Embed Size (px)
DESCRIPTION
sellar masses
Citation preview
11/27/2014 Causes, presentation, and evaluation of sellar masses
http://www.uptodate.com/contents/causes-presentation-and-evaluation-of-sellar-masses?topicKey=ENDO%2F6632&elapsedTimeMs=4&view=print&displayedV… 1/15
Official reprint from UpToDate www.uptodate.com ©2014 UpToDate
AuthorPeter J Snyder, MD
Section EditorDavid S Cooper, MD
Deputy EditorKathryn A Martin, MD
Causes, presentation, and evaluation of sellar masses
All topics are updated as new evidence becomes available and our peer review process is complete.Literature review current through: Oct 2014. | This topic last updated: Jan 14, 2014.
INTRODUCTION — Sellar masses typically present in one or more ways:
This topic will review the causes, clinical manifestations, and evaluation of sellar masses. The clinical presentation
and management of individual pituitary tumors and of hypopituitarism are discussed separately. (See appropriate
topic reviews.)
CAUSES — Pituitary adenomas are the most common cause of sellar masses from the third decade on,
accounting for up to 10 percent of all intracranial neoplasms [1-3]. Other disorders, which are often difficult to
distinguish from pituitary adenomas by imaging, include physiologic enlargement of the pituitary and benign and
malignant tumors (table 1).
Pituitary adenomas — Pituitary adenomas are benign tumors of the anterior pituitary, but they are true
neoplasms, as shown by clonality studies [4,5].
Incidence and prevalence — There are few population studies of the incidence and prevalence of pituitary
adenomas. However, a population-based study in Northern Finland, where all patients within a health care district
are referred to a predetermined medical center, found the following standardized incidence rates per 100,000
(cases diagnosed between 1992 and 2007) [6]:
Past studies of pituitary adenomas in the population are thought to have underestimated their true prevalence. In a
current report from a single community of over 80,000 inhabitants in England, the prevalence of pituitary
adenomas per 100,000 was fourfold higher than previous estimates [7]:
Genetics — Classic oncogene mutations are rarely found in pituitary adenomas, but mutations in the following
genes may play a role in the development of one or more types of pituitary adenomas:
®
®
With neurologic symptoms, such as visual impairment or headache●
As an incidental finding on magnetic resonance imaging (MRI) performed for some other reason●
With hormonal abnormalities●
All pituitary adenomas – 4.0●
Lactotroph adenomas – 2.2●
Clinically nonfunctioning adenomas – 1.0●
Somatotroph adenomas – 0.34●
Corticotroph adenomas – 0.17●
All adenomas – 77.6●
Lactotroph adenomas – 44.4●
Nonfunctioning adenomas – 22.2●
Somatotroph adenomas – 8.6●
Corticotroph adenomas – 1.2●
11/27/2014 Causes, presentation, and evaluation of sellar masses
http://www.uptodate.com/contents/causes-presentation-and-evaluation-of-sellar-masses?topicKey=ENDO%2F6632&elapsedTimeMs=4&view=print&displayedV… 2/15
Classification — Adenomas are classified by size and the cell of origin. Lesions smaller than 1 cm are
classified as microadenomas, and lesions larger than 1 cm are classified as macroadenomas. The tumors can
arise from any type of cell of the anterior pituitary and may result in increased secretion of the hormone(s) produced
by that cell and/or decreased secretion of other hormones due to compression of other cell types [15].
Pituitary hyperplasia — There are several recognized causes of hyperplasia of the pituitary. These may present
as sellar masses and be misdiagnosed as pituitary adenomas:
Other benign tumors — Several other benign tumors can occur in or near the sella, including
craniopharyngiomas, meningiomas, and less commonly, pituicytomas.
Craniopharyngioma — Craniopharyngiomas are solid or mixed solid-cystic benign tumors that arise from
remnants of Rathke's pouch along a line from the nasopharynx to the diencephalon. Most are either intrasellar or
suprasellar. About 50 percent present clinically during childhood and adolescence, the other 50 percent present
MEN1 – Loss of function mutations of this tumor suppressor gene appear to be responsible for the tumors
that occur in the parathyroids, pancreatic islets, and pituitary glands of patients who have multiple endocrine
neoplasia type 1 syndrome [8]. However, mutations in this gene do not appear to cause sporadic pituitary
adenomas [9]. (See "Multiple endocrine neoplasia type 1: Definition and genetics".)
●
Gs-alpha – An activating mutation of the alpha subunit of the guanine nucleotide stimulatory protein (Gs-
alpha) gene is found in approximately 40 percent of somatotroph adenomas [10,11]. These mutations result in
constitutive activation of adenylyl cyclase, which may play a role in both cell division and excessive growth
hormone secretion by these adenomas. (See "Causes and clinical manifestations of acromegaly".)
●
PTTG – The pituitary tumor transforming gene, which was cloned from a rat pituitary tumor cell line, is
overexpressed in most human pituitary adenomas compared with nonadenomatous pituitary tissue [12,13].
●
FGF receptor-4 – A truncated form of the receptor for fibroblast growth factor-4 has been identified in human
pituitary adenomas. Transgenic mice that express this mutation in their lactotroph cells develop lactotroph
adenomas [14].
●
Gonadotroph adenomas usually present as clinically nonfunctioning sellar masses. (See "Clinical
manifestations and diagnosis of gonadotroph and other clinically nonfunctioning pituitary adenomas".)
●
Thyrotroph adenomas may present as clinically nonfunctioning sellar masses that secrete only alpha or TSH-
B subunits or may cause hyperthyroidism due to increased secretion of intact thyroid stimulating hormone.
(See "Disorders that cause hyperthyroidism", section on 'TSH-mediated hyperthyroidism'.)
●
Corticotroph adenomas usually cause Cushing's disease. (See "Establishing the cause of Cushing's
syndrome".)
●
Lactotroph adenomas usually cause hyperprolactinemia, which leads to hypogonadism in women and men.
(See "Clinical manifestations and evaluation of hyperprolactinemia".)
●
Somatotroph adenomas typically cause acromegaly due to increased growth hormone secretion. (See
"Causes and clinical manifestations of acromegaly".)
●
Lactotroph/somatotroph adenoma combinations that secrete both prolactin and growth hormone [16] are well
recognized and cause the clinical syndromes of both hormones. Other mixed cell adenomas, sometimes
called plurihormonal adenomas, can involve any combination of cells, but are uncommon.
●
Lactotroph hyperplasia during pregnancy (see "Causes of hyperprolactinemia")●
Thyrotroph and gonadotroph hyperplasia due to long-standing primary hypothyroidism and primary
hypogonadism, respectively [17-21]
●
Somatotroph hyperplasia due to ectopic secretion of growth hormone-releasing hormone [22]●
11/27/2014 Causes, presentation, and evaluation of sellar masses
http://www.uptodate.com/contents/causes-presentation-and-evaluation-of-sellar-masses?topicKey=ENDO%2F6632&elapsedTimeMs=4&view=print&displayedV… 3/15
after age 20, some not until age 70 or 80. The major presenting symptoms are growth retardation in children and
abnormal vision in adults. In addition, pituitary hormonal deficiencies, including diabetes insipidus, are common.
(See "Craniopharyngioma".)
Meningioma — A meningioma is a usually benign tumor arising from the meninges anywhere within the head.
Some arise near the sella, causing visual impairment and hormonal deficiencies. (See "Meningioma: Clinical
presentation and diagnosis".)
Pituicytoma — This is an uncommon, low-grade (WHO grade 1), indolent glioma arising from the pituicytes of
the posterior pituitary. It presents as a sellar mass, which is usually mistaken for a pituitary adenoma, and has no
known hormonal secretory function.
Malignant tumors — Some malignant tumors arise within or near the sella, and others metastasize to this site.
Primary — Malignancies that arise in the parasellar region include germ cell tumors, sarcomas, chordomas,
and lymphomas. Pituitary carcinomas are rare [23].
Metastatic disease — Metastases to the hypothalamus and pituitary gland account for 1 to 2 percent of sellar
masses [1,25]. They occur most commonly with breast cancer in women and lung cancer in men, but can be seen
with many other cancers [26,27]. Symptoms, which occur in approximately 7 percent of patients, include diabetes
insipidus, anterior pituitary dysfunction, visual field defects, retroorbital pain, and ophthalmoplegia [25]. Survival in
36 patients in one series averaged six months [27].
Cysts — Rathke's cleft, arachnoid, and dermoid cysts can produce sellar enlargement, possibly resulting in visual
impairment, diabetes insipidus, anterior pituitary hormonal deficiencies, and hydrocephalus. (See
"Craniopharyngioma".)
Abscess — Pituitary abscesses, which are rare, can occur in a normal or diseased pituitary gland. In a series of 24
patients, 16 (33 percent) presented with symptoms and physical findings consistent with a pituitary mass, while
only eight had features suggestive of infection (fever, leukocytosis, meningismus) [28]. Imaging studies including CT
and MRI were unable to distinguish between pituitary abscess and pituitary adenoma. As a result, most patients
were diagnosed at the time of surgical exploration.
Arteriovenous fistula of the cavernous sinus — Arteriovenous fistulae of the cavernous sinus can cause modest
enlargement of the pituitary gland. Pituitary size returns toward baseline after the fistula is blocked [29].
Hypophysitis — Several types of hypophysitis can enlarge the pituitary early in their course. Lymphocytic
Germ cell tumors – Germ cell tumors, also called ectopic pinealomas, usually occur through the third decade
of life and may present with headache, nausea, vomiting, and lethargy (from increased intracranial pressure in
patients with pineal lesions), diplopia, hypopituitarism or diabetes insipidus (with suprasellar tumors), and
paralysis of upward conjugate gaze (Parinaud's syndrome). Imaging shows a mass in the third ventricle and
serum concentrations of human chorionic gonadotropin-beta (B-hCG), and/or alpha fetoprotein (AFP) may be
increased. Although these lesions are highly malignant and metastasize readily, they are also highly
radiosensitive. (See "Intracranial germ cell tumors".)
●
Chordomas – Chordomas usually are locally aggressive tumors that can metastasize. They often arise in the
clivus and present with headaches, visual impairment, and anterior pituitary hormonal deficiencies. (See
"Chordoma and chondrosarcoma of the skull base", section on 'Chordoma'.)
●
Primary lymphoma – Primary central nervous system (CNS) lymphoma, which sometimes involve the pituitary
and hypothalamus, is an intracranial neoplasm that is being recognized with increasing frequency. A review of
13 patients with pituitary involvement noted neurologic symptoms (headaches and visual and oculomotor
impairment) and/or deficiencies of anterior pituitary hormones and antidiuretic hormone [24]. MRI shows a
sellar mass with variable extrasellar extension. (See "Clinical presentation, pathologic features, and diagnosis
of primary central nervous system lymphoma".)
●
11/27/2014 Causes, presentation, and evaluation of sellar masses
http://www.uptodate.com/contents/causes-presentation-and-evaluation-of-sellar-masses?topicKey=ENDO%2F6632&elapsedTimeMs=4&view=print&displayedV… 4/15
infiltration of the pituitary usually occurs in late pregnancy or the postpartum period, but can also be seen in women
at other times and infrequently in men [30] and increasingly due to anti-CTLA-4 treatment of malignancies [31-33]. It
is characterized by headaches of an intensity out of proportion to the size of the lesion and hypopituitarism, in
which adrenal insufficiency is unusually prominent. (See "Causes of hypopituitarism", section on 'Hypophysitis'.)
CLINICAL MANIFESTATIONS — Sellar masses can present with neurologic symptoms, abnormalities related to
undersecretion or oversecretion of pituitary hormones, or as an incidental finding on radiologic examination
performed for some other reason.
Visual defects — Impaired vision is the most common symptom that leads a patient with a nonfunctioning
adenoma, of which over 80 percent are gonadotroph adenomas, to seek medical attention [34]. (See "Clinical
manifestations and diagnosis of gonadotroph and other clinically nonfunctioning pituitary adenomas".)
Visual impairment is caused by suprasellar extension of the adenoma, leading to compression of the optic chiasm.
The most common complaint is diminished vision in the temporal fields (bitemporal hemianopsia). One or both eyes
may be affected and, if both, to variable degrees. Diminished visual acuity occurs when the optic chiasm is more
severely compressed. Other patterns of visual loss can also occur. Thus, an intrasellar lesion should be suspected
when there is any unexplained pattern of visual loss.
The onset of the visual deficit is usually so gradual that many patients do not seek ophthalmologic consultation for
months or even years. Even at this time, the reason for the deficit may not be recognized, unless a visual field
examination is performed, further delaying the diagnosis.
Other neurologic symptoms — Other neurologic symptoms that may cause a patient with a sellar mass to seek
medical attention include:
Hormone deficiencies — At the time of initial presentation with a neurologic symptom, many patients with sellar
masses, when carefully questioned, admit to symptoms of pituitary hormone deficiencies. However, these
symptoms are not usually the reason that the patient seeks medical attention.
The most common pituitary hormone deficiencies are of gonadotropins, resulting in hypogonadism in both men and
women.
EVALUATION OF A SELLAR MASS — Sellar masses should be evaluated both radiologically and hormonally.
Radiologic procedures
MRI — Magnetic resonance imaging (MRI) is the single best imaging procedure for most sellar masses, and
there is usually no need to perform any other imaging study. Certain MRI findings suggest a greater likelihood of
some kinds of sellar masses than others [35]. As an example, a mass that is separate from the pituitary gland
generally indicates that the mass is not a pituitary adenoma (image 1). However, no finding is usually
pathognomonic of any one kind of mass (image 2).
Unenhanced image — Normal pituitary tissue and most sellar lesions, pituitary adenomas, and other
Headaches, presumably caused by expansion of the sella. The quality of the headache is not specific.●
Diplopia, induced by oculomotor nerve compression resulting from lateral extension of the adenoma.●
Pituitary apoplexy induced by sudden hemorrhage into the adenoma, causing excruciating headache and
diplopia.
●
Cerebrospinal fluid rhinorrhea, caused by inferior extension of the adenoma, an extremely uncommon
presentation.
●
Parinaud syndrome, a constellation of neuroophthalmologic findings, most often paralysis of upward conjugate
gaze, that result from ectopic pinealomas. (See "Supranuclear disorders of gaze in children", section on
'Parinaud syndrome'.)
●
11/27/2014 Causes, presentation, and evaluation of sellar masses
http://www.uptodate.com/contents/causes-presentation-and-evaluation-of-sellar-masses?topicKey=ENDO%2F6632&elapsedTimeMs=4&view=print&displayedV… 5/15
tumors, have a signal that is similar to or slightly greater in intensity than that of central nervous system tissue.
Cystic lesions, such as Rathke's cleft cysts, often have a low intensity signal on T1-weighted images; however,
craniopharyngiomas and even pituitary adenomas may be partially cystic and, therefore, have low intensity signals.
Furthermore, the signal intensity on T1-weighted images will be high if the protein or lipid concentration of the cyst
fluid is high. On T2-weighted images, cystic lesions may have a high intensity signal (image 3). Hemorrhage into
the pituitary gland results in a high intensity signal on both T1- and T2-weighted images.
Meningiomas typically have a brighter and more homogeneous signal than pituitary adenomas. They also have a
suprasellar rather than a sellar epicenter and a dural-based attachment best seen after contrast enhancement [36].
Gadolinium-enhanced image — Normal pituitary tissue takes up gadolinium to a greater degree than
CNS tissue and therefore has a higher intensity signal than the surrounding CNS. Both micro- and macroadenomas
of the pituitary (as well as other sellar masses such as craniopharyngiomas and meningiomas) usually take up
gadolinium to a lesser degree than the normal pituitary but more than the CNS. Therefore, the degree of gadolinium
enhancement does not distinguish one kind of sellar mass from another. The postcontrast enhancement of
meningiomas is usually homogeneous. If a sellar lesion can be seen as separate from the normal pituitary, whether
on unenhanced or, more commonly, enhanced images, the lesion is not a pituitary adenoma (image 1).
Among patients with moderate to advanced renal failure (dialysis-dependent or estimated GFR less than 30
mL/min), the administration of gadolinium has been associated with the potentially severe syndrome of nephrogenic
systemic fibrosis. In such patients, gadolinium-based imaging should be avoided if possible. This issue, as well as
the role of hemodialysis after the procedure if gadolinium-based imaging must be performed, is discussed
separately. (See "Nephrogenic systemic fibrosis/nephrogenic fibrosing dermopathy in advanced renal failure",
section on 'If gadolinium must be given'.)
CT scan — Calcification in a craniopharyngioma or meningioma is seen better by CT scan than by MRI (image
4). (See "Craniopharyngioma".)
Hormonal evaluation — Hypothalamic-pituitary hormonal function should be evaluated whenever a sellar mass is
encountered.
Hormonal hypersecretion — Hypersecretion, with the exception noted below, is caused only by pituitary
adenomas. As a result, the demonstration of hormonal hypersecretion identifies both the sellar mass as a pituitary
adenoma and the kind of adenoma:
Thyrotroph adenomas are characterized by a clinically hyperthyroid patient who has a diffuse goiter and elevations
in serum FT4 and T3, but an inappropriately normal or elevated serum TSH level.
Hormonal hyposecretion — Hormonal hyposecretion can be caused by any hypothalamic or pituitary lesion
and therefore usually has no value in the differential diagnosis of a sellar mass. One exception to this statement is
A serum prolactin concentration >200 ng/mL generally identifies a lactotroph adenoma; values that are
between 20 and 200 ng/mL could be due to a lactotroph adenoma or to any other sellar mass.
●
The best single test for the diagnosis of acromegaly is measurement of serum insulin-like growth factor
(IGF)-1. Among patients with equivocal values, serum growth hormone levels can be measured after an oral
glucose load. (See "Diagnosis of acromegaly".)
●
Elevated 24-hour urine cortisol excretion associated with a high-normal or high ACTH concentration usually
indicates a corticotroph adenoma. (See "Establishing the diagnosis of Cushing's syndrome" and "Establishing
the cause of Cushing's syndrome".)
●
Gonadotroph adenomas can be identified by characteristic patterns of basal and TRH-stimulated
concentrations of gonadotropins and their subunits; these patterns differ somewhat in men and women. (See
"Clinical manifestations and diagnosis of gonadotroph and other clinically nonfunctioning pituitary adenomas".)
TRH is not currently available in the United States but is still available in many other countries.
●
11/27/2014 Causes, presentation, and evaluation of sellar masses
http://www.uptodate.com/contents/causes-presentation-and-evaluation-of-sellar-masses?topicKey=ENDO%2F6632&elapsedTimeMs=4&view=print&displayedV… 6/15
that the spontaneous development of central diabetes insipidus indicates that the lesion affects the hypothalamus
or the stalk and is therefore not a pituitary lesion. (See "Clinical manifestations and causes of central diabetes
insipidus".)
Although not generally useful in the differential diagnosis of a sellar mass, the possibility of hormonal hyposecretion
should be evaluated in all patients who have a sellar mass in order to identify and replace hormone deficiencies.
(See "Diagnosis of hypopituitarism".)
Pituitary incidentaloma — The extent of the evaluation in a patient with an incidentally discovered intrasellar MRI
signal abnormality depends upon its size. If it is larger than 10 mm, it should be evaluated as described above. If
the mass is smaller than 10 mm, especially much smaller, and the patient has no clinical findings of pituitary
dysfunction, we usually measure only the serum prolactin concentration which, in one report, was much more cost-
effective than either measurement of multiple hormones or performance of follow-up MRIs at 6 and 12 months [37].
One exception may be the patient who is quite anxious about the presence of a small pituitary tumor. No evaluation
for hormonal hyposecretion or visual abnormalities is necessary. (See "Incidentally discovered sellar masses
(pituitary incidentalomas)".)
INFORMATION FOR PATIENTS — UpToDate offers two types of patient education materials, “The Basics” and
“Beyond the Basics.” The Basics patient education pieces are written in plain language, at the 5 to 6 grade
reading level, and they answer the four or five key questions a patient might have about a given condition. These
articles are best for patients who want a general overview and who prefer short, easy-to-read materials. Beyond the
Basics patient education pieces are longer, more sophisticated, and more detailed. These articles are written at the
10 to 12 grade reading level and are best for patients who want in-depth information and are comfortable with
some medical jargon.
Here are the patient education articles that are relevant to this topic. We encourage you to print or e-mail these
topics to your patients. (You can also locate patient education articles on a variety of subjects by searching on
“patient info” and the keyword(s) of interest.)
SUMMARY AND RECOMMENDATIONS
Causes and presentation — Sellar masses usually present with neurologic symptoms, hormonal abnormalities,
or as an incidental finding on MRI. Pituitary adenomas are the most common cause of sellar masses, but other
causes include:
th th
th th
Basics topics (see "Patient information: Prolactinoma (The Basics)" and "Patient information: Pituitary
adenoma (The Basics)")
●
Beyond the Basics topics (see "Patient information: High prolactin levels and prolactinomas (Beyond the
Basics)" and "Patient information: Acromegaly (Beyond the Basics)" and "Patient information: Meningioma
(Beyond the Basics)")
●
Physiologic enlargement of the pituitary, most commonly during pregnancy but also in primary
hypothyroidism and primary hypogonadism. (See "Causes of hyperprolactinemia".)
●
Other benign tumors, such as craniopharyngioma and meningioma. (See "Craniopharyngioma" and
"Meningioma: Clinical presentation and diagnosis".)
●
Malignant tumors, both primary (germ cell tumor, chordoma, primary CNS lymphoma), and metastatic (most
commonly from breast and lung cancer). (See "Intracranial germ cell tumors" and "Chordoma and
chondrosarcoma of the skull base", section on 'Chordoma' and "Clinical presentation, pathologic features, and
diagnosis of primary central nervous system lymphoma".)
●
Sellar masses may also be due to a cyst, abscess, or arteriovenous fistula of the cavernous sinus. (See
'Cysts' above and 'Abscess' above and 'Arteriovenous fistula of the cavernous sinus' above.)
●
11/27/2014 Causes, presentation, and evaluation of sellar masses
http://www.uptodate.com/contents/causes-presentation-and-evaluation-of-sellar-masses?topicKey=ENDO%2F6632&elapsedTimeMs=4&view=print&displayedV… 7/15
Evaluation
Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
1. Gsponer J, De Tribolet N, Déruaz JP, et al. Diagnosis, treatment, and outcome of pituitary tumors and otherabnormal intrasellar masses. Retrospective analysis of 353 patients. Medicine (Baltimore) 1999; 78:236.
2. Freda PU, Post KD. Differential diagnosis of sellar masses. Endocrinol Metab Clin North Am 1999; 28:81.
3. Saeger W, Lüdecke DK, Buchfelder M, et al. Pathohistological classification of pituitary tumors: 10 years ofexperience with the German Pituitary Tumor Registry. Eur J Endocrinol 2007; 156:203.
4. Alexander JM, Biller BM, Bikkal H, et al. Clinically nonfunctioning pituitary tumors are monoclonal in origin. JClin Invest 1990; 86:336.
5. Herman V, Fagin J, Gonsky R, et al. Clonal origin of pituitary adenomas. J Clin Endocrinol Metab 1990;71:1427.
6. Raappana A, Koivukangas J, Ebeling T, Pirilä T. Incidence of pituitary adenomas in Northern Finland in 1992-2007. J Clin Endocrinol Metab 2010; 95:4268.
7. Fernandez A, Karavitaki N, Wass JA. Prevalence of pituitary adenomas: a community-based, cross-sectionalstudy in Banbury (Oxfordshire, UK). Clin Endocrinol (Oxf) 2010; 72:377.
8. Bassett JH, Forbes SA, Pannett AA, et al. Characterization of mutations in patients with multiple endocrineneoplasia type 1. Am J Hum Genet 1998; 62:232.
9. Crabtree JS, Scacheri PC, Ward JM, et al. A mouse model of multiple endocrine neoplasia, type 1, developsmultiple endocrine tumors. Proc Natl Acad Sci U S A 2001; 98:1118.
10. Landis CA, Masters SB, Spada A, et al. GTPase inhibiting mutations activate the alpha chain of Gs andstimulate adenylyl cyclase in human pituitary tumours. Nature 1989; 340:692.
11. Vallar L, Spada A, Giannattasio G. Altered Gs and adenylate cyclase activity in human GH-secreting
Hypophysitis, especially lymphocytic (lymphocytic infiltration of the pituitary), occurs most commonly in
postpartum women, but can also be seen in women at other times, and rarely in men, but increasingly due to
anti-CTLA-4 treatment of malignancies. (See 'Hypophysitis' above and "Causes of hypopituitarism".)
●
We recommend magnetic resonance imaging (MRI) as the single best, and usually only, imaging procedure
for most sellar masses. Certain MRI findings suggest a greater likelihood of some kinds of sellar masses than
others. As an example, finding a mass that is separate from the pituitary gland generally indicates that the
mass is not a pituitary adenoma.
●
We recommend evaluation of hypothalamic-pituitary hormonal function whenever a sellar mass is
encountered. Hormonal hypersecretion is caused only by pituitary adenomas. Consequently, the
demonstration of hormonal hypersecretion identifies the sellar mass as a pituitary adenoma and also identifies
the type of adenoma. (See 'Hormonal evaluation' above.)
●
The extent of the evaluation in a patient with an incidentally discovered intrasellar MRI signal abnormality
(pituitary incidentaloma) depends upon its size. If it is larger than 10 mm, we recommend the hormonal
evaluation as described above. (See 'Hormonal evaluation' above.) If it is smaller than 10 mm and the patient
has no clinical findings of pituitary dysfunction, we recommend measuring only the serum prolactin
concentration. (See "Incidentally discovered sellar masses (pituitary incidentalomas)".)
●
Hormonal hyposecretion may be caused by any hypothalamic or pituitary lesion and therefore usually has no
value in the differential diagnosis of a sellar mass. One exception to this statement is that the spontaneous
development of central diabetes insipidus indicates that the lesion affects the hypothalamus or the stalk and
is therefore not a pituitary lesion. (See "Clinical manifestations and causes of central diabetes insipidus".)
●
11/27/2014 Causes, presentation, and evaluation of sellar masses
http://www.uptodate.com/contents/causes-presentation-and-evaluation-of-sellar-masses?topicKey=ENDO%2F6632&elapsedTimeMs=4&view=print&displayedV… 8/15
pituitary adenomas. Nature 1987; 330:566.
12. Zhang X, Horwitz GA, Heaney AP, et al. Pituitary tumor transforming gene (PTTG) expression in pituitaryadenomas. J Clin Endocrinol Metab 1999; 84:761.
13. Vlotides G, Eigler T, Melmed S. Pituitary tumor-transforming gene: physiology and implications fortumorigenesis. Endocr Rev 2007; 28:165.
14. Ezzat S, Zheng L, Zhu XF, et al. Targeted expression of a human pituitary tumor-derived isoform of FGFreceptor-4 recapitulates pituitary tumorigenesis. J Clin Invest 2002; 109:69.
15. Snyder PJ. Gonadotroph adenomas. In: Endocrinology, DeGroot LJ (Ed), WB Saunders, Philadelphia 2001.
16. Bassetti M, Spada A, Arosio M, et al. Morphological studies on mixed growth hormone (GH)- and prolactin(PRL)-secreting human pituitary adenomas. Coexistence of GH and PRL in the same secretory granule. JClin Endocrinol Metab 1986; 62:1093.
17. Shimono T, Hatabu H, Kasagi K, et al. Rapid progression of pituitary hyperplasia in humans with primaryhypothyroidism: demonstration with MR imaging. Radiology 1999; 213:383.
18. Alkhani AM, Cusimano M, Kovacs K, et al. Cytology of pituitary thyrotroph hyperplasia in protracted primaryhypothyroidism. Pituitary 1999; 1:291.
19. Groff TR, Shulkin BL, Utiger RD, Talbert LM. Amenorrhea-galactorrhea, hyperprolactinemia, and suprasellarpituitary enlargement as presenting features of primary hypothyroidism. Obstet Gynecol 1984; 63:86S.
20. Samaan NA, Stepanas AV, Danziger J, Trujillo J. Reactive pituitary abnormalities in patients with Klinefelter'sand Turner's syndromes. Arch Intern Med 1979; 139:198.
21. Scheithauer BW, Moschopulos M, Kovacs K, et al. The pituitary in klinefelter syndrome. Endocr Pathol 2005;16:133.
22. Ezzat S, Asa SL, Stefaneanu L, et al. Somatotroph hyperplasia without pituitary adenoma associated with along standing growth hormone-releasing hormone-producing bronchial carcinoid. J Clin Endocrinol Metab1994; 78:555.
23. Ragel BT, Couldwell WT. Pituitary carcinoma: a review of the literature. Neurosurg Focus 2004; 16:E7.
24. Giustina A, Gola M, Doga M, Rosei EA. Clinical review 136: Primary lymphoma of the pituitary: an emergingclinical entity. J Clin Endocrinol Metab 2001; 86:4567.
25. Fassett DR, Couldwell WT. Metastases to the pituitary gland. Neurosurg Focus 2004; 16:E8.
26. Schubiger O, Haller D. Metastases to the pituitary--hypothalamic axis. An MR study of 7 symptomaticpatients. Neuroradiology 1992; 34:131.
27. Morita A, Meyer FB, Laws ER Jr. Symptomatic pituitary metastases. J Neurosurg 1998; 89:69.
28. Vates GE, Berger MS, Wilson CB. Diagnosis and management of pituitary abscess: a review of twenty-fourcases. J Neurosurg 2001; 95:233.
29. Sato N, Putman CM, Chaloupka JC, et al. Pituitary gland enlargement secondary to dural arteriovenousfistula in the cavernous sinus: appearance at MR imaging. Radiology 1997; 203:263.
30. Thodou E, Asa SL, Kontogeorgos G, et al. Clinical case seminar: lymphocytic hypophysitis:clinicopathological findings. J Clin Endocrinol Metab 1995; 80:2302.
31. Dillard T, Yedinak CG, Alumkal J, Fleseriu M. Anti-CTLA-4 antibody therapy associated autoimmunehypophysitis: serious immune related adverse events across a spectrum of cancer subtypes. Pituitary 2010;13:29.
32. Yang JC, Hughes M, Kammula U, et al. Ipilimumab (anti-CTLA4 antibody) causes regression of metastaticrenal cell cancer associated with enteritis and hypophysitis. J Immunother 2007; 30:825.
33. Ribas A, Comin-Anduix B, Chmielowski B, et al. Dendritic cell vaccination combined with CTLA4 blockade inpatients with metastatic melanoma. Clin Cancer Res 2009; 15:6267.
34. Snyder PJ. Gonadotroph adenomas. In: The Pituitary, 2nd, Melmed S (Ed), Blackwell Science Inc., Malden,MA 2002. p.575.
35. Pressman BD. Pituitary imaging. In: The Pituitary, 2nd, Melmed S (Ed), Blackwell Science Inc., Malden, MA2002. p.663.

11/27/2014 Causes, presentation, and evaluation of sellar masses
http://www.uptodate.com/contents/causes-presentation-and-evaluation-of-sellar-masses?topicKey=ENDO%2F6632&elapsedTimeMs=4&view=print&displayedV… 9/15
36. Taylor SL, Barakos JA, Harsh GR 4th, Wilson CB. Magnetic resonance imaging of tuberculum sellaemeningiomas: preventing preoperative misdiagnosis as pituitary macroadenoma. Neurosurgery 1992; 31:621.
37. King JT Jr, Justice AC, Aron DC. Management of incidental pituitary microadenomas: a cost-effectivenessanalysis. J Clin Endocrinol Metab 1997; 82:3625.
Topic 6632 Version 8.0
11/27/2014 Causes, presentation, and evaluation of sellar masses
http://www.uptodate.com/contents/causes-presentation-and-evaluation-of-sellar-masses?topicKey=ENDO%2F6632&elapsedTimeMs=4&view=print&displayed… 10/15
GRAPHICS
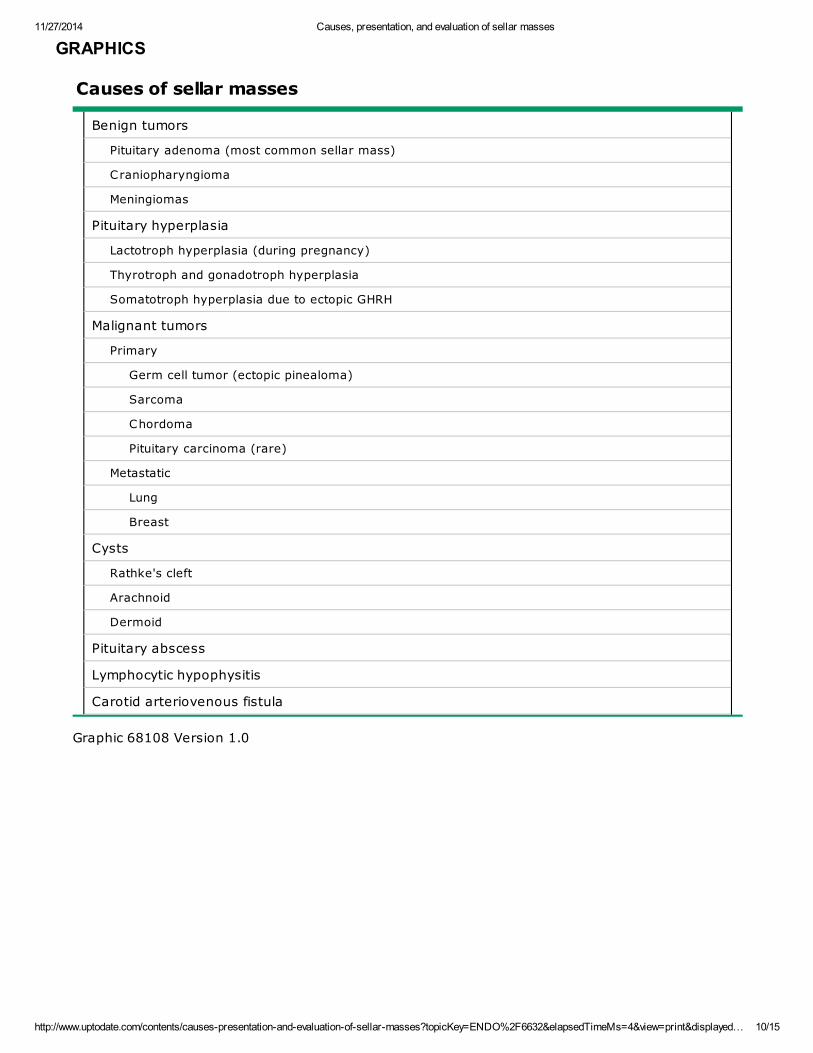
Causes of sellar masses
Benign tumors
Pituitary adenoma (most common sellar mass)
Craniopharyngioma
Meningiomas
Pituitary hyperplasia
Lactotroph hyperplasia (during pregnancy)
Thyrotroph and gonadotroph hyperplasia
Somatotroph hyperplasia due to ectopic GHRH
Malignant tumors
Primary
Germ cell tumor (ectopic pinealoma)
Sarcoma
Chordoma
Pituitary carcinoma (rare)
Metastatic
Lung
Breast
Cysts
Rathke's cleft
Arachnoid
Dermoid
Pituitary abscess
Lymphocytic hypophysitis
Carotid arteriovenous fistula
Graphic 68108 Version 1.0

11/27/2014 Causes, presentation, and evaluation of sellar masses
http://www.uptodate.com/contents/causes-presentation-and-evaluation-of-sellar-masses?topicKey=ENDO%2F6632&elapsedTimeMs=4&view=print&displayed… 11/15
Sellar mass
MRI shows enhancement of only the rim of a suprasellar mass (M) and
of the normal pituitary inferior to it following the administration of
gadolinium. The clear distinction between the mass and the normal
pituitary indicates that the mass is not a pituitary adenoma. The mass
was found on surgery to be a craniopharyngioma.
Courtesy of Peter J Snyder, MD.
Graphic 56435 Version 2.0

11/27/2014 Causes, presentation, and evaluation of sellar masses
http://www.uptodate.com/contents/causes-presentation-and-evaluation-of-sellar-masses?topicKey=ENDO%2F6632&elapsedTimeMs=4&view=print&displayed… 12/15
Sellar masses
The unenhanced MRI on the left shows in sagittal view a clinically
nonfunctioning pituitary adenoma that is extending just above the sella
(arrow). The unenhanced MRI on the right shows a sellar mass of similar
size (arrow), which is interpreted radiologically as a pituitary adenoma,
but pathologically was found to be lymphocytic hypophysitis.
Courtesy of Peter J Snyder, MD.
Graphic 63618 Version 2.0

11/27/2014 Causes, presentation, and evaluation of sellar masses
http://www.uptodate.com/contents/causes-presentation-and-evaluation-of-sellar-masses?topicKey=ENDO%2F6632&elapsedTimeMs=4&view=print&displayed… 13/15
Sellar mass
The MRI on the left shows in sagittal view a very large pituitary
adenoma elevating the optic chiasm (arrow). The MRI on the right
shows a sellar mass of similar size, which has a much brighter signal
than the mass on the left (arrow). The reason for the brighter signal
could have been hemorrhage into a pituitary adenoma, but in this
case was found surgically to be fluid in a craniopharyngioma.
Courtesy of Peter J Snyder, MD.
Graphic 76412 Version 2.0
11/27/2014 Causes, presentation, and evaluation of sellar masses
http://www.uptodate.com/contents/causes-presentation-and-evaluation-of-sellar-masses?topicKey=ENDO%2F6632&elapsedTimeMs=4&view=print&displayed… 14/15
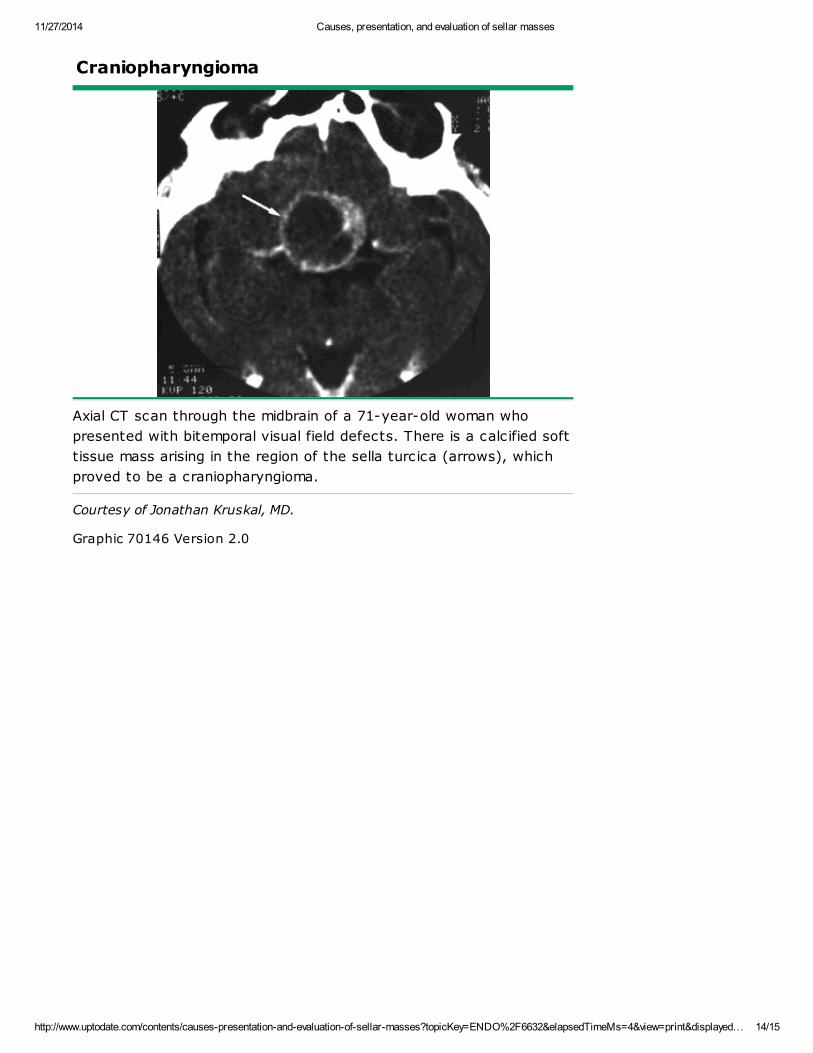
Craniopharyngioma
Axial CT scan through the midbrain of a 71-year-old woman who
presented with bitemporal visual field defects. There is a calcified soft
tissue mass arising in the region of the sella turcica (arrows), which
proved to be a craniopharyngioma.
Courtesy of Jonathan Kruskal, MD.
Graphic 70146 Version 2.0

11/27/2014 Causes, presentation, and evaluation of sellar masses
http://www.uptodate.com/contents/causes-presentation-and-evaluation-of-sellar-masses?topicKey=ENDO%2F6632&elapsedTimeMs=4&view=print&displayed… 15/15
Disclosures: Peter J Snyder, MD Grant/Research/Clinical Trial Support: AbbVie [Testosterone (Testosterone gel)]; Novartis [Cushing'ssyndrome, acromegaly (Pasireotide, octreotide)]; Cortendo [Cushing's syndrome (COR203)]; Novo Nordisk [Grow th hormone (Grow thhormone)]; Ipsen [Acromegaly (Lanreotide)]. Consultant/Advisory Boards: Novartis [Cushing's syndrome (Pasireotide)]; Novo Nordisk[Grow th hormone (Grow th hormone)]; Pfizer [Acromegaly (Pegvisomant)]. David S Cooper, MD Nothing to disclose. Kathryn A Martin,MD Employee of UpToDate, Inc.
Contributor disclosures are review ed for conflicts of interest by the editorial group. When found, these are addressed by vetting througha multi-level review process, and through requirements for references to be provided to support the content. Appropriately referencedcontent is required of all authors and must conform to UpToDate standards of evidence.
Conflict of interest policy
Disclosures