Embed Size (px)
Citation preview

www.ccna-ccnv.ca
CCNA: What students in Aging research
need to know..SPA 2021

Click to edit Master title style
Disclosure slide• Faculty: Dr. Howard Chertkow
• Relationships with commercial interests:• Dr. Chertkow is co-investigator on pharma-sponsored
clinical trials of Roche, Immunotec, Lilly, Anavex Life Sciences, and Abbvie.
•Previous Industrial Support over five years for clinical trials, research studies, speakers boards, advisory boards, received from:•Pfizer Inc.•Bristol Myers Squibb• TauRx
•No Funding support has been received for this presentation

Click to edit Master title style
Funding Support for Dr. Chertkow• Dr. Chertkow is supported by a research chair from
Baycrest Health Science and University of Toronto.
• Canadian Institutes for Health Research• MOP 10392• MOP 29342• Foundation Grant Award 2015-22• CIHR: PI of operating grant for CCNA,plus “BRAIN” big data
and dementia operating grant
• Weston Foundation• The 11 partners of the CCNA contribute to the national
program.
Mitigating Bias: All recommendations for clinical therapy have been suggested by the Canadian Consensus Conference on Diagnosis and Treatment of Dementia

4
CCNA Basics
• Established following Canada’s commitment to tackle dementia
following G8 Summit in 2012
• Funders : CIHR (Institute of Aging) and partners
• Phase I (2014-2019) = $33 million;
• Phase II (after peer review 2019-24) = $42 million
• Research strategy to accelerate discovery, innovation and adoption of
new knowledge, directed at the prevention, treatment, and management
of the neurodegenerative diseases of aging
• Goal: To improve the quality of life of individual Canadians living
with these diseases

BC 26 AB
30 SK20 ON
118
QC 96
NB4
NS12
MB7
Phase II - 313 CCNA researchers across Canada
Key factors:• Inclusion• Collegiality• Compromise• Willingness to work together

CCNA Phase II at a Glance
PARTNER ORGANIZATIONSPROGRAMSCCNA is a Government of Canada initiative, also supported byseveral national, provincial and non-profit organizations.

8
Principles of CCNA
Before CCNA
• Individual Canadian researchers receive individual grants to pursue ideas on their own in a “bottom up” fashion
What CCNA Adds
• Adds a “top down” organized attack on the coming dementia epidemic to avoid funding gaps
• Promotes collaboration and coordination: we are advancing the science strategically and faster
• Adds novel national team funding for specific Canadian “strengths”
• Enhances synergy between neurologists, geriatricians, psychiatrists, psychologists, and basic scientists working together
• Accelerates progress in basic science and therapy
• Catalyzes research on all of the dementias (all neurodegenerative diseases, NDD)
• Provides cohorts and infrastructure not accessible to single research scientists
• Connects with CLSA and scientists working on “normal aging”

CCNA Training and Capacity Building Program
Training and Capacity Building (TCB)
Program Leader: Dr. Manuel Montero-Odasso
▪ The CCNA/ASC specifically funding a set of trainees working under
the supervision of affiliated CCNA investigators
▪ Training will be enhanced by planned professional development
and networking opportunities (workshops, cafés, meetings)
▪ Novel grant support for training opportunities, workshops
▪ Developing on-line modules for “extra” training domains
▪ Building a national dementia student identity
▪ Opening this up to all students working in dementia-related fields,
whether funded directly by CCNA or not

Six Goals of the CCNA in Phase II
Understand subgroups
Develop new treatment molecules
Preventionstrategies
Allow earlier diagnosis
Innovate with new life improvement tools/strategies
Optimize health care delivery

Goal Details 10-15 Year Deliverable
1. Understand Subgroups
2. Develop New Treatment Molecules
3. Develop Prevention Strategies
4. Allow Earlier Diagnosis
5. Innovate Life Improvements
6. Optimize Health Care Delivery
Six Goals of CCNA
Elucidate cause and recognition of novel AD subgroups
Paradigm shift, new subgroup targets for therapies
Develop personalized therapy according to subgroups
New, effective validated therapies for ADRD
Develop evidence-based combination prevention strategies
Strategies for public health policy-makers to implement
Biomarker combinations to recognize subgroups before symptoms are florid
Algorithms for clinical diagnosis.
1. Hearing and vision support2. New technologies3. Driverless cars4. Reduced multi-morbidity5. Reduced stigma strategies6. Specific strategies for indigenous populations
Applied to produce better quality of life in individuals with ADRD
1. Delineate best clinical practices across provinces2. Optimize care for dementia in rural setting3.Optimize care for dementia in Indigenous population
Knowledge translation into clinical practice for improved outcomes

12
About the Teams
• All teams are national (members from multiple institutions) and topic-based
• Teams play to “Canadian research strengths”
• Five-year research program and budget of the team with deliverables
• Annual meetings to promote interaction and synergy
• Promotion of young researchers: 17 young Canadian researchers in leadership positions
• Leveraging of funding with other agencies
• 14 of the teams will leverage data from the COMPASS-ND cohort
COMPASS-ND = “COMPrehensive ASSessment of Neurodegenerative Diseases”
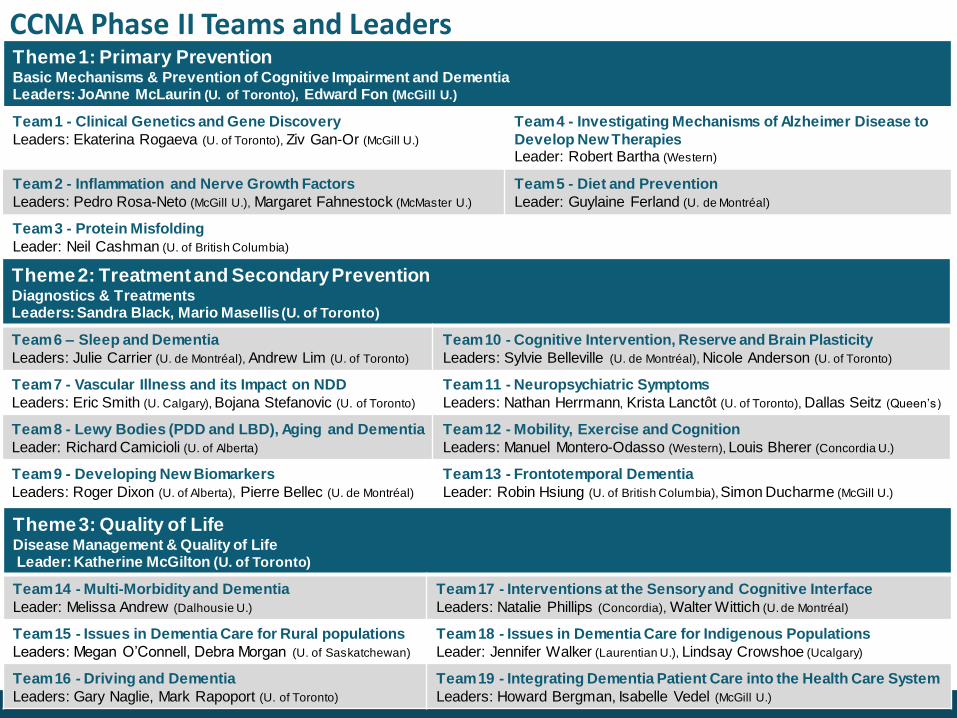
CCNA Phase II Teams and LeadersTheme 1: Primary PreventionBasic Mechanisms & Prevention of Cognitive Impairment and DementiaLeaders: JoAnne McLaurin (U. of Toronto), Edward Fon (McGill U.)
Team 1 - Clinical Genetics and Gene Discovery
Leaders: Ekaterina Rogaeva (U. of Toronto), Ziv Gan-Or (McGill U.)
Team 4 - Investigating Mechanisms of Alzheimer Disease to
Develop New TherapiesLeader: Robert Bartha (Western)
Team 2 - Inflammation and Nerve Growth Factors
Leaders: Pedro Rosa-Neto (McGill U.), Margaret Fahnestock (McMaster U.)
Team 5 - Diet and Prevention
Leader: Guylaine Ferland (U. de Montréal)
Team 3 - Protein Misfolding
Leader: Neil Cashman (U. of British Columbia)
Theme 2: Treatment and Secondary PreventionDiagnostics & Treatments Leaders: Sandra Black, Mario Masellis (U. of Toronto)
Team 6 – Sleep and Dementia
Leaders: Julie Carrier (U. de Montréal), Andrew Lim (U. of Toronto)
Team 10 - Cognitive Intervention, Reserve and Brain Plasticity
Leaders: Sylvie Belleville (U. de Montréal), Nicole Anderson (U. of Toronto)
Team 7 - Vascular Illness and its Impact on NDD
Leaders: Eric Smith (U. Calgary), Bojana Stefanovic (U. of Toronto)
Team 11 - Neuropsychiatric Symptoms
Leaders: Nathan Herrmann, Krista Lanctôt (U. of Toronto), Dallas Seitz (Queen’s)
Team 8 - Lewy Bodies (PDD and LBD), Aging and Dementia
Leader: Richard Camicioli (U. of Alberta)
Team 12 - Mobility, Exercise and Cognition
Leaders: Manuel Montero-Odasso (Western), Louis Bherer (Concordia U.)
Team 9 - Developing New Biomarkers
Leaders: Roger Dixon (U. of Alberta), Pierre Bellec (U. de Montréal)
Team 13 - Frontotemporal Dementia
Leader: Robin Hsiung (U. of British Columbia), Simon Ducharme (McGill U.)
Theme 3: Quality of LifeDisease Management & Quality of LifeLeader: Katherine McGilton (U. of Toronto)
Team 14 - Multi-Morbidity and Dementia
Leader: Melissa Andrew (Dalhousie U.)
Team 17 - Interventions at the Sensory and Cognitive Interface
Leaders: Natalie Phillips (Concordia), Walter Wittich (U. de Montréal)
Team 15 - Issues in Dementia Care for Rural populations
Leaders: Megan O’Connell, Debra Morgan (U. of Saskatchewan)
Team 18 - Issues in Dementia Care for Indigenous Populations
Leader: Jennifer Walker (Laurentian U.), Lindsay Crowshoe (Ucalgary)
Team 16 - Driving and Dementia
Leaders: Gary Naglie, Mark Rapoport (U. of Toronto)
Team 19 - Integrating Dementia Patient Care into the Health Care System
Leaders: Howard Bergman, Isabelle Vedel (McGill U.)

14
Synergies Built Over Time
CCNA promotes cross-
fertilization, synergy, and
interaction between
teams

Neurodegenerative Disease Groups
Frontotemporal dementia
Alzheimer’s
Parkinson’s
15
CCNA allows
comparison between
Neurodegenerative
Disease groups

16
Women, Sex, Gender and Dementia Cross-cutting Program
First national dementia initiative to bring the “sex and gender lens” to all aspects of dementia research

17
Issues in Indigenous Dementia Care
1.4 million Indigenous Peoples in Canada have 3X the incidence of dementia in old age relative to other Canadians
• Why?
➢ Genetics?
➢ Stress? Poverty?
➢ Vascular disease and vascular risk factors?
➢ Epigenetics to be worked out?
➢ Other factors?
• Can we find more accurate ways to detect and diagnose dementia in this population?: Development of CICA - The Canadian Indigenous Cognitive Assessment
• Can we find ways to combine “Western” medicine approaches with traditional medicine to best give treatment?

18
Promotion of Research in Indigenous Populations
Dr. Jennifer WalkerCRC Chair In Indigenous Health
School of Rural and Northern HealthLaurentian University
CCNA Lead of ICH
Indigenous Cognitive Health (ICH) Team and Program
Goals:
• Building Capacity - we need more researchers from Indigenous communities
• Building appropriate training
• Building our ability to do research in Indigenous communities, and sensitivity to cultural issues
• Interaction with all the teams

Impact of CCNA over Past 7 Years
General Existence Effects
• CCNA has created a national dementia research community
in Canada now based on interactive and collaborating teams
rather than individual researchers
• Impressive interaction at meetings, webinars – there is really
now a Canadian dementia research community
• Leveraging has occurred
• Synergy has occurred

COMPASS-ND Information Leaflet
Recruitment at 29 sites across Canada

Recruitment Targets for COMPASS-ND
21
Diagnosis Number
Subjective Cognitive Impairment 200
Mild Cognitive Impairment (MCI) 300
Subcortical Ischemic Vascular MCI 200
Mild AD 150
Dementia of mixed etiology 200
Lewy Body Disease/Parkinson's
Dementia/Parkinson's MCI200
Frontotemporal dementia spectrum
(behavioural variant, primary progressive aphasia, progressive supranuclear palsy, corticobasal syndrome)
60

22
MCI
SCI
AD
LBD
FTDVCI
Mixed
If narrowly-focused criteria,
will produce homogeneous
groups that represent a
small fraction of the
dementia population
May exclude co-morbidities
and mixed dementias
ADNI example
Choice of Inclusion and Exclusion Criteria

23
Choice of Inclusion and Exclusion Criteria
MCI
SCI
AD
LBD
FTD
VCI
Mixed
Broadly inclusive
criteria will produce
heterogeneous groups
that cover the entire
dementia population
Include almost all co-
morbidities and mixed
dementias
More ecological and
“real-life” dementia
=Approach we are
using in COMPASS-
ND

24
Clinical Cohorts Study Flow
1. Recruitment
into CCNA
2. Informed
Consent
Signed
3. History,
Physical &
Cognitive
Evaluation
▪ Assess inclusion/exclusion criteria
▪ Demographics, medical/surgical history
▪ Sensory Assessment (Hearing, Vision,
Olfaction)
▪ Grip strength & Gait Assessment▪ Physical/Neurological examination
4.
Questionnaires
▪ General and Mental health
▪ Social Network
▪ Nutrition
▪ Sleep
▪ Physical Activity
5.
Psychometric
Testing▪ National battery
6. Biosamples
6A. Blood 6B. Saliva and
fecal sample6C. CSF
7. Sample
Processing
8. Sample
Shipping to
Biobank
9. MRI Imaging
Acquisition
10. MRI IT &
Databasing
C-Brain LORIS
11. Brain
Donation
Program and
follow-up in
Clinic

Repository /download
Data types: behavior, clinical, imaging, genetic
On-line remote MRI browser
Data querying GUI (volumes, surfaces, behavior)
e.g. NIH database of normal brain development
Acquisition management
Project management tools
Double data entry/ range checking
Automated 3D image QC
Java-based remote 3D image QC
150 behavioral instruments
MANTIS bug-tracking
Analysis pipelines
External pipelines for analysis (MNI, SPM, FSL, LONI,
AFNI). Integrated with grid-computing networks (CBRAIN,
NeuGrid)
25
80 man-years of development
Web-based, secure data transfer of multi-site data
Generalized open-source MYSQL architecture - flexible,
extensible
Applications in development, neurodegeneration (US, Europe,
Asia)
LORIS
LORIS Database

Clinical Visit – Test Battery
26

Core Cognitive Battery for Clinical Cohorts
27
=in CLSA
=in ONDRI
=in both CIMA-Q &
ONDRI
Tests used in other groups
=in CIMA-Q
=in both CLSA & ONDRI
=in both CLSA & CIMA-Q
Pre-Morbid IQ WAIS III Vocabulary
Memory RAVLT
Brief Visuospatial Memory test
CCNA-CIMA-Q Face-Name Association
Digit Symbol incidental recall
Envelope test
Executive function DKEFS Colour-Word Interference
DKEFS Phonemic Fluency
CCNA-CIMA-Q sentence inhibition task
Trailmaking
Reaction time test
Language Animal Fluency
NACC Language battery
Attention/Psychomotor speed WAIS-III Digit Symbol-Coding
Digit span F & B
General MoCA
Visuoperceptual Line Orientation
Object Decision test
VOSP letter completion
=in CLSA, CIMA-Q & ONDRI

CCNA Genetics in COMPASS-ND
Genetics Team:
Ekaterina
Rogaeva/Ziv Gan-Or
Kathy
Siminovitch-Clinical
Genomics Centre, Mt.
Sinai, Toronto
▪ Infinium Global Screening Array-24 v3.0 BeadChip for each subject- will analyze 210,000 neurological SNPs.
▪ Data stored in LORIS
▪ Pax tube for RNA-Seq
▪ Epigenomics
Genetics Platform

MRI Imaging
29
CDIPCanadian Dementia Imaging Protocol
www.cdip-pcid.ca

30
COMPASS-ND will provide
Biosamples for all Canadian
researchers:
▪ Plasma/serum
▪ Saliva
▪ CSF
▪ Urine
▪ Microbiome (fecal, oral swabs)
(Being analyzed by Dr.
Brett Finlay and colleagues at
UBC)

Biosample Storage and Shipping
31
▪ Aliquoted biosamples are sent from
sites to the biorepository in
Edmonton via cryoshipper on a
quarterly basis.
▪ Frozen, to be accessed and used
by Canadian scientists and their
students over coming years.

Blood Core Analyses
32
▪ General health
• Complete Blood Count• Electrolytes (Na, K, CL, bicarbonate)
• Creatinine, Urea• Liver function (AST, ALT, ALP, bilirubin)• B12
• Calcium• Albumin
• 25-OH vitamin D level• Ferritin
• Glycosylated Hemoglobin
• Insulin level• Glucose
• Homocysteine -increased plasma
homocysteine level is a strong, independent risk factor for the development of dementia and Alzheimer's disease
• Cystatin-C-variation in an amyloidogenic cysteine protease inhibitor affect AD risk
• VEGF Vascular endothelial growth factor –role in angiogenesis, neuroprotection.
▪ Inflammation
• Insulin like growth factor-1
• Tumour necrosis factor-alpha
• Interleukin-6
• C-reactive protein
▪ Lipidomics
• Total Cholesterol
• Triglycerides
• HDL-C
• LDL-C
• apoA-1
• apoB
▪ Synaptic function, plasticity
• BDNF levels
(Being carried out at Jewish General Hospital Clinical Labs)
New: Simoa Serum samples for NfL, serum phospho-tau181, Abeta42/40,GFAP- lab of Dr. Cheryl Wellington, UBC

Blood Core Analyses (cont’d.)
33
Hormones Oxidative Stress
• ACTH
• Androstenedione
• Luteinizing Hormone
• FSH
• DHEA-S
• Estrone Sulphate
• Testosterone (total)
• DHT
• Estrone
• Estradiol
• Prolactin
• Cortisol
• SHBG
• TSH
• Vitamin E
• Alpha-1 antitrypsin
• Biliverdin
• ferritin

CSF Core Analyses
34
(To be carried out at Judes Poirier’s laboratory at Douglas Mental
Health University Institute)
Abeta 42
Total tau
Phospho tau 181
Alpha Synuclein

Microbiome Analyses
(Being carried out by B. MacVicar and B. Finlay at UBC)
▪ Alteration in the human microbiome in gut and mouth may be an unappreciated factor in various NDD. New frontier.
▪ Reflects inflammatory state
▪ GI tract bacteria can influence host innate-immune, neuroinflammatory-, neuromodulatory- and neurotransmission-functions
▪ Mouth biology and AD risk?

36
Big Data on Dementia ̶ COMPASS-ND
COMPASS-ND will provide deeply phenotyped cohorts through:
• Extensive clinical information gathered
• Genetic information: Infinium Global Screening Array-24 v3.0 BeadChip
for each subject. = 240,000 SNP’s (all known neurological genes)
• 3T MRI-standardized MRI imaging protocol via Canadian Dementia Imaging Platform (CDIP)
• Baseline volumetrics, hippocampal volumes
• Neuropsychology → national battery
• Microbiome assessment
• Longitudinal follow-up planned
• Serum biomarkers
• Brain donation program, standardized neuropathology protocol (eventually brain tissue will be available for studies)

5/4/2021
COMPASS-ND Data
• First 400 subjects now released on LORIS database.
• Data on LORIS will be released regularly over coming year.
• Completion of subject recruitment December 2021.
• Release of full dataset to CCNA members by Feb 2022
• There are a set of 100 “quarantined projects” already being written by CCNA writing groups…privileged priority.
• All other topics/questions can be addressed/written by Canadian scientists and their students. 12 months after full release of data there will be “open science” availability to international community.
• Planned longitudinal follow-up of all subjects after three years.
• Brain bank and brain collection protocol now established at Douglas Mental Health University Institute.
• We encourage SPA students to look into LORIS accounts via CCNA member labs.

38
COMPASS-ND will provide a
normative comparison group -
elderly subjects screened for
normal cognition - screen out
MCI, SCI…no memory
complaints:
▪ Planned 200 MRI studies within
CLSA sub-cohort (E. Smith)
▪ Planned normal CCNA neuropsych
normative group of 600 (R. Dixon,
N. Phillips to coordinate this)

What we can get from a normal comparison group:
▪ Norms for MRI volumes
▪ Imaging norms
▪ Canadian CCNA neuropsychology battery norms
▪ Biosamples - norms for CSF, for saliva
metabolomics, …
All in appropriate elderly Canadian populations

40
Conclusion
•Many opportunities for students interested in dementia within CCNA•Students can join via their lab/faculty member•Some students have joined CCNA independently•Networking, mentorship, access to data and samples
www.ccna-ccnv.ca





























