-
7/21/2019 CBS Cambodia
1/9
Community-based surveillance: a pilot study from rural
Cambodia
Sophal Oum1, Daniel Chandramohan2 and Sandy Cairncross2
1 Ministry of Health, Phnom Penh, Cambodia2 Department of
Infectious and Tropical Diseases, London School of Hygiene and
Tropical Medicine, London, UK
Summary objective This study seeks to assess the performance of
a community-based surveillance system
(CBSS), developed and implemented in seven rural communes in
Cambodia from 2000 to 2002 to
provide timely and representative information on major health
problems and life events, and so permitrapid and effective control
of outbreaks and communicable diseases in general.
methods Lay people were trained as Village Health Volunteers
(VHVs) to report suspected
outbreaks, important infectious diseases, and vital events
occurring in their communities to local health
staff who analysed the data and gave feedback to the volunteers
during their monthly meetings.results Over 2 years of its
implementation, the system was able to detect outbreaks early,
regularly
monitor communicable disease trends, and to provide continuously
updated information on pregnancies,
births and deaths in the rural areas. In addition, the system
triggered effective responses from bothhealth staff and VHVs for
disease control and prevention and in outbreaks.
conclusion A CBSS can successfully fill the gaps of the current
health facility-based disease sur-
veillance system in the rapid detection of outbreaks, in the
effective monitoring of communicable dis-
eases, and in the notification of vital events in rural
Cambodia. Its replication or adaptation for use in
other rural areas in Cambodia and in other developing countries
is likely to be beneficial and cost-effective.
keywords community based surveillance, village health worker,
outbreak, communicable disease
control, Cambodia
Introduction
The World Health Organization asserts that effective
communicable disease control relies on effective response
systems, and effective response systems rely on effective
disease surveillance (WHO 2000). Routine health facility
based disease surveillance systems, such as those on which
most developing countries depend, could provide neither a
complete nor a representative picture of health problems inthe
communities because patients who cannot get access to
public health facilities or who choose not to use them arenot
reported by these systems. In order to overcome this
limitation of facility-based health information systems,
community-based surveillance systems (CBSS), based upona network
of lay people involved in the systematic
detection and reporting of health-related events from their
community, have been employed in a variety of settings.
The operational characteristics and the performance of
these CBSS have varied. For example, the type of data
collected has varied, depending on the objectives of each
CBSS. It has included the incidence of specific
infectiousdiseases such as Guinea worm infection (Cairncrosset
al.
1999), yaws (Anselmiet al.1995), malaria (Ruebushet al.
1994; Ghebreyesus et al. 2000), and tuberculosis (Bala-
subramanianet al.1995); pregnancy outcomes (Ahluwaliaet
al.1999); nutritional status of children (Valyaseviet al.
1995); and vital events (Jaravaza et al.1982). CBS systems
have been shown to provide useful information formonitoring
disease control programmes (Cairncross et al.
1996; Ghebreyesus et al. 2000; Howard-Grabman 2000).However,
these programmes have each focussed on a single
disease and thus did not maximize the value of scarce
resources available at the peripheral level. A CBSS target-ing
all common diseases and vital events would be more
appropriate and resource-efficient (Manderson 1992;
Cairncrosset al. 1996). In this paper, we report the
experience of a CBSS in rural Cambodia, including its
development and feasibility, its performance in terms of
Tropical Medicine and International Health
volume 10 no 7 pp 689697 july 2005
2005 Blackwell Publishing Ltd 689
-
7/21/2019 CBS Cambodia
2/9
sensitivity and positive predictive value, and its
usefulness
to local health services.
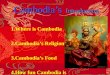
Materials and methodsA CBSS has been developed and implemented
since July
2000 in seven rural communes located in four provinces in
Cambodia (Figure 1). The four provinces chosen for this
pilot study were among those in the Border MalariaControl
Project funded by the European Commission,
which provided financial support for the surveillance
system. The seven communes comprised 52 villages and
had a total population of about 30 000 inhabitants in the
year 2000. They were served by four health centres, eachwith a
catchment population of 700010 000, and by four
referral hospitals, each serving about 10 such catchments.
Other providers of health care included traditional healers,
private practitioners, Traditional Birth Attendants, anddrug
sellers.
The events to be reported by the CBSS were identified
through discussion with health staff and Village
HealthVolunteers (VHVs) based on their public health import-
ance, severity and potential for an outbreak as well as the
existence of a control programme. They included malaria,chronic
cough, acute severe diarrhoea, measles and haem-
orrhagic fever, and births and deaths. A standard case
definition was used throughout the system to collect data at
the village level. It was adapted from case definitions usedat
the health centre level:
Suspected malaria: Any person with high and inter-
mittent fever associated with chills. Separate episodes
were considered as different cases.Suspected measles: Any child
(under 15 years) with
fever and maculo-papular rash and any of the
following: cough, runny nose, or red eyes.
Severe acute diarrhoea: Any person aged five years ormore with
acute watery diarrhoea of more than three
Figure 1 Map of Cambodia showing the location of communes for
pilot study, 20002002.
Tropical Medicine and International Health volume 10 no 7 pp
689697 july 2005
S. Oumet al. Community-based surveillance in Cambodia
690 2005 Blackwell Publishing Ltd
-
7/21/2019 CBS Cambodia
3/9
motions a day and severe dehydration characterized
by sunken eyes and intense thirst. Here too, separateepisodes
were considered as different cases.Haemorrhagic fever: Any child
with high and per-
sistent fever of abrupt onset, associated with maculo-papular
rash and petechiae/gingival bleeding/bloody
stool.Chronic cough: Any person with cough for more than
21 days. VHVs have to report the same case everymonth until the
patient is cured or has died.Cluster of cases: A group of five or
more similar cases
occurring unusually closely together in any village
within a week.
Data on these events were collected by VHVs and
reported to data collation and analysis teams based in
health centres. VHVs reported immediately any clustering
of cases (more than five cases within a week) and deathsbecause
of acute diarrhoea to the data collation and
analysis team. Health centre staff considered such events to
be potential outbreaks and reported them immediately to
the staff based at operational district offices who investi-
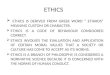
gated and took measures to control outbreaks. The VHVsalso
reported every month the total number of cases of
each event included in the surveillance system using amonthly
report form (Figure 2). This was done in a
monthly meeting of VHVs and health centre staff in which
the data were collated and analysed, and remedial actions
discussed. The collated data were reported to the team in
the Operational District office who gave feedback and
investigated any unusual increase in the number of casesand
neonatal deaths.
At least one VHV was enrolled per village, either
selected by health centre staff or elected by the villagers.
Health staff involved in the CBSS included three staff ateach
health centre, two at each Operational District and
one at each Provincial Health Department.A series of 3-day
initial training workshops was held for
both VHVs and health staff at each project site shortly
before the implementation of the system. It was followed
by a monthly half day of refresher training separately for
VHVs and health staff and further training in collation and
analysis of data for the health staff. The training of VHVs
focused on disease recognition using a syndromic approachand on
methods for prevention. Slides and videocassettes
were used to train VHVs to recognize diseases and events
accurately, and to contribute better to disease prevention
and control.
A household survey was conducted in July 2001 in all
villages in three of the seven communes, in order to
obtainvillage-based data to validate VHVs case reports of
diseases and other health-related events during the
preceding month (for cases of disease) and year (for
vitalevents). The CBSS standard case definitions were used.
Causes of deaths were assessed by verbal autopsy based on
the standard CBSS definitions; deaths of infants under
28 days were investigated for neonatal tetanus using astandard
verbal autopsy questionnaire, and so were deaths
suspected to be because of measles. Each case and vital
event reported during this survey was then matched to the
CBSS data using household identifiers. Matching of reportswas
carried out in the field, when the VHVs were present
for clarification if needed. Survey and outbreak investiga-
tion data were taken as the reference value. Cases reported
by VHVs that matched those detected by the household
survey or an outbreak investigation were considered astrue
positive for the estimation of the sensitivity and
positive predictive value of the CBSS.
Results
Disease surveillance
Table 1 shows the total number of cases of malaria,
measles, severe diarrhoea and haemorrhagic fever as well
as person-months with chronic cough, as reported by the
CBSS from September 2000 to August 2002. Only a third
of malaria, chronic cough, and haemorrhagic fever cases,just
over a quarter of severe diarrhoea cases, and less than
one in 20 cases of measles had contacted a health facility.
The monthly incidence of malaria, severe diarrhoea,
measles and haemorrhagic fever reported by the CBSS from
September 2000 to August 2002 is shown in Figures 35,with
comparison between the total cases (including cases
treated at home and health facilities) with those treated
athealth facility alone. With the exception of July 2001, the
total monthly incidence of malaria had steadily declined
from over 250 cases in September 2000 to around 100
cases in August 2002. The decline of malaria cases reported
by the CBSS as treated at health facility alone over thesame
period was substantially less marked than that the
total malaria incidence, which also reflects a relativeincrease
of the use of public health facility for malaria
treatment. The CBSS data also show that a relatively small
number of cases of haemorrhagic fever, measles, and severe
diarrhoea had contacted a health facility.
Vital events
CBSS data show that 95% of births and deaths occurred at
home. Home deliveries were assisted almost exclusively
by Traditional Birth Attendants (TBAs) and 90% of
perinatal deaths occurred at home. Most deaths because
Tropical Medicine and International Health volume 10 no 7 pp
689697 july 2005
S. Oumet al. Community-based surveillance in Cambodia
2005 Blackwell Publishing Ltd 691
-
7/21/2019 CBS Cambodia
4/9
Reporting Month:
Village: Commune: . District:
I. Vital events
1. Pregnancies ( =No TT vaccination; =Received 1 TT dose;
=Received 2+ TT doses)
< 7 months gestational age 79 months gestational age
Total
2. Newborns (Delivered at: =home and by TBA; =public health
facility;
=home by trained midwife)
Alive Died within 7 days Stillborn Total
3. Deaths
Place (tick) Presumed cause of death**Name Sex
(circle)
Age*
PublicHospital
Home/others
Principal syndromes precedingdeath (specify)
If maternaldeath: tick
M / F
M / F
M / F
M / F
* Age = in days if under a month; in months if under a year; in
years if 1+ years
** Immediate report if death due to diarrhoea
II. Communicable diseases
Age(years)
Chroniccough
(Cough more
than 21 days)
Severe
diarrhoea
(Acute watery
diarrhoea +
dehydration)
Suspected
malaria
(High &
intermittent fever +
chills)
Haemorrhagic fever
(High fever of abrupt
onset + maculo-papular
rash + petechiae /
gingival bleeding /
bloody stool)
Suspected
measles
(Fever + maculo
papular rash +
cough/ runny
nose/ red eye)
04
514
15+
Total
(a)
(b)
LEGEND: = 1 case NOT treated at any public health facility; = 1
case treated at health centre, referral ornational hospital. NOTE:
Immediate report to health centre if clustering of cases (i.e. 5 +
similar cases) in a given week
Figure 2 English translation of VHVs monthly recording and
reporting form: (a) front, and (b) back (TT, tetanus toxoid; TBA,
traditionalbirth attendant).
Tropical Medicine and International Health volume 10 no 7 pp
689697 july 2005
S. Oumet al. Community-based surveillance in Cambodia
692 2005 Blackwell Publishing Ltd
-
7/21/2019 CBS Cambodia
5/9
of malaria, chronic cough, diarrhoea, haemorrhagic fever
and measles also occurred at home (Table 2).The infant and
under-five mortality rates, calculated
from data generated by the CBSS from all project
communes in the second year of project implementation,were 72.9
and 89.0 per 1000 live births respectively,
slightly lower than those of the previous year which had
been 80.0 and 107.5 per 1000 live births respectively
(Table 3).
Detection of outbreaks
From August 2000 to September 2002 two outbreaks of
malaria were detected in a commune; seven outbreaks of
Table 1 Number of cases of diseases* reported by CBSS,Cambodia
September 2000 to August 2002
Syndrome/disease
Treated athealth facility,n (%)
Treatedat home,n(%)
Totalcases,n
Malaria 1481 (36.9) 2533 (63.1) 4014Chronic cough 762 (38.6)
1214 (61.4) 1976Severe diarrhoea 101 (28.5) 254 (71.5) 355Measles
10 (4.4) 218 (95.6) 228Haemorrhagic fever 16 (32.7) 33 (67.3)
49
* For chronic cough, the table shows person-months with
cough.For malaria and diarrhoea, separate episodes are considered
asdifferent cases.
0
50
100
150
200
250
300
Sep'00Oct Nov Dec Jan'01FebMar Apr May Jun Jul Aug Sep Oct Nov
DecJan'02Feb Mar Apr May Jun Jul Aug
No.ofcases
Malaria: total
Malaria: health facility alone
Figure 3 Monthly incidence of malariareported by CBSS, showing
proportiontreated in health facility alone, all pilotstudy
communes, 20002002.
0
5
10
15
20
25
30
35
40
45
50
Sep'00Oct NovDecJan'01 Feb Mar Apr May Jun Jul Aug Sep Oct Nov
DecJan'02FebMar Apr May Jun Jul Aug
Number
ofcases
Measles: total
Measles: health facility alone
Diarrhoea: total
Diarrhoea: health facility alone
Figure 4 Monthly incidence of measlesand severe diarrhoea
reported by CBSS,showing proportions treated in healthfacility
alone, all pilot study communes,20002002.
Tropical Medicine and International Health volume 10 no 7 pp
689697 july 2005
S. Oumet al. Community-based surveillance in Cambodia
2005 Blackwell Publishing Ltd 693
-
7/21/2019 CBS Cambodia
6/9
severe acute diarrhoea were reported in two communes; 10
outbreaks of measles were detected in three communes;
and two clusters of haemorrhagic fever cases were reportedin one
commune. All these, with the exception of one
measles outbreak, were confirmed to be true outbreaks.
The information obtained by the CBSS drove local
health staff to respond rapidly and investigate outbreaks.
For instance, in Chan Mul commune, when reports of a
suspected outbreak of measles were brought to the atten-
tion of the commune health centre, a team of health centre
staff immediately went to the affected villages to verify
the
reports and subsequently undertook necessary control
measures as well as further investigations of the outbreak.
Accuracy of the reported cases of common syndromes and
vital events
The sensitivity of VHVs reporting of cases of communic-able
disease ranged from 65% for malaria to 93% for
measles. The positive predictive value (PPV) of VHVsreport on
communicable diseases ranged from 82% for
severe diarrhoea to 90% for measles. Concerning vital
events, 76% of women 79 months pregnant and 82% of
births in the three surveyed communes were reported by
VHVs (Table 4). The CBSS detected 95% of all deaths inthe three
communes during the year prior to the survey.
Discussion
A large proportion of cases of major infectious diseases did
not seek medical treatment at public health facilities and
were therefore not reported by the health facility-based
0
2
4
6
8
10
12
Sep'00 Oct Nov DecJan'01Feb MarApr May Jun Jul Aug Sep Oct Nov
DecJan '02FebMar Apr May Jun Jul Aug
No.ofcases
Haemorrhagic fever: total
Haemorrhagic fever: health facility alone
Figure 5 Monthly incidence of haemor-rhagic fever reported by
CBSS, showingproportion treated in health facility alone,all pilot
study communes, 20002002.
Table 2 Place of births and deaths reported by CBSS, pilot
studycommunes, Cambodia September 2000 to August 2002
Vital events
At healthfacilities,n(%)
Athome,n(%)
Total,n
Total births 89 (5) 1594 (95) 1683Total deaths 22 (5) 424 (95)
446Causes of death
Perinatal causes 3 (10) 28 (90) 31Malaria 6 (20) 24 (80)
30Chronic cough 3 (16) 16 (84) 19
Diarrhoea 1 (6) 17 (94) 18Haemorrhagic fever 2 (20) 8 (80)
10Measles 0 (0) 4 (100) 4All other causes 7 (2) 326 (98) 333
Table 3 Infant and under-5 mortalityrates, all pilot study
communes, Cambodia20002002
Project periodNumber oflive births
Infantmortality
Under-5 mortality
n Rate* n Rate*
Year 1 (September 2000 to August 2001) 837 67 80.0 90 107.5Year
2 (September 2001 to August 2002) 809 59 72.9 72 89.0
* Rate per 1000 live births.
Tropical Medicine and International Health volume 10 no 7 pp
689697 july 2005
S. Oumet al. Community-based surveillance in Cambodia
694 2005 Blackwell Publishing Ltd
-
7/21/2019 CBS Cambodia
7/9
surveillance system. Health facility data therefore could
not allow the detection of all measles, severe diarrhoea
orhaemorrhagic fever outbreaks. They also could not capture
all births and deaths in the rural areas because the majorityof
these vital events occurred at home. In contrast, the
CBSS captured more comprehensive and representative
data for major communicable diseases and detected
diseaseoutbreaks more frequently and more rapidly than the
routine disease surveillance system.
An additional factor is that in Cambodia, health staff
sometimes inflate the number of cases they have treated
in their routine monthly reports, in order to receive
additional quantities of drugs and supplies, either for
private practice or to replace date-expired stocks.
Surveillance data collected by the CBSS are not subjectto such
bias.
Most importantly, the CBSS provided a forum forinformation
sharing and joint decision-making between
local health staff and VHVs, which led to better collabor-
ation and active community participation between thesetwo sets
of key players in disease control and prevention.
The system also empowered the local health staff and
community in disease surveillance and outbreak response,
based on which they could take effective follow-up and
corrective action.
A tendency for malaria and diarrhoea incidence to
decline with time can be seen in Figures 3 and 4. Bothtendencies
can also be seen in the health facility data. This,
and the maintained level of reported incidence of measles
and haemorrhagic fever, supports the view that any suchdecline
is not attributable to a fall in sensitivity of the
CBSS. It would be tempting to attribute the decline toimproved
preventive interventions and outbreak response,
but such year-on-year variations are common in infectiousdisease
surveillance. A longer time series, or reliable data
from non-CBSS communes, would be required to confirm
that the CBSS had contributed to a sustained decline in
disease incidence.
Factors underlying the performance of the CBSS
The high performance of the Cambodian CBSS is linked to
the importance of events monitored, the system design andits key
players. Events monitored by it were multiple,
important, relevant and relatively easy for local people to
identify. The diseases or syndromes to be reported werelocally
the most important communicable diseases in terms
of severity, burden or epidemic potential. They are all
targets of national control programmes, and effective
control measures are available. Births and deaths, on the
contrary, constitute important and relevant information
needed for appropriate planning of disease control and
prevention activities as well for monitoring infant and
childmortality, as birth and death registration are not
available
in Cambodia. All these events have elicited the interest of
health staff and VHVs, who are the end users of the datathey
collect.
The system design, including two-way flow of informa-tion,
instant feedback, local use of data, and simplicity as
well as its decentralized management contributed to the
success of the operation of the CBSS. The monthly
feedback meeting is a central feature of the Cambodia
CBSS and is crucial for its success. It enables information
to
be fed back to all participants of the system and decisions
to be made to address identified issues within the same day
of data reporting and minimizes the related workload ofthe
health staff as well. This process challenges all
participants to take necessary remedial action together, the
results of which can be closely monitored by them at thenext
monthly feedback meeting. The system has, therefore,
overcome constraints that have hampered many previousCBS systems
including delayed feedback and non-partici-
pation of local health staff and communities in dataanalysis,
decision-making and action-taking. Additionally,
the feedback meeting provides an opportunity for con-
tinuing training of VHVs and health staff, thereby contri-
buting to the improvement of the system.
Table 4 Sensitivity and positive predictivevalue (PPV) of the
CBSS, household surveyof three communes, July 2001
Events
Casesdetectedin survey*
Casesreportedby CBSS
Truepositivecases
Sensitivity(%)
PPV(%)
Malaria 88 65 57 65 88Chronic cough 73 62 55 75 89Severe
diarrhoea 12 12 10 82 82Measles (7/2000 to 6/2001) 92 96 86 93
90Pregnancy (79 months) 85 67 65 76 97Birth 34 28 28 82 100
* Gold standard for estimating sensitivity and PPV of CBSS:
Household Survey for malaria,chronic cough, and pregnancy (recall
period 1 month) and outbreak investigations formeasles (1
year).
Tropical Medicine and International Health volume 10 no 7 pp
689697 july 2005
S. Oumet al. Community-based surveillance in Cambodia
2005 Blackwell Publishing Ltd 695
-
7/21/2019 CBS Cambodia
8/9
The Cambodia CBSS, in which data are actively
collected through periodic home visits, yields a
higherproportion of cases reported than passive data collection
surveillance systems. The use of tally sheets to record
and report events is most appropriate for semi-literateVHVs in
remote areas and helps to reduce errors in data
collection. Furthermore, a CBS system which is
developed with local participation and locally managed
is likely to be more effective than vertically-run pro-grammes
and projects developed and implemented by
national, international or non-governmental organizations.
Finally, another contributing factor in the success of CBSS
is themotivational mechanism to maintain VHVs voluntary
work. It included travel costs, per diem and food given toVHVs
who attended their monthly meeting with health staff
at the health centre, free medical care, training, rewards
and
recognition as well as the immediate response of health
staff
to the information reported by VHVs and instant feedbackof
information to them. As a result, VHVs were willing to
travel quite frequently to collect data in their own village
as
well as to travel by foot or motorbike to the health
centre,located typically 411 km from their home, for the
monthly
meeting, which almost all regularly attended.
Constraints
The VHVs were sometimes unable to collect data from
people living too far away from their house, especially
those temporarily moving to camp by their farm landduring the
rice-planting and harvesting seasons. For
instance, the majority of households not visited by VHVsin June
2001 were located further than 1.5 km from their
house. Also, the response of health staff to the information
generated by the CBSS was not yet optimal in many
projectcommunes because of low salaries and inadequate funding
for health services.
Costs and sustainability
The annual cost of the Cambodia CBSS was about US$0.5
per capita including occasional visits from Phnom Penh
fortraining, supervision, and evaluation. This cost would be
lower by half if the system were operated by the District
alone; that is, without the research and development inputby one
of us (SO). It appears to be lower than that of many
similar systems running in developing countries to date,because
of its use of existing health infrastructure and staff,
which costs much less than projects run by non-govern-
mental organizations where additional staff and facilities
have to be funded (ONeill 1993; Cairncrosset al. 1997).
The amount of staff time required to manage the system
was relatively small; 1 day per month for the monthly
meeting, plus a half day of training, and time spent onoutbreak
response, if any. The VHVs spent 34 half days
per month on home visits for data collection, in addition to
their day at the monthly meeting.
In 2004, the system proved to be replicable as it has
beenimplemented, with support from Save the Children Aus-
tralia, throughout an operational district of 100 000
inhabitants. It is being implemented in two more districts,
and a fourth is planned for early 2005.The Cambodian CBSS has
many attributes that could
make it more viable that is sustainable than other
CBSSs. First, VHVs and health staff have the capability to
run and manage the system by themselves, with little
technical or supervisory support from the central level.Second,
the system is built on the existing health system
and resources, following the Ministry of Health policy and
strategy to strengthen the Operational District structure.
It
gives the Operational District and health centre a mech-anism to
fulfil their role in disease prevention and control
in the communities. Third, the Cambodian CBSS comprises
mechanisms to maintain VHVs motivation to continue theCBSS. The
mechanisms include continuous training, sup-
portive supervision, health care benefits, work recognition,
instant feedback, and involvement in data analysis and
decision-making.
We conclude that a community based surveillancesystem run by
VHVs and local health staff is feasible and
that this system can produce useful information for
monitoring trends and to identify potential outbreaks of
common infectious diseases.
Acknowledgements
This study would not have been possible without financial
assistance from the European Commission and Cambo-
dias Ministry of Health for which we are very grateful. We
wish to thank in particular Dr Frederick Gay, Dr Andrew
Corwin, Ms Sarah McFarlane, Dr Kyi Minn, Prof FelicityCutts, Ms
Susanne Wise, Dr Gertrud Schmid-Ehry and
many other people for their encouragement and inputs
during the development and refinement of the CBSS
inCambodia.
References
Ahluwalia I, Kouletio M, Curtis Ket al. (1999) Community
empowerment: CDC collaboration with the CARE Community-
Based Reproductive Health Project in two districts in
Tanzania.
Journal of Womens Health and Gender-Based Medicine8,
10151018.
Anselmi M, Araujo E, Narvaez A, Cooper PJ & Guderian RH
(1995) Yaws in Ecuador: impact of control measures on the
Tropical Medicine and International Health volume 10 no 7 pp
689697 july 2005
S. Oumet al. Community-based surveillance in Cambodia
696 2005 Blackwell Publishing Ltd
-
7/21/2019 CBS Cambodia
9/9
disease in the Province of Esmeraldas.Genitourinary Medicine
71, 343346.
Balasubramanian R, Sadacharam K, Selvaraj Ret al.(1995)
Feasibility of involving literate tribal youths in
tuberculosis
case-finding in a tribal area in Tamil Nadu. Journal
ofTuberculosis and Lung Disease76, 355359.
Cairncross S, Braide EI & Bugri SZ (1996) Community
participation in the eradication of guinea worm disease.Acta
Tropica61, 121136.
Cairncross S, Cutts FT & Peries H (1997) Vertical
programmes;
what are they good for? Authors reply. Lancet 350,
812813.
Cairncross S, Anemana SD, Olsen A (1999) Towards the eradi-
cation of Guinea worm: a Danish-Ghanaian collaboration.
Parasitology Today5, 127129.
Ghebreyesus TA, Witten KH, Getachew A et al. (2000) The
community-based malaria control programme in Tigray, nor-
thern Ethiopia; a review of programme set-up, activities,
out-
comes and impact. Parassitologia 42, 255290.
Howard-Grabman L (2000) Bridging the gap between commu-
nities and services providers: developing accountability
through community mobilisation approaches.IDS Bulletin 31,
8896.
Jaravaza VS, McCoy MC, Dando BC (1982) Unified National
Health Information System. Pat II: the village health worker
health information system.Central African Journal of
Medicine
28, 5764.
Manderson L (1992) Community participation and malaria con-trol
in Southeast Asia: defining the principles of involvement.
Southeast Asian Journal of Tropical Medicine and Public
Health
23(Suppl. 1), 916.
ONeill K. (1993). Community-based surveillance: a critical
examination of nine case-studies. MSc Dissertation. London
School of Hygiene and Tropical Medicine, University of Lon-
don, London.
Ruebush TK 3rd, Zeissig R, Koplan JP, Klein RE, Godoy HA
(1994) Community participation in malaria surveillance and
treatment. III. An evaluation of modifications in the
Volunteer
Collaborator Network of Guatemala.American Journal of
Tropical Medicine and Hygiene50, 8598.
Valyasevi A, Winichagoon P, Dhanamitta S (1995) Community-
based surveillance for action towards health and nutrition:
experience in Thailand. Food and Nutrition Bulletin 16, 120
125.
WHO (2000) An integrated approach to communicable disease
surveillance.Weekly Epidemiological Record75, 18.
Authors
Sophal Oum, Ministry of Health, Phnom Penh, Cambodia. Tel:
+855-12-500-565; Fax: +855-23-883-561; E-mail: Sophal_oum@
hotmail.com
Daniel Chandramohan(corresponding author) andSandy Cairncross,
London School of Hygiene and Tropical Medicine, Keppel
Street, London WC1E 7HT, UK. Tel.: 00-44-20-7927 2322; E-mail:
[email protected], sandy.cairncross@lshtm.
ac.uk
Tropical Medicine and International Health volume 10 no 7 pp
689697 july 2005
S. Oumet al. Community-based surveillance in Cambodia
2005 Blackwell Publishing Ltd 697