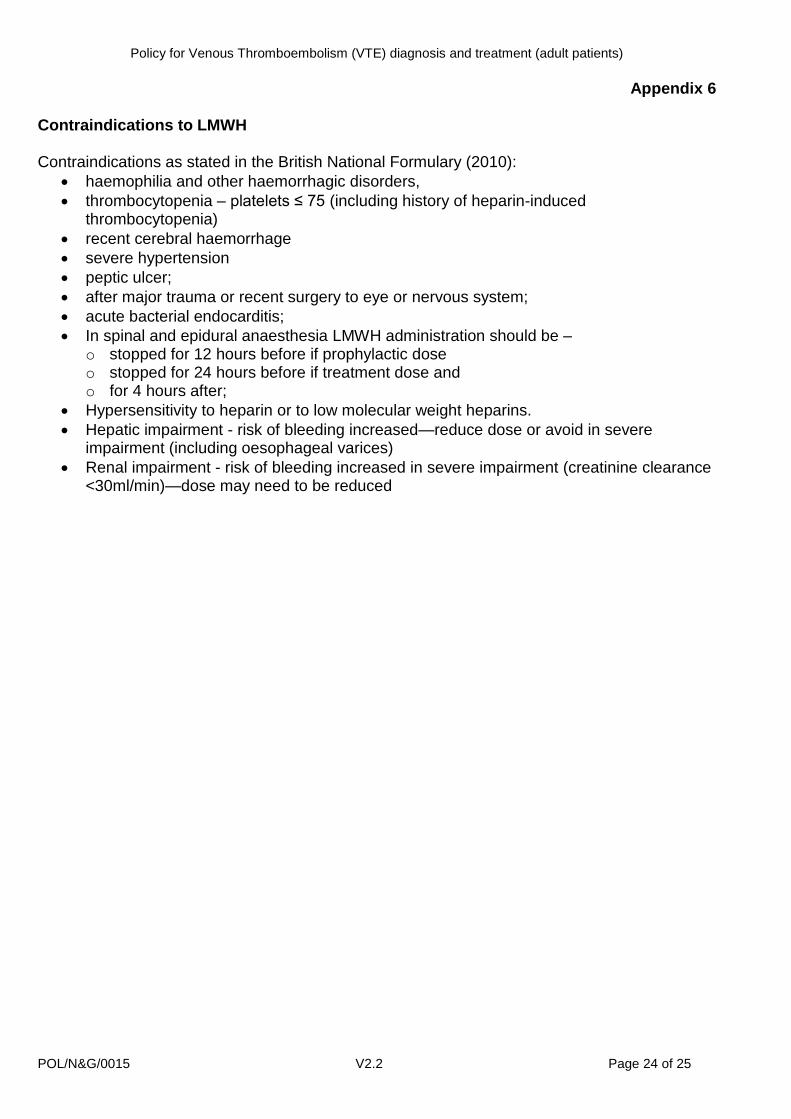
Appendix 6
Contraindications to LMWH Contraindications as stated in the British National Formulary (2010):
haemophilia and other haemorrhagic disorders,
thrombocytopenia – platelets ≤ 75 (including history of heparin-induced thrombocytopenia)
recent cerebral haemorrhage
severe hypertension
peptic ulcer;
after major trauma or recent surgery to eye or nervous system;
acute bacterial endocarditis;
In spinal and epidural anaesthesia LMWH administration should be – o stopped for 12 hours before if prophylactic dose o stopped for 24 hours before if treatment dose and o for 4 hours after;
Hypersensitivity to heparin or to low molecular weight heparins.
Hepatic impairment - risk of bleeding increased—reduce dose or avoid in severe impairment (including oesophageal varices)
Renal impairment - risk of bleeding increased in severe impairment (creatinine clearance <30ml/min)—dose may need to be reduced
Appendix 1
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 25 of 25
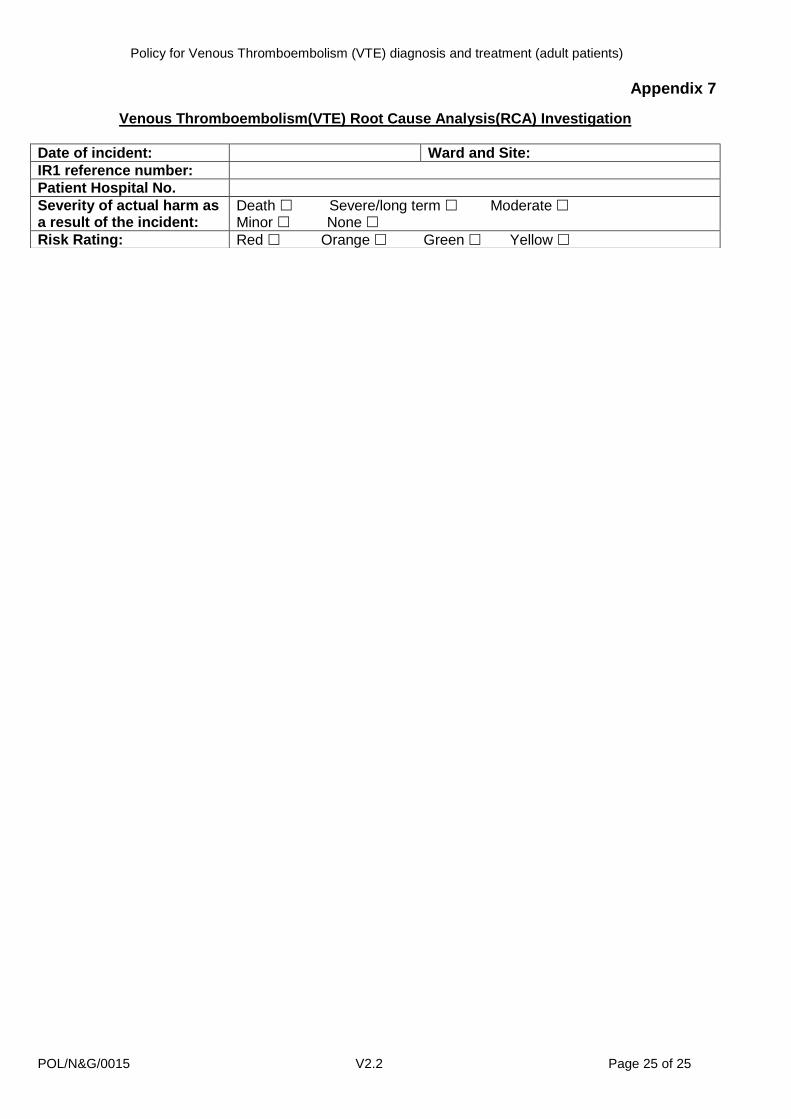
Appendix 7
Venous Thromboembolism(VTE) Root Cause Analysis(RCA) Investigation
Date of incident: Ward and Site:
IR1 reference number:
Patient Hospital No.
Severity of actual harm as a result of the incident:
Death Severe/long term Moderate Minor None
Risk Rating: Red Orange Green Yellow
Policy for Venous Thromboembolism (VTE) diagnosis and treatment (adult patients)
POL/N&G/0015 V2.2 Page 26 of 25
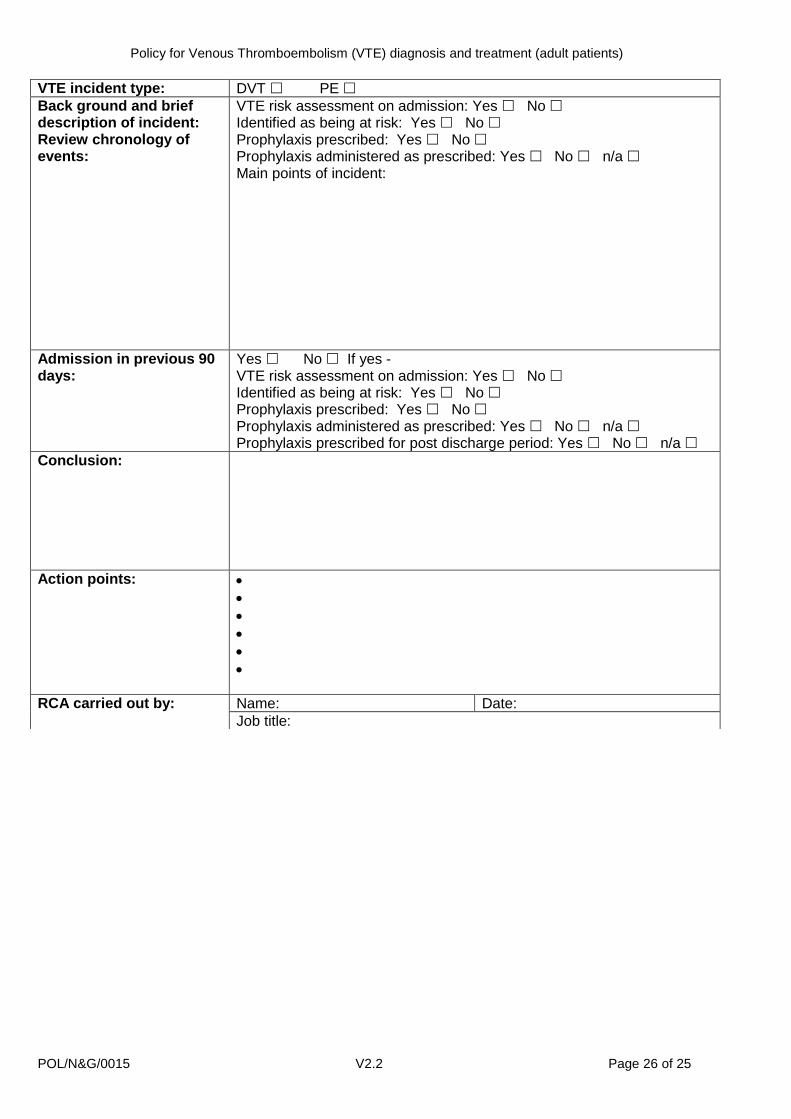
VTE incident type: DVT PE
Back ground and brief description of incident: Review chronology of events:
VTE risk assessment on admission: Yes No Identified as being at risk: Yes No Prophylaxis prescribed: Yes No Prophylaxis administered as prescribed: Yes No n/a Main points of incident:
Admission in previous 90 days:
Yes No If yes - VTE risk assessment on admission: Yes No Identified as being at risk: Yes No Prophylaxis prescribed: Yes No Prophylaxis administered as prescribed: Yes No n/a Prophylaxis prescribed for post discharge period: Yes No n/a
Conclusion:
Action points:
RCA carried out by: Name: Date:
Job title:





![Cellulitis in Adults - WRHN in Adults.pdf• cellulitis is an acute bacterial infection of the dermis and subcutaneous tissue [1]: • Erysipelas is a form of cellulitis caused by](https://img.pdfslide.us/doc/110x75/5e37a2a00fa2bc6b5a461882/cellulitis-in-adults-in-adultspdf-a-cellulitis-is-an-acute-bacterial-infection.jpg)