Embed Size (px)
Citation preview

IFU 108-F Page 1 of 45
TORUS STENT GRAFT SYSTEM
INSTRUCTIONS FOR USE Device Description The Torus Stent Graft System is an endovascular device delivered via a small
diameter catheter to improve blood treat femoro-popliteal disease. When
used in conjunction with the PQ Snare and the PQ Crossing Device, Torus is
designed to create a fully-percutaneous bypass (the DETOUR procedure)
via an endovascular blood conduit from the origin of the SFA, through the
adjacent femoral vein, and back into the arterial lumen at the distal
reconstitution site (Figure 1).
The Torus Stent Graft System consists of a stent graft (Figure 2) and a
delivery catheter (Figure 3). The stent graft (SG) is a self-expanding
endoprosthesis comprised of a flexible, self-expanding composite structure
made of a nitinol (NiTi = Nickel:Titanium) wire frame encapsulated in an
expanded Polytetraflueorethylene (ePTFE) film. The stent graft is pre-
mounted on a delivery catheter which is an over-the-wire 8Fr system,
compatible with a 0.035” guidewire and has a 135 cm working length. The
handle of the delivery system consists of an internal pulley mechanism
activated through turning an external knob. Once at the target site, the
user can slide the outer sheath proximally by turning the knob to expose
the stent graft.
CAUTION-INVESTIGATIONAL DEVICE. LIMITED BY
FEDERAL (OR UNITED STATES) LAW TO
INVESTIGATIONAL USE

IFU 108-F Page 2 of 45
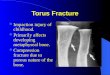
Figure 1: The DETOUR procedure
with the Torus Stent Graft System Figure 2: Torus Stent Graft
Figure 3: Torus Delivery System

IFU 108-F Page 3 of 45
Indication For Use The Torus Stent Graft System is intended to improve blood flow in patients with symptomatic peripheral arterial disease due to >15 cm long occlusions and diffuse stenoses of femoro-popliteal arteries, including in-stent restenosis, with reference vessel diameters ranging from 5.0 – 6.7 mm.
Contraindications The Torus Stent Graft System is contraindicated for use in the coronary and cerebral vasculature. The DETOUR procedure is contraindicated for use in patients with:
• A history of deep vein thrombosis
• Patent femoral vein <10 mm in diameter and without duplicate femoral vein
• Untreated flow-limiting aortoiliac occlusive disease
• Lack of patent single vessel runoff • Known hypersensitivities, allergies or contraindications
to: nitinol, PTFE; aspirin, heparin, antiplatelet, anticoagulant or thrombolytic therapy; or anticoagulation or contrast media.
Catalogue Reference Numbers
Catalogue Number Description
TO-5.5X200 Torus Stent Graft System – 5.5mm X 200mm
TO-6.0X100 Torus Stent Graft System – 6.0mm X 100mm
TO-6.0X150 Torus Stent Graft System – 6.0mm X 150mm
TO-6.0X200 Torus Stent Graft System – 6.0mm X 200mm
TO-6.7X100 Torus Stent Graft System – 6.7mm X 100mm
TO-6.7X150 Torus Stent Graft System – 6.7mm X 150mm
TO-6.7X200 Torus Stent Graft System – 6.7mm X 200mm
Sizing – Vessel Diameter Labeled Device
Diameter (mm)
Recommended Vessel Diameter
(mm)
Available Device Nominal Lengths
(mm)
Recommended Balloon Diameter for Post-Dilation
(mm)
5.5 5.0-5.5 200 5.5
6.0 5.6-6.0 100, 150, 200 6.0
6.7 6.1-6.7 100, 150, 200 7.0

IFU 108-F Page 4 of 45
Sizing – Bypass Length Lesion Length
(cm)
# of Stent Grafts
Stent Graft 1 Nominal Length
(mm)
Stent Graft 2 Nominal Length
(mm)
Stent Graft 3 Nominal Length
(mm)
15-17 2 150* 150 N/A
100 200 N/A
18-22 2 200 150 N/A
23-26 2 200 200 N/A
27-32 3 200* 150 150
3 200 200 100
32+ 3 200 200 200 *Preferred configuration
Warnings
• For single use only. Do not reuse, reprocess, or re-sterilize. Reuse, reprocessing, or re-sterilization may compromise the structural integrity of the device and/or lead to device failure, which in turn, may result in patient injury, illness, or death. Reuse, reprocessing, or re-sterilization may also create a risk of contamination of the device and/or cause patient infection or cross-infection, including, but not limited to, the transmission of infectious disease(s) from one patient to another. Contamination of the device may lead to injury, illness, or death of the patient.
• The Torus Stent Graft System must be used with visual guidance (e.g., fluoroscopy) by physicians skilled in percutaneous, intravascular techniques in a fully equipped catheterization laboratory.
• Do not use the Torus Stent Graft System if the package is opened or damaged.
• Do not use the Torus Stent Graft System past the stated use-by date on the package label.
• Special care should be taken to ensure that the appropriate size stent grafts are selected prior to implantation. Native vessel dimensions must be accurately measured, not estimated.
• Do not cannulate or puncture the SG. Cannulating or puncturing the SG may result in damage to the ePTFE lining and/or the NiTi frame, resulting in compromised performance or failure of the SG.
• Do not cut the SG or attempt to surgically implant the SG. The SG should only be placed and deployed using the Torus Stent Graft System on which it is pre-loaded.
• Inadvertent, partial or failed deployment or migration of the SG may require surgical intervention.

IFU 108-F Page 5 of 45
Precautions
• Store the Torus Stent Graft System in a cool, dry environment and away from direct sunlight.
• Inspect the Torus Stent Graft System prior to use. Do not use if the device appears to be bent, kinked or damaged in any way.
• Do not expose the Torus Stent Graft System to organic solvents (e.g. alcohol).
• Only use the Torus Stent Graft System with an 0.035” guidewire with minimum length of 300 cm.
• Only use the Torus Stent Graft System with a minimum 8F sheath.
• Antiplatelet medication should be initiated prior to placement of the SG. Effective anticoagulation therapy should be maintained at a dosage deemed appropriate by the physician.
• After use, dispose of the Torus Stent Graft System product and packaging in accordance with hospital, administrative and/or local government policy.
MRI Safety and Compatibility: MR Conditional Non-clinical testing of the SG has demonstrated that the device is MR conditional. Patients with this device can be safely scanned in an MR system meeting the following conditions:
• Static magnetic field of 1.5 T. • Maximum spatial field gradient of 3000 G/cm (30 T/m). • Maximum MR system reported, whole body averaged specific
absorption rate (SAR) of 2 W/kg (Normal Operating Mode). Under the scan conditions defined above, the SG is expected to produce a maximum temperature rise of less than 1ºC after 15 minutes of continuous scanning. Testing of the image artifacts near the device was not performed. The artifact size is unknown and may significantly obscure MR image features in the neighborhood of the device. Possible Complications
• Procedure Related: As with all procedures that utilize techniques for introducing a catheter into a vessel, complications may occur. These complications include, but are not limited to: access vessel (arterial/venous) occlusion; amputation; aneurysm or pseudoaneurysm; arteriovenous fistula; bleeding complications; death; device or deployment malfunction/failure; drug reactions to

IFU 108-F Page 6 of 45
antiplatelet agents or contrast medium; embolism (peripheral or pulmonary); fever in absence of infection; hemorrhage or hematoma; hypotension/hypertension; infection local or systemic including bacteremia or septicemia; malapposition or migration; malposition; myocardial infarction; pain (insertion site, leg and/or foot); renal insufficiency or failure secondary to contract medium; shock; side branch occlusion; stroke or transient ischemic attack; thrombosis; vessel wall trauma (dissection, perforation or rupture); vessel spasm; venous flow disruption (deep vein thrombosis, phlebitis, leg swelling and/or development of varicose veins); and/or worsening claudication.
• Device Related: Complications and adverse events can occur when using any endovascular device. These complications include, but are not limited to: access vessel (arterial/venous) occlusion; amputation; aneurysm or pseudoaneurysm; arteriovenous fistula; bleeding complications; death; device or deployment malfunction/failure; embolism (peripheral or pulmonary); fever in absence of infection; hemorrhage or hematoma; infection local or systemic including bacteremia or septicemia; malapposition or migration; malposition; myocardial infarction; pain (insertion site, leg and/or foot); side branch occlusion; stroke or transient ischemic attack; thrombosis; vessel wall trauma (dissection, perforation or rupture); vessel spasm; venous flow disruption (deep vein thrombosis, phlebitis, leg swelling and/or development of varicose veins); and/or worsening claudication.
How Supplied
The Torus Stent Graft System is supplied sterile and is intended for Single
Use Only.
Directions for Use – Guidewire Placement for DETOUR Procedure
Set-Up
1. Inspect the PQ Crossing Device and PQ Snare pouch for damage. Do not use device if the package has been opened or damaged.
2. Using sterile technique, remove the PQ Crossing Device and PQ Snare from the package and transfer to the sterile field. Inspect the catheters for any visible signs of damage.
3. Flush the PQ Crossing Device and advance the Outer Handle to ensure the Stabilizer deploys and Needle can be deployed by depressing the

IFU 108-F Page 7 of 45
Button. After deploying the needle, retract the outer handle, collapsing the stabilizer and returning the PQ Crossing Device to the neutral position.
WARNING: Do not place finger or other body parts near Distal Tip of PQ Crossing Device prior to deploying the Needle.
4. Flush the PQ Snare, retract the Outer Sheath and advance the Proximal Handle to confirm NiTi Cage operation. Re-advance Outer Sheath over NiTi Cages.
Isolate Vascular Targets
1. Gain femoral vein (FV) access through tibial percutaneous venous access and place a 7Fr sheath.
2. Load an 0.014” guidewire through the rear Guidewire Port and advance PQ Snare through the 7Fr sheath.
3. Advance the PQ Snare ipsilaterally in the FV at a level just above the arterial lesion and deploy the NiTi Cages.
4. Gain contra-lateral common femoral arterial access using standard technique and place an 8Fr sheath.
5. Load a 300 cm 0.014” guidewire through the rear Needle guidewire lumen of the PQ Crossing Device and advance until the distal tip is just visible then retract approximately 5 cm.
6. Backload the 0.014” guidewire in RX Port and advance PQ Crossing Device to the lesion in the SFA.
Create Proximal Anastomosis
1. Rotate fluoroscopy head to superimpose the femoral vein over the femoral artery, adjusting both lateral and cranial/caudal planes to optimize overlap of the FV and SFA.
2. Rotate 90 degrees in either direction to obtain orthogonality of the vessels in a planar view.
3. Using the Crown Marker Band System, orient the PQ Crossing Device towards the upper NiTi Cage in the FV.
4. Rotate counter-clockwise and advance the Outer Handle forward until the Stabilizer is deployed and the Outer Handle is locked in place. Re-confirm orientation of the PQ Crossing Device. If orientation is not adequate retract the Outer Handle and repeat until appropriate orientation is achieved with Stabilizer deployed.

IFU 108-F Page 8 of 45
WARNING: Do not rotate PQ Crossing Device while Stabilizer is deployed.
5. Depress the Button to deploy the Needle into the adjacent FV.
WARNING: Place hand and fingers on the inner handle (not on the
guidewire port area) to avoid pinching gloves during needle
deployment.
6. Advance the 300 cm 0.014” guidewire through the Needle to confirm FV access. Repeat Steps 2-5 until venous access is confirmed.
CAUTION: Do not advance the guidewire significantly through the
Needle tip prior to Needle deployment. Doing so may damage the
device.
NOTE: If the PQ Crossing Device Needle extends through both walls of
the target vein, partially retract Needle using the Outer Handle and
advance guidewire to gain venous access.
7. Retract the Needle using the Outer Handle and snare the guidewire in the upper NiTi Cage by retracting the Proximal PQ Snare Handle and advancing the outer sheath.
CAUTION: Do not attempt to snare the guidewire with the PQ Crossing Device Needle advanced. Doing so may damage the devices. CAUTION: Do not attempt to snare the guidewire with the lower NiTi Cage. If the guidewire is snared by the lower cage, retract the guidewire and NiTi cages, reposition the PQ Snare and re-attempt snare procedure until snare with upper NiTi Cage is confirmed. CAUTION: Do not advance the guidewire significantly past the upper NiTi Cage. A long segment of guidewire may interfere with the ability to advance the Outer Sheath over the NiTi Cage and damage the device.
8. Withdraw the PQ Snare through the venous access site.
9. Withdraw the PQ Crossing Device while ensuring the distal portion of the guidewire remains externalized at the ipsilateral venous access site.
WARNING: Ensure the Stabilizer and Needle are retracted prior to
removing the PQ Crossing Device.

IFU 108-F Page 9 of 45
10. Retract Outer Sheath and deploy NiTi cages to remove the snared guidewire from PQ Snare.
11. Inspect the guidewire for damage.
Create Distal Anastomosis
1. Re-advance PQ Snare over the guidewire in the FV and deploy the upper NiTi Cage distal to the lesion.
CAUTION: Ensure Outer Sheath is positioned over collapsed NiTi Cages
prior to advancing through introducer sheath.
2. Load a 300 cm 0.014” guidewire through the rear Needle guidewire lumen of the PQ Crossing Device and advance until the distal tip is just visible then retract approximately 5 cm.
3. Backload the guidewire in the PQ Crossing Device RX Port and re-advance the PQ Crossing Device to the proximal anastomosis.
4. While maintaining tension on the guidewire at both access sites, gently advance the PQ Crossing Device through the proximal anastomosis into the FV.
WARNING: Do not deploy the Stabilizer prior to advancing through
the proximal anastomosis.
WARNING: Do not exert excessive force while advancing through the
anastomosis. Ensure tension is applied to the guidewire at both
access sites and gently advance PQ Crossing Device until FV access is
confirmed fluoroscopically.
5. Advance the PQ Crossing Device over the wire until it docks to the PQ Snare’s tip.
6. Repeat steps 1-3 from the Proximal Anastomosis instructions to obtain an orthogonal view of the FV and target artery (either SFA or Popliteal Artery).
7. Using the Crown Marker Band System, orient the PQ Crossing Device towards the SFA/Popliteal artery.
8. Advance the Outer Handle until the Stabilizer is deployed and rotate the Outer Handle until it is locked in place. Re-confirm orientation of the PQ Crossing Device and adjust if necessary.
9. Depress the Button to deploy the Needle through the venous and arterial walls and into the adjacent SFA/Popliteal artery.

IFU 108-F Page 10 of 45
WARNING: If the PQ Crossing Device Needle extends through both walls of the target artery, partially retract Needle using the Outer Handle and advance guidewire to gain arterial access.
10. Advance the 300cm guidewire through the Needle to confirm arterial access. Repeat Steps 7-9 as necessary until guidewire placement is confirmed in target artery.
CAUTION: Do not advance the guidewire distal to the Needle exit window prior to deploying the Needle. Doing so may damage the device.
11. Withdraw the PQ Snare through the venous access site.
12. Withdraw the PQ Crossing Device while ensuring distal arterial guidewire position is maintained.
WARNING: Ensure the Stabilizer and Needle are retracted prior to removing the PQ Crossing Device.
Directions for Use – Torus Stent Graft Placement for DETOUR Procedure
Sizing and Selection of the Stent Graft
1. Prior to opening the sterile package, check that the diameter and length of the SGs are correct.
2. Select the appropriate SG diameters for the distal and proximal vessels using the table provided in “Sizing”
3. Select the appropriate SG lengths based on the length of the proposed bypass.
A. The lengths provided in “Sizing” are the nominal stent graft lengths.
B. It is important that the stent graft occupy at least 3 cm of the arterial lumen on both the distal and proximal sides of the lesion.
4. When overlapping (telescoping) grafts, at least 6 cm of overlap is required.
A. A 5.5 mm SG may only be placed proximally into a 5.5 mm SG.
B. A 6.0 mm SG may be placed proximally into a 5.5 mm or 6.0 mm SG.
C. A 6.7 mm SG may be placed proximally into a 6.0 mm or 6.7 mm SG.
Medication

IFU 108-F Page 11 of 45
Preparation of patients receiving the SG should include initiation of an appropriate dosage of oral antiplatelet medication prior to and following the procedure. Effective anticoagulation therapy should be maintained throughout the procedure and continued into the postoperative period, as deemed appropriate by the treating physician.
Set-up 1. Inspect the Torus Stent Graft System pouch for damage. Do not use the
device if the package has been opened or damaged.
2. Using sterile technique, remove the device from the package and transfer to the sterile field. Inspect the device for any visible signs of damage.
CAUTION: Do not deploy the SG prior to insertion. The SG is self-expanding and cannot be re-loaded on the delivery system.
3. Flush Guidewire Lumen using the luer connector on the proximal end of the device using heparinized-saline until fluid exits the catheter tip.
4. Flush the SG Lumen using the flush port on the device handle until fluid exits the sides of the Torus Stent Graft System, proximal to the SG location.
Stent Graft Placement
1. Insert the Torus Stent Graft System over a 0.035” guidewire and advance to the treatment site.
2. Advance the Torus Stent Graft System through the proximal and distal anastomoses.
WARNING: Do not exert excessive force while advancing through the anastomosis. Gently advance Torus Stent Graft System until distal arterial access is confirmed fluoroscopically. Re-dilate anastomosis if significant resistance is encountered.
3. Advance the distal marker band of the Torus Stent Graft System a minimum of 3 cm distal to the distal anastomosis, leaving the proximal marker band within the FV.
4. Hold the Torus Stent Graft System handle flat on the table with the knob facing up and turn the knob in the direction of the arrow to deploy the stent graft.
5. Remove the Torus Stent Graft System.
CAUTION: When removing the delivery system avoid displacing the SG.
6. Insert the second Torus Stent Graft System over the same guidewire

IFU 108-F Page 12 of 45
and advance through the proximal anastomosis.
7. Position the distal marker band approximately 6 cm inside of the deployed stent graft and the proximal marker band at least 3 cm proximal to the proximal anastomosis in the SFA. After confirming position at both locations, deploy the stent graft completing the bypass.
8. Remove the Torus Stent Graft System.
CAUTION: When removing the delivery system avoid displacing the SG.
9. If a third stent graft is needed to complete the bypass necessary, insert the third stent graft over the same guidewire and advance through the proximal anastomosis.
10. Position the distal marker band approximately 6 cm inside of the deployed stent graft and the proximal marker band at least 3 cm proximal to the proximal anastomosis in the SFA. After confirming position at both locations, deploy the stent graft completing the bypass.
WARNING: When deploying the proximal stent graft please ensure that the proximal edge (exposed end) of the stent graft is 1-2 mm above the ostium of the superficial femoral artery (Figure 4).
Figure 4: SG Proximal Edge Optimal Position

IFU 108-F Page 13 of 45
11. Remove the Torus Stent Graft System.
12. Dilate each stent graft along its entire length using the balloons designated in “Sizing”.
WARNING: Do not dilate outside the margins of the deployed stent graft(s).
13. Remove the guidewire and proceed with vessel closures.
Disposal After use, dispose of product and packaging in accordance with hospital, administrative and/or local government policy.
Storage and Handling Store devices in a cool, dry environment and away from direct sunlight.
Definition of Symbols
Batch code
Consult instructions for use
Manufacturer
Do not resterilize
Do not reuse
Sterilized using ethylene oxide
Catalogue number
Caution
Keep away from sunlight
Use-by date
Do not use if package is
damaged
Contains or Presence of
Phthalate
Authorized European
representative
Keep dry
MR Conditional
Symbols were derived from “ISO 15223 Medical Devices – Symbols to be Used with Medical Device Labels, Labelling and
2797

IFU 108-F Page 14 of 45
Information to be Supplied”, “ASTM F2503 – Standard Practice for Marking Medical Devices and Other Items for Safety in
the Magnetic Resonance Environment”, and “EN 15986 Symbol for Use in the Labelling of Medical Devices –
Requirements for Labelling of Medical Devices Containing Phthalates”.
Manufacturer and EC Representative
PQ Bypass, Inc. 1971 Milmont Drive Milpitas, CA 95035 U.S.A.
HealthLink Europe BV De Tweeling 20-22
5215 MC’s-Hertogenbosch The Netherlands

IFU 108-F Page 15 of 45
TORUS STENTGRAFT-SYSTEM
GEBRAUCHSANWEISUNG
Beschreibung des Geräts Das Torus Stentgraft-System ist ein endovaskuläres Gerät, das über einen
Katheter mit kleinem Durchmesser eingeführt wird, um die Blutbehandlung
bei einer femoropoplitealen Erkrankung zu behandeln. Bei Verwendung
mit dem Schlingenkäfigsystem und dem Kronen-Markierungsbandsystem,
ist Torus so konzipiert, dass es einen vollständig perkutanealen Bypass (das
DETOUR-Verfahren) über einen endovaskulären Blutkanal vom Ursprung
der Arteria femoralis superficialis durch die angrenzende Vena femoralis
und zurück in das arterielle Lumen an der distalen Wiederherstellungsstelle
bildet (Abbildung 1).
Das Torus Stentgraft-System besteht aus einem Stentgraft (Abbildung 2)
und einem Einführkatheter (Abbildung 3). Der Stentgraft (SG) ist eine
selbstexpandierende Endoprothese, die aus einer flexiblen,
selbstexpandierenden Verbundstruktur aus einem in ePTFE (expandiertes
Polytetraflueorethylen) eingekapselten Nitinol (NiTi = Nickel:Titan)-
Drahtrahmen besteht. Der Stentgraft ist auf einen Einführkatheter
vorgeladen, der ein 8Fr-Über-den-Draht-System ist, das kompatibel mit
einem 0,035”-Führungsdraht ist und eine Arbeitslänge von 135 cm hat. Der
Griff des Einführsystems besteht aus einem internen Zugmechanismus, der
durch Drehen eines externen Stellrads aktiviert wird. An der Zielstelle kann
der Anwender die äußere Schleuse proximal verschieben, indem das
Stellrad zur Exposition des Stentgrafts gedreht wird.
VORSICHT-PRÜFINSTRUMENT. VON US-
BUNDESSTAATLICHEN (ODER NATIONALEN)
GESETZEN AUF DIE VERWENDUNG ZU
FORSCHUNGSZWECKEN BESCHRÄNKT
DE

IFU 108-F Page 16 of 45
Abbildung 1: Das DETOUR-Verfahren mit dem Torus
Stentgraft-System
Abbildung 2: Torus Stentgraft
Abbildung 3: Torus Einführsystem
Gebrauchsanweisung Das Torus Stentgraft-System dient zur Verbesserung der Durchblutung bei Patienten mit symptomatischer peripherer arterieller Verschlusskrankheit aufgrund > 15 cm langer Okklusionen und diffuser Stenosen in
Vena
femoralis
TORUS
Stentgraft
Knie
Blockade
Arteria
femoralis
superficialis

IFU 108-F Page 17 of 45
femoropoplitealen Abschnitten, einschließlich In-Stent-Restenosen, mit Referenz-Gefäßdurchmessern zwischen 5,0 und6,7 mm. Kontraindikationen Das Torus Stentgraft-System ist nicht zur Verwendung im koronaren oder zerebralen Gefäßsystem indiziert. Das DETOUR-Verfahren ist kontraindiziert bei Patienten, auf die Folgendes zutrifft:
• Tiefe Venenthrombose in der Vorgeschichte
• Offensichtliche Vena femoralis mit einem Durchmesser von < 10 mm und ohne zweite Vena femoralis
• Unbehandeltes gefäßverengendes Leriche-Syndrom
• Abwesenheit eines offensichtlichen Ablaufs über ein Gefäß
• Bekannte Überempfindlichkeiten, Allergien oder Kontraindikationen gegenüber: Nitinol, PTFE, Aspirin, Heparin, Thrombozytenaggregationshemmer, Antigerinnungs oder Thrombolysetherapien oder Antigerinnungs oder Kontrastmittel.
Katalog-Referenznummern
Katalognummer Beschreibung
TO-5,5X200 Torus Stentgraft-System – 5,5 mm X 200 mm
TO-6,0X100 Torus Stentgraft-System – 6,0 mm X 100 mm
TO-6,0X150 Torus Stentgraft-System – 6,0 mm X 150 mm
TO-6,0X200 Torus Stentgraft-System – 6,0 mm X 200 mm
TO-6,7X100 Torus Stentgraft-System – 6,7 mm X 100 mm
TO-6,7X150 Torus Stentgraft-System – 6,7 mm X 150 mm
TO-6,7X200 Torus Stentgraft-System – 6,7 mm X 200 mm

IFU 108-F Page 18 of 45
Größe – Gefäßdurchmesser
Beschrifteter Gerätedurchmesser
(mm)
Empfohlener Gefäßdurchmesser
(mm)
Verfügbare Geräte-
Nennlängen (mm)
Empfohlener Ballondurchmesser zur
anschließenden Dilatation (mm)
5,5 5,0–5,5 200 5,5
6,0 5,6–6,0 100, 150, 200 6,0
6,7 6,1–6,7 100, 150, 200 7,0
Größe – Bypasslänge
Läsionslänge (cm)
Anz. der Stentgrafts
Stentgraft 1 Nennlänge
(mm)
Stentgraft 2 Nennlänge
(mm)
Stentgraft 3 Nennlänge
(mm)
15–17 2 150* 150 n. v.
100 200 n. v.
18–22 2 200 150 n. v.
23–26 2 200 200 n. v.
27–32 3 200* 150 150
3 200 200 100
32+ 3 200 200 200 *Idealkonfiguration
Warnungen
• Nur zur einmaligen Verwendung. Nicht wiederverwenden, wieder-aufbereiten oder erneut sterilisieren. Die Wiederverwendung, Wiederaufbereitung oder erneute Sterilisation kann die strukturelle Integrität des Geräts beeinträchtigen und/oder das Versagen des Geräts verursachen, was wiederum zu Verletzung, Krankheit oder Tod des Patienten führen kann. Die Wiederverwendung, Wiederaufbereitung oder erneute Sterilisation kann außerdem das Kontaminationsrisiko des Geräts erhöhen und/oder zu Infektionen des Patienten oder Kreuzkontaminationen führen, einschließlich, aber nicht beschränkt auf die Übertragung von Infektionskrankheiten zwischen Patienten. Die Kontamination des Geräts kann zu Verletzung, Krankheit oder Tod des Patienten führen.
• Das Torus Stentgraft-System muss unter visueller Führung (z. B. Fluoroskopie) von einem qualifiziertem Arzt in perkutanen, intravaskulären Verfahren in einem vollständig ausgestattetem Katheterlabor durchgeführt werden.

IFU 108-F Page 19 of 45
• Das Torus Stentgraft-System nicht verwenden, wenn die Verpackung geöffnet oder beschädigt ist.
• Das Torus Stentgraft-System nicht nach Ablauf des auf der Verpackung verzeichneten Verfallsdatum verwenden.
• Vor der Implantation ist darauf zu achten, dass die geeigneten Stentgraft-Größen ausgewählt werden. Die Größe des nativen Gefäßes muss exakt abgemessen und darf nicht geschätzt werden.
• Den SG nicht kanülieren oder punktieren. Das Kanülieren oder Punktieren des SG kann Schäden der ePTFE-Beschichtung und/oder des NitinolRahmens verursachen und zu einer eingeschränkten Leistung oder dem Versagen des SG führen.
• Den SG nicht durchschneiden oder versuchen, chirurgisch zu implantieren. Der SG darf ausschließlich mit dem Torus Stentgraft-System, auf das er vorgeladen ist, platziert und expandiert werden.
• Die unbeabsichtigte, teilweise oder fehlgeschlagene Expandierung oder Migration des SG kann einen chirurgischen Eingriff erforderlich machen.
Vorsichtsmaßnahmen
• Das Torus Stentgraft-System an einem kühlen, trockenen Ort vor Sonnenlicht geschützt aufbewahren.
• Das Torus Stentgraft-System vor dem Gebrauch überprüfen. Das Gerät nicht verwenden, wenn es in irgendeiner Weise verbogen, geknickt oder beschädigt aussieht.
• Das Torus Stentgraft-System nicht mit organischen Lösungsmitteln (z. B. Alkohol) in Kontakt bringen.
• Das Torus Stentgraft-System nur mit einem 0,035″-Führungsdraht mit einer Mindestlänge von 300 cm verwenden.
• Das Torus Stentgraft-System ausschließlich mit mindestens einer 8F-Schleuse verwenden.
• Vor der Platzierung des SG sollte mit der Verabreichung von Thrombozytenaggregationshemmern begonnen werden. Eine wirksame Antikoagulationstherapie sollte in einer vom Arzt empfohlenen Dosierung fortgeführt werden.
• Das Torus Stentgraft-System-Produkt und die Verpackung nach dem Gebrauch gemäß den Krankenhausvorschriften, Verwaltungs-bestimmungen und/oder lokalen gesetzlichen Regulierungen entsorgen.

IFU 108-F Page 20 of 45
MRT-Sicherheit und -Kompatibilität Bedingt MRT-tauglich Außerklinische Tests zum SG haben erwiesen, dass das Gerät bedingt MRT-tauglich ist. Patienten mit diesem Gerät können sich in MRT-Systemen, die die folgenden Bedingungen erfüllen, sicher einer MRT-Untersuchung unterziehen:
• Statisches Magnetfeld von 1,5 T. • Maximaler räumlicher Gradient des Magnetfelds von 3.000 G/cm
(30 T/m). • Berichtete maximale MRT-Rate, durchschnittliche Ganzkörper-SAR
(spezifische Absorptionsrate) von 2 W/kg (Normalbetriebsmodus). Unter den oben angegebenen Scanbedingungen ist davon auszugehen, dass der SG bei 15-minütigem kontinuierlichen Scannen einen maximalen Temperaturanstieg von weniger als 1 ºC erzeugt. Tests zu den Bildartefakten in Gerätenähe wurden nicht durchgeführt. Die Artefaktgröße ist nicht bekannt und kann dazu führen, dass MRT-Bildmerkmale in der Nähe des Gerätes erheblich verdeckt werden.
Mögliche Komplikationen
• Verfahrensbezogen: W Diese Komplikationen beinhalten, sind jedoch nicht beschränkt auf: Zugangsgefäßverschluss (arteriell/venös); Amputation; Aneurysma oder Pseudoaneurysma; arteriovenöse Fistel; Blutungskomplikationen; Tod; Geräte oder Ausfahr Funktionsstörung / Ausfall; Nebenwirkungen der Thrombozytenaggregationshemmer oder des Kontrastmittels; Embolie (peripher oder pulmonal); Fieber ohne Vorliegen einer Infektion; Hämorrhagie oder Hämatom; Hypotonie/Hypertonie; lokale oder systemische Infektion, einschließlich Bakteriämie oder Sepsis; Malapposition oder Migration; Fehlstellung; Myokardinfarkt; Schmerz (Einführungsstelle, Bein und/oder Fuß); Niereninsuffizienz oder Versagen als Begleiterscheinung des Kontrastmittels; Schock; Seitenastverschluss; Schlaganfall oder transient-ischämische Attacke; Thrombose; Gefäßwandtrauma (Dissektion, Perforation oder Ruptur); Gefäßspasmus; Störung des venösen Flusses (tiefe Venenthrombose, Phlebitis, Beinschwellung und/oder Entstehung von Krampfadern); und/oder Verschlechterung der Claudicatio.
• Gerätebezogen: Diese Komplikationen beinhalten, sind jedoch nicht darauf beschränkt: Zugangsgefäßverschluss (arteriell/venös); Amputation; Aneurysma oder Pseudoaneurysma; arteriovenöse Fistel; Blutungskomplikationen; Tod; Funktionsstörung/Ausfall des Geräts oder beim Ausfahren; Embolie (peripher oder pulmonal); Fieber ohne Vorliegen einer Infektion; Hämorrhagie oder Hämatom; lokale oder

IFU 108-F Page 21 of 45
systemische Infektion, einschließlich Bakteriämie oder Sepsis; Malapposition oder Migration; Fehlstellung; Myokardinfarkt; Schmerz (Einführungsstelle, Bein und/oder Fuß); Seitenastverschluss; Schlaganfall oder transient-ischämische Attacke; Thrombose; Gefäßwandtrauma (Dissektion, Perforation oder Ruptur); Gefäßspasmus; Störung des venösen Flusses (tiefe Venenthrombose, Phlebitis, Beinschwellung und/oder Entstehung von Krampfadern); und/oder Verschlechterung der Claudicatio.
Lieferzustand
Das Torus Stentgraft-System wird in sterilem Zustand geliefert und ist
ausschließlich für eine einmalige Verwendung vorgesehen.
Gebrauchsanweisung – Platzierung des Führungsdrahts für das DETOUR-Verfahren
Vorbereitung
• Das Anastomosensystem und das Schlingenkäfigsystem auf Schäden untersuchen. Das Gerät nicht verwenden, wenn die Verpackung geöffnet oder beschädigt ist.
• Unter Anwendung steriler Technik das Anastomosensystem und das Schlingenkäfigsystem aus der Verpackung entnehmen und in das sterile Feld legen. Die Katheter auf sichtbare Anzeichen von Schäden untersuchen.
• Das Anastomosensystem durchspülen und den äußeren Griff vorschieben, um den Stabilisator auszufahren und die Nadel durch Betätigen der Taste einzuführen. Den äußeren Griff nach Einführen der Nadel zurückziehen, indem der Stabilisator eingeklappt und das Anastomosensystem wieder in die neutrale Position gestellt wird.
WARNUNG: Die Finger oder andere Körperteile von der distalen Spitze des Anastomosensystems vor der Einführung der Nadel fernhalten.
• Das Schlingenkäfigsystem ausspülen, die äußere Schleuse zurückziehen und den proximalen Griff vorschieben, um die Funktion des Nitinol-Rahmens zu überprüfen. Die äußere Schleuse erneut über den Nitinol-Rahmen vorschieben.
Vaskuläre Ziele isolieren
1. Über den perkutanen Gefäßzugang der Vena tibialis einen Zugang zur

IFU 108-F Page 22 of 45
Vena femoralis (VF) herstellen und eine 7Fr-Schleuse platzieren.
2. Einen 0,014”-Führungsdraht über die hinteren Führungsdrahtöffnung laden und das Schlingenkäfigsystem durch die 7Fr-Schleuse vorschieben.
3. Das Schlingenkäfigsystem ipsilateral in die VF direkt über der arteriellen Läsion vorschieben und den Nitinol-Rahmen platzieren.
4. Standardmäßigen kontralateralen Zugang zur Arteria femoralis mit Standardtechniken herstellen und eine 8Fr-Schleuse platzieren.
5. Einen 300 cm langen 0,014″-Führungsdraht durch das Lumen des hinteren Nadelführungsdrahts des Anastomosensystems laden und vorschieben, bis die distale Spitze sichtbar ist, dann ungefähr 5 cm zurückziehen.
6. Die RX-Öffnung mit 0,014″-Führungsdraht backloaden und das Anastomosensystem bis zur Läsion in der AF vorschieben.
Proximale Anastomose herstellen
1. Den Fluoroskopiekopf drehen, um die Vena femoralis über die Arteria femoralis zu legen, indem die lateralen und kranialen/kaudalen Ebenen angepasst werden, um die Überlappung der VF und AF zu optimieren.
2. Um 90 Grad in die eine oder andere Richtung drehen, um die Gefäße in der planaren Ansicht rechtwinklig anzuzeigen.
3. Das Anastomosensystem mithilfe des Kronen-Markierungsbandsystems am oberen Nitinol-Rahmen in der VF ausrichten.
4. Das System gegen den Uhrzeigersinn drehen und den Außengriff nach vorne schieben, bis der Stabilisator ausgefahren und der Außengriff eingerastet ist. Die Ausrichtung des Anastomosensystems erneut kontrollieren. Bei unangemessener Ausrichtung den Außengriff zurückziehen und den Vorgang wiederholen, bis mit dem ausgefahrenen Stabilisator eine geeignete Ausrichtung erreicht ist.
WARNUNG: Das Anastomosensystem mit dem ausgefahrenen Stabilisator nicht drehen.
5. Die Taste drücken, um die Nadel in die angrenzende VF einzuführen.
WARNUNG: Hand und Finger auf den Innengriff legen (nicht auf die
Öffnung für den Führungsdraht), um zu vermeiden, dass während des
Ausfahrens der Nadel Handschuhe durchstochen werden.
6. Den 300 cm langen 0,014″-Führungsdraht durch die Nadel führen, um den Zugang zur VF zu bestätigen. Die Schritte 2–5 wiederholen, bis der

IFU 108-F Page 23 of 45
Venenzugang gesichert ist.
VORSICHT: Den Führungsdraht vor Einsatz der Nadel nicht weit durch
die Nadelspitze vorschieben. Dies könnte das Gerät beschädigen.
HINWEIS: Wenn die Nadel des Anastomosensystems beide Wände der
Zielvene durchsticht, die Nadel mit dem Außengriff teilweise zurück
ziehen und den Führungsdraht in die Vene vorschieben.
7. Die Nadel mit dem Außengriff zurückziehen und den Führungsdraht im oberen Nitinol-Rahmen fangen, indem das proximale Schlingenkäfigsystem zurückgezogen und die äußere Schleuse vorgeschoben wird.
VORSICHT: Nicht versuchen, den Führungsdraht mit der Schlinge zu fassen, solange die Nadel des Anastomosensystems ausgefahren ist. Andernfalls können die Geräte beschädigt werden. VORSICHT: Nicht versuchen, den Führungsdraht mit dem unteren Nitinol-Rahmen zu fangen. Wenn der Führungsdraht mit dem unteren Schlingenkäfig gefangen wird, den Führungsdraht und die Nitinol-Rahmen zurückziehen, den Schlingenkäfig erneut positionieren und den Prozess wiederholen, bis der Draht mit dem oberen Nitinol-Rahmen gefangen ist.
VORSICHT: Den Führungsdraht nicht zu weit über den oberen Nitinol-Rahmen hinaus schieben. Ein zu langes Stück Führungsdraht kann verhindern, dass die äußere Schleuse über den Nitinol-Rahmen geschoben werden kann, und somit das Gerät beschädigen.
8. Den Schlingenkäfig durch den Venenzugang zurückziehen.
9. Das Anastomosensystem zurückziehen und dabei darauf achten, dass das distale Ende des Führungsdrahts außerhalb des ipsilateralen Venenzugangs bleibt.
WARNUNG: Darauf achten, dass der Stabilisator und die Nadel
eingefahren sind, bevor das Anastomosensystem entfernt wird.
10. Die äußere Schleuse einfahren und mit den Nitinol-Rahmen den eingefangenen Führungsdraht aus dem Schlingenkäfig entfernen.
11. Den Führungsdraht auf Schäden untersuchen.
Distale Anastomose herstellen
1. Den Schlingenkäfig erneut über den Führungsdraht in der VF vorschieben

IFU 108-F Page 24 of 45
und den oberen Nitinol-Rahmen distal zur Läsion ausfahren. VORSICHT: Darauf achten, dass die äußere Schleuse über den
expandierten Nitinol-Rahmen positioniert ist, bevor sie durch die
Einführungsschleuse vorgeschoben wird.
2. Einen 300 cm langen 0,014″-Führungsdraht durch das Lumen des hinteren Nadelführungsdrahts des Anastomosensystems laden und vorschieben, bis die distale Spitze sichtbar ist, dann ungefähr 5 cm zurückziehen.
3. Den Führungsdraht über die RX-Öffnung des Anastomosensystems backloaden und das Anastomosensystem erneut zur proximalen Anastomose vorschieben.
4. Den Führungsdraht an beiden Zugängen gespannt halten und das Anastomosensystem vorsichtig durch die proximale Anastomose in die VF einführen.
WARNUNG: Den Stabilisator nicht ausfahren, bevor die proximale
Anastomose erreicht ist
WARNUNG: Auf dem Weg durch die Anastomose keine übermäßige
Kraft ausüben. Den Führungsdraht an beiden Zugängen gespannt
halten und das Anastomosensystem vorsichtig vorschieben, bis der
VF-Zugang fluoroskopisch bestätigt ist.
5. Das Anastomosensystem über den Draht vorschieben, bis es die Spitze des Schlingenkäfigsystems berührt.
6. Die Schritte 1–3 aus den Anweisungen zur proximalen Anastomose wiederholen, um eine rechtwinklige Ansicht der VF und der Zielarterie (entweder AF der Arteria poplitea) zu erhalten.
7. Mit dem Kronen-Markierungsbandsystem das Anastomosensystem zur AF/Arteria poplitea ausrichten.
8. Die äußere Schleuse vorschieben, bis der Stabilisator ausgefahren ist und die äußere Schleuse drehen, bis sie einrastet. Ausrichtung des Anastomosensystems erneut überprüfen und nötigenfalls anpassen.
9. Die Taste drücken, um die Nadel durch die Venen- und Arterienwände und in die angrenzende AF/Arteria poplitea einzuführen.
WARNUNG: Wenn die Nadel des Anastomosensystems beide Wände
der Zielarterie durchsticht, die Nadel mit dem Außengriff teilweise
zurückziehen und den Führungsdraht in die Arterie vorschieben.

IFU 108-F Page 25 of 45
10. Den 300 cm langen Führungsdraht durch die Nadel führen, um den Arterienzugang zu bestätigen. Bei Bedarf die Schritte 7–9 wiederholen, um die Platzierung des Führungsdrahts in der Zielarterie zu kontrollieren.
VORSICHT: Den Führungsdraht nicht distal zum Austrittsfenster der
Nadel vorschieben, bevor die Nadel ausgefahren ist. Andernfalls
könnte das Gerät beschädigt werden.
11. Den Schlingenkäfig durch den Venenzugang zurückziehen.
12. Das Anastomosensystem zurückziehen und dabei darauf achten, dass die distale Position des Führungsdrahts in der Arterie beibehalten wird.
WARNUNG: Darauf achten, dass der Stabilisator und die Nadel
eingefahren sind, bevor das Anastomosensystem entfernt wird.
Gebrauchsanweisung – Platzierung des Torus Stentgraft für das DETOUR-Verfahren
Größen und Auswahl des Stentgrafts 1. Vor dem Öffnen der sterilen Verpackung überprüfen, dass der
Durchmesser und die Länge des SG korrekt sind.
2. Die geeigneten SG-Durchmesser für die distalen und proximalen Gefäße mit der unter „Größen“ angegebenen Tabelle auswählen.
3. Die geeigneten SG-Längen basierend auf der Länge des gewählten Bypasses auswählen.
A. Die unter „Größen“ angegebenen Längen sind die Nennlängen für Stentgrafts.
B. Es ist wichtig, dass der Stentgraft mindestens 3 cm des Arterienlumens sowohl an der distalen als auch der proximalen Seite der Läsion belegt.
4. Bei sich überschneidenden (ineinander schiebbaren) Grafts ist eine Überlappung von mindestens 6 cm erforderlich.
A. Ein 5,5 mm langer SG kann nur proximal in einen 5,5 mm langen SG platziert werden.
B. Ein 6,0 mm langer SG kann proximal in einen 5,5 mm oder 6,0 mm langen SG platziert werden.
C. Ein 6,7 mm langer SG kann proximal in einen 6,0 mm oder

IFU 108-F Page 26 of 45
6,7 mm langen SG platziert werden.
Medikation Die Vorbereitung von Patienten auf die Implantation eines SG sollte die orale Verabreichung von Thrombozytenaggregationshemmern in geeigneter Dosierung vor und nach dem chirurgischen Eingriff beinhalten. Eine wirksame Antikoagulationstherapie sollte während des gesamten chirurgischen Eingriffs und, nach Ermessen des behandelnden Arztes, postoperativ fortgeführt werden.
Vorbereitung 1. Den Beutel des Torus Stentgraft-Systems auf Schäden untersuchen.
Das Gerät nicht verwenden, wenn die Verpackung geöffnet oder beschädigt ist.
2. Unter Anwendung steriler Technik das Gerät aus der Verpackung entnehmen und in das sterile Feld legen. Das Gerät auf sichtbare Anzeichen von Schäden untersuchen.
VORSICHT: Den SG nicht vor dem Einführen ausfahren. Der SG ist selbstexpandierend und kann im Einführsystem nicht erneut geladen werden.
3. Das Lumen des Führungsdrahts mit dem Luer-Konnektor am proximalen Ende des Geräts mit heparinisierter Kochsalzlösung durchspülen, bis die Flüssigkeit aus der Katheterspitze austritt.
4. Das SG-Lumen über die Spülöffnung auf dem Gerätegriff durchspülen, bis die Flüssigkeit an den Enden des Torus Stentgraft-Systems proximal zur Stelle des SG austritt.
Platzierung des Stentgrafts
1. Das Torus Stentgraft-System mithilfe eines 0,035”-Führungsdrahts einführen und bis zur Behandlungsstelle vorschieben.
2. Das Torus Stentgraft-System durch die proximalen und distalen Anastomosen führen.
WARNUNG: Auf dem Weg durch die Anastomose keine übermäßige Das Torus Stentgraft-System vorsichtig vorschieben, bis der distale Arterienzugang fluoroskopisch gesichert ist. Die Anastomose erneut dilatieren, wenn signifikanter Widerstand festgestellt wird.

IFU 108-F Page 27 of 45
3. Das distale Markierungsband des Torus Stentgraft-Systems mindestens 3 cm distal zur distalen Anastomose führen, wobei das proximale Markierungsband im VF bleibt.
4. Den Griff des Torus Stentgraft-Systems flach zum Tisch mit dem Stellrad nach oben zeigend halten und das Rad in Pfeilrichtung drehen, um den Stentgraft zu expandieren.
5. Das Torus Stentgraft-System entfernen.
VORSICHT: Beim Entfernen des Einführsystems darauf achten, die
Position des SG nicht zu verändern.
6. Das zweite Torus Stentgraft-System mithilfe desselben Führungsdrahts einführen und durch die proximale Anastomose schieben.
7. Das distale Markierungsband ungefähr 6 cm im expandierten Stentgraft und das proximale Markierungsband mindestens 3 cm proximal zur proximalen Anastomose in der AFS positionieren. Nachdem die Position an beiden Stellen kontrolliert wurde, den Stentgraft expandieren und den Bypass abschließen.
8. Das Torus Stentgraft-System entfernen.
VORSICHT: Beim Entfernen des Einführsystems darauf achten, die
Position des SG nicht zu verändern.
9. Wenn ein dritter Stentgraft für den Bypass nötig ist, diesen dritten Stentgraft über denselben Führungsdraht einführen und bis zur proximalen Anastomose vorschieben.
10. Das distale Markierungsband ungefähr 6 cm im expandierten Stentgraft und das proximale Markierungsband mindestens 3 cm proximal zur proximalen Anastomose in der AFS positionieren. Nachdem die Position an beiden Stellen kontrolliert wurde, den Stentgraft expandieren und den Bypass anlegen.
WARNUNG: Beim Expandieren des proximalen Stentgrafts sicherstellen, dass der proximale Rand (exponiertes Ende) des Stentgrafts 1–2 mm über dem Ostium der Arteria femoralis superficialis sitzt (Abbildung 4).

IFU 108-F Page 28 of 45
Abbildung 4: Optimale Position des proximalen SG-Endes
11. Das Torus Stentgraft-System entfernen.
12. Den Stentgraft auf der gesamten Länge mit den unter „Größen“ genannten Ballons dilatieren.
WARNUNG: Nicht über die Ränder des/der expandierten Stentgraft(s) hinaus dilatieren.
13. Den Führungsdraht entfernen und mit den Gefäßverschlüssen fortfahren.
Entsorgung
Das Produkt und die Verpackung nach dem Gebrauch gemäß den
Krankenhausvorschriften, Verwaltungsbestimmungen und/oder lokalen
gesetzlichen Regulierungen entsorgen.
Lagerung und Handhabung
Die Geräte an einem kühlen, trockenen Ort vor Sonnenlicht geschützt
aufbewahren.
Ca. Rand der SG-Länge: 7,638 mm

IFU 108-F Page 29 of 45
Definition der Symbole
Chargennummer
Siehe Gebrauchsanweisung
Hersteller
Nicht erneut sterilisieren
Nicht erneut verwenden
Mit Ethylenoxid sterilisiert
Katalognummer
Vorsicht
Vor Sonnenlicht geschützt
aufbewahren
Verfallsdatum
Nicht verwenden, wenn Packung beschädigt ist
Enthält oder Anwesenheit
von Phthalaten
Autorisierter Europäischer
Vertreter
Trocken aufbewahren
Bedingt MRT-tauglich
Die Symbole wurden von „ISO 15223 Medizinprodukte – Bei Aufschriften von Medizinprodukten zu verwendende
Symbole, Kennzeichnung und zu liefernde Informationen“, „ASTM F2503 – Standardpraxis zur Kennzeichnung von
Medizinprodukten und sonstigen Geräten bezüglich ihrer Sicherheit in der Magnetresonanzumgebung“ und „EN 15986
Symbol zur Kennzeichnung von Medizinprodukten – Anforderungen zur Kennzeichnung von phthalathaltigen
Medizinprodukten“ abgeleitet.
Hersteller und Vertreter in der EG
PQ Bypass, Inc. 1971 Milmont Drive Milpitas, CA 95035 USA
HealthLink Europe BV De Tweeling 20-22
5215 MC’s-Hertogenbosch Niederlande
2797

IFU 108-F Page 30 of 45
SYSTEM STENTGRAFTÓW TORUS
INSTRUKCJA STOSOWANIA Opis wyrobu System stentgraftów Torus jest wyrobem do użytku
wewnątrznaczyniowego. Jest on wprowadzany do wnętrza naczynia za
pomocą cewnika o niewielkiej średnicy w celu poprawy ukrwienia przy
niedrożności udowo-podkolanowej. W przypadku użycia z pętlą PQ i
systemem wprowadzającym PQ, Torus jest przeznaczony do pełnego
pomostowania przezskórnego (procedura OBEJŚCIA) za pośrednictwem
kanału wewnątrznaczyniowego prowadzonego od początku tętnicy udowej
powierzchownej, przez sąsiadującą żyłę udową i z powrotem do światła
tętnicy przy dystalnej lokalizacji rekonstrukcji (Rysunek 1).
System stentgraftów Torus składa się ze stentgraftu (Rysunek 2) oraz
cewnika wprowadzającego (Rysunek 3). Stentgraft (SG) jest
samorozprężalną endoprotezą składającą się z elastycznej,
samorozprężalnej konstrukcji kompozytowej wykonanej z ramy z Nitinolu
(NiTi = nikiel:tytan) umieszczonej w folii z ekspandowanego
politetrafluoroetylenu (ePTFE). Stentgraft jest fabrycznie zamocowany na
cewniku wprowadzającym w systemie OTW 8Fr, zgodnym z prowadnikiem
0,035” o długości roboczej wynoszącej 135 cm. Rękojeść systemu
wprowadzania obejmuje wewnętrzny mechanizm koła pasowego
aktywowany poprzez obracanie pokrętła zewnętrznego. Po umieszczeniu
stentgraftu w miejscu docelowym użytkownik może przesunąć koszulkę
zewnętrzną proksymalnie, obracając pokrętło, aby rozprężyć stentgraft.
PRZESTROGA – WYRÓB BADANY. ZASTOSOWANIE
OGRANICZONE DO BADANIA NA MOCY PRAWA
FEDERALNEGO LUB AMERYKAŃSKIEGO
PL

IFU 108-F Page 31 of 45
Rysunek 1: Procedura OBEJŚCIA z użyciem systemu stentgraftu
Torus
Rysunek 2: Stentgraft Torus
Rysunek 3: System wprowadzający Torus
Żyła udowa
Stentgraf torus
Kolano
Niedrożność
Tętnica udowa
powierzchowna

IFU 108-F Page 32 of 45
Wskazania do stosowania System stentgraftu Torus jest przeznaczony do poprawy przepływu krwi u pacjentów z objawową chorobą tętnic obwodowych spowodowaną okluzjami o długości > 15 cm i rozsianą stenozą tętnic udowo-podkolanowych, w tym restenozą wewnątrz stentu, przy referencyjnych średnicach naczyń 5,0–6,7x mm. Przeciwwskazania Stosowanie systemu stentgraftu Torus jest przeciwwskazane w naczyniach wieńcowych i mózgowych. Stosowanie procedury OBEJŚCIA jest przeciwwskazane u pacjentów z:
• zakrzepicą żył głębokich w wywiadzie;
• drożną żyłą udową < 10 mm średnicy i bez duplikowanej żyły udowej;
• nieleczoną chorobą okluzyjną aortalno-biodrową ograniczającą przepływ;
• brakiem drożnego naczynia odprowadzającego; • znane nadwrażliwości, alergie i przeciwwskazania do
stosowania: nitinolu, PTFE, aspiryny, heparyny, leków przeciwzakrzepowych, leków przeciwpłytkowych, leczenia trombolitycznego lub środków przeciwzakrzepowych i kontrastu.
Katalogowe numery referencyjne
Numer katalogowy Opis
TO-5.5X200 System stentgraftów Torus – 5,5 mm × 200 mm
TO-6.0X100 System stentgraftów Torus – 6,0 mm × 100 mm
TO-6.0X150 System stentgraftów Torus – 6,0 mm × 150 mm
TO-6.0X200 System stentgraftów Torus – 6,0 mm × 200 mm
TO-6.7X100 System stentgraftów Torus – 6,7 mm × 100 mm
TO-6.7X150 System stentgraftów Torus – 6,7 mm × 150 mm
TO-6.7X200 System stentgraftów Torus – 6,7 mm × 200 mm

IFU 108-F Page 33 of 45
Określanie rozmiaru – średnica naczynia
Średnica wyrobu
podana na etykiecie
(mm)
Zalecana średnica naczynia
(mm)
Dostępne nominalne długości
wyrobu (mm)
Zalecana średnica balonika do postdylatacji (mm)
5,5 5,0–5,5 200 5,5
6,0 5,6–6,0 100, 150, 200 6,0
6,7 6,1–6,7 100, 150, 200 7,0
Określanie rozmiaru – długość pomostu tętniczego (bypassu)
Długość zmiany
(cm)
Liczba stentgraftów
Długość nominalna
stentgraftu 1 (mm)
Długość nominalna
stentgraftu 2 (mm)
Długość nominalna stentgraftu 3
(mm)
15–17 2 150* 150 Nd.
100 200 Nd.
18–22 2 200 150 Nd.
23–26 2 200 200 Nd.
27–32 3 200* 150 150
3 200 200 100
32+ 3 200 200 200 *Konfiguracja preferowana
Ostrzeżenia
• Tylko do jednorazowego użytku. Nie stosować, nie przetwarzać ani nie sterylizować ponownie. Ponowne zastosowanie, przetwarzanie lub sterylizacja mogą uszkodzić strukturalną integralność wyrobu i/lub prowadzić do nieprawidłowego działania wyrobu, co z kolei może spowodować obrażenia ciała, chorobę lub śmierć pacjenta. Ponowne zastosowanie, przetwarzanie lub sterylizacja mogą również powodować ryzyko skażenia wyrobu i/lub powodować zakażenia lub zakażenia krzyżowe u pacjentów, w tym między innymi przenoszenie chorób zakaźnych pomiędzy pacjentami. Skażenie wyrobu może prowadzić do obrażeń ciała, choroby lub śmierci pacjenta.
• System stentgraftów Torus należy stosować pod kontrolą wzrokową (np. za pomocą fluoroskopii) przez lekarza zaznajomionego z technikami przezskórnymi i dożylnymi we w pełni wyposażonej pracowni cewnikowania.
• Nie stosować systemu stentgraftów Torus, jeśli opakowanie zostało otwarte lub uszkodzone.

IFU 108-F Page 34 of 45
• Nie stosować systemu stentgraftów Torus po upływie daty przydatności do użycia określonej na etykiecie opakowania.
• Należy dołożyć wszelkich starań, aby zapewnić dobór odpowiednich rozmiarów stentgraftów przed implantacją. Wymiary niezmodyfikowanego naczynia należy dokładnie zmierzyć, a nie oszacować.
• Nie kaniulować ani nie przebijać stentgraftu. Kaniulowanie lub przebijanie stentgraftu może uszkodzić powłokę ePTFE i/lub ramę NiTi, powodując pogorszenie działania lub niesprawność stentgraftu.
• Nie przecinać stentgraftu ani nie podejmować prób przeprowadzenia chirurgicznej implantacji stentgraftu. Stentgraft należy implantować i wprowadzać wyłącznie za pomocą systemu stentgraftów Torus, w którym jest umieszczony.
• Przypadkowe, częściowe lub nieudane wprowadzenie bądź przemieszczenie stentgraftu może wymagać interwencji chirurgicznej.
Środki ostrożności
• System stentgraftów Torus należy przechowywać w chłodnym i suchym środowisku z dala od bezpośredniego światła słonecznego.
• Sprawdzić system stentgraftów Torus przed użyciem. Nie stosować, jeśli system wydaje się być wygięty, skręcony lub uszkodzony w jakikolwiek sposób.
• Nie narażać systemu stentgraftów Torus na działanie rozpuszczalników organicznych (np. alkoholu).
• System stentgraftów Torus należy stosować wyłącznie z prowadnikiem 0,035″ o minimalnej długości 300 cm.
• System stentgraftów Torus należy stosować wyłącznie z koszulką 8F lub większą.
• Terapię przeciwpłytkową należy rozpocząć przed wprowadzeniem SG. Skuteczna terapia przeciwkrzepliwa powinna być kontynuowana z wykorzystaniem takich dawek, jakie lekarz uzna za odpowiednie.
• Po użyciu produkt i opakowanie systemu stentgraftów Torus należy poddać utylizacji zgodnie z polityką szpitala, polityką administracyjną lub lokalną polityką ustawową.

IFU 108-F Page 35 of 45
Bezpieczeństwo i zgodność z obrazowaniem MR: Warunkowo bezpieczne podczas obrazowania MR Badania niekliniczne stentgraftu wykazały, że wyrób jest warunkowo bezpieczny podczas obrazowania MR. Pacjenci, u których wszczepiono ten wyrób, mogą bezpiecznie przejść badanie rezonansem magnetycznym przy spełnieniu następujących warunków:
• Statyczne pole magnetyczne 1,5 T. • Maksymalny gradient przestrzenny pola 3000 G/cm (30 T/m). • Maksymalny zgłaszany przez system MR współczynnik absorpcji
specyficznej (SAR) uśredniony dla całego ciała 2 W/kg (normalny tryb roboczy).
Oczekuje się, że w opisanych powyżej warunkach skanowania stentgraft wywoła maksymalny wzrost temperatury mniejszy niż 1ºC po 15 minutach ciągłego skanowania. Nie przeprowadzano badań pod kątem artefaktów obrazów w pobliżu wyrobu. Nie jest znana wielkość artefaktów i może ona znacząco przesłaniać cechy obrazu MR w sąsiedztwie wyrobu. Możliwe powikłania
• Związane z procedurą: Podobnie jak w przypadku wszelkich innych zabiegów wykorzystujących techniki wprowadzania cewnika do naczynia krwionośnego, mogą wystąpić powikłania. Do tych powikłań zalicza się między innymi: niedrożność naczynia dostępowego (tętnicy/żyły); amputację; tętniaka lub tętniaka rzekomego; przetokę tętniczo-żylną; powikłania krwotoczne; zgon; nieprawidłowe działanie/awarię urządzenia lub nieprawidłowe wprowadzanie; niepożądane reakcje na leki przeciwpłytkowe lub środek cieniujący; zatorowość (obwodowa lub płucna); gorączka bez objawów infekcji; krwotok lub krwiak; niedociśnienie/nadciśnienie tętnicze; infekcja miejscowa lub ogólnoustrojowa łącznie z bakteriemią lub posocznicą; nieprawidłowa apozycja lub przemieszczenie; nieprawidłowe umieszczenie; zawał mięśnia sercowego; ból (miejsce wprowadzenia, noga i/lub stopa); niewydolność nerek lub niewydolność wtórna wskutek zastosowania środka cieniującego; wstrząs; niedrożność gałęzi bocznej; udar lub przemijający napad niedokrwienny mózgu; zakrzepica; uraz ściany naczynia (rozwarstwienie, perforacja lub pęknięcie); skurcz naczyń; zaburzenie przepływu żylnego (zakrzepica żył głębokich, zapalenie żyły, obrzęk nóg i/lub rozwój żylaków); i/lub pogarszające się chromanie.

IFU 108-F Page 36 of 45
• Związane z wyrobem: Przy zastosowaniu każdego wyrobu wewnątrznaczyniowego mogą wystąpić powikłania i zdarzenia niepożądane. Do tych powikłań zalicza się między innymi: niedrożność naczynia dostępowego (tętnicy/żyły); amputację; tętniaka lub tętniaka rzekomego; przetokę tętniczo-żylną; powikłania krwotoczne; zgon; nieprawidłowe działanie/awarię urządzenia lub nieprawidłowe wprowadzanie; zatorowość (obwodowa lub płucna); gorączka bez objawów infekcji; krwotok lub krwiak; infekcja miejscowa lub ogólnoustrojowa łącznie z bakteriemią lub posocznicą; nieprawidłowa apozycja lub przemieszczenie; nieprawidłowe umieszczenie; zawał mięśnia sercowego; ból (miejsce wprowadzenia, noga i/lub stopa); niedrożność gałęzi bocznej; udar lub przemijający napad niedokrwienia mózgu; zakrzepica; uraz ściany naczynia (rozwarstwienie, perforacja lub pęknięcie); skurcz naczyń; zaburzenie przepływu żylnego (zakrzepica żył głębokich, zapalenie żyły, obrzęk nóg i/lub rozwój żylaków); i/lub pogarszające się chromanie.
Sposób dostawy Dostarczany system stentgraftów Torus jest sterylny i przeznaczony wyłącznie do jednorazowego użytku.
Wskazówki dotyczące stosowania – umieszczanie prowadnika w celu przeprowadzenia procedury obejścia
Przygotowanie
1. Sprawdzić opakowanie systemu wprowadzającego PQ i pętli PQ przed użyciem. Nie stosować wyrobu, jeśli opakowanie zostało otwarte lub uszkodzone.
2. Stosując technikę sterylną, wyjąć system wprowadzający PQ i pętlę PQ z opakowania i przenieść do pola sterylnego. Sprawdzić cewniki pod kątem widocznych oznak uszkodzenia.
3. Przepłukać system wprowadzający PQ i przesunąć rękojeść zewnętrzną, żeby upewnić się, że stabilizator działa oraz że igła może zostać wprowadzona poprzez naciśnięcie przycisku. Po wprowadzeniu igły należy wycofać rękojeść zewnętrzną, składając stabilizator i przywracając system wprowadzający PQ do pozycji neutralnej.
OSTRZEŻENIE: Palce i inne części ciała nie powinny znajdować się w pobliżu końcówki dystalnej systemu wprowadzającego PQ przed wprowadzeniem igły.

IFU 108-F Page 37 of 45
4. Przepłukać pętlę PQ, zsunąć koszulkę zewnętrzną i przesunąć rękojeść proksymalną, aby upewnić się, że klatka NiTi działa. Ponownie nałożyć koszulkę zewnętrzną na klatki NiTi.
Odizolowanie naczyń docelowych
1. Uzyskać dostęp do żyły udowej (FV) za pomocą przezskórnego dostępu żylnego w regionie kości piszczelowej i wprowadzić koszulkę 7Fr.
2. Wprowadzić prowadnik 0,014″ przez tylny port prowadnika i przeprowadzić pętlę PQ przez koszulkę 7Fr.
3. Wprowadzić pętlę PQ z tej samej strony do żyły udowej na poziomie nieco powyżej zmiany tętniczej i ustawić klatki NiTi.
4. Uzyskać kontralateralny dostęp do tętnicy udowej wspólnej za pomocą akceptowalnych klinicznie technik naczyniowych i wprowadzić koszulkę 8Fr.
5. Przełożyć prowadnik 0,014″ o długości 300 cm przez tylne światło prowadnika igły systemu wprowadzającego PQ i przesuwać go, dopóki nie pojawi się końcówka dystalna, a następnie wycofać ok. 5 cm.
6. Włożyć prowadnik 0,014″ do portu RX i doprowadzić system wprowadzający PQ do docelowej zmiany w tętnicy udowej.
Utworzyć anastomozę proksymalną
1. Obrócić głowicę fluoroskopu, aby nałożyć żyłę udową na tętnicą udową, dostosowując ustawienie na płaszczyźnie bocznej oraz w płaszczyźnie dogłowowej/doogonowej w celu optymalizacji nałożenia żyły i tętnicy udowej.
2. Obrócić o 90 stopni w dowolnym kierunku w celu uzyskania ortogonalności naczyń w widoku płaskim.
3. Za pomocą systemu pasm znaczników Crown ustawić system wprowadzający PQ w kierunku górnej klatki NiTi w żyle udowej.
4. Obracać w kierunku przeciwnym do ruchu wskazówek zegara i przesuwać rękojeść zewnętrzną do przodu, dopóki stabilizator nie zostanie rozłożony, a rękojeść zewnętrzna odpowiednio zablokowana. Ponownie potwierdzić orientację systemu wprowadzającego PQ. Jeśli orientacja nie jest odpowiednia, wycofać rękojeść zewnętrzną i powtarzać do czasu uzyskania odpowiedniej orientacji przy rozłożonym stabilizatorze.
OSTRZEŻENIE: Nie obracać systemu wprowadzającego PQ, jeśli stabilizator jest rozłożony.

IFU 108-F Page 38 of 45
5. Wcisnąć przycisk, aby wprowadzić igłę do przylegającej żyły udowej (FV).
OSTRZEŻENIE: Położyć dłoń i palce na rękojeści wewnętrznej (nie
w obszarze portu prowadnika), aby uniknąć przyszczypania rękawicy
podczas wprowadzania igły.
6. Wprowadzić prowadnik 0,014″ o długości 300 cm przez igłę, aby potwierdzić dostęp do żyły udowej. Powtarzać kroki 2–5 do czasu potwierdzenia dostępu żylnego.
PRZESTROGA: Nie wysuwać prowadnika przez końcówkę igły przed
wprowadzeniem igły. Może to uszkodzić wyrób.
UWAGA: Jeśli igła systemu wprowadzającego PQ przejdzie przez obie
ściany żyły docelowej, należy ją częściowo wycofać za pomocą
rękojeści zewnętrznej i przesunąć prowadnik, aby uzyskać dostęp do
światła żyły.
7. Wycofać igłę za pomocą rękojeści zewnętrznej i pochwycić prowadnik w dystalnej klatce NiTi, wycofując proksymalną rękojeść pętli PQ i nasuwając koszulkę zewnętrzną.
PRZESTROGA: Nie podejmować prób pochwycenia prowadnika, jeśli igła systemu wprowadzającego PQ jest wysunięta. Może to uszkodzić wyrób. PRZESTROGA: Nie podejmować prób pochwycenia prowadnika za pomocą dolnej klatki NiTi. Jeśli prowadnik zostanie pochwycony przez dolną klatkę, należy go wycofać razem z klatkami, skorygować ustawienie pętli PQ, a następnie powtarzać procedurę pochwycenia do czasu potwierdzenia doprowadzenia pętli do górnej klatki NiTi. PRZESTROGA: Nie należy znacznie wysuwać prowadnika poza górną klatkę NiTi. Długi segment prowadnika może ograniczyć możliwość przesuwania koszulki zewnętrznej nad klatkę NiTi i uszkodzić wyrób.
8. Wyjąć pętlę PQ przez miejsce dostępu żylnego.
9. Wyjąć system wprowadzający PQ, zwracając uwagę na to, aby dystalny fragment prowadnika pozostał na zewnątrz przy miejscu dostępu żylnego.
OSTRZEŻENIE: Należy się upewnić, że igła została wycofana i stabilizator został złożony przed wyjęciem systemu wprowadzającego PQ.

IFU 108-F Page 39 of 45
10. Wyjąć koszulkę zewnętrzną i wprowadzić klatki NiTi w celu wyjęcia pochwyconego prowadnika z pętli PQ.
11. Sprawdzić prowadnik pod kątem uszkodzeń.
Utworzyć anastomozę dystalną
1. Ponownie nasunąć pętlę PQ na prowadnik w żyle udowej i wprowadzić górną klatkę NiTi w kierunku dystalnym względem zmiany.
PRZESTROGA: Należy zwrócić uwagę, aby koszulka zewnętrzna została
ustawiona nad złożonymi klatkami NiTi przed przesunięciem jej przez
koszulkę wprowadzającą.
2. Przełożyć prowadnik 0,014″ o długości 300 cm przez tylne światło prowadnika igły systemu wprowadzającego PQ i przesuwać go, dopóki nie pojawi się końcówka dystalna, a następnie wycofać ok. 5 cm.
3. Umieścić prowadnik w porcie RX systemu wprowadzającego PQ oraz ponownie przesunąć system wprowadzający PQ do anastomozy proksymalnej.
4. Utrzymując naprężenie prowadnika w obu miejscach dostępu, delikatnie przesunąć system wprowadzający PQ przez anastomozę proksymalną do żyły udowej.
OSTRZEŻENIE: Nie rozkładać stabilizatora przed przejściem przez
anastomozę proksymalną.
OSTRZEŻENIE: Nie stosować zbyt dużej siły podczas przechodzenia
przez anastomozę. Zastosować odpowiednie naprężenie prowadnika
w obu miejscach dostępu i delikatnie przesuwać system
wprowadzający do czasu potwierdzenia dostępu do żyły udowej za
pomocą fluoroskopii.
5. Przesunąć urządzenie wprowadzające PQ na prowadniku, dopóki nie zostanie pochwycone przez końcówkę pętli PQ.
6. Powtórzyć kroki 1–3 z instrukcji dotyczącej anastomozy proksymalnej w celu uzyskania widoku prostopadłego żyły udowej i docelowej tętnicy (tętnica udowa albo tętnica podkolanowa).
7. Za pomocą systemu pasm znaczników Crown ustawić system wprowadzający w kierunku tętnicy udowej/podkolanowej.

IFU 108-F Page 40 of 45
8. Przesuwać rękojeść zewnętrzną do przodu, dopóki stabilizator nie zostanie rozłożony, a rękojeść zewnętrzna odpowiednio zablokowana. Ponownie sprawdzić orientację systemu wprowadzającego PQ i w razie potrzeby wyregulować.
9. Wcisnąć przycisk i wprowadzić igłę do przylegającej tętnicy udowej/podkolanowej przez ściany żylne i tętnicze.
OSTRZEŻENIE: Jeśli igła systemu wprowadzającego PQ przejdzie przez
obie ściany tętnicy docelowej, należy ją częściowo wycofać za
pomocą rękojeści zewnętrznej i przesunąć prowadnik, aby uzyskać
dostęp do tętnicy.
10. Wprowadzić prowadnik o długości 300 cm przez igłę, aby potwierdzić dostęp tętniczy. W razie potrzeby powtarzać kroki 7–9 do czasu potwierdzenia umieszczenia prowadnika w tętnicy docelowej.
PRZESTROGA: Nie przesuwać prowadnika w kierunku dystalnym do
światła wyjścia igły przed wprowadzeniem igły. Może to uszkodzić
wyrób.
11. Wyjąć pętlę PQ przez miejsce dostępu żylnego.
12. Wyjąć system wprowadzający PQ, utrzymując pozycję dystalnego prowadnika w tętnicy.
OSTRZEŻENIE: Należy się upewnić, że igła została wycofana i stabilizator został złożony przed wyjęciem systemu wprowadzającego PQ.
Wskazówki dotyczące stosowania – Implantacja stentgraftów Torus w celu przeprowadzenia procedury obejścia
Rozmiar i wybór stentgraftu
1. Przed otwarciem jałowego opakowania sprawdzić, czy średnica i długość stentgraftu są prawidłowe.
2. Wybrać odpowiednie średnice stentgraftów do naczyń dystalnych i proksymalnych, korzystając z tabeli „Rozmiary”.
3. Wybrać odpowiednie długości stentgraftów na podstawie długości proponowanego bypassu.

IFU 108-F Page 41 of 45
A. Długości wymienione w tabeli „Rozmiary” to nominalne długości stentgraftów.
B. Jest ważne, żeby stentgraft znajdował się przynajmniej 3 cm w świetle tętnicy zarówno po stronie dystalnej, jak i proksymalnej zmiany.
4. Podczas nakładania na siebie (teleskopowania) graftów wymagana jest przynajmniej 6-centymetrowa zakładka.
A. Stentgraft 5,5 mm można umieścić proksymalnie wyłącznie w stentgrafcie 5,5 mm.
B. Stentgraft 6,0 mm można umieścić proksymalnie w stentgrafcie 5,5 mm lub 6,0 mm.
C. Stentgraft 6,7 mm można umieścić proksymalnie w stentgrafcie 6,0 mm lub 6,7 mm.
D.
Leki
Przygotowanie pacjentów otrzymujących SG powinno obejmować rozpoczęcie terapii lekami przeciwpłytkowymi w odpowiedniej dawce, przed zabiegiem i po zabiegu. Skuteczna terapia przeciwkrzepliwa powinna być stosowana przez cały czas zabiegu i kontynuowana w okresie pooperacyjnym według uznania lekarza prowadzącego.
Przygotowanie
1. Przed użyciem sprawdzić torebkę zawierającą system stentgraftów Torus pod kątem uszkodzeń. Nie stosować wyrobu, jeśli opakowanie zostało otwarte lub uszkodzone.
2. Stosując technikę sterylną, wyjąć wyrób z opakowania i przenieść do pola sterylnego. Sprawdzić wyrób pod kątem widocznych oznak uszkodzenia.
PRZESTROGA: Nie rozprężać stentgraftu przed wprowadzeniem. Stentgraft jest samorozprężalny i nie można go ponownie umieścić w systemie wprowadzającym.
3. Przepłukiwać światło prowadnika za pomocą złącza Luer na proksymalnym końcu wyrobu roztworem heparynizowanej soli fizjologicznej, aż płyn pojawi się na końcu cewnika.
4. Przepłukiwać światło stentgraftu za pomocą portu do płukania na

IFU 108-F Page 42 of 45
rękojeści urządzenia, aż płyn wypłynie po bokach systemu stentgraftu Torus, proksymalnie do lokalizacji stentgraftu.
Implantacja stentgraftów
1. Nałożyć system stentgraftu Torus na prowadnik 0,035″ i przesunąć go w miejsce zabiegu.
2. Przeprowadzić system stentgraftu Torus przez anastomozę proksymalną i dystalną.
OSTRZEŻENIE: Nie stosować zbyt dużej siły podczas przechodzenia przez anastomozę. Delikatnie przesuwać system stentgraftu Torus, dopóki dostęp tętniczy nie zostanie potwierdzony za pomocą fluoroskopii. Ponownie rozszerzyć anastomozę w przypadku napotkania istotnego oporu.
3. Przeprowadzić dystalne pasmo znacznika systemu stentgraftu Torus w minimalnej odległości dystalnej 3 cm względem anastomozy dystalnej, pozostawiając proksymalne pasmo znacznika w obrębie żyły udowej.
4. Przytrzymać rękojeść systemu stentgraftu Torus płasko na stole, tak aby pokrętło było skierowane w górę, i obrócić je w kierunku wskazanym przez strzałkę w celu rozprężenia stentgraftu.
5. Usunąć system stentgraftów Torus.
PRZESTROGA: Podczas wyjmowania systemu SGDS uważać, aby nie
przesunąć stentgraftu.
6. Nałożyć system stentgraftu Torus na ten sam prowadnik i przesunąć go przez anastomozę proksymalną.
7. Ustawić dystalne pasmo znaczników ok. 6 cm wewnątrz wprowadzonego stentgraftu i proksymalne pasmo znaczników przynajmniej 3 cm proksymalnie w kierunku anastomozy proksymalnej w tętnicy udowej powierzchownej. Po potwierdzeniu pozycji w obu lokalizacjach wprowadzić stentgraft i zakończyć pomostowanie.
8. Usunąć system stentgraftów Torus.
PRZESTROGA: Podczas wyjmowania systemu SGDS uważać, aby nie
przesunąć stentgraftu.
9. Jeśli do wykonania pomostowania potrzebny jest trzeci stentgraft, nałożyć trzeci stentgraft na ten sam prowadnik i przesunąć go przez anastomozę proksymalną.

IFU 108-F Page 43 of 45
10. Ustawić dystalne pasmo znaczników ok. 6 cm wewnątrz wprowadzonego stentgraftu i proksymalne pasmo znaczników przynajmniej 3 cm proksymalnie w kierunku anastomozy proksymalnej w tętnicy udowej powierzchownej. Po potwierdzeniu pozycji w obu lokalizacjach wprowadzić stentgraft i zakończyć pomostowanie.
OSTRZEŻENIE: Podczas wprowadzania stentgraftu proksymalnego należy się upewnić, że proksymalna krawędź (odsłonięty koniec) tego stentgraftu znajduje się 1–2 mm powyżej odejścia tętnicy udowej powierzchownej (Rysunek 4).
Rysunek 4: Optymalna pozycja krawędzi proksymalnej stentgraftu
11. Usunąć system stentgraftów Torus.
12. Rozszerzyć każdy stentgraft na całej długości za pomocą baloników określonych w tabeli „Rozmiary”.
OSTRZEŻENIE: Nie rozszerzać poza marginesy wprowadzonych stentgraftów.
13. Wyjąć prowadnik i wykonać zamknięcie naczynia.
Utylizacja
Po użyciu produkt i opakowanie należy poddać utylizacji zgodnie z polityką
szpitala, polityką administracyjną lub lokalną polityką ustawową.
Proks. krawędź długości
stentgraftu: 7,638 mm

IFU 108-F Page 44 of 45
Przechowywanie i obsługa
Wyroby należy przechowywać w chłodnym i suchym środowisku z dala od
światła słonecznego.
Definicje i symboleop
Kod partii
Patrz instrukcja
użytkowania
Producent
Nie sterylizować ponownie
Nie stosować ponownie
Sterylizowano za
pomocą tlenku etylenu
Numer katalogowy
Uwaga
Chronić przed światłem
słonecznym
Data przydatności do użycia
Nie używać, jeśli
opakowanie jest uszkodzone
Zawiera ftalany lub możliwa obecność
ftalanów
Autoryzowany
przedstawiciel na terenie UE
Przechowywać w suchym miejscu
Warunkowo bezpieczne
podczas obrazowania MR
Symbole pochodzą z dokumentu „ISO 15223 Wyroby medyczne – Symbole do stosowania na etykietach wyrobów medycznych, w ich oznakowaniu i w dostarczanych z nimi informacjach”, „ASTM F2503 – Standardowa praktyka oznaczania bezpieczeństwa wyrobów medycznych i innych elementów w środowisku rezonansu magnetycznego” oraz „EN 15986 Symbole używane w oznakowaniu wyrobów medycznych – Wymagania dotyczące oznakowania wyrobów medycznych zawierających ftalany”.
2797

IFU 108-F Page 45 of 45
Producent i przedstawiciel WE
PQ Bypass, Inc. 1971 Milmont Drive Milpitas, CA 95035 Stany Zjednoczone
HealthLink Europe BV De Tweeling 20-22
5215 MC ‘s-Hertogenbosch Holandia