Embed Size (px)
Citation preview

2004CCNCCCNC
PRESENTATION:NC Medicaid Reform
“Improving Quality While Controlling Cost”
PRESENTATION:NC Medicaid Reform
“Improving Quality While Controlling Cost”
L. Allen Dobson ,Jr. MD FAAFPSenior Policy Advisor /CCNCNC Department of Health &Human Services
L. Allen Dobson ,Jr. MD FAAFPSenior Policy Advisor /CCNCNC Department of Health &Human Services
HOME
NEXT
LAST

2004CCNCCCNC

2004CCNCCCNC
ObjectivesObjectivesGeneral problems facing State Medicaid ProgramsCommunity Care of NC- our experience and what led us to our current programDiscussion of ongoing initiatives and resultsA few take home thoughts
General problems facing State Medicaid ProgramsCommunity Care of NC- our experience and what led us to our current programDiscussion of ongoing initiatives and resultsA few take home thoughts

2004CCNCCCNC
“States Struggle with Medicaid budgets”
“States Struggle with Medicaid budgets”
Policy Tools Utilized by StatesPA, PDL, Supplemental rebatesReimbursement cutsEligibility cutsFixed rate contracts- managed care organizationsDisease Management??New-Recipient self purchased plan with fixed $ amount- Fla
Policy Tools Utilized by StatesPA, PDL, Supplemental rebatesReimbursement cutsEligibility cutsFixed rate contracts- managed care organizationsDisease Management??New-Recipient self purchased plan with fixed $ amount- Fla

2004CCNCCCNC

2004CCNCCCNC

2004CCNCCCNC
The Cost EquationThe Cost EquationEligibility and benefit- who you cover and for whatReimbursement- what you payUtilization- how much services are provided
We just have not figured out how to manage utilization!!!
Eligibility and benefit- who you cover and for whatReimbursement- what you payUtilization- how much services are provided
We just have not figured out how to manage utilization!!!

2004CCNCCCNC

2004CCNCCCNC
North Carolina MedicaidNorth Carolina MedicaidPCCM ( Access I) started in 1992HMO contracted in 3 metro area 1997First ( 7) community networks ( Access II/III) piloted 1998Most HMOs did not renew- 2001CCNC( Access II/III) became single Medicaid strategy 2002
PCCM ( Access I) started in 1992HMO contracted in 3 metro area 1997First ( 7) community networks ( Access II/III) piloted 1998Most HMOs did not renew- 2001CCNC( Access II/III) became single Medicaid strategy 2002

2004CCNCCCNC
Current NC Medicaid FactsCurrent NC Medicaid Facts1.2 million covered (15.2% 0f population)686,000 children covered45% of all babies born covered30.5 % of recipients consume 74.5% resourcesDrug cost now equals hospital cost was increasing at double digit rate yearlyInpatient care (hosp,NH,MRC) consumes 40.7%Physicians account for only 9-10% of costs!!!
1.2 million covered (15.2% 0f population)686,000 children covered45% of all babies born covered30.5 % of recipients consume 74.5% resourcesDrug cost now equals hospital cost was increasing at double digit rate yearlyInpatient care (hosp,NH,MRC) consumes 40.7%Physicians account for only 9-10% of costs!!!

2004CCNCCCNC
ISSUES:• No real care coordination system at the local level
• PCPs feel limited in their ability to manage care in the current system
• Local public health departments and area mental health programs are not coordinated into the medical care management process
• Duplication of services at the local level• State “Silo Funding”

2004CCNCCCNC
Issues(continued..)Issues(continued..)
Only 1/3 of Medicaid budget is women and children. 2/3 disabled and elderly which is less suitable for typical commercial managed care approachLarge portion of the state’s Medicaid population is in rural counties where there is minimal managed care activity
Only 1/3 of Medicaid budget is women and children. 2/3 disabled and elderly which is less suitable for typical commercial managed care approachLarge portion of the state’s Medicaid population is in rural counties where there is minimal managed care activity

2004CCNCCCNC
SOCIAL SERVICES
SILO
EMSSILO
HOSPITALSSILO
PUBLICHEALTH
SILO
MH/DD/SASSILO
DOCTORSSILO OTHER
PROVIDERSSILO
OURSYSTEM

2004CCNCCCNC Silos Within SilosDivision of Social Services
Carolina Access MCR(Managed Care Representative)* Gathers & processes local enrollment data* Interprets Access roles for the state* Gathers local Medicaid statistics* Patients & doctors representative
Medicaid IntakeTransportationWork First/Job PlacementChild Protection ServicesAdult Protection ServicesDay CareChild SupportEmergency Assistance
Food Stamps
Division of Public Health
Child Services CoordinationMaternity Care CoordinationMaternal Outreach ProgramHealth CheckPostpartum Newborn/ Nurse Home
Visiting ProgramIntensive Home Visitor ProgramImmunization ProgramFamily PlanningWIC/Breast Feeding PromotionCommunicable DiseaseEnvironmental HealthHealth Promotions

2004CCNCCCNC
Carolina Access I (10+ yr experience)The statewide PCCM has resulted in:
• Medicaid patients linked with a primary care provider increasing access to services across the state
• Primary care providers willing to serve as a gatekeepers and assist patients with appropriateutilization of the health care system( $2.50pmpm)
IMPROVED ACCESSThe problem was that it did not address the population that consumed the most resources!!

2004CCNCCCNC
Options consider for NC Medicaid
Options consider for NC Medicaid
State Operated
Contracted Out
Locally Run
State Operated
Contracted Out
Locally Run
HOME
NEXT
LAST

2004CCNCCCNC
Primary GoalsPrimary Goals
Improve the care of the Medicaid population while controlling costs
Develop Community based networks capable of managing populations
Improve the care of the Medicaid population while controlling costs
Develop Community based networks capable of managing populations
HOME
NEXT
LAST

2004CCNCCCNC
Basic Operating PremiseBasic Operating PremiseRegardless of who manages Medicaid, the hospitals, physicians and safety net providers in NC serving patients remain the same and must be engagedWe need to transform Medicaid management from a regulatory function to a health management functionWe must carefully balance cost containment with quality improvement effortsDecision making must be driven by data & outcomes monitoredWe must help transform healthcare system from acute care model to chronic illness model
Regardless of who manages Medicaid, the hospitals, physicians and safety net providers in NC serving patients remain the same and must be engagedWe need to transform Medicaid management from a regulatory function to a health management functionWe must carefully balance cost containment with quality improvement effortsDecision making must be driven by data & outcomes monitoredWe must help transform healthcare system from acute care model to chronic illness model

2004CCNCCCNC
“Management rather than Regulation”
“Management rather than Regulation”

2004CCNCCCNC
Goals Achieved By:Goals Achieved By:
Making Sure People Get Care When They Need It
Increasing local provider collaboration
Obtaining Quality Care
Implementing Best Practice Guidelines
Managing Medicaid Costs
Making Sure People Get Care When They Need It
Increasing local provider collaboration
Obtaining Quality Care
Implementing Best Practice Guidelines
Managing Medicaid Costs
December 9, 2003
HOME
NEXT
LAST
CCNCCCNC

2004CCNCCCNC
Community Care of North CarolinaCommunity Care of North Carolina
Joins other community providers (hospitals, health departments and departments of social services) with physicians
Creates community networks that assume responsibility for managing recipient care
Joins other community providers (hospitals, health departments and departments of social services) with physicians
Creates community networks that assume responsibility for managing recipient care
Build on ACCESS IBuild on ACCESS I
HOME
NEXT
LAST

2004CCNCCCNC
Community Care of North CarolinaCommunity Care of North CarolinaFocuses on improved quality, utilization and cost effectiveness of chronic illness care
15 Networks with more than 3000 physicians
595,000 enrollees
Focuses on improved quality, utilization and cost effectiveness of chronic illness care
15 Networks with more than 3000 physicians
595,000 enrollees
HOME
NEXT
LAST

2004CCNCCCNC
AccessCare Network SitesAccessCare Network CountiesAccess II Care of Western NCAccess III of Lower Cape Fear
Cabarrus Community Care Plan
Central Piedmont Access IICarolina Community Health Partnership
Comm. Care Partners of Gtr. Mecklenburg
Community Care Plan of Eastern NCCommunity Health PartnersNorthern Piedmont Community Care
Partnership for Health Management
Sandhills Community Care NetworkWake County Access II
Community Care of North CarolinaCommunity Care of North Carolina
HOME
NEXT
LAST
Access II and III Networks – 9/04Access II and III Networks – 9/04

2004CCNCCCNC
Community Care Networks: Community Care Networks: Non-profit organizationsIncludes all providers including safety net providersSteering/Governance committeeMedical management committeeReceive $2.50 PM/PM from the StateHire care managers/medical management staff
Non-profit organizationsIncludes all providers including safety net providersSteering/Governance committeeMedical management committeeReceive $2.50 PM/PM from the StateHire care managers/medical management staff
HOME
NEXT
LAST

2004CCNCCCNC
What Networks DoWhat Networks DoAssume responsibility for Medicaid recipients
Identify costly patients and costly services
Develop and implement plans to manage utilization and cost
Create the local systems to improve care & reduce variability
Implement improved care management and disease management systems
Assume responsibility for Medicaid recipients
Identify costly patients and costly services
Develop and implement plans to manage utilization and cost
Create the local systems to improve care & reduce variability
Implement improved care management and disease management systems
HOME
NEXT
LAST

2004CCNCCCNC
Key Program Areas in Managing Clinical Care:Key Program Areas in Managing Clinical Care:
Implementing quality improvement — Best practice processes
Implementing disease management
Managing high-risk patients
Managing high-cost services
Building accountability through monitoring & reporting
Implementing quality improvement — Best practice processes
Implementing disease management
Managing high-risk patients
Managing high-cost services
Building accountability through monitoring & reporting
HOME
NEXT
LAST

2004CCNCCCNC
Managing Clinical CareManaging Clinical Care
HOME
NEXT
LAST
Clinical Directors Group • Select targeted diseases/care processes• Review evidenced-based practice guidelines• Define the program• Establish program measures
• Select targeted diseases/care processes• Review evidenced-based practice guidelines• Define the program• Establish program measures
I
ASTHMAASTHMA
DIABETESDIABETES
PHARMACYPHARMACY
HIGH-RISK & -COSTHIGH-RISK & -COST
EDED
Local Medical Mgmt. Comm.
• Implement state-level initiatives• Develop local improvement initiatives• Implement state-level initiatives• Develop local improvement initiatives
PRACTICE A PRACTICE B PRACTICE C
Care Managers and Access II and III quality improvement staff support clinical management activitiesCare Managers and Access II and III quality improvement staff support clinical management activities
III
IIGASTRO-ENTERITISGASTRO-ENTERITIS
OTITIS MEDIAOTITIS MEDIA
CHILD DEVELOPMENTCHILD DEVELOPMENT
ADHDADHD
FEVERFEVER
DEPRESSIONDEPRESSION
LOW BIRTH WEIGHTLOW BIRTH WEIGHT
ANCILLARY SERVICESANCILLARY SERVICES
BEST PRACTICES

2004CCNCCCNC
Improving Quality “Disease Management”
Improving Quality “Disease Management”

2004CCNCCCNC
Current Disease Management Initiatives
Current Disease Management Initiatives
AsthmaDiabetesPilots in Depression, ADHD, Special Needs Children, Gastroenteritis, Otitis Media and Low Birth Weight
AsthmaDiabetesPilots in Depression, ADHD, Special Needs Children, Gastroenteritis, Otitis Media and Low Birth Weight
HOME
NEXT
LAST

2004CCNCCCNC
Asthma InitiativeAsthma Initiative
First program initiative – began Jan. 1999 Adopted best practice guidelines (NIH)Implemented continuous quality improvement processes at each practicePhysicians set performance measuresProvide regular monitoring and feedback
First program initiative – began Jan. 1999 Adopted best practice guidelines (NIH)Implemented continuous quality improvement processes at each practicePhysicians set performance measuresProvide regular monitoring and feedback
HOME
NEXT
LAST

2004CCNCCCNC
Asthma InitiativeAsthma Initiative
HOME
NEXT
LAST
KeyKey
Process MeasuresProcess Measures
47%
56%64% 64%
49%
93% 95% 92%
67%
78% 75% 73%
0%
20%
40%
60%
80%
100%
'99 '00 '01 '02 '99 '00 '01 '02 '99 '00 '01 '02
47%
56%64% 64%
49%
93% 95% 92%
67%
78% 75% 73%
0%
20%
40%
60%
80%
100%
'99 '00 '01 '02 '99 '00 '01 '02 '99 '00 '01 '02
1 2 3
1 No. with asthmawho had documentation of staging
No. with asthmawho had documentation of staging
2 No. staged II – IV on inhaled corticosteroids
No. staged II – IV on inhaled corticosteroids
3 No. staged II – IV who have an AAPNo. staged II – IV who have an AAP

2004CCNCCCNC
Asthma InitiativeAsthma Initiative
HOME
NEXT
LAST
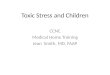
Pediatric Asthma Hospitalization RatesPediatric Asthma Hospitalization Rates
8.2
5.3
0123456789
10
Access I Access II & III
8.2
5.3
0123456789
10
Access I Access II & III
April 2000 - December 2002April 2000 - December 2002
KeyKeyIn patient admission rate per 1000 member monthsIn patient admission rate per 1000 member months

2004CCNCCCNC
Asthma Pilot DM Findings from Sheps:Asthma Pilot DM Findings from Sheps:
CY 2000 Annual Savings $ 290,000
CY 2001 Annual Savings $ 1,470,000
CY 2002 Annual Savings $ 1,580,000
CY 2000 Annual Savings $ 290,000
CY 2001 Annual Savings $ 1,470,000
CY 2002 Annual Savings $ 1,580,000

2004CCNCCCNC
Diabetes InitiativeDiabetes InitiativeSecond program-wide initiative – began July 2000Adopted best practice guidelines (ADA)Implement continuous quality improvement processes at each practicePhysicians set performance measuresProvide regular monitoring and feedback
Second program-wide initiative – began July 2000Adopted best practice guidelines (ADA)Implement continuous quality improvement processes at each practicePhysicians set performance measuresProvide regular monitoring and feedback
HOME
NEXT
LAST

2004CCNCCCNC
Diabetes InitiativeDiabetes InitiativeACCESS II-III Diabetes Chart Audit ResultsACCESS II-III Diabetes Chart Audit Results
0
10
20
30
40
50
60
70
80
90
100
BP Referral forDial. Eye exam
Foot Exam HbA1c every 6mo.
Lipid Prof ile Album.Screening
Flu Vaccine PneumococcalVaccine
Per
cent
age
0
10
20
30
40
50
60
70
80
90
100
BP Referral forDial. Eye exam
Foot Exam HbA1c every 6mo.
Lipid Prof ile Album.Screening
Flu Vaccine PneumococcalVaccine
Per
cent
age
Baseline (July – Dec. ’00)Baseline (July – Dec. ’00) July – Dec. ‘01July – Dec. ‘01 Jan. – June ‘02Jan. – June ‘02 July.- Dec. ‘02July.- Dec. ‘02

2004CCNCCCNC
SOURCE: February 20, 2004Sheps Center Report
SOURCE: February 20, 2004Sheps Center Report
Diabetes Disease Management Findings:
Overall pmpm costs for CCNC diabetes lower than Access9% lower hospital admissions
Diabetes Disease Management Findings:
Overall pmpm costs for CCNC diabetes lower than Access9% lower hospital admissions

2004CCNCCCNC
Diabetes DM Findings from Sheps:Diabetes DM Findings from Sheps:
Cost savings for diabetes care for 3 year period approximately $2.1 million
Potential > $11.3 million total savings in 2003 if CCNC were statewide with asthma and diabetes DM
Cost savings for diabetes care for 3 year period approximately $2.1 million
Potential > $11.3 million total savings in 2003 if CCNC were statewide with asthma and diabetes DM

2004CCNCCCNC
Managing Costs“ Targeted Approach”
Managing Costs“ Targeted Approach”

2004CCNCCCNC
Managing High-Cost Services:Managing High-Cost Services:Pharmacy
— Nursing home polypharmacy— PAL— Ambulatory polypharmacy
Emergency DepartmentAncillary ServicesIn-home Care
Pharmacy— Nursing home polypharmacy— PAL— Ambulatory polypharmacy
Emergency DepartmentAncillary ServicesIn-home Care
HOME
NEXT
LAST
MANAGING HIGH-COST SERVICES

2004CCNCCCNC
ED InitiativeED InitiativeTarget enrollees with 3 or more ED visits in 6 month time periodCare managers perform outreach, education & follow-upSpecial mailings target top 3 reasons for ED visits (otitis media, fever, upper respiratory infections)
Reinforce “medical home” concept
Target enrollees with 3 or more ED visits in 6 month time periodCare managers perform outreach, education & follow-upSpecial mailings target top 3 reasons for ED visits (otitis media, fever, upper respiratory infections)
Reinforce “medical home” concept
HOME
NEXT
LAST

2004CCNCCCNC
HOME
NEXT
LAST
ED InitiativeED Initiative
56.92
45.49
36.437.9530.8
42.05
0
10
20
30
40
50
60
Access I2001
CCNC2001
Access I2002
CCNC2002
Access I2003
CCNC2003
56.92
45.49
36.437.9530.8
42.05
0
10
20
30
40
50
60
Access I2001
CCNC2001
Access I2002
CCNC2002
Access I2003
CCNC2003
ED Utilization Rate – 7/1/01 – 6/30/03 – Children < 21 yearsED Utilization Rate – 7/1/01 – 6/30/03 – Children < 21 years
UR
Rat
e Pe
r 100
0 M
MU
R R
ate
Per 1
000
MM
Fiscal YearFiscal Year

2004CCNCCCNC
HOME
NEXT
LAST
ED InitiativeED Initiative
$8.32
$4.17
$7.90
$5.80
$0
$1
$2
$3
$4
$5
$6
$7
$8
$9
Access I 2001 Access II & III2001
Access I 2002 Access II & III2002
$8.32
$4.17
$7.90
$5.80
$0
$1
$2
$3
$4
$5
$6
$7
$8
$9
Access I 2001 Access II & III2001
Access I 2002 Access II & III2002
ED Cost PMPM – 7/1/01 – 6/30/02 – Children < 21 yearsED Cost PMPM – 7/1/01 – 6/30/02 – Children < 21 years
ED C
ost P
MPM
ED C
ost P
MPM
Fiscal YearFiscal Year
Savings CalculationSavings Calculation(Access I PMPM –Access II-III) x Access II-III Enrollment
(Access I PMPM –Access II-III) x Access II-III Enrollment
Total Savings – ’01-’02$10,362,190Total Savings – ’01-’02$10,362,190

2004CCNCCCNC
Cost Effective Prescribing 2003Cost Effective Prescribing 2003“How to make a difference in rising prescription drug costs!”“How to make a difference in rising prescription drug costs!”
HOME
NEXT
LAST

2004CCNCCCNC
HOME
NEXT
LAST
NC Medicaid Expenditures:Prescription DrugsNC Medicaid Expenditures:Prescription Drugs
$ 0
$ 2 0 0 , 0 0 0 , 0 0 0
$ 4 0 0 , 0 0 0 , 0 0 0
$ 6 0 0 , 0 0 0 , 0 0 0
$ 8 0 0 , 0 0 0 , 0 0 0
$ 1 , 0 0 0 , 0 0 0 , 0 0 0
$ 1 , 2 0 0 , 0 0 0 , 0 0 0
$ 1 , 4 0 0 , 0 0 0 , 0 0 0
1 9 9 9 2 0 0 0 2 0 0 1 2 0 0 2 2 0 0 3 2 0 0 4
$ 0
$ 2 0 0 , 0 0 0 , 0 0 0
$ 4 0 0 , 0 0 0 , 0 0 0
$ 6 0 0 , 0 0 0 , 0 0 0
$ 8 0 0 , 0 0 0 , 0 0 0
$ 1 , 0 0 0 , 0 0 0 , 0 0 0
$ 1 , 2 0 0 , 0 0 0 , 0 0 0
$ 1 , 4 0 0 , 0 0 0 , 0 0 0
1 9 9 9 2 0 0 0 2 0 0 1 2 0 0 2 2 0 0 3 2 0 0 4
FY99$557,772,670FY99$557,772,670
FY00$754,505,194FY00$754,505,194
FY01$927,240,693FY01$927,240,693
FY02$1,056.158.750FY02$1,056.158.750

2004CCNCCCNC
Process – PALProcess – PAL
Pharmacy committee defines drug classes and unit dosesMedicaid calculates relative drug cost and rank ( net costs- includes rebates)Inform Access II and III physiciansMeasure changes in prescribing patternsState-wide rollout began Nov 2003
Pharmacy committee defines drug classes and unit dosesMedicaid calculates relative drug cost and rank ( net costs- includes rebates)Inform Access II and III physiciansMeasure changes in prescribing patternsState-wide rollout began Nov 2003
HOME
NEXT
LAST

2004CCNCCCNC
PAL — Prescription Advantage ListPAL — Prescription Advantage List
HOME
NEXT
LAST

2004CCNCCCNC
Anticipated SavingsAnticipated SavingsPAL- $ 30 -40 million annual savings expectedOther Pharmacy Management/Policy Initiatives:Selected Prior ApprovalSpecialty Disease RegistryActive Intervention Selected OTC coverage
PAL- $ 30 -40 million annual savings expectedOther Pharmacy Management/Policy Initiatives:Selected Prior ApprovalSpecialty Disease RegistryActive Intervention Selected OTC coverage

2004CCNCCCNC
Nursing Home Polypharmacy Initiative( “Active Intervention”)
Nursing Home Polypharmacy Initiative( “Active Intervention”)Community Care of North CarolinaCommunity Care of North Carolina
HOME
NEXT
LAST

2004CCNCCCNC
InterventionIntervention
Pharmacist / Physician TeamsReview drug profiles / medical records of Medicaid patients in nursing homesDetermine if a drug therapy problem existsRecommend a changePerform follow-up to determine if change was made
Pharmacist / Physician TeamsReview drug profiles / medical records of Medicaid patients in nursing homesDetermine if a drug therapy problem existsRecommend a changePerform follow-up to determine if change was made
HOME
NEXT
LAST

2004CCNCCCNC
Screening CriteriaScreening CriteriaNursing home residents with . . .− >18 drugs used in a 90 day period
9208 residents met this criteria
Medicaid database uses criteria to flag charts
Nursing home residents with . . .− >18 drugs used in a 90 day period
9208 residents met this criteria
Medicaid database uses criteria to flag charts
HOME
NEXT
LAST

2004CCNCCCNC
Flagging CriteriaFlagging Criteria
Inappropriate Rx for the elderly “Beers drugs”Drugs used beyond usual time limitDrug Use Warnings & precautionsPrescription Advantage List “PAL”Potential Therapeutic Duplication
Inappropriate Rx for the elderly “Beers drugs”Drugs used beyond usual time limitDrug Use Warnings & precautionsPrescription Advantage List “PAL”Potential Therapeutic Duplication
HOME
NEXT
LAST

2004CCNCCCNC
Preliminary FindingsPreliminary FindingsPatients reviewed: 9208Recommendations made: 8559− Unnecessary therapy – 19%− More cost effective drug – 56%− Wrong dose – 7%− Potential adverse reaction – 9%− Needs additional therapy – 3%− Other – 6%
Recommendations implemented: 6359 (74%)
Patients reviewed: 9208Recommendations made: 8559− Unnecessary therapy – 19%− More cost effective drug – 56%− Wrong dose – 7%− Potential adverse reaction – 9%− Needs additional therapy – 3%− Other – 6%
Recommendations implemented: 6359 (74%)
HOME
NEXT
LAST

2004CCNCCCNC
HOME
NEXT
LAST
Potential Cumulative Savings from InterventionsPotential Cumulative Savings from InterventionsDollars in MillionsDollars in Millions
$0$2$4$6$8
$10
$12$14
$16
Nov Jan
Mar
May Jul
Sep Nov Jan
Mar
May Jul
Sep Nov
$0$2$4$6$8
$10
$12$14
$16
Nov Jan
Mar
May Jul
Sep Nov Jan
Mar
May Jul
Sep Nov

2004CCNCCCNC
Cost/Benefit EstimatesCost/Benefit Estimates

2004CCNCCCNC
Community Care of North CarolinaCommunity Care of North Carolina
Cost - $8.1 Million(Cost of Community Care operation)
Savings - $60,182,128 compared to FY02
Savings- $203,423,814 compared to FFS
(Mercer Cost Effectiveness Analysis – AFDC only for Inpatient, Outpatient, ED, Physician Services, Pharmacy, Administrative Costs, Other)
Cost - $8.1 Million(Cost of Community Care operation)
Savings - $60,182,128 compared to FY02
Savings- $203,423,814 compared to FFS
(Mercer Cost Effectiveness Analysis – AFDC only for Inpatient, Outpatient, ED, Physician Services, Pharmacy, Administrative Costs, Other)
July 1, 2002 – Jun 30, 2003July 1, 2002 – Jun 30, 2003
HOME
NEXT
LAST

2004CCNCCCNC
NC Medicaid ExpendituresNC Medicaid Expenditures
012345678
1 9 9 6 1 9 9 7 1 9 9 8 1 9 9 9 2 0 0 0 2 0 0 1 2 0 0 2 2 0 0 3
Bil
lion
s
C o s t s
012345678
1 9 9 6 1 9 9 7 1 9 9 8 1 9 9 9 2 0 0 0 2 0 0 1 2 0 0 2 2 0 0 3
Bil
lion
s
C o s t s

2004CCNCCCNC
Pilot InitiativesPilot InitiativesTherapy servicesLow birth weightDisparitiesMental health integrationPoly-pharmacy in outpatient settingsSickle cellCommunity Access programs (uninsured)Special needs population
Therapy servicesLow birth weightDisparitiesMental health integrationPoly-pharmacy in outpatient settingsSickle cellCommunity Access programs (uninsured)Special needs population
HOME
NEXT
LAST

2004CCNCCCNC
Big Lessons & ChallengesBig Lessons & ChallengesThere are no easy $ 100 million decisions- but there may be 50 $ 2million decisions ( you just have to find them)Providers must be engaged- but a challenge to keep their attentionMust make policy decisions consistent with program goals and visionSavings are additive (the total sum of savings seem to be greater than the sum of individual initiatives)
There are no easy $ 100 million decisions- but there may be 50 $ 2million decisions ( you just have to find them)Providers must be engaged- but a challenge to keep their attentionMust make policy decisions consistent with program goals and visionSavings are additive (the total sum of savings seem to be greater than the sum of individual initiatives)

2004CCNCCCNC
Other Lessons LearnedOther Lessons Learned1. Top down approach is not effective in N.C.2. Community ownership a must3. Can’t do it alone - must partner4. Incentives must be aligned5. Must develop systems that change behavior at the
practice and community level6. Have to be able to measure outcomes (data and
feedback important- “you get what you inspect…”)7. Lasting change takes time and reinforcement8. There are indirect quality and cost benefits to the
community
1. Top down approach is not effective in N.C.2. Community ownership a must3. Can’t do it alone - must partner4. Incentives must be aligned5. Must develop systems that change behavior at the
practice and community level6. Have to be able to measure outcomes (data and
feedback important- “you get what you inspect…”)7. Lasting change takes time and reinforcement8. There are indirect quality and cost benefits to the
communityHOME
NEXT
LAST

2004CCNCCCNC
HOME