Embed Size (px)
Citation preview

Vol. 4, 1521-1526, Ju,u’ 1998 Clinical Cancer Research 1521
CD28, a Marker Associated with Tumoral Expansion in
Multiple Myeloma’
Nelly Robillard,2 Ga#{235}tan Jego,2
Catherine Pellat-Deceunynck, Danielle Pineau,
Denis Puthier, Marie-Paule Mellerin,
Sophie Barill#{233}, Marie-Jos#{233} Rapp,
Jean-Luc Harousseau, Martine Amiot, and
Regis Bataille3
Laboratoire d’H#{233}matologie (N. R.. D. P.. M-P. M.. R. B.l.
Oncogenese Immunoh#{233}matologique. Institut National de Ia Sante et
de Ia Recherche M#{233}dicale Unite 463 1G. J.. C. P-D.. D. P.. S. B..
M. A., R. B.]. and Departement dHematologie Clinique [M-J. R.,J-L. H.]. Institut de Biologic. 44 093 Nantes Cedex 01. France
ABSTRACT
CD28 expression was thoroughly investigated on
plasma cells of monocbonal gammopathy of undetermined
significance, multiple myeloma (MM), and human myeloma
cell lines. CD28� plasma cells were detected in 19% of 31
monoclonal gammopathy of undetermined significance,
41 % of I 16 MM, and 100% of 13 human myeloma cell lines.CD28� myeloma cells were detected in 21 of 79 (26%) MM
cases at diagnosis, 13 of 22 (59%) at medullary relapse (P <
0.009), and 14 of 15 (93%) at extramedullary relapse (P
0.05), including 10 of 10 (100%) secondary plasma cell
leukemias (P = 0.05). Serial studies in individual patients
confirmed the emergence of CD28� myeloma cells with
tumoral expansion and treatment failure. This was signifi-
cantly correlated with the expression of CD28 ligand, i.e.,
CD86 (but not CD8O), and with an increase in the prolifer-ative activity (labeling index) of myeloma cells in bone mar-
row. Whereas the expression of CD56 defines a particular
subset of myeloma patients, CD28 is the only antigen for
which expression correlates with tumor progression. Our
data show that an aggressive compartment of CD28” and
CD86� myeloma cells emerges during the course of MM in
vivo, indicating that CD28 could be aberrantly expressed on
highly malignant (possibly mutated) myeloma cells. Con-
versely, a subset of proliferative plasmablasts coexpressing
CD28 and CD86 could be the normal counterpart of the
Received I 2/2/97: revised 3/16/98: accepted 3/23/98.
The costs of publication of this article were defrayed in part by the
payment of page charges. This article must therefore be hereby marked
advertise,nent in accordance with 18 U.S.C. Section 1734 solely to
indicate this fact.
I This work was supported by the Programme Hospitalier de Recherche
Clinique and by La Ligue contre Ic Cancer des Deux S#{232}vres(to G. J.).
2 The first two authors contributed equally to this work.
3 To whom requests for reprints should be addressed. at Laboratoired’H#{233}matologie. Institut de Biologic. 9 Quai Moncousu. 44 093
Nantes Cedex 01. France. Phone: 33 (0)2-40-08-40-49: Fax: 33 (0)2-
40-08-41-14.
clonogenic myeloma stem cell because a subset of CD28�
plasma cells was observed in 6 of 6 cases of reactive plas-
mocytosis.
INTRODUCTION
CD28, a well-documented antigen expressed on human T
lymphocytes. plays an essential role in T-cell activation and
1-cell-B-cell interactions through its specific ligands, especially
CD86 (reviewed in Refs. 1-4). It is now well established that
signaling through the 1-cell receptor is necessary but not suffi-
cient to induce antigen-specific 1-cell activation and cytokine
secretion. A costimulatory signal involving the 1-cell surface
molecule CD28 and its ligands is essential for 1-cell clonal
expansion. lymphokine secretion, and effector function. If this
costimulatory signal is not delivered, I cells enter a state of
long-term unresponsiveness to specific antigen (referred to as
anergy; Refs. 1-4). In 1989, Kozbor et a!. (5) reported the
expression of CD28 on seven of seven HMCLs4 but not on
resting B cells from peripheral blood or lymphoid organs, lym-
phoblastoid cell lines. or any other B-cell tumors. In 1990. Lee
et a!. (6) confirmed the expression of CD28 gene by malignant
plasma cells from RPMI 8226 HMCL as a series of four distinct
CD28 mRNA species: I .3-, 1 .5-, 3.5-, and 3.7-kb transcripts that
were identical to those of I lymphocytes. More recently. we
used flow cytometry and double immunofluorescence to rein-
vestigate the expression of CD28 on normal and malignant
plasma cells and HMCLs (7-9) and found that normal plasma
cells from tonsils and bone marrow did not express CD28 (7).
However, this work showed for the first time that CD28 is
expressed on fresh human myeboma cells from some but not all
patients with MM (7). Finally. all HMCLs. unlike nonmalignant
EBV� lymphoblastoid cell lines, express CD28 (7-9). A major
issue is to clarify the clinical significance of this antigen on
human myeloma cells because our initial study showed a po-
tential correlation between CD28 expression and disease sever-
ity (7). This study, which evaluated CD28 expression in a large
number of patients with either benign or malignant plasma cell
disorders, clearly shows that this antigen is a marker associated
with disease progression and treatment failure.
MATERIALS AND METHODS
Patients. The expression of CD28 on plasma cells was
investigated in 31 individuals with MGUS and 1 16 patients with
MM. without (ti 106) or with (ii = 10) a significant leukemic
phase (secondary PCL). For these latter MM patients, the phe-
notype of myeloma cells was determined on bone marrow
4 The abbreviations used are: HMCL, human myeloma cell line: MM.
multiple myeloma: MGUS, monoclonal gammopathy of undetermined
significance; PCL. plasma cell leukemia: mAb, monocbonal antibody:
PE. phycoerythrin: Ab. antibody: BrdUrd. bromodeoxyuridine.
Research. on August 4, 2021. © 1998 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

1522 CD28 Expression on Human Myeloma Cells
myeboma cells or both bone marrow and peripheral blood my-
eboma cells. Low- or high-risk MGUS was classified according
to our previously reported criteria (10). The diagnostic criteria
for MM were those of the Southwest Oncology Group (1 1).
Seventy-nine MM patients (with or without a leukemie phase)
were studied at diagnosis, 22 at medullary relapse, and 15 at
extramedullary relapse (10 secondary PCLs, 3 pleural effusions,
I skin and 1 ascitis) and treatment failure. Six patients with
peripheral blood reactive plasmocytosis during the course of
viral infections (n 4) or B- and 1-cell lymphomas (n 2)
were included. In these patients, peripheral blood plasma cells
were processed as myeloma cells.
HMCLs. The XGs and SBN1 HMCL were established
by ourselves (8, 12). U266 and RPMI 8226 were purchased
from American Type Culture Collection (Manassas, VA), and
OPM2, LP1 , L363, and NCI H929 were from DSM (Germany).
ANBL6 was a generous gift from D. Jelinek (Mayo Clinic,
Rochester, MN).
mAbs. mAbs against the following antigens were used:
Apo 2.7, CD19, CD28, CD38, CD45, CD56, CD8O, CD86, and
CDI38 (i.e., syndeean-l). Apo 2.7-PE, anti-CD]9-PE, anti-
CD28-FITC, anti-CD38-FITC, anti-CD45FITC, control IgG 1-
FITC, and control IgGi-PE were obtained from Immunotech
(Marseilles, France); anti-CD28-PE, anti-CD56-PE, and anti-
CD8O-PE were from Beeton Dickinson (Heidelberg, Germany);
anti-CD86-PE was from Pharmingen (San Diego, CA); rabbit
antihuman K light ehain-PE Ab was from DAKO (Gbostrup,
Denmark); and mouse antihuman X light ehain-PE was from
Caltag laboratories (San Francisco, CA). B-B4 anti-CD138 mAb
was a gift from Dr. J. Wijdenes, Diacbone Research (Besan#{231}on,
France). B-B4 mAb (CD138) is specific for normal and malig-
nant plasma cells in bone marrow and peripheral blood and
recognizes syndeean-l (7, 13). Purified B-B,, mAb was biotiny-
lated as described previously (7).
Phenotypic Analysis. For immunofluorescence staining,
5 x l0� cells were incubated with different FIIC- or PE-
conjugated or biotinylated mAbs for 30 mm at 4#{176}Cin the
presence of 20% human AB serum, followed by incubation (20
mm at 20#{176}C)with streptavidin coupled to Quantum Red (Sigma
Chemical Co., St. Louis, MO). Cells were fixed in 1% formal-
dehyde and analyzed on a FACSealibur flow cytometer with
Cell Quest Software (Becton Dickinson). Data acquisition was
always performed in two steps: first, 10,000 total cells were
collected; and second, at least 5,000 plasma cells (CDl38�)
were acquired with an activated live gate on SSC versus CD 138
dot plot. Apoptotie plasma cells were recognized by low ex-
pression of CD138 and Apo 2.7 staining and excluded from
analysis.
CDI38 plasma cell identification was controlled by coex-
pression of CD138, CD38, and intracytoplasmie K/X immuno-
fluorescence in a three-color assay. Briefly, cells were first
surface-stained with CD138-biotin-streptavidin-Quantum Red
and CD38-PE as described above, fixed, and permeabilized
overnight in PBS with 1% paraformaldehyde and 0.01% Tween
20. For intracytoplasmie �ciX staining, permeabilized cells were
washed and incubated for 30 mm at 20#{176}Cwith PE-conjugated
Abs in PBS with 0.5% Tween 20. Cells were washed, and at
least 5000 plasma cells (K- or X-positive cells) were collected.
Careful analysis of the three-color staining revealed that >98%
Table 1 Expres sion of CD28, CD8O, and CD 86 by HMCLs
HMCLs CD28 CD8O CD86
U266 + - -
RPMI 8226 + - -
L363 + - + (weak)
ANBL-6 + - + (weak)
NCI-H929 + .- -
LPI + - -
OPM2 + - -
SBNI + - -
XGI + - + (weak)
XG2 + - + (weak)
XG5 + - -
XG6 + - -
XG7 + - -
of either K- or X-positive cells coexpressed CD138 and bright
CD38.
Labeling Index of Myeloma Cells. The labeling index
of myeboma cells was measured according to a modification of
Carayon and Bord (14) using anti-BrdUrd mAb (BUS-]; Cym-
bus Bioscience, Euromedex, Souffelweyersheim, France) and
analyzed by flow cytometry. The percentage of myeloma cells
in S phase was determined by the number of positive cells for
BrdUrd staining within the viable population of intracytoplas-
mie K-/X-positive plasma cells. Briefly, ]06 cells were incubated
with or without (control) 50 p.M BrdUrd for 2 h at 37#{176}Cin 5%
CO2 incubator, washed, and permeabilized overnight in PBS
containing I % paraformaldehyde and 0.01 % Tween 20 at 4#{176}C.
After two washes, cells were incubated for 30 mm at 37#{176}Cwith
50 Kunitz units of DNase I (Sigma). After DNase digestion,
cells were washed in 0.5% Tween 20 PBS and labeled using
PE-coupled anti-light chain Abs for 30 mm at room temperature.
Following two washes, both control cells and the incorporated
BrdUrd cells were stained with 10 p.1 of FITC-BU5-l mAb in
PBS supplemented with 0.5% Tween 20 and 20% AB serum for
45 mm at room temperature. After two washes, the cells were
resuspended in PBS and analyzed immediately on a FACSea1i-
bur flow cytometer. For this purpose, data acquisition was
performed on 50,000 cells and then on 10,000 live gated K-/X-
positive cells when the plasmacytosis represented <20% of
cells.
Statistical Analyses. The Wileoxon rank sum test, the x2test (with Yates correction, if necessary), and the Fisher exact
test were used for statistical studies.
RESULTS
CD28 Is Expressed on All HMCLs. CD28 gene was
expressed on all 13 HMCLs tested (Table 1) as a series of four
distinct transcripts that were identical to those of I lymphocytes
(data not shown). Although CD8O, a CD28 ligand, was not
expressed on HMCLs, a weak but significant expression of
CD86, another CD28 ligand, was found on 4 of 13 (30%)
HMCLs (Table 1).
CD28 Myeboma Cells Emerge during Tumoral Expan-
sion in Patients with MM. To investigate the clinical and
biological significance of CD28 expression in fresh human
myeloma cells, we used the largest pool of patients with plasma
Research. on August 4, 2021. © 1998 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

MGUS MM
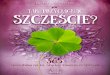
Fig. I Changes in CD28 expres-
sion on myeloma cells according
to disease activity in patients with
MM: comparison with MGUSand human myeloma cell lines.
1 00’
90
80
70
% 60
50
40
30
20
10
0
MGUS Diagnosis Medullary Extramed Cell linesrelapse relapse
Clinical Cancer Research 1523
cell disorders ever studied. CD28 was clearly expressed on
freshly explanted malignant plasma cells in 41 % of patients with
MM. The median percentage of CD28� myeboma cells per
patient was 100% (range = 10-100%). Few patients with
<10% of CD28� myeboma cells were classified as CD28
MM. A more detailed analysis ofCD28 expression on malignant
plasma cells showed a clear correlation with disease progres-
sion. As indicated in Fig. I, CD28� myeboma cells were only
found in 26% of previously untreated patients with MM but in
72% of relapsing patients (P < 0.0001). When relapses were
investigated more carefully, CD28� myeboma cells were found
in 59% of medublary relapses but in 93% of extramedullary
relapses (P = 0.05). For the extramedullary relapses, 10 samples
came from MM patients in leukemie phase (i.e. , secondary
PCL), and 5 came from ascitis, skin lesions, or pleural effusions.
In the former cases, CD28 expression was found in 10 of 10
cases. Of note, in two of these secondary PCLs, CD28 was
expressed on peripheral blood myeboma cells but not on bone
marrow myeboma cells. In the batter eases, CD28 expression was
found in four of five samples. Thus, tumoral expansion was
clearly associated with a growing CD28� myeloma cell com-
partment. It is noteworthy that CD28 expression was observed
in >90% of extramedullaiy tumors, which are usually associ-
ated with treatment failure. Serial evaluations of CD28 were
performed in three patients to clearly show that CD28 expres-
sion emerged during tumoral expansion in individual patients. In
all three eases, medullary relapse was associated with the ap-
pearanee of CD28. In one of these cases, CD28 evaluation was
performed at diagnosis, medublary relapse, and extramedullary
relapse (i.e., secondary PCL). As indicated in Fig. 2, an expand-
ing CD28� myeboma cell compartment was detected in eon-
junction with tumor progression (0, 53, and 94%, respectively,
for the three evaluation times). Interestingly, CD28� plasma
cells were found in 19% of individuals with MGUS. The subset
of CD28� MGUS was too small (ii = 6 of 31) to allow any
conclusions to be drawn. However, the follow-up of these
individuals, as compared to patients with CD28 MGUS, will
MMCell lines
be of particular interest in terms of malignant conversion into
overt MM.
CD28 Myeloma Cells Also Emerge in the Special Subset
of MM Lacking CD56. CD19 and CD56 antigens were thor-
oughly investigated in conjunction with CD28. We and others
have previously reported that malignant plasma cells lack CD19
but overexpress CD56, as compared to normal plasma cells (7.
15-17). As expected, most patients included in the current study
did not express CD19 (98.8% ofeases) but overexpressed CD56
(83% at diagnosis). Interestingly. as previously pointed out by
Kawano and colleagues ( 17), no patient (of 1 16 total patients)
presented the phenotype of normal plasma cells (CDl9�,
CD56). Of note, CD56 was completely lost in malignant
plasma cells of patients with secondary PCL, both in bone
marrow and peripheral blood (ii = 10). To determine whether
this could have been due to late down-regulation of the antigen
in secondary PCL, we reinvestigated CD56 expression in the
original samples at diagnosis from four CD56 secondary
PCLs. In three of these four eases, CD56 was partially or totally
lacking on bone marrow plasma cells at diagnosis. Thus, in
contrast to CD28, CD56 did not correlate with disease progres-
sion but designated a specific subset of myeboma patients de-
tectable at diagnosis. Interestingly, CD28 was more frequently
observed at diagnosis in CD56 (57% of cases) than CD56�
patients (17%, P = 0.002; Table 2). Furthermore, as indicated in
Table 2, CD28 expression increased significantly with disease
progression in both CD56 subsets of patients.
CD28 Expression Correlates. The importance of Ii-
gands in the biology of CD28 led us to investigate the expres-
sion of CD8O and CD86 on fresh human myeboma cells. CD8O
was not found in 20 consecutive patients with MM, regardless of
disease activity, whereas significant CD86 expression was ob-
served in 17 of 25 (68%) consecutive patients with MM. Inter-
estingly, a significant association was found between CD28 and
CD86 expression: all CD28� MM patients (n = 10) expressed
CD86 but only 46% of CD28 patients expressed CD86 (7 of
15: P = 0.018: Fig. 3A).
Research. on August 4, 2021. © 1998 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Diagnosis Medullary Extra-Relapse medullary
Relapse
C.)
�:E;::�!�I i�!
�-�;---1)#{176} 10
�. -
C.)
� ‘�
10 10 10 10 10
aC.)
1111 �llIu 1�
� -
C’)
1o� � 1I� 1110 �Jl I;2 �3 �
CD38
C’)�.
c’J�.
�.
0%C,)
�!__
Tho#{176} ;‘�;i �‘�2 � 4
-�.
94%C.)
Q’
C�
�100. � ‘�‘T�2 ;‘�;�� �4
CD28
1524 CD28 Expression on Human Myeloma Cells
5 G. Jego et al. , manuscript in preparation.
Fig. 2 Serial analysis of
CD28 cells in the CD138’
plasma cell population in a pa-
tient with MM at diagnosis,
medullary relapse, and ex-tramedullary relapse (second-
ary leukemic phase).
Given the significant association of a detectable compart-
ment of CD28� myeloma cells with disease progression, we
searched for a correlation between the presence of this compart-
ment and tumor kinetics in the bone marrow of newly diagnosed
patients with MM. It was particularly noteworthy that the me-
dian labeling index of myeloma cells was 4% (range = 0.6-
4.5%) in 7 CD28� patients but only 1.1% (range = 0-4.5%) in
16 CD28 patients (P = 0.02; Fig. 3B). These data indicate that
CD28� MM were more proliferative (and thus more aggressive)
than CD28 MM at diagnosis.
CD28 Is Detected on Reactive Plasma Cells. We pre-
viously found that nonproliferative and highly differentiated
plasma cells within bone marrow did not express CD28 (7). In
view of our current results in MM, it seemed to be of interest to
investigate CD28 expression on reactive plasma cells, which are
highly proliferative but less differentiated (l8).� Six eases of
reactive plasmocytosis were studied using the same method-
ological approach, and the median percentage of reactive poly-
clonal plasma cells in peripheral blood was found to be 9%
(range - 4-70%). In all eases, the phenotype was normal:
CDl38��, CD38���, K�/X�, CD19�, CD1 la�, and CD56.
A significant population of CD28� plasma cells was found in all
eases (range = 1-12%, median = 6%).
DISCUSSION
CD28, a well-documented antigen expressed on human 1
lymphocytes, plays an essential role in 1-cell activation and
1-cell-B-cell interactions through its specific ligands: B7-l , i.e.,
CD8O; and B7-2, i.e., CD86 (]-4). In 1989, Kozbor et a!. (5)
reported the expression of CD28 on 7 of 7 HMCLs, an obser-
vation confirmed by us and others (7-9, 19). Thus, it is clear that
CD28 is a universal marker expressed on 100% of HMCLs but
not on other cells of the B-cell lineage, including EBV� B-cell
lines. At the transcriptional level, its expression on HMCLs is
identical to that of I cells. Although all HMCLs express CD28,
none express CD8O, and only 30% express CD86 weakly,
Research. on August 4, 2021. © 1998 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Bp=0.02 p=0.02
Fig. 3 CD28 expression correlates.A, expression of CD86 on plasma
cells (CD138�) according to CD28expression. B, labeling index of
plasma cells was defined as described
in “Materials and Methods.” Median
values are indicated in the figure (-).
0
(I)U)U)
a.
U)
CDCD0C.)
A
1 00
5 0 ______\ \ \ ‘ \
%‘ ,‘ S “ S
5’’’’’
S S S S S
0� - _____
1� � � 1’ �
‘‘‘5’
‘‘‘‘/,
‘‘‘5’
‘5’’’
‘‘5’’
‘‘‘‘5
‘‘‘‘/,‘‘‘5’
‘‘‘‘5
‘‘5’’
‘5’’’
‘‘5’’
5.
�4.
‘Ca)
�0C
a)
.E 2a)
U)
-I
0
41’ 41’
4�.
41’41’
41’
I --I-- I
CD28 CD28� CD28 CD28�
(n=15) (n=10) (n=16) (n=7)
Clinical Cancer Research 1525
6 Manuscript in preparation.
T able 2 Expression of C D28 in both CD56� and CD56 subsets of MM
Disease status CD56� subset CD56 subset
Diagnosis
Medullary relapse
Il7%(10/56) �
I56% (9/16) J
P = 0.002
P=0.006
I57%(12/2l)
100% (5/5) P = 0.01
Extramedullary relapse
Extramedullary sites 75% (3/4) 100% (1/1)
Secondary PCL No patient 100% (10/10)
whereas EBV� B-cell lines strongly express both CD8O and
CD86.
More recently, we have found that (a) malignant plasma
cells from some patients with MM express CD28, as do those of
HMCLs (7), and that (b) normal well-differentiated and non-
proliferative plasma cells (in bone marrow) do not express
CD28 (7). Here, we carried out a more thorough assessment of
this “1-cell antigen” on freshly explanted malignant plasma
cells. Our current data clearly show that CD28 appears during
disease progression. A continual increase in the percentages of
MM patients expressing CD28 was found between the initial
and terminal phases of the disease and at treatment failure, when
almost all patients expressed CD28. This pattern was also ob-
served in the important subset of MM lacking CD56 and is
currently being investigated.6 Serial studies have clearly con-
firmed this concept in individual patients. The concept that
CD28 expression is associated with tumoral expansion is also
supported by the fact that the labeling index of newly diagnosed
patients with CD28� MM was 4 times greater than that of
CD28 MM. This point strongly supports the concept that
CD28� MM is more aggressive (because it is more prolifera-
tive) than other forms. From a practical point of view, CD28
expression could be of prognostic value in MM and also in
MGUS because CD28 was found to be expressed in some
patients with these presenting features. Further investigation is
needed to clarify these points. Basically, these in vivo data
suggest that CD28 expression on malignant plasma cells could
reflect intrinsic cell malignancy (in terms of oncogenic events
accumulated in a clone) with higher proliferative capacity. It is
of interest to emphasize that HMCLs generally emerge from
samples obtained during extramedullary relapse or from the
peripheral blood of secondary PCL, for which 100% of samples
and cells express CD28 as HMCLs, with frequent Ras and p53
point mutations (20, 21). Further investigation will be necessary
to clarify the mechanisms leading to the up-regulation of CD28
on these tumors. It would appear that these observations are not
consistent with our finding of CD28 expression in 6 of 6 cases
of reactive plasmocytosis in which plasma cells were not ma-
lignant. However, these cases of reactive plasmocytosis were
highly proliferative.5 Thus, the intrinsic malignancy of myeloma
cells related to the occurrence of Ras and/or p53 mutations
(Refs. 20 and 2 1 ; or other unknown oncogenic mutations) dur-
ing disease progression could make them proliferative enough to
express CD28. Another possibility is that a normal but prolif-
Research. on August 4, 2021. © 1998 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

1526 CD28 Expression on Human Myeloma Cells
erative CD28� plasmablast could be the normal counterpart of
the myeboma stem cell, although it is undetectable in most
patients at diagnosis. It is noteworthy that our observation of
CD28 on reactive plasma cells provides the first evidence of
CD28 expression on the normal B-cell lineage in vivo, a finding
that requires further investigation. Although the expression of
CD28 is clearly associated with tumoral expansion, there is no
clear function for this antigen, not only on myeloma cells but
also on normal (reactive) plasma cells. However, activation of
this antigen through its CD86 ligand (although weakly ex-
pressed) could facilitate myeloma cell survival by up-regulation
of antiapoptotic molecules such as Bel-XL, as described for I
lymphocytes (22, 23). In this context, it is noteworthy that
chemoresistance in MM, which is associated with overexpres-
sion of CD28 (this data), is also related to overexpression of
Bcl-XL (24). Thus, further investigation is needed to delineate
the role of CD28 on reactive plasma cells and human myeboma
cells.
ACKNOWLEDGMENTS
We thank C. Ville for typing this manuscript and M. Etrillard for
technical assistance.
REFERENCES
I . Linsley, P. S., and Ledbetter, J. A. The role of the CD28 receptor
during cell responses to antigen. Annu. Rev. Immunol., 11: 191-212,
1993.
2. Rudd, C. E., Janssen, 0., Cai, Y. C., Da Silva, A. J., Raab, M., andPrasad, K. V. S. Two-step TCR CD3-CD4. and CD28 signaling in T
cells. SH2/SH3 domains, protein tyrosine and lipid kinases. Immunol.
Today. 15: 225-234, 1994.
3. June, C. H., Bluestone, J. A., Nadler, L. M., and Thompson, C.B.
The B7 and CD28 receptor families. Immunol. Today, 15: 321-337,
1994.
4. Guinan, E. C., Gribben, J. G., Boussiotis, V. A., Freeman, G. J., and
Nadler, L. M. Pivotal role of the B7:CD28 pathway in transplantation
tolerance and tumor immunity. Blood, 84: 3261-3282, 1994.
5. Kozbor, D., Moretta, A., Messner, H. A., Moretta, L.. and Croce,
C. M. Tp44 molecules involved in antigen-independent T cell activation
are expressed on human plasma cells. J. lmmunol., 138: 4128-4132,
1987.
6. Lee. K. P., Taylor, C., Petryniak. B.. Turka, L. A., June, C. H., and
Thompson, C. B. The genomic organization of the CD28 gene: impli-
cations for the regulation of CD28 mRNA expression and heterogeneity.
J. Immunol., 145: 344-352, 1989.
7. Pellat-Deceunynck, C., Bataille, R., Robillard, N, Harousseau, J. L.,Rapp, M. J., Juge-Morineau. N., Wijdenes. J.. and Amiot, M. Expressionof CD28 and CD4O in human myeloma cells: a comparative study with
normal plasma cells. Blood, 84: 2597-2603, 1994.
8. Zhang, X. G., Gaiblard, J. P., Robillard, N., Lu, Z. Y., Gu, Z. J.,
Jourdan, M., Boiron, J. M., Bataille, R., and Klein, B. Reproducible
obtaining of human myeboma cell lines as a model for tumor stem cell
study in human multiple myeloma. Blood, 83: 3654-3663, 1994.
9. Pellat-Deceunynek, C.. Amiot, M., Bataille, R., Van Riet, Y., VanCamp, B., Omede. P., and Boceadoro, M. Human myeboma cell lines as
a tool for studying the biology of multiple myeboma: a reappraisal 18
years after. Blood. 86: 4001-4002, 1995.
10. Bataille, R., Chappard, D., and Basle, M. F. Quantifiable excess of
bone resorption in monoebonab gammopathy is an early symptom of
malignancy: a prospective study of 87 bone biopsies. Blood, 87: 4762-
4769. 1996.
I I. Durie, B. G. M., and Salmon, S. E. Multiple myeboma, macrogbobu-
linaemia and monoclonal gammopathies. In: A. V. Hoffbrand, M. C.Brain, and J. Hish (eds.), Recent Advances in Haematobogy, pp. 243-
261. 1977.
12. Barill#{233},S., Akhoundi, C.. Colette, M., Mellerin. M. P., Rapp, M. J.,
Harousseau, J. L., Bataille, R., and Amiot, M. Metalboproteinases in
multiple myeloma. Production of matrix metalboproteinase-9 (MMP-9),
activation of proMMP-2 and induction of MMP-l by myeloma cells.
Blood, 90: 1649-1655, 1997.
13. Wijdenes, J., Vooijs, W. C.. Clement, C.. Post, J., Morard, F., Vita,
N., Laurent, P., Sun, R. X., Klein, B., and Dore, J. M. A plasmocyte
selective monocbonab antibody (B-B4) recognizes syndeean- I . Br. J.Haematol., 94: 318-323, 1996.
14. Carayon, P., and Bord, A. Identification of DNA-replicating lym-
phocyte subsets using a new method to label the bromo-deoxyuridine
incorporated into the DNA. J. Immunol. Methods, 147: 225-230, 1992.
15. Pellat-Deceunynck, C., Puthier, D., Rapp, M. J., Harousseau, J. L.,Bataille, R., and Amiot, M. Adhesion molecules on human plasma cells:
significant changes in expression related to malignant transformation,
tumor spreading and immortalization. Cancer Res., 55: 3647-3653,
I 995.
16. Van Camp, B., Dune, B. G. M., Spier, C., De Wade, M., Van Riet,I., Vela, E., Frutiger, Y., Richter, L., and Grogan, T. M. Plasma cells inmultiple myeboma express a natural killer cell-associated antigen: CD56
(NKH-1; Leu-19). Blood, 76: 377-382, 1990.
17. Harada, H., Kawano, M. M., Huang. N., Harada, Y., Iwato, K..
Tanabe, 0., Tanaka, H., Sakai, A., Asaoku, H., and Kuramoto, A.Phenotypic difference of normal plasma cells from mature myeloma
cells. Blood, 81: 2658-2663. 1993.
18. Gavarotti, P., Boecadoro, M., Redoglia, V., Golzio, F., and Pileri,
A. Reactive plasmocytosis: case report and review of the literature. AetaHaematol., 73: 108-1 10, 1985.
19. Westendorf, J. J., Ahmann, G. J., Greipp. P. R., Witzig, T. E, Kyle,R. A., Lust, J. A., and Jelinek, D. F. Establishment and characterization
of three myeloma cell lines that demonstrate variable cytokine responses
and abilities to produce autoerine interleukin-6. Leukemia (Baltimore).
10: 866-876, 1996.
20. Mazars, G. R., Portier, M., Zhang, X. G., Jourdan, M., Bataille, R.,
Theillet. C., and Klein, B. Mutations of the p53 gene in human myeloma
cell lines. Oneogene, 7: 1015-1018, 1992.
21. Portier, M., Moles, J. P., Mazars, G. R., Jeanteur, P., Bataille, R.,Klein. B., and Theillet, C. p53 and Ras gene mutations in multiple
myeloma. Oneogene, 7: 2539-2543, 1992.
22. Boise, L. H., Minn, A. J., Noel, P. J., June, C. H., Aceavitti, M. A..Lindsten, T., and Thompson, C. B. CD28 costimulation can promote
survival by enhancing the expression of bel-XL. Immunity. 3: 87-98,
1995.
23. Lin, R. H., Hwang, Y-W., Yang, B. C., and Lin, C. S. TNFreceptor-2-triggered apoptosis is associated with the down-regulation of
bcl-XL on activated T cells and can be prevented by CD28 costimula-
tion. J. Immunol., 158: 598-603, 1997.
24. Tu, Y., Renner, S., Xu, F., Fleishman, A., Taylor, J., Weisz, J.,
Vescio, R., Rettig, M., Berenson, J., Krajewski, S., Reed, J. C., and
Lichtenstein, A. Bcl-X expression in multiple myeloma: possible mdi-
cator of ehemoresistance. Cancer Res., 58: 256-262, 1998.
Research. on August 4, 2021. © 1998 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

1998;4:1521-1526. Clin Cancer Res N Robillard, G Jego, C Pellat-Deceunynck, et al. myeloma.CD28, a marker associated with tumoral expansion in multiple
Updated version
http://clincancerres.aacrjournals.org/content/4/6/1521
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/4/6/1521To request permission to re-use all or part of this article, use this link
Research. on August 4, 2021. © 1998 American Association for Cancerclincancerres.aacrjournals.org Downloaded from















![Automation Server Serwer Automatyki - Schneider Electric ... · PDF file[Automation Server Family] ... Każdy moduł można oddzielić od jego podstawy zaciskowej, ... Rysunek: Konstrukcja](https://img.pdfslide.us/doc/110x75/5a7d7f087f8b9a0a668ddf1b/automation-server-serwer-automatyki-schneider-electric-automation-server-family.jpg)