Embed Size (px)
Citation preview

Causes,implicationsandpossibleresponsestotheimplementationofstaffingmoratoriainthepublichealthsysteminSouthAfricaduringtimesofbudget
austerity
July2016

2
CONTENTS
Summaryandrecommendations............................................................................................3
1.Introduction................................................................................................................................6
2.Thebudgetaryoriginsofthecurrentcrisis...................................................................8
3.MTBPS2015andBudget2016/17:adeepeningHRcrisis..................................104.Impactofpoorlymanagedstaffingmoratoria............................................................11
5.Advancingtherighttohaveaccesstohealthcareintimesofausterity.........13
6.Thelegalframework:obligationsandtoolsfordecision-making.....................13
7.Possiblecoursesofactionindealingwithfrozenposts:threescenarios......14
7.1Continueoncurrentpathofausterity:wearetrainingforoverseascareersandtheprivatesector...........................................................................................147.2Findthemoney:allocatingadditionalresourcestofillposts......................177.3Doingthingsdifferently:maximisingbenefits....................................................18

3
SummaryandrecommendationsThepurposeof thisworkingpaper is todrawattention to the causes, consequencesandpossible responses to the implementation ofmoratoria on the filling of postswithin thehealth system.Human resourcemoratoria, also referred to as the ‘freezing of posts’ hasbecomeanincreasinglycommonoccurrencewithinthepublichealthsystemoverthelasttwoyears.Even though there are several contributing factors that result in the implementation ofmoratoriaonthe fillingofposts,evidencesuggests that thecause isprimarilybudgetary.While provincial health expenditure has more than doubled in real terms over the lastdecade, slow economic growth has meant that government revenue is becomingincreasingly constrained. Health budgets are increasingly unable to keep pacewith costincreasesthatcontinuetooutstripinflation.SubstantialrealincreasestotheCompensationofEmployees(CoE)budgetitemhasoftenbeen cited as the primary culprit for costs in the health system outpacing budgetaryincreases.While this is true tosomeextent,poorplanninghasmeant that littlehasbeendonetopreparethehealthsystemfortheimplementationofausteritymeasures.Provincial departments have managed budgetary pressures by shifting money betweenbudgetitemsandoverspendingonCoEinthehopethattheywillreceiveadditionalfundinginfuturetoaccountforoverspending.Intheabsenceof‘bailouts’fromtheTreasury,thisoverspendinghascontributedtogrowingaccrualsandagrowingbudgetdeficitthatmustbe recovered from future budgets without necessary adjustments being made for thisexpenditure.Inrecentyearsandinanefforttocontroloverspendingprovincialdepartmentsofhealthand treasuries have started implementing staffingmoratoria. This has either been doneofficially(includingmemosandinstructionsonthefillingofposts)orunofficiallythroughrepeateddelaysinmakingappointments.Areadingofthe2015MTBPSrevealsthatthesituationisboundtobecomefarworseoverthe2016/17-2018/19MTEF.Again, while health budgets increase beyond inflation they areinsufficient tomeet growing cost pressures due to higher than inflationary increases tosalariesandgoodsandservicescosts.1
Inthisworkingpaperwedrawattentiontohowausteritymeasures,astheyarecurrentlybeingimplemented,arehavingcatastrophicconsequencesforhealthcare,particularlyforruralhealthsettings.Theseconsequencesincludediminishedcapacitytodeliverservices;poor supervision of existing staff; weakened support processes (e.g. procurement);additionalstrainbeingputonalreadyoverburdenedstaff;andconsequently,overburdenedstaffleavingthepublicservicedeepeningthecrisis.
1CostsofprovidinghealthservicesoftenincreasebeyondConsumerPriceInflationbecausethecostofmedicines,medicalsuppliesandothermedicalservicesincreasebeyondinflationeachyear.Between2008and2011,forexample,inflationonmedicalproductswasatleast2percentagepointshigherthanCPIinflationsee:http://econex.co.za/wp-content/uploads/2015/03/econex_researchnote_36.pdf

4
Wearguethatablanketapproachtotheimplementationofmoratoriaonthefillingofpostsis a significant threat to the right to have access to health care as provided for in theConstitution and that such an approach acts contrary to the principles of administrativejustice.We then present three scenarios that outline different approaches to managing budgetausterityandtheirpossibleoutcomes.Thefirstscenariowediscussisthe‘continueonthecurrentpathofausterity’approach,whichinvolvestheblanketfreezingofpostsasacostsavingmeasure.Thesecondscenariowepresentisthe‘findingthemoney’scenariowhereadditional budget is allocated to account for cost increases. Finally, we present thescenario:“realitycheck:maximisingscarceresourcestogreatestimpact”.Since this working paper there has been some movement on the implementation of astrategyaimedatbalancingtheneedforcostcontainmentinCoEandtheneedtoensurethat the impact of austeritymeasures on frontline service delivery is minimised. In the206/17budget theTreasurynotesthatwhilegovernmentdepartmentsarebusyrevisinghuman resourceplans to includeausteritymeasures, all non-criticalpostswill be frozenwith the exception of front-line posts including teachers, nurses, doctors, police officersandothercriticalposts.While this is an important step,webelieve that doesnot go far enough in clarifying thescopeofwhatiscriticalandmayinfactlackthenuancenecessarytoaccountforpoststhatarenot‘front-line’butarenonethelesscritical.Inarecentroundtable(1April2016)withthe National Department of Health, the Treasury and rural health partners we revisedguidelinesdevelopedbytheRHAPandotherruralhealthstakeholdersinNovember2015,which sets out and approach to identifying critical posts that extends beyond frontline-posts.Theserevisedguidelinesare:
1) The National Department of Health in collaboration with the Treasuryshouldprovideguidance throughpolicyonhowprovincesareexpected toprotectcriticalpostsattimesofausterity.Thisshouldinclude:
• Inputbyhealthandpartners,inparticulararounddefinitionofcritical.• Principles of transparency and consultation, which should include
transparency on savings in managerial/admin positions versus frontlinehealth professionals, and an escalation procedure in the event thatprovincesdonotimplementtheguidelines
• Anationalplanregardingcommunicationanddistributiontoprovincesaswelltimeframesforthereleaseoftheguidelines
• Some standardization in implementation: what is required from people;whoisresponsibleforwhat.
2) Adequate consideration should be given to inhospitable and underserved
areas so as to ensure disadvantaged communities are not furthermarginalisedintheiraccesstohealthcare.Thisincludesbutisnotlimitedtoruralhealthcontextsfortheiruniquecharacteristicsandchallenges.

5
3) It is national policy to use normative guides “WISN” where available(currentlyforclinicsandCHCs)toidentifytheminimumpoststobefilled.
• Whiledoingso,facilitiesmustensuretoadequatedata,whichisnotlimited
toheadcountandotherutilizationdata.Populationdatamustbeused toinclude unmet need, as alluded to in section 6 of the WISN normativeguidelines. In the event that current staffing levels are less than theminimum“WISN”norms,additionalstaffing is tobeadvocated forby thefacility.Intheeventthatnofundingisavailableforsuchadditionalstaffing,the facility needs to identify the critical healthposts to beprioritized, asguidedbythenationalguidelines
4) Critical posts need to be defined locally and these can include healthprofessionals and support staff. The purpose is not to define whichcategoriesofstaffaretobeconsideredcritical.InsteadtheconsequencesonpatientcareshouldbethedeterminingfactorondecidingwhetherpostAinfacility B is critical under the given circumstances. Here critical posts aresimplydefinedasthosethatpotentiallyhavecatastrophicconsequencesforservicedeliveryiftheyremainunfilled.
Herekeyunderlyingprinciplesindefiningcriticalinclude:• Theprotectionoffrontlinehealthprofessionals• Theprotectionofservicestothepoorandthemarginalised-whohavethe
leastoptionofservices• Provincially:themoreruralthemoreprotection• Districtlevel:themoreruraldistrictsthemoreprotection
5) DistrictsareexpectedtodevelopcostedHRplansbutthisdoesnothappen;
if suchplansare inplace it canhelpDistrictManagers to identifypriorityposts at times of staffing moratoria. The National and ProvincialDepartments of Health must ensure Districts have such plans in place.TreasuryshouldprovidesupportinthecostingoftheHRplans.
6) Decision–making on cost-saving and cost-cutting must be made at the
district level by giving districts the amount to be saved and allowing thedistricttodecide.
• Thesedecisionsmustbesupportedbyguidelinesondefiningcriticalposts
andmustbe informedby thePromotionofAdministrative Justice (PAJA)principles of evidence-based decision-making, rationality andproportionality togiveeffect to the constitutionaldutyofGovernment toprogressivelyrealisetherighttohealth.
7) Corruptionandunauthorizedexpenditureshouldbeperformancemanaged
instead of punishing all managers and districts by withdrawing theirdelegationsofauthoritiesforthetransgressionsofothers.Thiswouldmean

6
thatprovincialdepartmentsandinstitutionsshouldbeheldaccountableforperformancemanagement.
8) In the event of a Section100 intervention orwhenTreasury co-manages a
Health Department, there should be an up-front agreement around theprioritizationofhealthneedsandclearprocessesforappointmentstooccur.
• In thisevenstrategiesmustbeput inplace toreducethetime it takes tomake appointments when there is co-management/S100 intervention toovercometimecostsofaddedlayersofdecision-making.
• Process’needtobepredictable,aspeoplegetfrustrated,startinterveningetc.
1.IntroductionThe Rural Health Advocacy Project was established in 2009 as apartnership initiativebetween theRuralDoctorsAssociationofSouthernAfrica (RuDASA), theWitsCentre forRuralHealth(WCRH)andSECTION27.Ourworkrevolvesaroundtheconstitutionalrightofruralandremotecommunities tohaveequitableaccess tocomprehensive,qualityhealthcare.Informedbythevoicesofruralhealthcareworkersandcommunitiesontheground,the RHAP aims to facilitate self-advocacy, generate debate, monitor implementation ofhealthpoliciesinruralareas,supportpro-equitygovernmentinterventions,andinfluencedecision-makingthatisintunewithlocalruralrealities2.Ourinterestintheresourcingofthehealthsystememergesoutofthefactthatinresource-constrainedenvironmentsitiscriticalthatavailableresourcesareallocatedequitablyandusedefficientlyandeffectivelytoachievethegreatestpossible impact.There isanaddedfinancialcosttoprovidethesamequalityservicetoremotecommunitiesandthismustbeincorporated in thepolicy,planningand,most importantly,budgetingprocess. In reality,this added cost factor is often not considered, leading to inequitable financing andultimately inequitableaccess to care for rural communities.At the same time therehavebeenweaknessesinhowresourcesarebeingused:overspending,underspending,andthemismanagementoffundscontinuestocompromisecareinmanyruralsettings.Ourworkonhealthcarefinancingcoversabroadscopeofissuesrelatingtotheequitable,efficientandeffectivedistributionanduseofresources forruralhealth.Forthisworkingpaper,however,ourfocuswillbenarrowedtothepotentialimpactcurrentbudgetpolicydecisionswillhaveontherecruitment,retentionanddistributionofhumanresourcesforhealth,withaparticularfocusontheseissueswithinaruralcontext.The availability of human resources for health is a particularly vexing issue in ruralcontexts inSouthAfricaand isa secondcore focusof theRHAP’swork.Generally, SouthAfrica, as many countries worldwide, is faced with a severe crisis in terms of humanresources forhealth. Inequitiesexist in thedistributionofhumanresourcesbetween theprivate and public sectors aswell as between rural and urban areas. About 60% of thenurses and 40%of the doctors serve the 85%of the population using the public healthsector.Vacancyratesaretheworstinruralprovinces,andthethreemostruralprovinces
2FormoreinformationontheworkoftheRHAPvisitwww.rhap.org.za

7
have the country’s lowest doctor-to-patient ratios3. Inequities also exist within ruralprovincesanddistricts,withwidevariationsinstaffinglevelsbetweenfacilitiesleadingtoinefficientuseofscarcehealthcareworkers.Inthisworkingdocumentwedrawattentiontoaparticularlytroublingtrenddevelopingwithinmost provincial departments of health, which if notmanaged properly will havecatastrophicconsequencesforthecountry’smostvulnerablepopulations.Overthelasttwofinancialyearswehavebecomeincreasinglyawareoftheimplementationofmoratoriaonthehiringofstafftofillvacantposts.
1. In some instances these have been official moratoria where circulars andmemoshavebeendistributedtomanagerswithinthedepartmentindicatingatotalblockonthefillingofvacantpostsorstrictcontrolsonwherepostsarefilled(i.e.postsareonlyfilledinexceptionalcircumstances).Currently,weareaware of official moratoria being implemented in the North West4, EasternCape5,KwaZulu-Natal6,MpumalangaandFreeStateprovinces.
2. Inotherinstancesmoratoriaarebeingimplementedindirectlyorbystealth.In
theseinstances,postsaresimplynotfilled(evenwheretherearecandidates)withoutanyclear indicationofwhyappointmentsarenotbeingmade.Thesepostsareeitherleftfrozen(i.e.theyarePERSALbutcannotbefilled)foralongperiodoftimeorareeventuallyabolishedfromPERSALalltogether.
Whiletherearemanycontributingfactorstothe implementationofstaffingmoratoriaorthefreezingofposts,itisourcontentionthattheprimarycausesarebudgetary.Inthisworkingdocumentwe:
1. Briefly outline the systemic causes of budgetary pressures that have lead totheimplementationofmoratoria;
2. Howthecurrentbudgetdocumentationindicatesthatthesituationislikelytobecomemoresevereoverthenextthreeyears;
3. Give a brief discussion of the consequences of blanketmoratoria on humanresourcesforhealth,particularlyinruralcontexts;
4. Presentthreedifferentscenariosforapproachingstaffingmoratoria;and5. Offerafewrecommendationsforactionsthatcouldbetakentomitigatesome
ofthemostsevereconsequencesofsuchmoratoria.
3Statsonthestateofruralhealth,andhealthcaremoregenerally,inSouthAfricaareavailableintheRHAP’sRuralHealthFactSheet2015availableathttp://www.rhap.org.za/wp-content/uploads/2015/09/RHAP-Rural-Health-Fact-Sheet-2015-web.pdf4AcopyoftheNWDoHcircularonfrozenpostsfor2014/15isavailableherehttp://www.rhap.org.za/wp-content/uploads/2015/10/Memo-by-NW-Provincial-Government_Staffing-Moratoria_September-2015.pdf5AcopyoftheNWDoHcircularonfrozenpostsfor2014/15isavailableherehttp://www.rhap.org.za/wp-content/uploads/2015/10/ECDoH-Circular-Staffing-Moratoria_frozen-posts_-September-2015.docx6AcopyoftheKZNDoHcircularonfrozenpostsfor2014/15isavailableherehttp://www.rhap.org.za/kzn-circular-october-2015-motatorium-in-filling-of-posts/

8
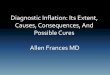
2.ThebudgetaryoriginsofthecurrentcrisisOver the last 15 years expenditure on health care has increased phenomenally. Since2001/02 provincial health expenditure has more than doubled in real terms fromapproximately R60 billion to more than R140 billion in 2014/15 (see Graph 1)7. Thisdramaticincreaseinexpenditurehasbeendrivenprimarilybyincreasedinvestmentintheresponse to HIV and AIDS and higher than inflationary increases in the cost ofCompensationofEmployees(CoE).Between2005/06and2014/15expenditureonCoEat theprovincial levelhas increasedby on average 8% in real terms year-on-year. Over the same period there have beenaveragerealincreasestogoodsandservicesandcapitalassetsof5%and2%inrealtermsrespectively(Graph1)8.Figure1:Graph1:ProvincialHealthExpenditure2001/02-2014/15(constantprocess2014/15)
CoEasaproportionofprovincialhealthexpenditurehasincreasedfrom54%in2005/06to64%in2014/15.Overthesameperiodtheproportionofprovincialhealthexpendituregoing togoodsandserviceshasdeclined from32%to28%whileexpenditureoncapitalassetshasdeclinedfrom8%to5%9.Increases in CoE have not, however, been driven primarily by an increase in theemploymentofhealthcareworkers.Therearetwoprimaryfactorsthathavecontributedtothedramaticincrease:
7NationalTreasury(2015).ProvincialGovernmentsExpenditureReview2011/12-2015/16:Health.Available:http://www.treasury.gov.za/publications/igfr/2015/prov/04.%20Chapter%204%20-%20Health.pdf8NationalTreasury(2009).ProvincialGovernmentsExpenditureReview2005/06-2011/12:Health.Available:http://www.treasury.gov.za/publications/igfr/2009/prov/04.%20Chapter%204%20-%20Health.pdf9Ibid

9
1. Wagesinthepublicsectorhavecontinuedtoincreasebeyondinflationeachyear.2. Therehasbeenanincreaseinthenumberofadministrativeandmanagementposts.
This was clearly articulated in the consolidated Integrated Support team Reports,commissionedby formerMinisterofHealthBarbaraHogan, in2009.The IST foundthat:
“Of serious concern is the considerable and continued growth in management andadministrative positions across the various provinces, especially in provincial head offices,relativetothegrowthinhealthcareprofessionalpositions”10Thetrendinthegrowthofpublicsectoradministrationattheexpenseofservicedeliverycadreshasonethathasbeenslowinggradually.The2015MTBPS11providesthefollowingfindingsfromarecentreviewonpublicsectoremploymentundertakenbyTreasury:“InMarch2015,nationalgovernmentdepartmentsemployed402748staff,downfrom404496 inMarch2012.This trendhasbeenoffsetby theexpansionofmanagerialpersonnel inadministrative and policy departments in central government. A recent national treasuryreviewshowedthat,across13departmentsanalysed,1158postswereaddedinthelastfiveyears.”(p.30)Attheprovinciallevelthetrenddoesappeartobereversingbutnotsufficientlytocountertheinflationarypressuresduetosalaryincreases:“Provincialstaffheadcountdeclinedfrom923553in2012to913033inMarch2015,withadecreaseofmorethan10000sincethestartofthecurrentfinancialyear.Thechangeshavenotnecessarilyresultedinsmallercompensationbudgets,largelyduetoaboveinflationwageincreasesandoccupation–specificadjustments”(p.30)Eventhoughhealthhasseensubstantialincreasesinitsbudgetoverthelastdecadeapointhasbeenreachedinthelastfewyearswhereprovincialhealthbudgetscannolongerkeeppace with substantial cost increases and the impact of inefficiencies and irregularexpenditure.Based on our own research we found that in the past years there was a view withinprovincialdepartmentsofhealththattheycouldoverspendonCoEbudgetsduringthefirsthalf of the year and that this overspendingwould be accommodated in the adjustmentsbudgets.12WhenadjustmentstotheirCoEbudgetswerenolongersufficienttoaccommodatehigherthanbudgetedCoEcostincreases,departmentshavebeenforcedtoshiftfundsfromgoodsandservicesandcapitalassetslineitemstoensurethatCoEiscoveredinfull.
10NationalDepartmentofHealth(2010).ConsolidatedReportoftheIntegratedSupportTeamInvestigationintoOverExpenditureinthePublicHealthSystem.Available:http://section27.org.za.dedi47.cpt1.host-h.net/wp-content/uploads/2010/06/Consolidated-IST-Report1.pdf11SouthAfricanTreasury(2015).MediumTermBudgetPolicyStatement2015/16.Available:http://www.treasury.gov.za/documents/mtbps/2015/mtbps/MTBPS%202015%20Full%20Document.pdf12RuralHealthAdvocacyProject(forthcoming).BudgetMapping:aqualitativeandquantitativeassessmentofbudgetingandexpenditureforruralhealthinSouthAfrica.

10
Inmany instancesdepartmental spendingwasnotproperlyadjusted for theseshiftsandexpenditureongoodsandservicescontinuedas‘normal’.Departmentshavemanagedthisover expenditure by delaying payments to service providers well beyond government’scommitment to pay invoices within 30 days. This has resulted in snowballing accruals,which have to be paid for from future budgets. These budgets then do not adequatelyaccountfortheneedtoclearoutstandingaccrualsandsoaccrualpaymentsaremadefrombudgetsthatshouldgotowardexpenditureinthecurrentfinancialyear.Thisresults inahiddenbudgetdeficit that isnotproperlymanaged,which in turnresults in furtheroverexpenditureandaccruals.Accrualswithinprovincialdepartmentsofhealth are substantial andhave reached crisisproportions in several provinces. In 2012/13 accruals totalled R3 billion in the EasternCape and R4 billion in Gauteng. By the end of 2014/15 the North West ProvincialDepartment of Health had accruals of R900 million, of which R600 million were foroverduepayments.Inthepastprovincialtreasurieshave,tosomeextent,beenamenableto‘bailouts’butthisisnolongerthecase.Departmentsarenowbeingrequiredtoimplementanumberofcost-savingandcost-cuttingmeasuresinordertoensurethattheyremainwithinbudget.Thesecost cutting measures are widespread and involve every aspect of departmentalfunctioning.In the North West, for example, a memorandum13dated 24 November 2014 from thedepartment’sChiefFinancialOfficer(CFO)announced:
i. Totalembargoonallappointmentsii. Totalembargoonnormalmaintenanceofphysicalinfrastructureiii. Totalembargoonpurchaseofequipment
Thesecost-cuttingmeasuresarebecomingmorepervasiveandarebeingimplementedineveryprovincewith varyingdegrees of impact. The concern for us now is that on-goingbudgetary pressures, if not managed properly will only deepen the crisis, withconsequencesmostacutelyfeltinpoorandlargelyruralprovinces.
3.MTBPS2015andBudget2016/17:adeepeningHRcrisisOnWednesday20October2015,theMinisterofFinance,MrNhlanhlaNene,presentedtheMediumTermBudgetPolicyStatement (MTBPS)14toParliament. The toneof thisyear’sMTBPS was particularly troubling and indicates a potential deepening of budget crisesalready being experienced within key service delivery departments such as health andeducation.Whileexpenditureacrossgovernmentwillcontinuetoincreasebyon-average1.6%aboveinflationeachyearoverthenextthreeyears,pooreconomicgrowthandincreasestothe
13http://www.rhap.org.za/wp-content/uploads/2015/10/Memo-by-NW-Provincial-Government_Staffing-Moratoria_September-2015.pdf14ThepurposeoftheMTBPSistocommunicatetheeconomiccontextinwhichbudgetingforservicedeliverywilltakeplaceoverthenextthreeyears.Itcommunicatesprioritiesaswellasbudgetaryconstraintsthatarebeingconsidered.

11
public sectorwagebill of 10.1% (more than2%above inflation)willmean thatbudgetswillremainunderseverepressurefortheforeseeablefuture.Servicedeliverydepartmentsarebeingforcedtoreprioritiseand“domorewithless”.Practically this means the implementation of further austerity measures that seem toinevitablyleadtofurtherstaffingmoratoria.TheMTBPSstatesthatinordertoaddresstheimpactofhigherthaninflationincreasestotheCompensationofEmployees(CoE):“TherevisedMTEFprovidesno fundstoexpandpublicsectoremploymentover thenextthreeyears.Departmentsthathadplannedtoexpandheadcountor fillvacanciesneedtopostpone their plans. Some institutionsmay need to reduce the number of people theyemploy.”(p.30)Departmentsarealsobeingaskedtoshiftfundsawayfromotherareasofthebudget,suchasgoodsandservicesand infrastructure toaccommodate increases in theCoE thathavenotbeenbudgetedfor.WhiletheNationalTreasuryhasstatedthatthisreprioritisationofbudgetswillbedoneina manner that “avoids any compromises to service delivery”, it remained unclear whatmeasureswouldbetakentoavoidcatastrophicconsequences,especiallyastheyrelatetodepartmentsbeingabletofillcriticalpostswithinthehealthsystem.In the 2016/17 National Budget Review15, which outlines spending priorities fro theupcomingyeartheTreasurydidprovidesomeadditionaldetailonmeasuresthatwouldbetakentolimittheimpactonservicedeliveryfromausteritymeasuresaimedatcontainingthe CoE budget item. Recognising that a blanket moratoria on appointments wouldseriouslycompromiseservicedeliveryintheBudgetReview,theTreasurynotesthat:“Effective 1 April 2016, appointments for non-critical vacant posts will be blocked ongovernment’s payroll system, pending the submission of revised human resource plans. Inmanycases,thesedepartmentalplanswillreducepersonnelheadcountsinadministrativeandmanagerial posts, eliminate unnecessary positions and establish a sustainable level ofauthorised, funded posts. Positions for teachers, nurses, doctors, police officers and othercriticalpostswillbeexcludedfromthelock,whichisaimedatadministrativeandmanagerialpersonnel.”(p.5)This statement indicated that the Treasury had shifted its thinking and was starting aprocessofidentifyingcriticalposts
4.Impactofpoorlymanagedstaffingmoratoria
15Available:http://www.treasury.gov.za/documents/national%20budget/2016/review/FullReview.pdf

12
BasedonarecentrapidassessmentbyRHAPontheimpactofstaffingmoratoriaandthefreezingofpostsonprovincialhealth systems16, particularly in rural areaswe found thefollowing:
1. Freezingofpostsresultsincriticalpostsremainingunfilled,whichhasanobvious consequence for access to care for patients as there are fewerhealthcareprovidersofferingservicesforagrowingdemand.
2. If a frozen post results in reduced supervision of junior health care
professionals/ workers, then the impact is significant beyond theindividual post not being filled. Here the impact involves diminishedaccountability, skills transfer and support for junior health careprofessionals.
3. Where frozen posts affect a capacitating component of the service
delivery process, such as procurement or financing processes, then theimpact is more significant for the bottleneck created. This limits theefficacyofservicesprovidedbyhealthcareworkers.
4. Frozen posts can result in reduced management of health care
professionals/workers aswell as other staff diminishing accountabilitymechanismsandefficientmanagementofscarceresources.
5. Ifapost is frozen ina facilityatwhich themanagement ispoor,and/or
the workload is high, then the impact of the frozen post is felt moreacutely,asistheresilienceofthehealthcareworkermoreeasilyerodedtodealwiththeconsequences.
6. Frozen posts have particularly severe consequences for rural facilities,
which are generally already understaffed. When posts remain unfilledother health careworkers are required to ‘pick-up the slack’. This addsundue pressure on remaining health care workers. This results in a‘dominoeffect’wherestaffresignorrelocateduetostress.Thosenewlyvacantpostsgounfilled,addinganadditionalburdenonstaffthatremain.Thiscontinuesuntilservicedeliverycollapsesentirelyatafacility.
The following quotes illustrate the impact of frozen posts on patients and health careworkersinNorthWestProvincealone:“MaternalandChildservicesareseverelyaffected,therearenotenoughnurses,nomidwives,andyouwill find 1 midwife on night duty. It goes against protocol because patients cannot be monitoredregularlycorrectly.Thisresultsinmaternaldeaths”.(Doctor)“ThetrainingofRegistershasbeengreatlyaffected,ItrytoassistwhereIcan.OurDCSTteamdoesnothave a Family Physician currently. There are simply no strategies that have been put in place toalleviatethesekindofproblems.”(Doctor)“Therehavebeennostaffappointmentsinthedistricteversincethestaffingmoratorium.Nurseshaveeitherresignedorretired.Theonesthatretiredtooktheirpensionduetotheconfusionthatiftheydid
16AcopyoftheRHAP’srapidassessmentintofrozenpostsisavailablefromtheRHAP’swebsite

13
not retire they would not have access to their pension. The Doctors that have left have not beenreplaced”.(Doctor)“The financial situation has affected us, our staff morale is low. We are no longer being paid forworkingovertime.Thishaslednursestoabusetheirsickleavedays.Thenursesprefertoparticipateinmoonlighting because they know that they will not get paid for working overtime. It is difficultbecauseitslikeyourdoingworkthatwassupposedtobedonebytwonurses.TheClinicalstaffarereallyoverworked.Becausethisisapsychiatristhospitalweneedpsychologists,twopsychologistsarenotenoughforall thewards.Patientshereneedcounselling.Wearetoldthattherearenopostsduetoalackofmoney.”(Nurse)“Services are affected, you know thatwe have to complywith theNational Core Standards, butwewontbeabletobecause,patient-waitingtimehasincreased.Beforeifwehard5ProfessionalNurseswewould be able to cut down patient waiting time. But nowwith 3 Professional Nurses they is adefinitedelay”.(Nurse)“Butyouknowsomeof theproblemsthathappenareduetoburnoutthat isexperiencedbydoctorsandnurses,theshortageofstaffisaseriousissue.Maybethingswillbebetterinthenextfinancialyearbutwhatguaranteedowehave”.(Doctor)Itisnotjustpatientsandcoalfacehealthcareworkerswhoaresuffering.Wehavereceivedreportsofseniormanagerssuccumbingundertheincreasingpressurestodeliverwithlessresources.Weareawarethatinoneruralprovince,5seniormanagersarebookedoffforstress-relatedproblems.
5.AdvancingtherighttohaveaccesstohealthcareintimesofausterityIfweappreciate that theremay simplynotbe sufficient resources to allocate topreventstaffingmoratoria itbecomesessentialthatsolutionsarefoundthatprotectcriticalpostswithin the health system. Blanket moratoria and the freezing of posts are untenable,unnecessaryandpossiblyunlawful.
6.Thelegalframework:obligationsandtoolsfordecision-makingSection27oftheConstitution(Act108of1996)affordseveryonethe“righttohaveaccessto health care services”, which right must be progressively realised within availableresources.TheConstitutionisexplicitthatitisthegovernment’sdutytoensurethateverymeasure,includinglegislativemeasures,istakentoensurethatthisrightisrealised.Giventhe catastrophic consequences on the health systemof the freezing of critical posts, thisimplicitlyincludesanobligationtoidentifywaystopreventthefreezingofcriticalposts.Therightofaccesstohealthcareservicesrequiresthatthestategoesfurtherthanmerelystatingtherightordevelopingstrategiesforitsrealisation.Withoutimplementableplans17andbudgetsattachedtothoseplans,thestate’sobligationsarenotmet.Itisinsufficientforthestatemerelytoarguethatfundsarenotavailable18orthataparticularpriorityhasnot
17GovernmentoftheRepublicofSouthAfrica&OthersvGrootboom&Others2000(11)BCLR1169(CC)at[40].18RailCommutersActionGroupvTransnetLtdt/aMetrorail2005(2)SA359(CC)at[88].

14
beenbudgetedfor.19Finally, iftherealisationofrightsisdependentontheoperationandefficiencyofsystems,theninefficientbudgetingandexpenditureisaviolationofrights.20Inadditiontolayingouttheobligationsonthestateregardingbudgetingforrights,thelawprovides good guidance on how to take decisions on the allocation of resources in thecontextofrights.Section 33 of the Constitution prescribes that everyone has the right to administrativeactionthatislawful,reasonableandprocedurallyfairandsection195oftheConstitutionprovidesforpublicadministrationgovernedbydemocraticvaluesandprinciplesincludingefficient,economicandeffectiveuseofresources.The administrative law requirement that decisions be reasonable has given rise tojurisprudence on themeaning of reasonableness as it relates to governmental decision-making.Foradecisiontobeconsideredreasonable, itmustberationalandproportional.Thismeansthatitmustbesupportedbyevidence,itmustfurtherthepurposeforwhichitwas made, and it must not be disproportionately onerous in effect. In this context,reasonabledecision-makingonhowtoapplyresourceswithinthehealthcaresectorwouldrequireanassessmentofthemaximumavailableresourcesthatcanbemadeavailable.Theneeds of the health care system should be assessed and the extent of the budgetaryshortfallestablished.Theimpactofpossiblecutsshouldbeconsidered,andadecisionthatensuresmaximumrealisationoftherightwithminimumdisruptionandminimumonerouseffectsshouldbetaken.Itisdifficulttoseehowadecisiontofreezethefillingofallposts,includingcriticalposts,andnot at the very least to use funding from recently vacated posts to fill human resourcesvacancieswheretheyareneededforservicedeliveryandtherealisationoftheright,couldbeconsideredareasonabledecision.TheobligationsandtoolsintheConstitutionandthelawguidedecision-makingandcanbeused to ensure an allocation of resources thatmaximally advances access to health careservices.
7.Possiblecoursesofactionindealingwithfrozenposts:threescenariosThereareanumberofwaysthatthegovernmentcanapproachthemanagementofhumanresourcesforhealthinthecurrentclimateofbudgetausterity.Anycoursetakenwillhavedifferent costs and trade-offs that must be considered. Below we offer three possiblescenarios andhoweachwill impact on both the implementation ofmoratoria and otherareasofservicedelivery.
7.1Continueoncurrentpathofausterity:wearetrainingforoverseascareersandtheprivatesector
The first approach that the government could take to managing austerity is to simplycontinuewithitscurrentcourseofaction.Inthisscenarioprovincialdepartmentsofhealth,
19CityofJohannesburgMetropolitanMunicipalityvBlueMoonlightProperties39(Pty)LtdandOthers2012(2)SA104(CC)at[74].20GlenistervPresidentoftheRepublicofSouthAfrica&Others[2008]JOL22590at[166]and[189].

15
with guidance from provincial treasuries, would continue to implement cost-cuttingmeasuresthatwouldnecessarilyincludehaltingthegrowthintheCoEbudgetitem.Basedontheapproachcurrentlybeingimplementedinmanyprovincesthiswouldinvolveputtingafreezeonthefillingofvacantposts.Herepostswillonlybefilledinexceptionalcircumstances,ifatall.Workingfromtheassumptionsthatsalarieswillcontinuetoincreasebeyondinflationeachyear while health budgets will struggle to keep pace with inflation, stabilising the CoEbudgetitemwillnotequatetostabilisingthestaffingestablishment.Infact,inthisscenarioastheTreasuryitselfsuggestsintheMTBPS,“Departmentsthatthathad planned to expand headcount or fill vacancies need to postpone their plans. Someinstitutionsmayneedtoreducethenumberofpeopletheyemploy”(p.30).ThismeansthatinpracticemaintainingthecurrentapproachtoausterityanditsfocusonmanagingCoEcosts,therewillinevitablybeareductioninthenumberoffundedpostsineach provincial departments staff establishment—a process that is already underway insomeprovinces.There are twobroad implications of taking this course of action. The first implication isthattherewillbeadeepeningofthecurrenthumanresourcesforhealthcrisisemerginginseveral provinces around the country. The consequences of which are described brieflyaboveandinmoredetailintheRHAP’srapidassessmentofstaffingmoratoria.Implications for the health system extend beyond difficulties in managing the filling ofposts over the short-term though. Actions taken now could potentially reverse steadyprogress beingmade in training anddeveloping human resources for the public system.Planstoexpandtheintakeofstudentsintomedicalschoolsandacceleratetheproductionof doctors through the Cuban programme could end up being a fruitless expenditure,wherebywe train health care professionals for the private sector or overseas.Why thismaysoundludicrous.TheanalysisabovecastsseriousdoubtonwhetherSouthAfricawillhavethefundingtoabsorbtheseadditionalgraduates.Data contained within the NDoHs HRH strategy 2012/13-2016/1721reveals that SouthAfricahaddonewellinincreasingthenumberofhealthcareprofessionalsworkingwithinthe public sector between 2002 and 2010. In that period the number of MedicalPractitionersworking in public service had increased by 60% or 6.1% on average eachyear.ThenumberofProfessionalNurses inthepublicsystemalso increasedsignificantlyby35%or3.9%eachyear.22WhilemuchoftheincreaseinthenumberofMedicalPractitionerscouldbeattributedtothe introduction ofmandatory community service of two years for all graduates it is animportantachievementnonetheless.
21NationalDepartmentofHealth(2013).HumanResourcesforHealthStrategyfortheHealthSector2013/14-2016/17.Availablehttp://www.gov.za/sites/www.gov.za/files/hrh_strategy_0.pdf22Ibid,p.21

16
Estimates for theperiodbetween2012and2014 reveal that totalnumbers entering thepublic service will have continued to increase. In the department’s HRH Strategy it isestimated thatby2014approximately1400medical schoolgraduateswouldbeenteringthepublicsectorfortheircommunityservice.Duetonaturalattrition(e.g.doctorsretiring)and doctors moving to the private sector, leaving medicine or moving abroad, it wasestimatedthatthetotalnumberofdoctorsworkinginthepublicsectorwouldincreasebyapproximately550individualsthatyear.23Thenumberofnurses(allcategories) isalsoestimatedtohaveincreasedsubstantially in2014. Accounting for all forms of attrition, the number of nurses working in the publicsectorwillhaveincreasedfrom143000in2013to148000bytheendof2014.Thismeansthatapproximatelyanadditional5000nurseswereaddedtotheestablishment.24If we assume that trends in training and the number of graduates entering the systemremainsconstantfortheforeseeablefuturethenthequestionemerges:howisthehealthsystem going to accommodate graduates for their community service if there is a goodchancethatprovincialhealthsystemswillneedtoreducethesizeoftheirestablishments?Theonelikelihoodisthatovertheshortterm,forMedicalPractitionersatleast,thesystemwillsimplynothireanypersonnelbeyondthoseundertakingtheirmandatorycommunityservice. So space will be made by not replacing staff at senior levels that retire, leavemedicalservicealltogether,movetotheprivatesectororabroad.If austerity continues for themedium term, the situation is then likely to become evenmorecomplicatedwhenapproximately1000Cubantraineddoctorsreturnannuallytothecountry from 2018 to 2023 to complete their training and undertake their communityservice.Thisisoverandabovethe1400(atleast)SouthAfricantrainedmedicalstudentsneedingtoenterthesystem.25Itisimportanttorememberherethatthesenumbersarejustformedicalpractitionersandnurses. They exclude numerous other categories of health care professionals such asphysiotherapists,occupationaltherapists,dentists,pharmacists,andspecialistswhoshouldalsobeabsorbedintopublicservice.Ifthehealthsystemcontinuesonthecurrenttrajectoryofausterity,theremaybespacetoabsorbmost community serviceprofessionals into the systemover the short-termandalimited number of professionals from other categories to replace those lost to naturalattrition.If,however,austeritycontinuesinto2018,thesituationislikelytobecomeevenmoredifficulttomanagesincethecapacitytoimplementcostsavings,gainefficiencyinthesystem and shift resources from non-prioritieswould have become exhausted. Thiswillmeanthatevenaccommodatingcommunityservicedoctorswillbevirtuallyimpossible.This brings us to the disconcerting, disillusioning and unacceptable, conclusion thatwithout significant financial increases to the CoE, which is unlikely to happen, manystudentsinSouthAfricaandthoseintheCubanprogrammearebeingtrainedtoenterthe
23Ibid,p.13324Ibid,p.13425Bateman,C.(2013).DoctorShortages:Unpackingthe‘CubanSolution’.IntheSouthAfricanMedicalJournal.103(9):603-609

17
private sector, move abroad, for other sectors in the economy, and in some casesunemployment.Theabovescenariohighlightsthatwearefacingasituationwheretheproblemisnolongerone of not being able to find health care professionals to fill vacant posts (even withintraditionally difficult rural settings) but rather one of not being able to accommodateincreasingnumbersofgraduateswhoareavailableandinmanyinstancesdesiretoworkinthepublicsector
7.2Findthemoney:allocatingadditionalresourcestofillpostsAnotherapproachcouldbe togivepriority tohumanresourceswithin thehealthsystemandidentifyingwaysofallocatingresourcestofillpostswhencandidatesareavailable.Therearepotentiallytwowaysofachievingthis:thefirstistosustainthetrendinmarginalgrowth in thenumberofhealthcareprofessionalsseenworking in thepublicsector26byidentifying ways of sourcing the revenue necessary to accommodate additionalremunerationpackages.TheNDoHhasestimatedthatiftheyweretofillallclinicalvacancies(identifiedasthe14mostimportantcategoriesofclinicalpersonnel)anadditionalR40billion(in2010terms)wouldneedtobeaddedtothehealthbudgetinthepublicsector.27Evenintimeswheretheavailabilityofbudgetislessofaconcernthanitisnow,fillingallvacantpostsatonceisnotpossiblebecauseofsignificantcostimplicationsandthefactthatthenumbersofhealthcareprofessionalsneededaresimplynotavailable.Amoreplausibleoptioninaversionofthisscenariowherethehealthsystemcontinuestoimprove access to health care professionals would be to sustain marginal increases inpersonnelinkeycategories(Nurses,doctors,OTs,Pharmacists,etc.),whichwouldincludeincreasesinsomecategoriesofsupportpersonnel(e.g.porters,cleanersandprocurement).Thisoptionwouldalsohavesignificantcostimplicationsforthehealthsystemthough.Forexample, if we assume that approximately 500 additional doctors will enter the publichealthsystemeachyearatanaveragecostofR85900028peryear,then(notaccountingforeffectsofinflation)anadditionalR430millionwouldneedtobeaddedtothebudgeteachyearfordoctorsalone.Assumingthatsalariesfordoctorskeeppacewithinflation,butnomore,thenthisnumberjumpstoR450millionfor2016/17.Even if a decision wasmade not to expand the clinical establishment within the publichealth systembut rather to keepnumbers at their current levels, as things arenow, thehealthsystemwouldstillneedtofindwaysofincreasingallocationsforCoE.Excludingthecost of recruitment to replace staff that leave the public service, for 2016/17 the health
26Thegovernmenthasbeenabletoincreasethenumberofprofessionalsenteringthepublicservicesince2002byincreasingtrainingandintroducingmandatorycommunityserviceforsomecategoriesofhealthcareworker27HumanResourcesForHealthStrategyforSouthAfrica2013/14-2016/17,AnnexureA,p.6
28MediancostfordoctorsworkinginthepublicsectortakenfromtheHRHStrategyandadjustedforinflationtoberepresentedintodaysterms

18
system will need to increase the CoE budget by R9.5 billion to accommodate the 10%increaseinremunerationagreedtofornextyearalone.29Thisismorethandoubletheprojectedincreasetothehealthsystemsentirebudgetforthatyear.Thismeansthatifadditionalresourcesarenotallocatedbeyondwhatwasprojectedin theMediumTermExpenditureFramework for2015/16, fundswillneed tobe shiftedfromotherareasinthebudget(e.g.goods&servicesandinfrastructure)inordertosustaincurrentstaffinglevels.
7.3Doingthingsdifferently:maximisingbenefitsThe above scenarios are either not desirable or realistic under the given circumstances.The currentpathof sweeping austerity and the implementationof blanketmoratoria onthefillingofpostsinmanyprovincesisuntenable.Thisapproachquicklyleadstoadeclineinaccesstoservicesandthequalityofservicesbeingdelivered.Itrunscontrarytoboththerighttohaveaccesstohealthcare,enshrinedinSection27oftheConstitutionandcannotbeconsideredrationalorproportionalintermsoflegislationsuchasPAJA.While identifying ways of bringing additional resources into the public health systemshould certainly be a priority, especially with regard to promoting greater access andequityinaccesstocare,overtheshort-termitisadifficultproposition.InprotectingaccesstohealthcarewithintheobligationsoftheConstitution,theNationalHealth Act and Promotion of Administrative Justice Act, it is evident that a differentstrategyhastobeapplied.Efficiencyinallocatingscarceresourcesisrequired.Efficiencyinthis this regard does not mean cost cutting though, it means spending money wheregreatestbenefitwillbeachievedandwheretheimpactofbudgetconstraintswillhavetheleastimpactonservicedelivery.Thiswouldconsistofimmediate,shorttermandmedium-to-longtermsolutions.Importantly theDepartment’sHRHStrategy recognises the threat thatausterityposes toservice delivery in rural areas through the implementation of blanketmoratoria on theappointmentofstaffandexplicitlystatesthatstakeholdersshould:“Ensurethatprovincesdonotfreezecriticalhealthprofessionalpostsinunderservedandrural areas as part of hiring moratoria resulting from overspending, through thedevelopment of norms for minimum numbers of health professionals for districtfacilities.”30BoththeNationalDepartmentofHealthandTreasuryhavestartedtoengagecriticallyontheprotectionofcriticalpostsasan interimsolutiontomanagingCoEexpenditurewhilelimiting its impact on service delivery. As mentioned earlier the Minister of Finance’sannouncement that frontline posts would be excluded from a freeze is the most publicexpressionof thisbut it isnot theonlypointof engagement.Aspart of aprocessof on-goingdirect consultationwith officialsworkingwithin the health systemat theNational
29CostestimatescalculatedbasedonprojectedconsolidatedhealthbudgetallocationscontainedwithintheNationalBudgetReview2015/16,availableat:http://www.treasury.gov.za/documents/national%20budget/2015/review/default.aspx30HumanResourcesForHealthStrategyforSouthAfrica2013/14-2016/17,P.125

19
andprovinciallevels,Treasuryofficials,healthcareworkers,civilsocietyandruralhealthpartners,theRHAPhasbeenworkingonandrefiningabroadsetofguidelinesthatprovidea more nuanced approach to identifying and protecting critical posts than the onedescribedbytheMinisterofFinance.Themostrecentversionoftheseguidelinesweredevelopedduringaroundtablemeeting,whichtookplaceon1April2016,ofruralpartnerstheNDoHandTreasuryondevelopingeffectiveHRHstrategiesduringtimesofausterity.Atthatmeetingtheagreedtoguidelinesweregivenasfollows:
1) The National Department of Health in collaboration with the Treasuryshouldprovideguidance throughpolicyonhowprovincesareexpected toprotectcriticalpostsattimesofausterity.Thisshouldinclude:
• Inputbyhealthandpartners,inparticulararounddefinitionofcritical.• Principles of transparency and consultation, which should include
transparency on savings in managerial/admin positions versus frontlinehealth professionals, and an escalation procedure in the event thatprovincesdonotimplementtheguidelines
• Anationalplanregardingcommunicationanddistributiontoprovincesaswelltimeframesforthereleaseoftheguidelines
• Some standardization in implementation: what is required from people;whoisresponsibleforwhat.
2) Adequate consideration should be given to inhospitable and underserved
areas so as to ensure disadvantaged communities are not furthermarginalisedintheiraccesstohealthcare.Thisincludesbutisnotlimitedtoruralhealthcontextsfortheiruniquecharacteristicsandchallenges.
3) It is national policy to use normative guides “WISN” where available
(currentlyforclinicsandCHCs)toidentifytheminimumpoststobefilled.• Whiledoingso,facilitiesmustensuretoadequatedata,whichisnotlimited
toheadcountandotherutilizationdata.Populationdatamustbeused toinclude unmet need, as alluded to in section 6 of the WISN normativeguidelines. In the event that current staffing levels are less than theminimum“WISN”norms,additionalstaffing is tobeadvocated forby thefacility.Intheeventthatnofundingisavailableforsuchadditionalstaffing,the facility needs to identify the critical healthposts to beprioritized, asguidedbythenationalguidelines
4) Critical posts need to be defined locally and these can include healthprofessionals and support staff. The purpose is not to define whichcategoriesofstaffaretobeconsideredcritical.InsteadtheconsequencesonpatientcareshouldbethedeterminingfactorondecidingwhetherpostAinfacility B is critical under the given circumstances. Here critical posts are

20
simplydefinedasthosethatpotentiallyhavecatastrophicconsequencesforservicedeliveryiftheyremainunfilled.
Herekeyunderlyingprinciplesindefiningcriticalinclude:• Theprotectionoffrontlinehealthprofessionals• Theprotectionofservicestothepoorandthemarginalised-whohavethe
leastoptionofservices• Provincially:themoreruralthemoreprotection• Districtlevel:themoreruraldistrictsthemoreprotection
5) DistrictsareexpectedtodevelopcostedHRplansbutthisdoesnothappen;
if suchplansare inplace it canhelpDistrictManagers to identifypriorityposts at times of staffing moratoria. The National and ProvincialDepartments of Health must ensure Districts have such plans in place.TreasuryshouldprovidesupportinthecostingoftheHRplans.
6) Decision–making on cost-saving and cost-cutting must be made at the
district level by giving districts the amount to be saved and allowing thedistricttodecide.
• Thesedecisionsmustbesupportedbyguidelinesondefiningcriticalposts
andmustbe informedby thePromotionofAdministrative Justice (PAJA)principles of evidence-based decision-making, rationality andproportionality togiveeffect to the constitutionaldutyofGovernment toprogressivelyrealisetherighttohealth.
7) Corruptionandunauthorizedexpenditureshouldbeperformancemanaged
instead of punishing all managers and districts by withdrawing theirdelegationsofauthoritiesforthetransgressionsofothers.Thiswouldmeanthatprovincialdepartmentsandinstitutionsshouldbeheldaccountableforperformancemanagement.
8) In the event of a Section100 intervention orwhenTreasury co-manages a
Health Department, there should be an up-front agreement around theprioritizationofhealthneedsandclearprocessesforappointmentstooccur.
• In thisevenstrategiesmustbeput inplace toreducethetime it takes tomake appointments when there is co-management/S100 intervention toovercometimecostsofaddedlayersofdecision-making.
• Process’needtobepredictable,aspeoplegetfrustrated,startinterveningetc.
ThescareresourcesavailableforhumanresourcesforhealthinSouthAfricamustbeusedto achieve greater equity and the right to access health. Within the tight fiscal climateevidence-based decision-making and efficient use of scarce resources becomes morepertinent than ever. Efficiency in this regard does not mean cost cutting. It means theallocationofresourcesthatmaximallyadvancesaccesstohealthcareservices,basedontheprinciplesenshrinedintheConstitutionandPAJA.

21
[ENDS]ForadditionalinformationorcommentonthisdiscussiondocumentpleasecontactDaygan