Embed Size (px)
DESCRIPTION
anatomy
Citation preview

SOME RECENT ADVANCES IN EMBRYOLOGY
Recent advances in science and technology, especially in genetics and molecular biology, have helped us to understand embryological development more clearly. Th e uses of ultrasonography in the monitoring of normal and abnormal development; and the use of techniques of in vitrofertilization (used in treatment of infertility) have helped us tremendously. Similarly, it is hoped that in near future we shall be able to use embryonic stem cells in the treatment of various degenerative, genetic and malignant diseases. Th e relationship between “genetics and embryology” is best refl ected in gametogenesis. Th e reduction in the number of chromosomes (haploid number) during gametogenesis and its restoration (diploid number) at the time of fertilization has helped us to understand the mode of inheritance of characters from parents to children. Th e anomalies in the number and structure of chromosomes lead to various birth defects and syndromes. Th e phenomenon of non-disjunction, which is due to abnormal mitosis, results in conditions like Turner syndrome, and Down’s syndrome. Recent advances in molecular biology have been considered in detail in Chapters CD3 and CD4. Th ey have helped us to understand the molecular control of development. Now we know that growth and development is totally under the control of genes. Very recently we have started understanding the role of specifi c genes in development (i.e., how, when and where selected genes are expressed in an embryo to develop a particular structure). For the fi rst time we have understood the role of growth factors and other signaling molecules in embryonic development. Similarly, we have started understanding the critical role of transcription factors including HOX genes in the development of the embryo. Th e knowledge of molecular biology is now helping us to understand the cause and mechanism of congenital malformations. At present we know about many mutant genes that are responsible for various kinds of birth defects.
Phases of the Cell Cycle
One cell cycle consists of the events taking place between the end of one cell division up to the end of the next cell division. Th e cell cycle may be divided into four stages. Th ese are the G1,
Some Miscellaneous Topics
Chapter CD 5

Human Embryology
S1, G2, and M phases. The G1, S1 and G2 phases are collectively known as interphase. This is the phase between two successive mitoses during which a cell duplicates its DNA contents and prepares itself for next cell division. In the M phase (mitosis phase) a cell divides into two daughter cells. Figure CD-5.1 shows the synthesis of DNA during interphase and the splitting
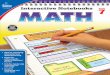
Fig. CD-5.1: The cell cycle consists of four phases i.e., G1 (Gap phase or pre-synthetic phase); S phase (synthetic phase in which DNA replicates); G2 phase (chromosome begins to get condensed and two sister chromatids are formed) and the M phase in which the cell divides into two daughter cells. Sister chromatids
split at the centromere and move into the two daughter cells.
Fig. CD-5.2: Summary of events occurring during one cell cycle.

Chapter CD 5 – Some Miscellaneous Topics
of sister chromatids during the M phase of the cell cycle. Fig. CD-5.2 presents the summary of events occurring during the interphase and the M phase of a cell cycle.
Inter-dependence of Oocyte and Follicular Cells
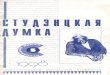
Both the oocyte and surrounding follicular cells are dependent on each other for further development. The follicular cells secrete meiotic inhibitory factors, which prevent primary oocytes from maturing beyond the prophase of the first meiotic division. This effect can last for many years. These inhibitory factors are transmitted to the oocyte via gap junctions present between microvilli of oocytes and of follicular cells. These junctions lie in the zona pellucida (Fig. CD-5.3). Follicular cells are also responsible for growth, metabolism and maturation of oocytes. Conversely, oocytes are responsible for proliferation and differentiation of follicular cells. Factors produced in the oocyte help in formation and maturation of Graafian follicles.
Prechordal Plate
The prechordal plate is a small collection of cells near the cranial end of the notochord. The cells in it are apposed to endoderm. These cells influence the formation of forebrain and eye. The prechordal must not be confused with the prochordal plate. Cranial migration of cells from the primitive knot and into the notochord occurs in two phases. 1. The first phase of migration forms the prechordal plate. 2. The second phase of migration of cells forms the notochordal process.
Fig. CD-5.3: Diagram to show the intimate relationship of oocyte and follicular cells (Gap junctions are present microvilli of the two.

Human Embryology
SOME CHROMOSOMAL ABNORMALITIES
Trisomies associated with autosomes:
�� Trisomy-21, Down’s syndrome�� Trisomy-13, Patau’s syndrome�� Trisomy-18, Edward’s syndrome
Disorders of Chromosome Structure
The most common abnormalities refer to chromosomes in which a portion of the chromosome is missing or is represented twice. The number of chromosomes is normal (46) but the structure of one or more chromosomes is abnormal. The abnormalities in structure of the chromosomes results because of chromosome breakage. Some important structural abnormalities are as follows.�� Deletion�� Inversion�� Ring chromosome�� Isochromosome�� Translocation �� Duplication�� Ring shaped chromosome.
These abnormalities are responsible for various disorders. This occurs because of missing genes (as in deletion), gain of genes (as in duplication), and also because of change in normal position of genes (as in inversion and translocation). Well-known structural abnormalities are associated with the deletion and translocation.
The following is a list of common syndromes associated with deletion:
Syndrome Affected chromosome number Cri-du-chat 5 (5p-) Prader-willi 15 Angelman 15 Wilms tumour 11 Miller –Diekar 17 Di-George 12
All the above syndromes are associated with many birth defects and mental retardation. Almost about 4% cases of Down’s syndrome are due to Robertsonian translocation.
How chromosomal abnormalities (numerical and structural) are detected in laboratories
Chromosomal analysis is required in many clinical conditions for proper diagnosis of genetic diseases. The chromosomal constituent of an individual is called the karyotype. Karyotyping

Chapter CD 5 – Some Miscellaneous Topics
is a procedure to obtain the karyotype of an individual. With the help of a karyotype, numerical and structural abnormalities of chromosomes can be easily identified. The analysis of chromosomes becomes very precise with the help of various banding techniques (G-banding, Q-banding, R-banding etc.). Fluorescent in situ hybridization (FISH) is a new diagnostic technique that uses a specific DNA probe to identify a specific chromosome. With the help of multicolor spectral karyotype (SKY), all chromosomes appear in colour and a multi-color karyotype is obtained. This technique is used to detect chromosomal abnormalities like deletion or translocation.
Gene Abnormalities (Gene Mutations)
Gene mutations are also responsible for various kinds of hemoglobinopathies (thalassaemia and sickle cell anemia etc) and inborn errors of metabolism (alkeptonuria, phenylketonuria, albinism, galactosemia etc.).
Fertilization
1. A very large number of capacitated spermatozoa succeed in passing through the cells of the corona radiata and reaching the ovum. However, only one of them is able to fertilize the ovum.
The glycoprotein of the zona pellucida is responsible for induction of the acrosomal reaction. The release of acrosomal enzymes (acrosin) helps the spermatozoon to penetrate the zona pellucida.
The zona pellucida contains three different glycoproteins ZP1, ZP2 and ZP3. The sperm head contains a specific binding site for ZP3. The sperm-binding site of the ZP3 molecule varies from species to species. This explains why the spermatozoa of one species cannot fertilize the egg of other species.
In Vitro Fertilization
The technique of in vitro fertilization includes the following steps:�� Stimulation of production of oocytes by administration of the drug clomiphene or
gonadotropin.�� Oocytes are collected by a laproscopic technique.�� Spermatozoa are are capacitated by treating them with certain ionic solutions.�� Oocytes and spermatozoa are kept in a petri dish containing a special culture medium.�� The fertilization and subsequent cleavage is monitored microscopically.�� Alternatively, an oocyte may be fertilized by microinjecting it with a spermatozoon.�� One or more embryos, (that have reached the eight cell stage, or have become a blastocyst),
are transferred to the uterus using a catheter.�� The remaining embryos, which are obtained from in vitro fertilization, but are not used,
can be stored for future use by freezing (cryo-preservation) for long periods.Only about 20 to 30% of embryo transfer attempts result in successful pregnancy.

Human Embryology
SOME CONGENITAL ABNORMALITIES
Caudal Regression Syndrome (Sirenomelia)
This condition is characterized by the absence of the sacrum and dysgenesis of the lower lumbar vertebrae. There may be dysgenesis and fusion of the legs. Other anomalies associated with the condition are renal agenesis, imperforate anus and abnormalities of genital organs. Sirenomelia results due to disruption of gastrulation. As a result insufficient mesoderm is formed in the caudal most region of the embryo. As a result caudal parts of the body (lower limb, lower vertebrae and urogenital system) are malformed. Abnormal gastrulation occurs either because of genetic abnormalities, or due to the effects of teratogens.
Some Known Disorders of Craniofacial Development
Many syndromes are associated with disorders of craniofacial development. Some of these are:�� Robin sequence,�� Mandibulo-facial dysostosis (Treacher Collins syndrome),�� Apert syndrome, and �� Crouzon syndrome.
These are genetic disorders, which are also termed the branchial arch syndromes. It is believed that neural crest cells are essential in the formation of the craniofacial region. Failure of the development of neural crest cells may lead to defective formation of the craniofacial region. The first branchial (or pharyngeal) arches (which give rise to the maxilla and the mandible), are particularly affected. This results in mandibulo-facial dysostosis also called the Treacher Collins-Franceschchetti syndrome.
Sternum
When the fusion of the two sternal bars is faulty, the body of the sternum shows a partial or even a complete midline cleft. This is due to mutation in the Hoxb-2 and Hoxb-4 genes. Minor degrees of non-fusion may result in a bifid xiphoid process or in midline foramina. Transverse clefts may also occur. Malformation of the xiphoid process is due to mutation in Hoxc-4 and Hoxa-5 genes.
Achondroplasia
Achondroplasia is an autosomal dominant trait. It is a skeletal growth syndrome characterized by short stature due to slow development of the middle portions of the long bones in the arms and legs. The most common form of achondroplasia is due to a defect of the Fibroblast Growth Factor Receptor (FGFR), and is recognised by exaggerated cranial growth and bossing and depression at the bridge of nose. A second form is pseudoachondroplasia, which is due to defect of Cartilage oligomeric Matrix Protein (COMP) in the joints and is characterized by more typical development of head and face.

Chapter CD 5 – Some Miscellaneous Topics
Cleidocranial Dysostosis
The formation of the clavicle is of particular importance as the bone ossifies in membrane and its developmental anomaly results in a syndrome called Cleidocranial dysplasia. The condition is due to mutation in Cbfa1 gene (core binding factor alpha-1) which causes hypoplasia and delayed ossification of clavicle and other membrane bones of skull. The person may also show the presence of supernumerary teeth. The gene CBFA1 is located on the short arm of chromosome number 6. CBFA1 gene controls differentiation of precursor cells into osteoblasts and is thus essential for membranous as well as endochondral bone formation.
SOME FACTS ABOUT THE NEURAL CREST
1. It is believed that neural crest cells are formed due to action of bone morphogenetic proteins (BMP-4/7) and Wnt, which are secreted by neighboring ectoderm.
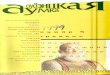
2. Neural crest cells are divided mainly into three divisions viz. cranial neural crest, circumpharyngeal neural crest and trunk neural crest. The neural crest cells of the above three divisions follow different migratory pathways (Fig. CD-5.4).
a. The cranial neural crest arises in the forbrain, midbrain and anterior rhombencephalic regions. Cells arising from the cranial part of the neural crest are believed to migrate into the mesenchyme of the head and neck and influence development of somitomeres. They play an important role in the development of bones, connective tissue and musculature of the head, and face.
Fig. CD-5.4: Various neural crest derivatives and migratory paths in the trunk. Neural crest cells migrate through a dorso-lateral pathway to form pigment cells. They migrate through a ventro-lateral pathway to form dorsal nerve root ganglia. They also migrate through a ventral pathway to form sympathetic ganglia,
preaortic ganglia and parasympathetic ganglia in the gut wall. They also form the adrenal medulla.

Human Embryology
b. The circumpharyngeal neural crest arises in the posterior rhombencephalic region and in the lower part of the pharynx. The neural crest cells from the anterior rhombencephalon migrate towards the developing heart and aortic arches where they contribute to the formation of the outflow tract of the heart, and of great vessels. The neural crest cells from the levels of somites 1 to 7 migrate towards the developing gut and form parasympathetic neurons and myenteric plexuses, which innervate the digestive tract.
c. The neural crest cells of the trunk arise from the level of the sixth somite to the level of the last somite. These cells migrate dorsolaterally to skin, and form melanocytes. Some cells also migrate ventro-laterally to form sensory ganglia. Ventrally they migrate to form sympathetic ganglia, the adrenal medulla, the pre-aortic ganglion and the parasympathetic ganglia and plexuses in the gut wall.
Neural Crest and Spiral Septum
The neural crest cells contribute to the formation of the spiral septum (in the truncus arteriosus and the outflow tracts of the right and left ventricles). These neural crest cells migrate from the region of the hindbrain to the developing heart. They pass through pharyngeal arches 3, 4 and 6. Failure of such migration of neural crest cells leads to congenital malformations of the outflow tract of the heart i.e., pulmonary stenosis, teratology of Fallot, persistent truncus arteriosus and transposition of great vessels. As the neural crest cells also contribute to the formation of various parts of the head and neck congenital anomalies of the heart and of the head and neck are often associated with each other.