Embed Size (px)
Citation preview
CCFP MedleyCCFP Medley
Rheumatological EmergenciesVavular HD & Endocarditis
Spinal #’s
Rheumatological EmergenciesVavular HD & Endocarditis
Spinal #’s
Rheumatology in the EdRheumatology in the Ed
• Acute Joint• Septic arthritis• Septic bursitis• SLE in the ED• RA in the ED
• Acute Joint• Septic arthritis• Septic bursitis• SLE in the ED• RA in the ED
Acute Painful JointAcute Painful Joint• Periarticular?
– Bursitis, tendonitis, cellulitis
• Mono or Polyarticular?– Mono needs to be sorted in out ED– Septic, gout, pseudogout, OA, trauma,
hemarthrosis, gonococcal
• Polyarthritis– Admit Med if systemically unwell, Rheum
triage for urgent referral if can go home
• Periarticular?– Bursitis, tendonitis, cellulitis
• Mono or Polyarticular?– Mono needs to be sorted in out ED– Septic, gout, pseudogout, OA, trauma,
hemarthrosis, gonococcal
• Polyarthritis– Admit Med if systemically unwell, Rheum
triage for urgent referral if can go home

Septic arthritisSeptic arthritis
• Acute monoarthritis is septic until proven otherwise
• Acute monoarthritis is septic until proven otherwise
Who is at risk for SA?Who is at risk for SA?
• immunocompromised• RA and other inflammatory
arthritis (including gout)• Prosthetic joints• IVDU
• immunocompromised• RA and other inflammatory
arthritis (including gout)• Prosthetic joints• IVDU
Clinical FeaturesClinical Features
• Knee > hip > shoulder > wrist > ankle > elbow
• 20% afebrile on presentation
• Pain is remarkable and limitation of ROM significant unless prior Abx
• Knee > hip > shoulder > wrist > ankle > elbow
• 20% afebrile on presentation
• Pain is remarkable and limitation of ROM significant unless prior Abx
Diagnostic TestingDiagnostic Testing
• WBC– 15% not elevated in septic
• ESR/CRP– No discriminatory value
• Uric acid level– May be normal in acute gout or elevated in
septic arthritis
• Blood Cultures– Aren’t back in the ED– Only 50% positive
• WBC– 15% not elevated in septic
• ESR/CRP– No discriminatory value
• Uric acid level– May be normal in acute gout or elevated in
septic arthritis
• Blood Cultures– Aren’t back in the ED– Only 50% positive
Arthrocentesis in SAArthrocentesis in SA
• Arthrocentesis essential– Thin, turbid– Cell count 5000 - > 50000
• Only 50-70% > 50000
– >75% PMNs– Glucose < 50% serum– GS positive in 50-70%
• If unclear, ortho opinion, admit, cover with Abx until BC return
• Arthrocentesis essential– Thin, turbid– Cell count 5000 - > 50000
• Only 50-70% > 50000
– >75% PMNs– Glucose < 50% serum– GS positive in 50-70%
• If unclear, ortho opinion, admit, cover with Abx until BC return
Pitfalls in Synovial Fluid Interpretation
Pitfalls in Synovial Fluid Interpretation
• Early• Previous antibiotics• Immunosuppressed
• Synovial WBC’s 2000-5000 not uncommon
• Early• Previous antibiotics• Immunosuppressed
• Synovial WBC’s 2000-5000 not uncommon

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Septic BursitisSeptic Bursitis
• Olecranon and prepatellar common• Difficult distinction
– When septic usually peribursal swelling and erythema +/- cellulitis
• No standardized approach• Aspiration if concerned
– WBC > 5000 likely septic
• Septic? I&D, IV Abx, F/U HPTP• Indeterminate? Oral Abx, F/U
• Olecranon and prepatellar common• Difficult distinction
– When septic usually peribursal swelling and erythema +/- cellulitis
• No standardized approach• Aspiration if concerned
– WBC > 5000 likely septic
• Septic? I&D, IV Abx, F/U HPTP• Indeterminate? Oral Abx, F/U
SLE in the EDSLE in the ED
SLE in the EDSLE in the ED
• Fever– Immunocompromised
• Neuro– Seizures– CVA– Psychosis
• Lupus cerebritis
• CT head, LP R/O meningoencephalitis– Bacterial, fungal, TB, brain abscess all possible
• Fever– Immunocompromised
• Neuro– Seizures– CVA– Psychosis
• Lupus cerebritis
• CT head, LP R/O meningoencephalitis– Bacterial, fungal, TB, brain abscess all possible
SLE in the EDSLE in the ED• Cardiac
– Pericarditis• Effusions usually benign
– Myocarditis• Common, usually little clinical
manifestation
– CAD• Increased prevalence
• Cardiac– Pericarditis
• Effusions usually benign
– Myocarditis• Common, usually little clinical
manifestation
– CAD• Increased prevalence
SLE in the EDSLE in the ED
• Pulmonary– Pleural effusions– PE – Oppurtunistic infections– Lupus pneumonitis (Dx of exclusion)
• Chest pain/dyspnea in the SLE patient very serious complaint
• Pulmonary– Pleural effusions– PE – Oppurtunistic infections– Lupus pneumonitis (Dx of exclusion)
• Chest pain/dyspnea in the SLE patient very serious complaint
SLE in the EDSLE in the ED
• NSAIDS may worsen lupus nephritis
• NSAIDS may worsen lupus nephritis
RA in the EDRA in the ED• Fever
– Immunosuppressed
• Acute joint– Do not dismiss monoarthritis as RA
flare • Think septic joint first• They know their disease
• Fever– Immunosuppressed
• Acute joint– Do not dismiss monoarthritis as RA
flare • Think septic joint first• They know their disease
RA in the EDRA in the ED
• Cardiac– Increased predisposition to CAD
• Unclear• chronic inflammation, steroids accelerating
atherosclerosis, vasculitis
– Pericarditis/pericardial effusions in @40% of patients
• Neuro– Nerve entrapment and neuritis common
• Cardiac– Increased predisposition to CAD
• Unclear• chronic inflammation, steroids accelerating
atherosclerosis, vasculitis
– Pericarditis/pericardial effusions in @40% of patients
• Neuro– Nerve entrapment and neuritis common
RA in the EDRA in the ED
• Trauma– Neck pain & neuro signs
• Rupture of transverse ligament, displacement of odontoid
• Trauma– Neck pain & neuro signs
• Rupture of transverse ligament, displacement of odontoid
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Blood Culture ResultBlood Culture Result
• July 1st• Abnormal lab result
– Single BC + coag negative staph?
– Single BC + Staph aureus?
• July 1st• Abnormal lab result
– Single BC + coag negative staph?
– Single BC + Staph aureus?
Infective Endocarditis (IE)Infective Endocarditis (IE)
• Prosthetic HV • IVDU• PHx endocarditis• Rheumatic or CHD• Calcific degenerative valve dz• MVP
• Prosthetic HV • IVDU• PHx endocarditis• Rheumatic or CHD• Calcific degenerative valve dz• MVP
Clinical FeaturesClinical Features
• Very nonspecific (viral)• Think in repeated visit for fever NYD• Early, often no murmur• IVDU often no murmur • 30-40% some central neuro
symptoms• 30-40% peripheral cutaneous
findings
• Very nonspecific (viral)• Think in repeated visit for fever NYD• Early, often no murmur• IVDU often no murmur • 30-40% some central neuro
symptoms• 30-40% peripheral cutaneous
findings
IE: Clinical SuspicionIE: Clinical Suspicion
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
IE: Clnical SuspicionIE: Clnical Suspicion
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
IE: Clnical SuspicionIE: Clnical Suspicion
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
IE: Clnical SuspicionIE: Clnical Suspicion
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
IE: Diagnostic Work-upIE: Diagnostic Work-up
• Lab findings nonspecific– Leukocytosis <50%
• 3 sets of BC’s– 1st and last 1 hour apart– 90-95% positive unless prior Abx
• TEE vs TTE
• Lab findings nonspecific– Leukocytosis <50%
• 3 sets of BC’s– 1st and last 1 hour apart– 90-95% positive unless prior Abx
• TEE vs TTE
IE: Diagnostic CriteriaIE: Diagnostic Criteria
• Duke Criteria– 2 major or 1 major/3 minor or 5 minorMajor
BC + from at least 2ECHO evidence
MinorPredispositionFeverStigmata (cutaneous, conunctival etc.)Single + BCECHO abnormal not meeting criteria
• Duke Criteria– 2 major or 1 major/3 minor or 5 minorMajor
BC + from at least 2ECHO evidence
MinorPredispositionFeverStigmata (cutaneous, conunctival etc.)Single + BCECHO abnormal not meeting criteria
IE: ManagementIE: Management
• Febrile prosthetic valve patients or persistent fever in IVDU - err on admission
• Vanco + Gent• Ceftriaxone + Gent
• Febrile prosthetic valve patients or persistent fever in IVDU - err on admission
• Vanco + Gent• Ceftriaxone + Gent
Quick CaseQuick Case
• 67m, acute CP, SOB• Looks unwell, clinically CHF• III/VI murmur at apex• ECG acute anterior MI
• 67m, acute CP, SOB• Looks unwell, clinically CHF• III/VI murmur at apex• ECG acute anterior MI
Acute Valvular RuptureAcute Valvular Rupture
Acute MVR– Flash pulmonary edema– MI + pulm edema + MR murmur– no ECG evidence of LVH/LAE
• Tx CHF normally, STAT ECHO, cath and IABP, contact CV Surgery
Acute MVR– Flash pulmonary edema– MI + pulm edema + MR murmur– no ECG evidence of LVH/LAE
• Tx CHF normally, STAT ECHO, cath and IABP, contact CV Surgery
Severe ASSevere AS
• CHF + exertional syncope• Tenuous pre/afterload balance• 1cm/50mmHg• Medication change?
• Gentle fluid resus if hypotensive
• Cardiology admission– Assess if surgical candidate
• CHF + exertional syncope• Tenuous pre/afterload balance• 1cm/50mmHg• Medication change?
• Gentle fluid resus if hypotensive
• Cardiology admission– Assess if surgical candidate
Quick CaseQuick Case
• 70f, AoVR, near-synopal at home• Hypotensive, CHF
• 70f, AoVR, near-synopal at home• Hypotensive, CHF
Prosthetic ValveProsthetic Valve
• Type, location, age• Ask for surgical card• Almost all some degree of
narrowing– mild systolic murmur common
• Diastolic murmur always abnormal– failure
• Type, location, age• Ask for surgical card• Almost all some degree of
narrowing– mild systolic murmur common
• Diastolic murmur always abnormal– failure
Acute Valvular FailureAcute Valvular Failure
• Hypotension + new onset CHF in patient with known prosthetic valve– Leaflet failure in bioprosthetic– Thrombosis of mechanical valve
• STAT TTE, cardiology and CV surgery• Anticoagulation if thrombosed, some
advocate thrombolyzed
• Hypotension + new onset CHF in patient with known prosthetic valve– Leaflet failure in bioprosthetic– Thrombosis of mechanical valve
• STAT TTE, cardiology and CV surgery• Anticoagulation if thrombosed, some
advocate thrombolyzed
Valvular EmergenciesValvular Emergencies
• IE• Rupture of native valve• Critical AS• Acute failure of prosthetic valve
– Thrombosis– Mechanical breakdown
• Embolization– Debris, clot, actual valve structure
• Hemolysis
• IE• Rupture of native valve• Critical AS• Acute failure of prosthetic valve
– Thrombosis– Mechanical breakdown
• Embolization– Debris, clot, actual valve structure
• Hemolysis
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
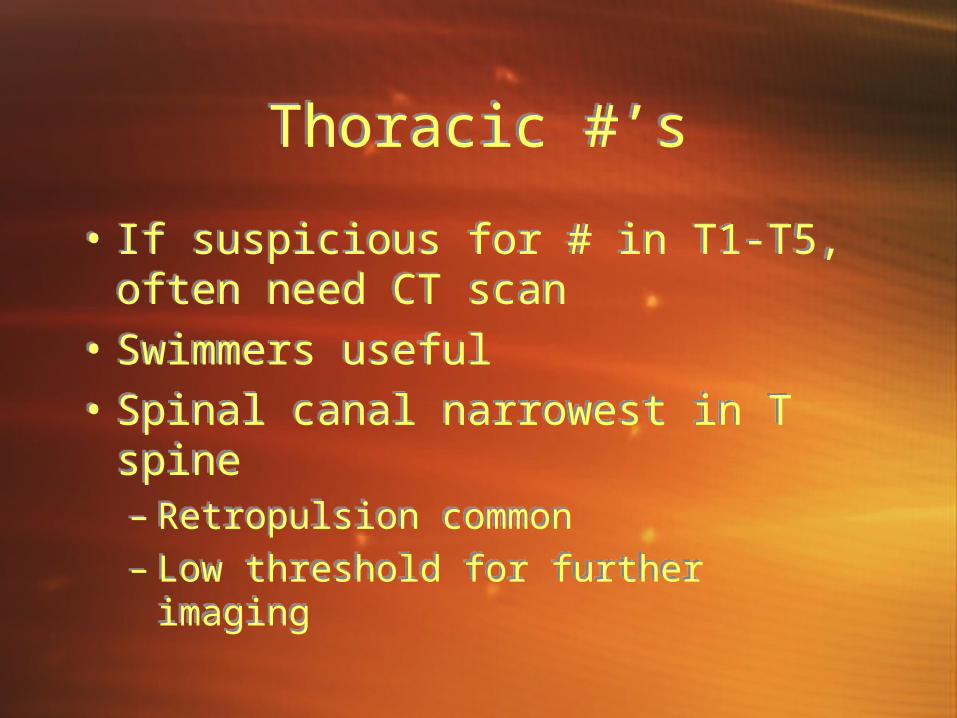
Thoracic #’sThoracic #’s
• If suspicious for # in T1-T5, often need CT scan
• Swimmers useful• Spinal canal narrowest in T spine
– Retropulsion common– Low threshold for further imaging
• If suspicious for # in T1-T5, often need CT scan
• Swimmers useful• Spinal canal narrowest in T spine
– Retropulsion common– Low threshold for further imaging
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
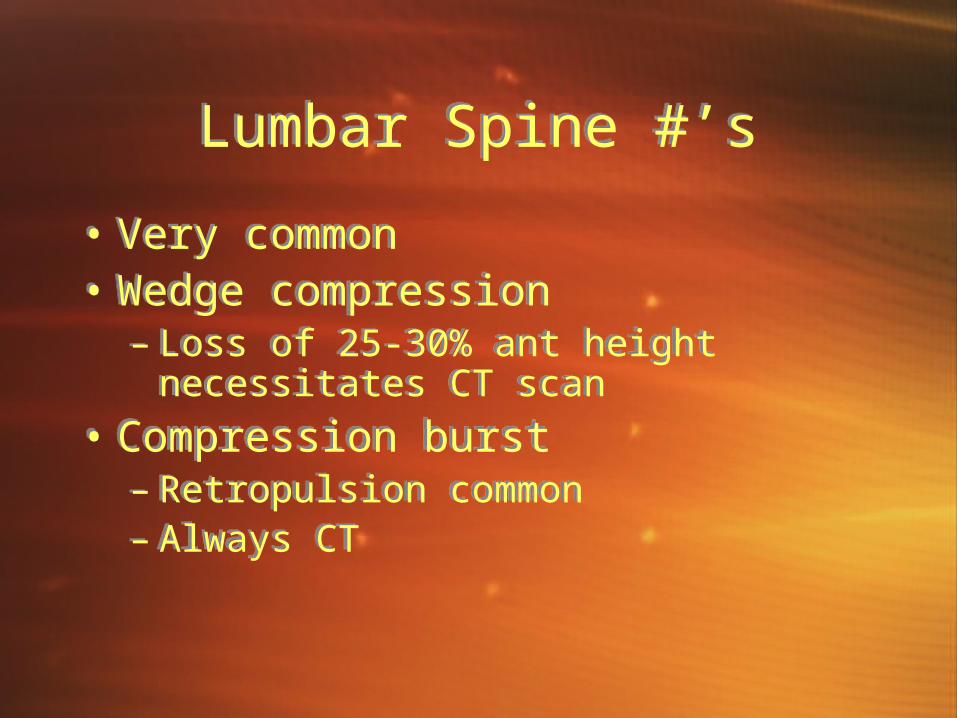
Lumbar Spine #’sLumbar Spine #’s
• Very common• Wedge compression
– Loss of 25-30% ant height necessitates CT scan
• Compression burst– Retropulsion common– Always CT
• Very common• Wedge compression
– Loss of 25-30% ant height necessitates CT scan
• Compression burst– Retropulsion common– Always CT
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
SummarySummary• Rheum
– Acute painful joint,– Septic Arthritis– SLE in ED– RA/CTD in ED
• Spine #’s– Review critical C spine #’s– T and L spine #’s
• Valvular Emergencies– IE– Acute MV rupture & critical AS– Prosthetic valve problems
• Rheum– Acute painful joint,– Septic Arthritis– SLE in ED– RA/CTD in ED
• Spine #’s– Review critical C spine #’s– T and L spine #’s
• Valvular Emergencies– IE– Acute MV rupture & critical AS– Prosthetic valve problems