Embed Size (px)
Citation preview
CCCCEEEENNNNLLLLEEEEEnd-of-Life Nursing Education ConsortiumEnd-of-Life Nursing Education ConsortiumEnd-of-Life Nursing Education ConsortiumEnd-of-Life Nursing Education Consortium
Module 1:Module 1:
Nursing Care at the Nursing Care at the End of LifeEnd of Life
EEEE LLLL NNNN EEEE CCCC
AgendaAgendaAgendaAgenda
• Review changes in how we age and dieReview changes in how we age and die• Hospice and palliative care – definitionsHospice and palliative care – definitions• Nursing homes and EOL careNursing homes and EOL care• Overview of death and dying in the VAOverview of death and dying in the VA• Nurses’ role in EOL careNurses’ role in EOL care
• Review changes in how we age and dieReview changes in how we age and die• Hospice and palliative care – definitionsHospice and palliative care – definitions• Nursing homes and EOL careNursing homes and EOL care• Overview of death and dying in the VAOverview of death and dying in the VA• Nurses’ role in EOL careNurses’ role in EOL care

EEEE LLLL NNNN EEEE CCCC
• Late 1800’sLate 1800’s• Early to mid 1900’sEarly to mid 1900’s
• Late 1800’sLate 1800’s• Early to mid 1900’sEarly to mid 1900’s
The Need for Improved Care The Need for Improved Care at the End of Lifeat the End of LifeThe Need for Improved Care The Need for Improved Care at the End of Lifeat the End of Life
EEEE LLLL NNNN EEEE CCCC
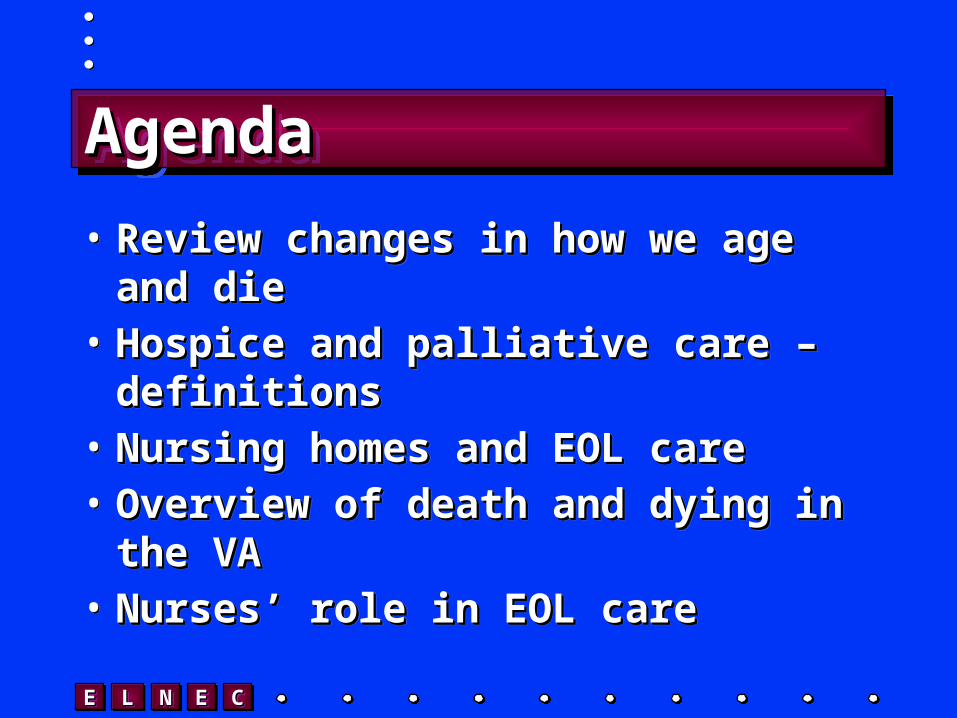
Cause of Death/Demographic and Social TrendsCause of Death/Demographic and Social Trends
Early 1900s Current
Medicine's Focus Comfort Cure
Cause of Death Infectious Diseases/Communicable Diseases
Chronic Illnesses
Death rate 1720 per 100,000(1900)
865 per 100, 000(1997)
Average LifeExpectancy
50 76
Site of Death Home Institutions
Caregiver Family Strangers/Health Care Providers
Disease/DyingTrajectory
Relatively Short Prolonged
EEEE LLLL NNNN EEEE CCCC
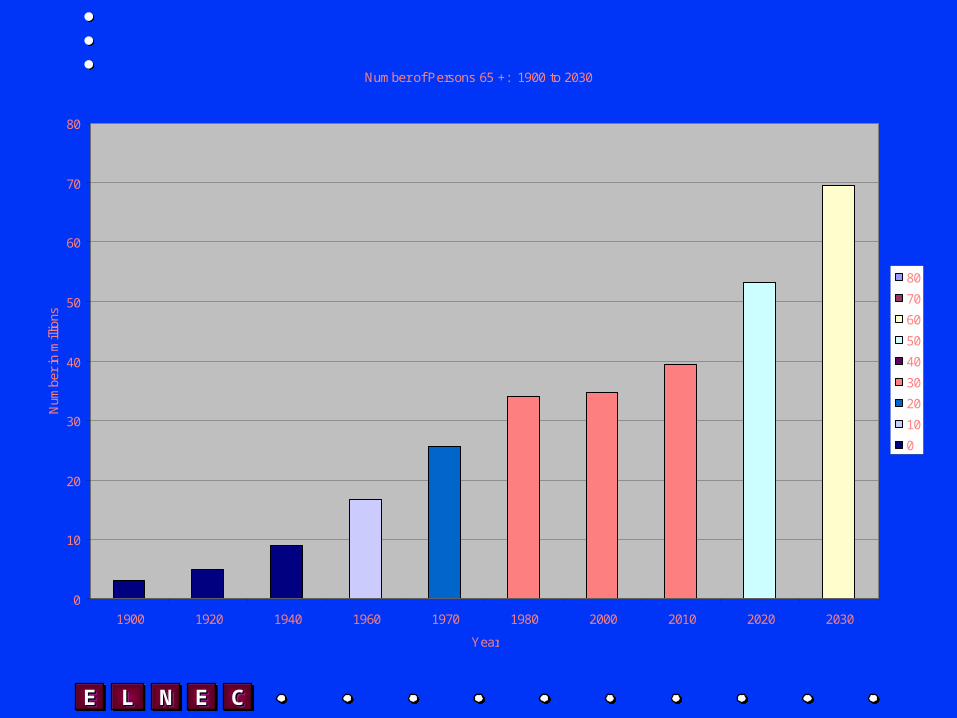
Number of Persons 65 +: 1900 to 2030
0
10
20
30
40
50
60
70
80
1900 1920 1940 1960 1970 1980 2000 2010 2020 2030
Year
Num
ber
in m
illio
ns
80
70
60
50
40
30
20
10
0

EEEE LLLL NNNN EEEE CCCC
Fantasy DeathFantasy DeathFantasy DeathFantasy Death
• Where are you?Where are you?• Who, if anybody is with you?Who, if anybody is with you?• What is important to you?What is important to you?
• Where are you?Where are you?• Who, if anybody is with you?Who, if anybody is with you?• What is important to you?What is important to you?
What is missing from this picture?
EEEE LLLL NNNN EEEE CCCC
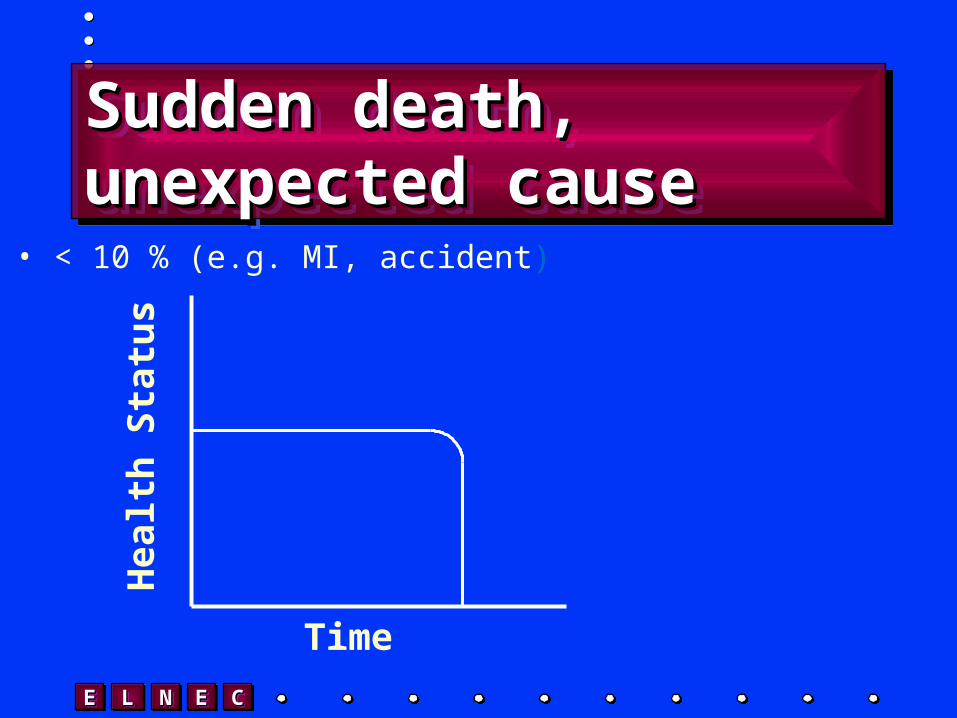
Sudden death, unexpected Sudden death, unexpected causecauseSudden death, unexpected Sudden death, unexpected causecause
• < 10 % (e.g. MI, accident)
Hea
lth
Sta
tus
Time

EEEE LLLL NNNN EEEE CCCC
Steady decline,Steady decline,short terminal phaseshort terminal phaseSteady decline,Steady decline,short terminal phaseshort terminal phase
Hea
lth
Sta
tus
Time
Decline
EEEE LLLL NNNN EEEE CCCC
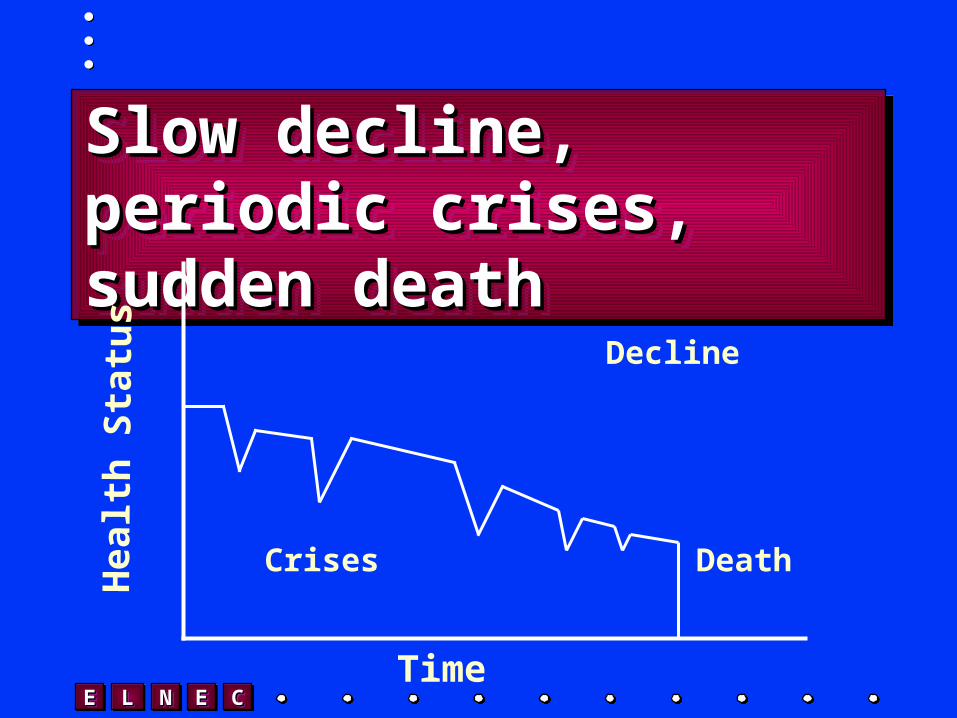
Slow decline, periodic crises, Slow decline, periodic crises, sudden deathsudden deathSlow decline, periodic crises, Slow decline, periodic crises, sudden deathsudden death
Hea
lth
Sta
tus
Time
Crises Death
Decline

EEEE LLLL NNNN EEEE CCCC
Death and Dying in America (cont.)Death and Dying in America (cont.)Death and Dying in America (cont.)Death and Dying in America (cont.)
• Disparity between Disparity between the way people the way people die/the way they die/the way they want to diewant to die
• Patient/family Patient/family perspectiveperspective
• Disparity between Disparity between the way people the way people die/the way they die/the way they want to diewant to die
• Patient/family Patient/family perspectiveperspective
EEEE LLLL NNNN EEEE CCCC
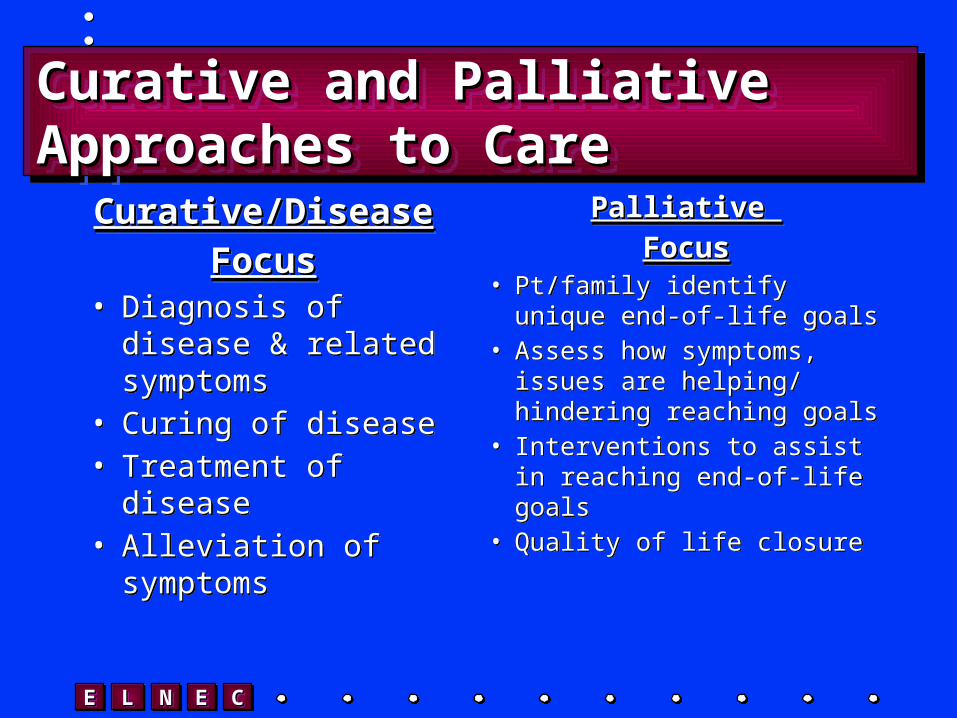
Curative and Palliative Approaches to Curative and Palliative Approaches to CareCareCurative and Palliative Approaches to Curative and Palliative Approaches to CareCare
Curative/DiseaseCurative/Disease
FocusFocus• Diagnosis of disease
& related symptoms• Curing of disease• Treatment of disease• Alleviation of
symptoms
Curative/DiseaseCurative/Disease
FocusFocus• Diagnosis of disease
& related symptoms• Curing of disease• Treatment of disease• Alleviation of
symptoms
Palliative Palliative
FocusFocus• Pt/family identify unique
end-of-life goals• Assess how symptoms,
issues are helping/ hindering reaching goals
• Interventions to assist in reaching end-of-life goals
• Quality of life closure
Palliative Palliative
FocusFocus• Pt/family identify unique
end-of-life goals• Assess how symptoms,
issues are helping/ hindering reaching goals
• Interventions to assist in reaching end-of-life goals
• Quality of life closure

EEEE LLLL NNNN EEEE CCCC
Principles of Hospice and Principles of Hospice and Palliative CarePalliative CarePrinciples of Hospice and Principles of Hospice and Palliative CarePalliative Care
• HospiceHospice
• Palliative CarePalliative Care
• HospiceHospice
• Palliative CarePalliative Care
EEEE LLLL NNNN EEEE CCCC
Philosophy and Principles of Philosophy and Principles of Hospice and Palliative CareHospice and Palliative CarePhilosophy and Principles of Philosophy and Principles of Hospice and Palliative CareHospice and Palliative Care
• Philosophy of Philosophy of carecare
• Goals of careGoals of care
• Philosophy of Philosophy of carecare
• Goals of careGoals of care

EEEE LLLL NNNN EEEE CCCC
Palliative CarePalliative CarePalliative CarePalliative Care
Curative Focus:Disease-specific Treatments
Palliative Focus:Comfort/Supportive Treatments
Bereavement Support

EEEE LLLL NNNN EEEE CCCC
General Principles of General Principles of Palliative CarePalliative CareGeneral Principles of General Principles of Palliative CarePalliative Care
• Patient and family as unit of carePatient and family as unit of care• Attention to physical, psychological, Attention to physical, psychological,
social and spiritual needssocial and spiritual needs• Interdisciplinary team approachInterdisciplinary team approach
EEEE LLLL NNNN EEEE CCCC
General Principles (cont.)General Principles (cont.)General Principles (cont.)General Principles (cont.)
• Education and support of Education and support of patient and familypatient and family
• Extends across illnesses and Extends across illnesses and settingssettings
• Bereavement SupportBereavement Support

EEEE LLLL NNNN EEEE CCCC
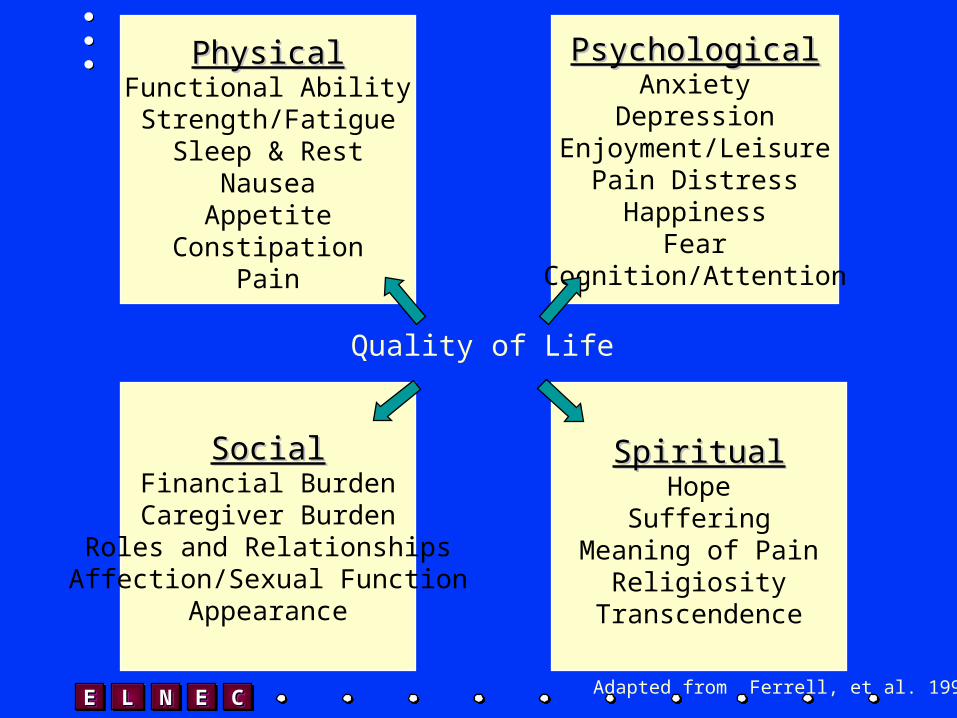
Model of Quality of LifeModel of Quality of LifeModel of Quality of LifeModel of Quality of Life
• Physical Well BeingPhysical Well Being• Psychological Well BeingPsychological Well Being• Social Well BeingSocial Well Being• Spiritual Well BeingSpiritual Well Being
• Physical Well BeingPhysical Well Being• Psychological Well BeingPsychological Well Being• Social Well BeingSocial Well Being• Spiritual Well BeingSpiritual Well Being
EEEE LLLL NNNN EEEE CCCC
PhysicalPhysicalFunctional AbilityStrength/Fatigue
Sleep & RestNauseaAppetite
ConstipationPain
PsychologicalPsychologicalAnxiety
DepressionEnjoyment/Leisure
Pain DistressHappiness
FearCognition/Attention
Quality of Life
SocialSocialFinancial BurdenCaregiver Burden
Roles and RelationshipsAffection/Sexual Function
Appearance
SpiritualSpiritualHope
SufferingMeaning of Pain
ReligiosityTranscendence
Adapted from Ferrell, et al. 1991
EEEE LLLL NNNN EEEE CCCC
• 1.6 million live in US nursing homes 1.6 million live in US nursing homes
• 17,000 long term care facilities. 17,000 long term care facilities.
• 90% of these people are over the age of 90% of these people are over the age of 6565
• 5.3 million NH residents projected by 20305.3 million NH residents projected by 2030References: National Center for Health Statistics, References: National Center for Health Statistics,
Highlights of Trends in the Health of Older Americans: United States, 1994, 1997Highlights of Trends in the Health of Older Americans: United States, 1994, 1997USA Today pg B1, Thurs, Sept 30, 1999 USA Today pg B1, Thurs, Sept 30, 1999
Graying of America -- Longterm careGraying of America -- Longterm care
EEEE LLLL NNNN EEEE CCCC
1.3 million nurses aides1.3 million nurses aides
$6.94 per hour -- average wage$6.94 per hour -- average wage
93% annualized turnover93% annualized turnover
The Hazards of Elder Care; Overexertion, Assault Put Aides at High Risk for InjuryThe Hazards of Elder Care; Overexertion, Assault Put Aides at High Risk for Injuryby Lorraine Adams in the Washington Post by Lorraine Adams in the Washington Post
October 31, 1999October 31, 1999
Caregiving in AmericaCaregiving in America
EEEE LLLL NNNN EEEE CCCC
Nursing Homes in CaliforniaNursing Homes in CaliforniaNursing Homes in CaliforniaNursing Homes in California
• Number of nursing homes and nursing Number of nursing homes and nursing home beds shrinking over last 10 yearshome beds shrinking over last 10 years
• 33% of nursing homes now operating at 33% of nursing homes now operating at a lossa loss
• With cuts to MediCal and Medicare, With cuts to MediCal and Medicare, unless something changes 97% will unless something changes 97% will operate at a lossoperate at a loss
• Number of nursing homes and nursing Number of nursing homes and nursing home beds shrinking over last 10 yearshome beds shrinking over last 10 years
• 33% of nursing homes now operating at 33% of nursing homes now operating at a lossa loss
• With cuts to MediCal and Medicare, With cuts to MediCal and Medicare, unless something changes 97% will unless something changes 97% will operate at a lossoperate at a loss
Something has to give…California Healthcare Foundation 7/03
EEEE LLLL NNNN EEEE CCCC
Veteran Deaths – Basic FactsVeteran Deaths – Basic FactsVeteran Deaths – Basic FactsVeteran Deaths – Basic Facts
• 29% of Americans dying each year are 29% of Americans dying each year are veteransveterans
• The majority of dying veterans are not enrolled The majority of dying veterans are not enrolled for by care by VAfor by care by VA
• A majority of enrolled veterans do not die in A majority of enrolled veterans do not die in VA facilitiesVA facilities
• A small shift of very sick and dying veterans A small shift of very sick and dying veterans not currently served by VA into the VA could not currently served by VA into the VA could swamp the systemswamp the system
• 29% of Americans dying each year are 29% of Americans dying each year are veteransveterans
• The majority of dying veterans are not enrolled The majority of dying veterans are not enrolled for by care by VAfor by care by VA
• A majority of enrolled veterans do not die in A majority of enrolled veterans do not die in VA facilitiesVA facilities
• A small shift of very sick and dying veterans A small shift of very sick and dying veterans not currently served by VA into the VA could not currently served by VA into the VA could swamp the systemswamp the system
EEEE LLLL NNNN EEEE CCCC
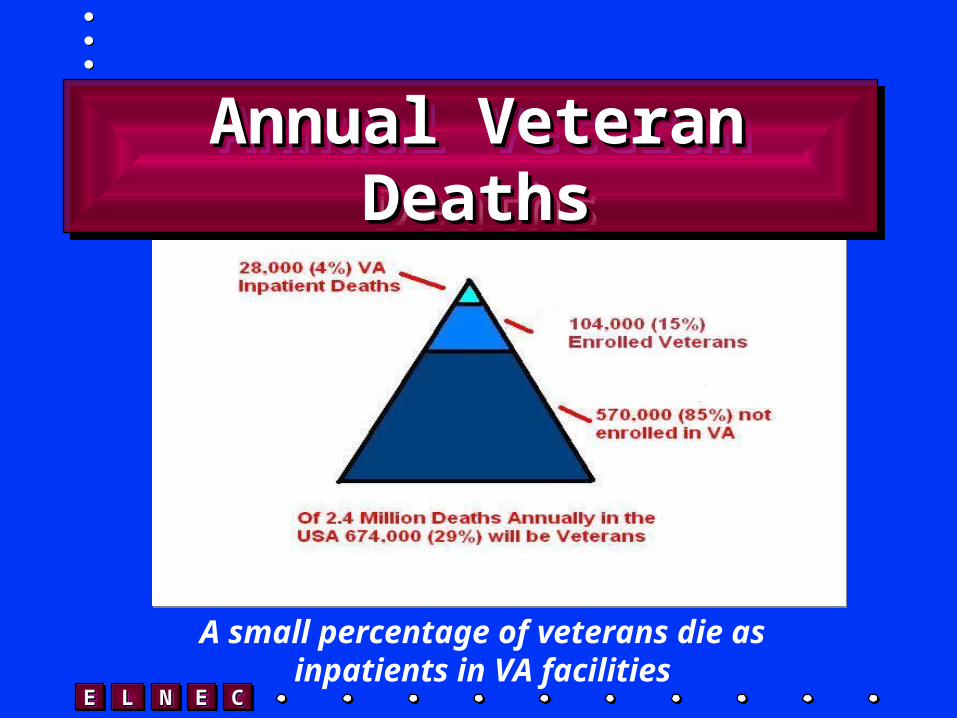
A small percentage of veterans die as inpatients in VA facilities
Annual Veteran DeathsAnnual Veteran DeathsAnnual Veteran DeathsAnnual Veteran Deaths

EEEE LLLL NNNN EEEE CCCC
National VA Mortality by VISN FY2000
0
500
1000
1500
2000
2500
3000
VISN
# Dea
ths b
y Loc
ation VAMC Total Deaths
Hospital Deaths
Nursing Home Deaths

EEEE LLLL NNNN EEEE CCCC
A Study of Death and Dying A Study of Death and Dying in VAin VAA Study of Death and Dying A Study of Death and Dying in VAin VA
James Breckenridge, PhD, James Hallenbeck, MDJames Breckenridge, PhD, James Hallenbeck, MD
Co-Principal InvestigatorsCo-Principal Investigators
VA Palo Alto HCSVA Palo Alto HCS
Preliminary data – do not citePreliminary data – do not cite
Funded by the Robert Wood Johnson FoundationFunded by the Robert Wood Johnson Foundation
EEEE LLLL NNNN EEEE CCCC
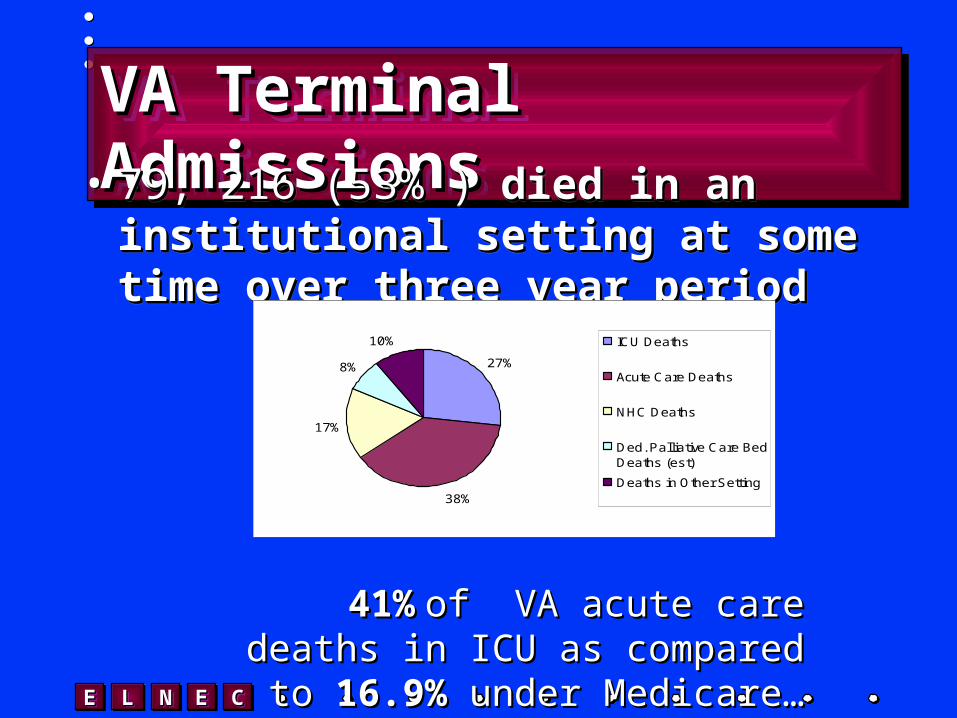
VA Terminal AdmissionsVA Terminal AdmissionsVA Terminal AdmissionsVA Terminal Admissions• 79, 216 (53% )79, 216 (53% ) died in an institutional died in an institutional
setting at some time over three year setting at some time over three year periodperiod
• 79, 216 (53% )79, 216 (53% ) died in an institutional died in an institutional setting at some time over three year setting at some time over three year periodperiod
27%
38%
17%
8%
10% ICU Deaths
Acute Care Deaths
NHC Deaths
Ded. Palliative Care BedDeaths (est)
Deaths in Other Setting
41%41% of VA acute care deaths of VA acute care deaths in ICU as compared to in ICU as compared to 16.9%16.9%
under Medicare…under Medicare…
EEEE LLLL NNNN EEEE CCCC
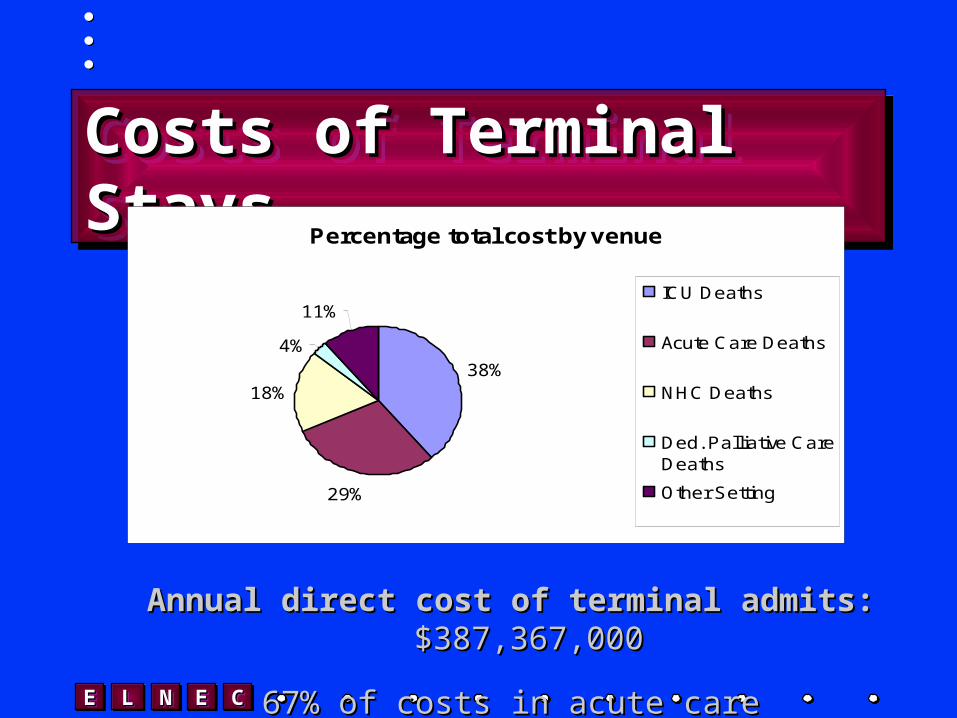
Costs of Terminal StaysCosts of Terminal StaysCosts of Terminal StaysCosts of Terminal StaysPercentage total cost by venue
38%
29%
18%
4%
11%ICU Deaths
Acute Care Deaths
NHC Deaths
Ded. Palliative CareDeaths
Other Setting
Annual direct cost of terminal admits:Annual direct cost of terminal admits: $387,367,000 $387,367,000
67% of costs in acute care67% of costs in acute care
EEEE LLLL NNNN EEEE CCCC
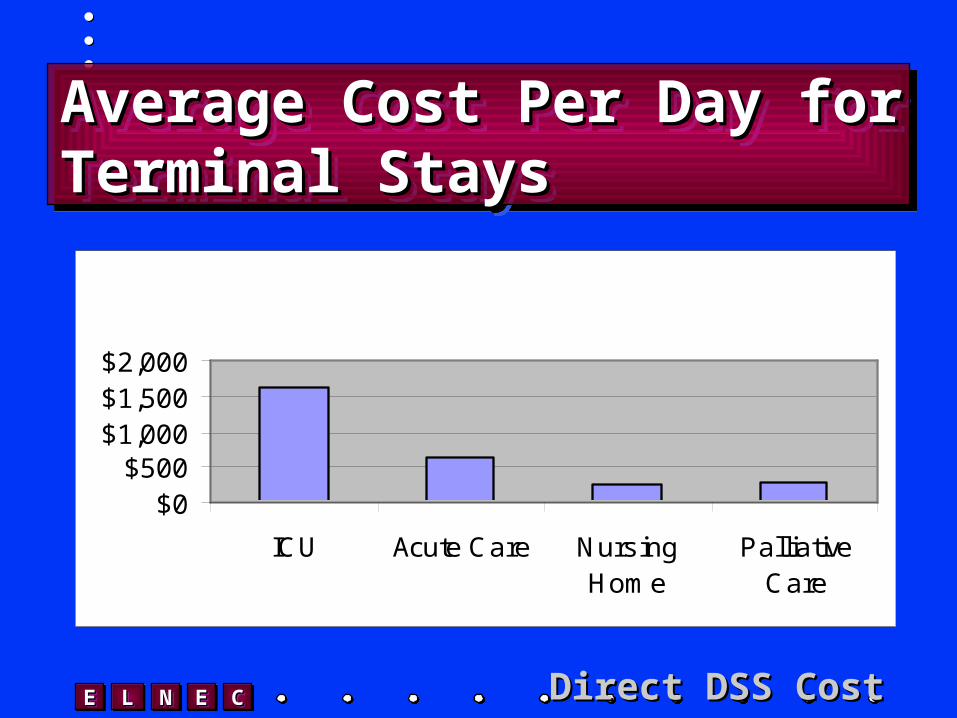
Average Cost Per Day for Average Cost Per Day for Terminal Stays Terminal Stays Average Cost Per Day for Average Cost Per Day for Terminal Stays Terminal Stays
$0$500
$1,000$1,500$2,000
ICU Acute Care NursingHome
PalliativeCare
Direct DSS CostDirect DSS Cost
EEEE LLLL NNNN EEEE CCCC
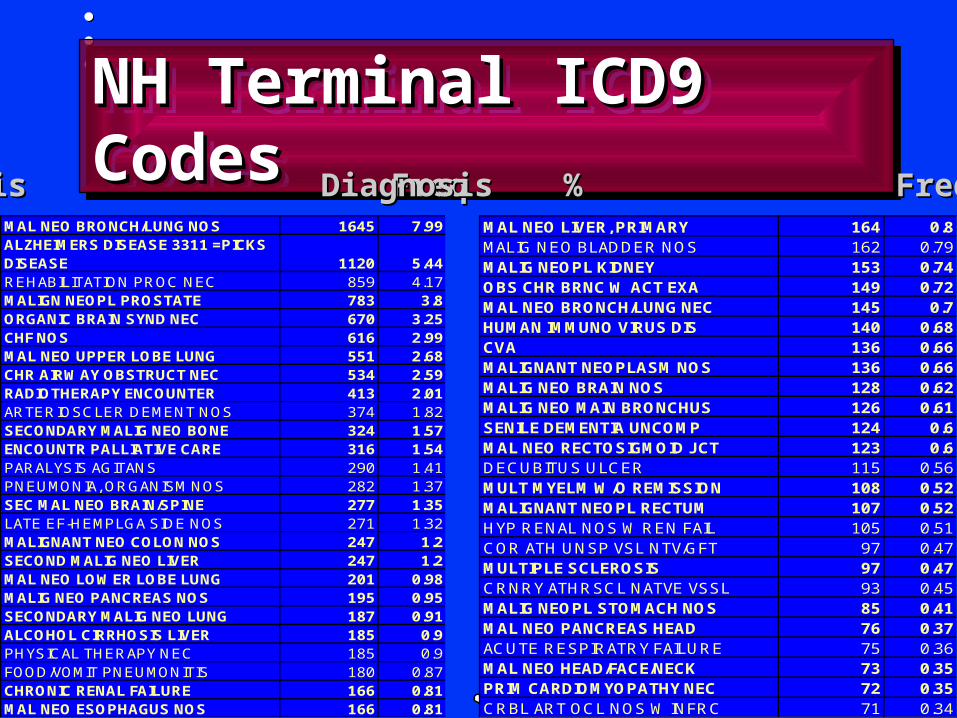
NH Terminal ICD9 CodesNH Terminal ICD9 CodesNH Terminal ICD9 CodesNH Terminal ICD9 Codes
MAL NEO BRONCH/LUNG NOS 1645 7.99ALZHEIMERS DISEASE 3311 =PICKS DISEASE 1120 5.44REHABILITATION PROC NEC 859 4.17MALIGN NEOPL PROSTATE 783 3.8ORGANIC BRAIN SYND NEC 670 3.25CHF NOS 616 2.99MAL NEO UPPER LOBE LUNG 551 2.68CHR AIRWAY OBSTRUCT NEC 534 2.59RADIOTHERAPY ENCOUNTER 413 2.01ARTERIOSCLER DEMENT NOS 374 1.82SECONDARY MALIG NEO BONE 324 1.57ENCOUNTR PALLIATIVE CARE 316 1.54PARALYSIS AGITANS 290 1.41PNEUMONIA, ORGANISM NOS 282 1.37SEC MAL NEO BRAIN/SPINE 277 1.35LATE EF-HEMPLGA SIDE NOS 271 1.32MALIGNANT NEO COLON NOS 247 1.2SECOND MALIG NEO LIVER 247 1.2MAL NEO LOWER LOBE LUNG 201 0.98MALIG NEO PANCREAS NOS 195 0.95SECONDARY MALIG NEO LUNG 187 0.91ALCOHOL CIRRHOSIS LIVER 185 0.9PHYSICAL THERAPY NEC 185 0.9FOOD/VOMIT PNEUMONITIS 180 0.87CHRONIC RENAL FAILURE 166 0.81MAL NEO ESOPHAGUS NOS 166 0.81
MAL NEO LIVER, PRIMARY 164 0.8MALIG NEO BLADDER NOS 162 0.79MALIG NEOPL KIDNEY 153 0.74OBS CHR BRNC W ACT EXA 149 0.72MAL NEO BRONCH/LUNG NEC 145 0.7HUMAN IMMUNO VIRUS DIS 140 0.68CVA 136 0.66MALIGNANT NEOPLASM NOS 136 0.66MALIG NEO BRAIN NOS 128 0.62MALIG NEO MAIN BRONCHUS 126 0.61SENILE DEMENTIA UNCOMP 124 0.6MAL NEO RECTOSIGMOID JCT 123 0.6DECUBITUS ULCER 115 0.56MULT MYELM W/O REMISSION 108 0.52MALIGNANT NEOPL RECTUM 107 0.52HYP RENAL NOS W REN FAIL 105 0.51COR ATH UNSP VSL NTV/GFT 97 0.47MULTIPLE SCLEROSIS 97 0.47CRNRY ATHRSCL NATVE VSSL 93 0.45MALIG NEOPL STOMACH NOS 85 0.41MAL NEO PANCREAS HEAD 76 0.37ACUTE RESPIRATRY FAILURE 75 0.36MAL NEO HEAD/FACE/NECK 73 0.35PRIM CARDIOMYOPATHY NEC 72 0.35CRBL ART OCL NOS W INFRC 71 0.34
Diagnosis Freq %Diagnosis Freq %Diagnosis Freq %Diagnosis Freq %
EEEE LLLL NNNN EEEE CCCC
VA Budget for EOL CareVA Budget for EOL CareVA Budget for EOL CareVA Budget for EOL Care
Of approximately Of approximately $17,000,000,000 allocated per $17,000,000,000 allocated per year by VHA for clinical care year by VHA for clinical care
10%10%
is for care in the last year of is for care in the last year of lifelife For 1.3% of For 1.3% of
enrolled veterans…enrolled veterans…

EEEE LLLL NNNN EEEE CCCC
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
National Palo Alto Lebanon Dayton
National vs three stations with palliative care units
FY 2000 Inpatient Deaths by Location
ICU (all)
General Medicine
Intermediate Medicine
Nursing Home
EEEE LLLL NNNN EEEE CCCC
Opportunities for GrowthOpportunities for GrowthOpportunities for GrowthOpportunities for Growth
• The last phase of life provides continued opportunities for positive growth in the face of suffering
• The last phase of life provides continued opportunities for positive growth in the face of suffering
EEEE LLLL NNNN EEEE CCCC
Extending Palliative Care Extending Palliative Care Across SettingsAcross SettingsExtending Palliative Care Extending Palliative Care Across SettingsAcross Settings
• Nurses as the Nurses as the constantconstant
• Expanding the Expanding the concept of healingconcept of healing
• Role of the nurseRole of the nurse
• Nurses as the Nurses as the constantconstant
• Expanding the Expanding the concept of healingconcept of healing
• Role of the nurseRole of the nurse
EEEE LLLL NNNN EEEE CCCC
Nurses’ Role in EOL CareNurses’ Role in EOL CareNurses’ Role in EOL CareNurses’ Role in EOL Care
• Nurse = “nurture” a good fit for EOL Nurse = “nurture” a good fit for EOL carecare
• Like other disciplines, necessary Like other disciplines, necessary knowledge and skills for EOL care knowledge and skills for EOL care neglected in traditional trainingneglected in traditional training
• Great job satisfaction possibleGreat job satisfaction possible
• Nurse = “nurture” a good fit for EOL Nurse = “nurture” a good fit for EOL carecare
• Like other disciplines, necessary Like other disciplines, necessary knowledge and skills for EOL care knowledge and skills for EOL care neglected in traditional trainingneglected in traditional training
• Great job satisfaction possibleGreat job satisfaction possible

EEEE LLLL NNNN EEEE CCCC
ConclusionConclusionConclusionConclusion
• Quality end of life care addresses Quality end of life care addresses Quality of Life concernsQuality of Life concerns
• Increased Nursing knowledge is Increased Nursing knowledge is essentialessential
• Nursing homes becoming Nursing homes becoming thethe major venue for EOL care in USmajor venue for EOL care in US

EEEE LLLL NNNN EEEE CCCC