Embed Size (px)
Citation preview

Catheter Ablation in Supraventricular Tachyarrhythmias
SANJAY DESHPANDE, M.D., MOHAMMAD JAZAYERI, M.D., ANWER DHALA, M.D.,
ZALMEN BLANCK, M.D., JASBIR SRA, M.D., and MASOOD AKHTAR, M.D.
From the Wisconsin Electrophysiology Group, University of Wisconsin-Milwaukee Clinical Campus, Milwaukee Heart Institute of Sinai Samaritan Medical Center and St. Lukes Medical Center, Milwaukee, Wisconsin
Introduction
The management of supraventricular tachyarrhyth- mias (SVTs) has undergone significant changes in the past decade. Until recently, drugs were the mainstay of therapy and arrhythmia surgery was offered as a last resort in selected patients. The advent of catheter ablation has revolutionized the management of these tachyarrhythmias. Catheter ablation in tachyarrhyth- mia management was first reported by Vedel et al.' as early as 1979, when it was used to interrupt atrio- ventricular (AV) conduction. The technique has since been refined and its application extended beyond AV junctional ablation, to ablation of accessory pathways (APs),2-" and AV nodal and more re- cently atrial ta~hycardias''-'~ and atrial flutter." A general introduction to the application of this interven- tional modality in SVT will be presented in this article.
Pathophysiological Substrates for Supraventricular Tachycardia
SVT is defined as any tachycardia originating above the level of the bundle of His. The underlying substrate in each SVT is unique and their management may be facilitated by a functional approach rather than view- ing them in a generic manner. This functional classifi-
cation of SVTs is based on the role of the AV node during tachycardia, and hence they are divided into:
(1) AV junctional reentrant tachyarrhythmias: use the AV node as a critical component of the reentrant circuit. They include AV nodal reentry, and AP me- diated tachycardias.
(2) Atrial tachyarrhythmias: which do not require the AV node for maintenance of tachycardia and the node is only used as a passive conductor. These in- clude atrial fibrillation (AF), flutter, and atrial tachy- cardia.
SVTs with an atrial origin are usually acquired and are commonly associated with underlying structural heart disease. In those individuals without identifiable abnormalities, fibrosis is uniformly noted if pathologi- cal evaluation is undertaken. The cellular genesis for fibrillation and flutter are primarily felt to be intraatrial reentry. However, an automatic mechanism is com- mon in atrial tachycardia.2'*22 In contrast, AV junc- tional reentrant SVTs are usually related to an anoma- lous substrate (dual AV nodal pathways or an acces- sory AV connection) and the heart is otherwise structurally normal. This distinction has important bearing on the management of these tachyarrhythmias. since in some patients with atrial SVTs, a permanent cure may not be feasible, recurrence is higher, and the underlying heart disease may govern long-term out- come despite controkure of the SVT.
Address for reprints: Sanjay Deshpande, M.D., Milwaukee Heart Institute, Sinai Samaritan Medical Center, 960 N. 12th Street, Mil- waukee, W1 53233. Fax: (414)283-621 l.
Submitted for publication May 2, 1994; accepted for publication May 9, 1994.
Clinical Manifestations
Symptoms related to SVT may be due to the rapid ventricular rate and loss of AV synchrony causing hy-
Vol. 8, No. 1, 1995 Journal of Interventional Cardiology 59

DESHPANDE. ET AL.
poperfusion, but may also be due to loss of AV syn- chrony alone, or irregularity of the ventricular rate as in AF or flutter. In most patients, the symptoms are relatively benign, however, presyncope and syncope due to tachyarrhythmia are not uncommon. In addi- tion, recurrent SVT may be psychosocially disabling and may significantly limit patients’ lifestyles. In a minority of patients, sudden cardiac death may be a clinical presentation, especially in those with multiple
Biophysical Basis of Ablative Therapy
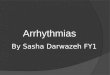
The goal of transcatheter ablative therapy is the lo- calized destruction of cardiac tissue that is putative in arrhythmogenesis, without compromising the struc- tural and functional integrity of surrounding tissue. Localization of the intended site is accomplished by manipulation of the catheter tip within the cardiac chamber, aided by fluoroscopy and intracardiac elec- trograms. During the application of catheter ablative therapies, energy is transferred from a generator, be- tween an endocardia1 catheter with a 4- to 5-mm plati- num tip and an adhesive electrosurgical dispersive patch, producing tissue trauma at the electrode tip- tissue interface (Fig. 1). Lesion volume is governed
by the nature of the energy source, area of contact, tissue characteristics, and the total amount of energy delivered.24 Several sources of energy have been uti- lized, and the quest continues to identify the ideal source. The primary modalities used for catheter abla- tion along with their comparative aspects are discussed below.
(1) Direct current shock: A conventional external defibrillator is used as the energy source. The applica- tion of high energy DC current results in the produc- tion of a nonhomogenous lesion primarily as a conse- quence of the high voltage electrical field generated during discharge. In addition, plasma arcing with tem- peratures reaching up to 1,700°C, and a shock wave that produces barotrauma contribute to tissue injury.24 Although historically the first source used’ with excel- lent results in early investigators hand^,*^*^^ this method has fallen into disrepute in current practice, primarily due to concerns regarding serious short- and long-term sequelae. These include cardiac perforation, tamponade, AV block, acute ventricular dysfunction, acute coronary artery spasm, ventricular tachyarrhyth- mia or fibrillation immediately postshock, and sudden cardiac death during long-term f~llow-up.~’ In addi- tion, short-term recurrence rates are higher due to the transient nature of the barotraumatic effects, necessi- tating a repeat ablation. By virtue of its destructive
Figure 1. Schematic representation of catheter ablation: energy from a power source is channeled through a large tip deflectable catheter. which has been positioned within the cardiac chambers, and the circuit is completed by an adhesive dispersive patch in the interscapular area. Localized tissue trauma is produced in the proximity of the electrode tip of the catheter leading to intemption of the arrhythmogenic circuit.
60 Journal of lnterventional Cardiology Vol. 8, No. I , 1995

CATHETER ABLATION IN SUPRAVENTRICULAR TACHYARRHYTHMIAS
force, a larger lesion volume is generated with DC shock than with other methods, and this may be advan- tageous should the target substrate be relatively deeper or diffuse.
(2) Radiofrequency energy: The modulated output from a conventional electrosurgical RF generator, originally an alternating current (frequency range 10 kHz-900 MHz) is delivered through the catheter. This generates heat in the tissues adjacent to the electrode tip, causing tissue damage by denaturation of protein and dehydration.” A clear advantage of RF energy is the ability to titrate the power output over a period of time during delivery so that lesion size can be con- trolled, in contrast to the instantaneous and seemingly uncontrollable outcome from a high energy DC shock.
At the present time, taking all these considerations into account, DC as an energy source has been rele- gated to a secondary status for catheter ablation at most centers, and RF energy has become the preferred
The catheter used for the ablative procedure chan- nels this energy to the tip electrode and the circuit is completed by an adhesive electrosurgical skin patch. A large tip electrode is usually used to optimize dissi- pation of energy to the adjacent tissues. Catheter tip- tissue impedance rise (implying excessive local tem- peratures) is prevented by the use of a larger catheter tip surface area, cooled by the surrounding blood flow, thermistor monitoring, or gradual titration of the en- ergy output. Manipulation of the catheter tip and accu- rate placement is facilitated by the use of catheters in which the terminal portion of the shaft can be deflected in a controlled manner. Catheter technology at this point in time is imperfect for the utilization of alterna- tive energy sources such as microwave, cryo, or laser and, therefore, has precluded clinical applications.
choice.4.5. 10, I I , 15.17.20.29
Catheter Ablation in Atrioventricular Junctional Reentrant
Supraventricular Tachycardias
(1) The reentrant nature of atrioventricular nodal reentrant tachycardia is based on the presence of at least two functionally disparate conducting pathways. Although the boundaries of the reentrant circuit are still a subject of controversy, it is generally believed that both the AV node and the perinodal atrium are inv01ved.I~ The so-called “fast” and “slow” AV
nodal pathways appear to be functionally distinct and anatomically separated thereby facilitating selective ablation of either. The right heart approach is univer- sally used for this procedure, and the slow pathway has been preferentially targeted with excellent results and a minimal risk of AV block.’0~1’~’3*’8
(2) The accessory pathway is an anomalous ana- tomica1 connection between the atria and ventricles and is located either at the mitral or tricuspid annulus. The AP may be capable of uni- or bidirectional con- duction, and may be manifest (delta wave on the sur- face echocardiogram) or concealed (capable of retro- grade transmission only). Accessory pathways may participate in several types of SVT, but the commonest form is the orthodromic in which the AP forms the retrograde limb and the AV node the antegrade limb of the reentrant circuit. The AP may also be involved in an antidromic tachycardia in which the direction of the circuit is the reverse of the orthodromic form. Additionally, the AP that is capable of antegrade con- duction may act as an “innocent bystander” and con- duct to the ventricles during AF, flutter, atrial tachy- cardia, or AV nodal reentry. Mapping and ablation is performed by positioning the ablation catheter tip electrode on the annulus in the vicinity of the AP as determined by electrogram analysis. Initial experience with this technique utilized DC shocks?’ however, RF energy has superseded this as the method of choice with exceptional long-term cure rate^.^.^.".' 8,29,30
Catheter Ablation in Atrial Supraventricular Tachyarrhythmias
(1) In atrialfibrillation, the reentrant process is not anatomically discrete, although the mechanism of the tachyarrhythmia appears to be reentrant in nature. Lo- calization by atrial mapping is not feasible since the reentry is chaotic, and ablation is exclusively used to limit the ventricular response in those patients who are symptomatic due to rapid or irregular ventricular rates. The AV node is, therefore, the target for catheter abla- tion, and one of two approaches is adopted:
imply- ing irreversible interruption of conduction in the distal segment of the AV node or the proximal portion of the His bundle with consequent complete AV block. This procedure usually requires implantation of a per- manent pacemaker thereafter, since the residual escape rhythm is chronotropically inadequate.
a. Ablation of the AV
Vol. 8, No. 1, 1995 Journal of Interventional Cardiology 61

DESHPANDE. ET AL.
b. Selective ablation of the antegrade slow AV nodal pathway, which has been shown to limit the ventricular response significantly, and may not require permanent pacing.34 This method has not been widely utilized since it is a relatively new application.
It is important to realize that catheter ablation in atrial fibrillation is a palliative procedure since the ar- rhythmic mechanism itself is not targeted. Conse- quently, it does not attenuate the thromboembolic risk, nor does it restore AV synchrony. It is, however, clearly beneficial in controlling the rapid ventricular response especially in those patients in whom medical management is limited, or has been unsatisfactory. Al- though either ~ ~ 2 5 . 2 6 or RFlo.18 .31-33 energy has been used for ablation of the AV junction, and has provided excellent and comparable results, RF energy has be- come the preferred source for the reasons previously mentioned.
( 2 ) The reentrant process in typical or type I atrial flutter is organized and mapping and ablation are pos- ~ i b l e . " . ~ ~ - ~ ~ In typical atrial flutter, a zone of slow conduction can be identified in the posteroseptal right atrium and appears to be critical in sustaining reentry since ablation in this region can terminate flutter and prevent its immediate reinduction. This area is anatom- ically defined and is posterior or inferior to the ostium of the coronary sinus. Initial experience with this pro- cedure was obtained using DC s h o ~ k s . ~ ' , ~ ~ Recent lit- erature on highly selected patients with type I flutter demonstrates the effectiveness of RF energy with ex- cellent results during short-term In the event that atrial flutter mapping and ablation is not successful, or flutter recurs during follow-up, the AV node may be secondarily targeted as in fibrillation, to limit the ventricular response and irregularity.
(3) Atrial tachycardias are an uncommon arrhyth- mia in adults, but are likely to be refractory to medical management."-" They are generally due to enhanced automaticity, but occasionally may be due to intra- atrial reentry. The site of origin is usually in the right atrial free wall, but may be in the left atrium or the interatrial septum. Results of catheter mapping and ablation have been gratifying with long-term follow- up.15-19 As in the case of flutter, should mapping and ablation be unsuccessful, ablation of the AV junction may be considered to control the ventricular rate.
Approaches for Catheter Ablation
A variety of options are available in the choice of analgesia and anesthesia during the ablation proce-
dure, ranging from none to general anesthesia. This is determined by several factors: the anticipated proce- dure time based on the experience of the team, patient preference, and individual tolerance. Monitored con- scious IV sedation using Midazolam, Fentanyl, Mor- phine, Meperidine, or Valium, alone or in combina- tion, is widely used with RF a b l a t i ~ n . ~ , ' ~ . ~ ~ In contrast, general anesthesia is essential when DC shock is used to obviate the anticipated discomfort. On occasion, tachycardias may not be inducible due to the depres- sant effects of these agents and may require the use of stimulants such as isoproterenol or atropine.
A comprehensive baseline electrophysiological study is an absolute prerequisite except when complete AV junction ablation is the only procedure contem- plated. The study requires the placement under flour- oscopic surveillance, of several multipolar electrode catheters. These are introduced percutaneously via the femoral, antecubital, subclavian, or internal jugular veins, and positioned under fluoroscopic guidance in the right atrium and ventricle, and the tricuspid annu- lus to obtain a His-bundle recording, and the coronary sinus to record activation along the left AV groove. During the study, incremental pacing and programmed extrastimulation is performed from the atrium and ven- tricle to establish antegrade and retrograde conduction characteristics and refractory periods of both normal and accessory tissues. In addition, the clinical tachy- cardia is induced and the electrophysiological mecha- nism is established with certainty using standard diag- nostic criteria. Reproducible and reliable induction of the clinical SVT prior to catheter ablation is essential to establish efficacy postablation. In addition, pre- and postablation conduction characteristics and refractory periods are compared to evaluate efficacy of ablative therapy.
Catheterization of the right heart is the conventional approach for ablation in SVT and is performed by can- nulation of the femoral vein. This approach suffices for most applications. However, left heart catheteriza- tion is necessary either for mapping and ablation of atrial tachycardia, left-sided APs, or the AV junction. Transseptal catheterization'8.30 or the retrograde femo- ral arterial route may be used for left heart catheteriza- tion; either adds to potential morbidity. Transesopha- geal echocardiography can be used to guide the transeptal puncture, catheter manipulation, and place- ment when performing left-sided AP ablation. This imaging tool can complement fluoroscopy and elec- trogram analysis in catheter placement and selection
62 Journal of Interventional Cardiology Vol. 8, No. 1, 1995

CATHETER ABLATION IN SUPRAVENTRICULAR TACHYARRHYTHMIAS
of the optimal site for catheter ablation, and recognize complications such as pericardial effusion or valvular regurgitation well in advance of hemodynamic mani- festation. The duration of hospitalization for the abla- tion procedure is generally 2-3 days.
The Learning Curve Phenomenon
The outcome in catheter ablation is somewhat de- pendent on the operator since catheter mapping and ablation requires a certain degree of skill. The impact of increasing operator experience is reflected not only as an improvement in success rates, but also shorter procedure and fluoroscopy times, and a reduction in procedural complications. In a published series of the experience with the first 400 patients, Calkins et al.39 observed that the percentage of patients with an initial failure of ablation of an AP significantly decreased only after the first 250 patients. The implications of such observations, similar to the published experience with coronary procedures, suggest that the procedure be performed only at centers with significant experi- ence, in order to anticipate an optimal outcome.
Radiation Exposure
A significant amount of radiation exposure, princi- pally related to fluoroscopy, can occur both to the pa- tient and the operator during catheter ablati~n.~'.~' The potential hazard for either person is the risk of develop- ment of a fatal malignancy or genetic defects. Fluoro- scopic exposure during AP ablation has been reported to range from a mean 23-44 minutes, and during AV nodal modification 19-25 minutes. This probably re- flects the ideal rather than the typical exposure since it may not be representative of unpublished experiences, which are likely to be higher. Considering that each hour of fluoroscopic exposure is associated with a life- time risk of developing a fatal malignancy of 0.1%, and a risk of a genetic defect of 20 per 1 million live births, this issue is one of significant concern when ablative therapy is contemplated. However, it is reas- suring to note that these radiation risks are actually acceptable when compared with the risks of alternative therapies such as antiarrhythmic or arrhyth- mia surgery.44 A considerable reduction in radiation risk can be achieved by minimizing fluoroscopy time,
avoidance of magnified fields, collimation of the ra- diographic beam, the use of pulsed fluoroscopy, and a "shared risk" approach with the use of several oper- a t o r ~ . ~ ' . ~ ~ It is important not to lose perspective by prolonging procedure times in the relentless pursuit of success, and accept failure rather than mounting radiation risk.
The Cost of Electrotechnology
Unlike some technologies, catheter ablation was de- veloped using existing hardware that was modified (electrosurgical RF generator), thereby avoiding addi- tional expense for the initial setup. Although it may appear as an aggressive and expensive curative option for a rhythm disturbance that is rarely lethal, the cost of long-term pharmacological therapy (including peri- odic physician and laboratory monitoring), emergency room visits or hospitalization for recurrent SVT, and lost work days, need to be taken into account. The substantial initial procedural costs (roughly $16,000) have been shown to be offset by the significant long- term savings in medical expenses especially when catheter ablation is offered to younger patients who are likely to incur these over their lifetime.46347 Obviously, complications or a failed ablation procedure would add needless expenditure besides risk, underscoring the importance of performing the procedure at experi- enced centers.
Complications
The enthusiasm for catheter ablation must be tem- pered by the knowledge that the procedure has the potential for morbidity and mortality. It is heartening to note that the recently published experience with this technique shows that the associated short-term mor- bidity and mortality are extremely low (nonlethal com- plication rates 0%-4%), although a publication bias is likely.2-20~30
(1) Generic complications: related to vascular ac- cess and catheter placement include development of a hematoma, arteriovenous fistulae, cardiac chamber perforation with hemopericardium or tamponade, deep venous thrombosis, thromboembolism, and septec- emia.
Vol. 8, No. 1, 1995 Journal of Interventional Cardiology 63

DESHPANDE. ET AL.
( 2 ) Complications related specifically to catheter ablation include the following:
a. AV block: has been primarily reported with se- lective “fast pathway” ablation, and rarely inadvert- ently when the slow pathway is targeted.10.”.”.’8 In view of this. fast pathway ablation has been relegated to a secondary choice in AV nodal modification, since the risk of block with slow pathway ablation is negligi- ble. The risk of AV block is also an issue when at- tempting ablation of a right anteroseptal AP due to its proximity to the AV node/His-bundle region. The development of inadvertent permanent AV block usu- ally necessitates permanent pacemaker implantation.
b. Valvular regurgitation: may occur due to damage to the chordal apparatus or the leaflets of the mitral. tricuspid. or aortic valve during catheter manipulation. It is an uncommon and usually inconsequential com- plication and is visualized as an eccentric jet on Dopp- ler echocardiography.
c. Other reported complications include myocardial infarction, aortic dissection. endocarditis, pericarditis. and death.
The Present Role of Catheter Ablation in Supraventricular Tachyarrhythmia
There is little doubt that the impetus behind the pro- liferation of catheter ablation has been its remarkable capability to cure several tachyarrhythmias, and not merely provide suppressive therapy (Table I ) . The use of antiarrhythmic drugs besides being limited by inef-
ficacy, is associated with a 3%-34% proarrhythmic risk including occasional fatalities, drug intolerance, organ toxicity, and the potential for genetic defects when used in women of childbearing age.42,43 Catheter ablation was introduced as an investigational proce- dure, to fill the void between failed drug therapy and the need for arrhythmia surgery, however its over- whelming success has propelled it to the status of a serious contender for the initial therapy of choice. The following sobering issues deserve consideration at this point.
The published experience with catheter ablation is far smaller than the actual number of patients who have undergone this procedure for the management of SVT.48 Data from a few select centers with a large experience is likely to be more favorable than the larger unpublished experience, and hence published success and complication rates are not necessarily the norm. Although electrophysiological testing per- formed months after catheter ablation has documented low recurrence rates and the absence of inducible ven- tricular tachyarrhythmia, the long-term result with re- gards to recurrence or long-term complications follow- ing catheter ablation is unavailable at this time. It is likely though, that it will parallel the favorable out- come from surgical experience. Finally, although un- common, serious complications including mortality may result from the procedure intended to cure a non- life-threatening illness. Therefore, albeit tempting, a uniform recommendation of catheter ablation as the initial therapy of choice for all untreated SVT patients is premature at this time.
Table 1. Resultc of Catheter Ablation in Supraventricular Tachycardia
Patient Succe\s AV Block Recurrence SVT Type AuthorNear ( n ) 9 % 7c
AVNRT Lee. 1991 39 85 8 5 Chen. 1993 100 98 2 2 Haiswguerrc. 1992 64 I 0 0 0 0 Kay. 1993 215 99 I 6
AP Jackman. 199 I I66 99 9 Calkins. 1992 ?SO 94 7 Suani. 1992 I 1 1 95 9 Ka!. 1993 363 95 5
AFL Feld. I992 12 83 16 Kdq. 1993 13 76 7
AT Tracy. 1993 10 80 20 Kay. 1992 16 I 0 0 18
Published data of the results of catheter ablation in supraventricular tachyarrhythmias using radiofrequency energy is tabulated above. AP = accessory pathway. AVNRT = AV nodal reentrant tachycardia. AFL = atrial flutter. AT = atrial tachycardia.
63 Journal of Intenentional Cardiology Vol. 8. No. 1. 1995

CATHETER ABLATION IN SUPRAVENTRICULAR TACHYARRHYTHMIAS
Figure 2. Therapeutic options in the management of atrioventricular reentrant tachycardias: a schematic representation of the reentrant circuit is accompanied by its typical electrocardiographic appearance, and the therapeutic options with potential target sites are highlighted as catheter ablation (C), antiarrhythmic drug therapy (D), or arrhythmia surgery (S). Atrioventricu- lar nodal reentrant tachycardia is depicted in panel A, and accessory pathway mediated tachycardia in panel B.
The decision to proceed with ablative therapy should be individualized after discussion of the pros and cons of all available therapeutic options with the patient (Figs. 2 and 3). Catheter ablation for SVT may be considered in the following situations:
a. Symptoms of SVT are unresponsive to conven- tional drug therapy.
b. SVT is paroxysmal but severely symptomatic or hemodynamically compromizing when it occurs, and chronic drug therapy seems onerous for relatively in- frequent episodes.
c. Drug therapy is limited by poor ventricular func- tion, bradycardia, or associated noncardiac disease (hepatic or renal dysfunction, or obstructive lung dis- ease).
d. Atrial fibrillation and severe sinus bradycardia (the “tachy-brady syndrome”) when drugs are used to limit rapid heart rates produces severe bradycardia, or permanent pacemaker implantation is contemplated for bradycardia, however, the patient remains symp- tomatic from rapid ventricular rates during AF with or without drug therapy.
e. Young patients or those with childbearing poten- tial in whom curative therapy is preferable to long- term pharmacological therapy.
f. Patient preference for therapy with a curative po- tential over drug therapy.
g. To avert potential catastrophic sequelae in pa- tients engaged in high risk occupations (pilots, ath- letes, and public and commercial vehicle operators).
Conclusion
Catheter ablation has emerged as a valuable addition in the therapeutic strategies available for the manage- ment of SVTs with a high rate of success and low recurrence and complication rates, providing an oppor- tunity for a cost-effective permanent cure. An optimal outcome may be expected from centers with a large experience, who are well beyond the learning curve. The development of this remarkable modality is not only a milestone in “techno-therapeutics”, but has
Vol. 8. No. 1, 1995 Journal of Interventional Cardiology 65

DESHPANDE, ET . AL
Figure 3. Therapeutic options in the management of atrial tachyar- rhythmias: a schematic representation of the arrhythrmc mechanism is accompanied by its usual electrocardiographic appearance, and the therapeutic options with potential target sites are highlighted as catheter ablation (C) and antiarrhythmic drug therapy (D). Atrial fibrillation is shown in panel A, type I atrial flutter in panel B. and atrial tachycardia in panel C. Rarely, arrhythmia surgery may be considered in atrial tachycardia.
also provided the electrophysiologist significant in- sights into the mechanisms of these tachycardias. De- spite the superb published results, its place in relation to alternative therapies in the management of SVT, has not been clearly established at this time.
References
1. Vedel J. Frank R. Fontaine G. et al. Bloc auriculo-ventriculaire intra-Hisien definitif induit au cours d’une exploration endo- ventriculaire droite. Arch Ma1 Coeur 1979;72: 107.
2.
3.
4.
5 .
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20
Borggrefe M, Budde T, Podczek A, et al. High frequency alternating current ablation of an accessory pathway in hu- mans. JACC 1987;10:576-582. Warin JF, Haissaguerre M, D’lvemois C, et al. Catheter abla- tion of accessory pathways: Technique and results in 248 pa- tients. PACE 1990; 13: 1609- 1614. Jackman WM, Wang X, Friday KJ. et al. Catheter ablation of accessory atrioventricular pathways (Wolff-Parhnson-White syndrome) by radiofrequency current. N Engl J Med 1991;
Calkins H, Langberg JJ. Sousa J, et al. Radiofrequency catheter ablation of accessory atrioventricular connections in 250 pa- tients: Abbreviated therapeutic approach to Wolff-Parkinson- White syndrome. Circulation 1992;85: 1337- 1346. Dick M, O’Conner BK, Serwer GA, et al. Use of radiofre- quency current to ablate accessory connections in children. Circulation 1991;84:2318-2324. Kuch K-H, Schluter M. Single-catheter approach to radiofre- quency current ablation of left-sided accessory pathways in patients with Wolff-Parkinson-White syndrome. Circulation
Chein WW, Cohen TI. Lee MA, et al. Electrophysiological findings and long-term follow-up of patients with the perma- nent form of junctional reciprocating tachycardia treated by catheter ablation. Circulation 1992;85: 1329- 1336. Warin JF, Haissaguerre M, Le Metayer P, et al. Catheter abla- tion of accessory pathways with a direct approach: Results in 35 patients. Circulation 1988;78:800-815. Deshpande S, Jazayeri MR. Bremner S, et al. Control of supra- ventricular tachycardia with transcatheter ablative technique using radio frequency as the energy source. Wis Med J 1993;
Jazayeri MR, Hempe SL, Sra JS, et al. Selective transcatheter ablation of the fast and slow pathway using radiofrequency energy in patients with atrioventricular nodal reentrant tachy- cardia. Circulation 1992;85: 1318-1328. Akhtar M, Jazayeri MR, Sra J, et al. Atrioventricular nodal reentry: Clinical, electrophysiological. and therapeutic consid- erations. Circulation 1993;88:282-295. Kay GN, Epstein AE, Dailey SM, et al. Selective radiofre- quency ablation of the slow pathway for the treatment of atrio- ventricular nodal reentrant tachycardia. Evidence for involve- ment of perinodal myocardium within the reentrant circuit. Circulation 1992;85:1675-1688. Lee MA, Morady F, Kadish A, et al. Catheter modification of the atrioventricular junction with radiofrequency energy for control of atrioventricular nodal reentry tachycardia. Circula- tion 1991;83:827-835. Walsh EP, Saul JP, Hulse E, et al. Transcatheter ablation of ectopic atrial tachycardia in young patients using radiofre- quency current. Circulation 1992;86:1138-I 146. Kay GN, Chong F. Epstein AE, et al. Radiofrequency ablation for treatment of primary atrial tachycardias. JACC 1993;21: 901-909. Gillette PC, Wampler DG. Garson A, et al. Treatment of atrial automatic tachycardia by ablation procedures. JACC 1985;6: 405-409. Kay GN. Epstein AE, Dailey SM, et al. Role of radiofrequency ablation in the management of supraventricular arrhythmias: Experience in 760 consecutive patients. J Cardiovasc Elec- trophysiol 1993;4(8):371-389. Tracy CM, Swartz JF, Fletcher RD, et al. Radiofrequency cath- eter ablation of ectopic atrial tachycardia using paced activa- tion sequence mapping. JACC 1993;2 l(4):9 10-91 7. Feld GK. Fleck P. Chen P, et al. Radiofrequency catheter abla- tion for the treatment of human type 1 atrial flutter: Identifica-
324:1605-1611.
1991 ;84:2366-2375.
92(9):507-5 17.
66 Journal of Interventional Cardiology Vol. 8, No. I , 1995

CATHETER ABLATION IN SUPRAVENTRICULAR TACHYARRHYTHMIAS
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
tion of a critical zone in the reentrant circuit by endocardial mapping techniques. Circulation 1992;86: 1233- 1240. Gillette PC, Garson A. Electrophysiologic and pharmacologic characteristics of automatic ectopic atrial tachycardia. Circula- tion 197756571-575. Goldreyer BN. Gallagher JJ, Damato AN. The electrophysio- logic demonstration of atrial ectopic tachycardia in man. Am Heart J 1973;85:205-215. Klein GJ, Bashore TM, Sellers TD, et al. Ventricular fibrilla- tion in the Wolff-Parkinson-White syndrome. N Engl J Med 1979;301: 1080. Avitall B, Khan M, Krum D, et al. Physics and engineering of transcatheter cardiac tissue ablation. JACC 1993;22:921-932. Gallagher JJ, Svenson RH. Kasell JH, et al. Catheter technique for closed-chest ablation of the atrioventricular conduction system. A therapeutic alternative for the treatment of refractory supraventricular tachycardia. N Engl J Med 1982;306:
Scheinman MM, Morady F, Hess DS, et al. Catheter induced ablation of the atrioventricular junction to control refractory supraventricular arrhythmias. J Am Med Assoc 1982;248: 851-855. Davies DW, Nathan AW. Camm AJ. Three sudden deaths after attempted high-energy catheter ablation of ventricular tachycardia. Br Heart J 1986;55:506-507. Haines D, Watson D, Verow A. Electrode radius predicts le- sion radius during radiofrequency energy heating. Validation of a proposed thermodynamic model. Circ Res 1990;67:
Calkins H, Sousa I, El-Atassi R, et al. Diagnosis and cure of the Wolff-Parkinson-White syndrome or paroxysmal supra- ventricular tachycardias during a single electrophysiologic test. N Engl J Med 1991;324:1612-1618. Swam JF, Tracy CM, Fletcher RC. Radiofrequency endocar- dial catheter ablation of accessory atrioventricular pathway atrial insertion sites. Circulation 1993;87:487-499. Langberg JJ, Chin MC, Rosenqvist M, et al. Catheter ablation of the atrioventricular junction with radiofrequency energy. Circulation 1989;80:1527-1535. Jackman WM, Wang X, Friday KJ. et al. Catheter ablation of atrioventricular junction using radiofrequency current in 17 patients: Comparison of standard and large-tip catheter elec- trodes. Circulation 1991;83: 1562-1576. Yeung-Lai-Wah JA, Alison JF, Lonergan L. et al. High success rate of atrioventricular node ablation with radiofrequency en- ergy. JACC 1991;18: 1753- 1758. Blanck Z, Dhala A. Krum D, et al. Dramatic reduction in ventricular response during atrial fibrillation by ablation the
194-200.
124- 129.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
atrioventricular nodal slow pathway: Electrophysiologic and clinical implications. (Abstract) Circulation 1993;88;4(2): 3 140. Klein GJ, Guiradon GM, Sharma AD, et al. Demonstration of macroreentry and feasibility of operative therapy in the com- mon type of atrial flutter. Am J Cardiol 198637587-591, Olshansky B, Okumura K, Henthorn R, et al. Atrial mapping of human atrial flutter demonstrates reentry in the right atrium. (Abstract) JACC 1988;7: 194A. Chauvin M, Brechenrnacher C. A clinical study of the applica- tion of endocardial fulguration in the treatment of recurrent atrial flutter. PACE 1989;12:219-224. Saoudi N, Atallah G. Kirkorian G, et al. Catheter ablation of the atrial myocardium in human type 1 atrial flutter. Circula- tion 1990;81:762-771, Calkins H, El-Atassi R, Kalbfleisch SJ, et al. Effect of operator experience on outcome of radiofrequency catheter ablation of accessory pathways. Am J Cardiol 1993;71:1104-1105. Calkins H, Niklason L, Sousa J, et al. Radiation exposure during radiofrequency catheter ablation of accessory atrioven- tricular connections. Circulation 1991;84:2376-2382. Lindsay BD, Eichling JO, Ambois HD, et aI. Radiation expo- sure to patients and medical personnel during radiofrequency catheter ablation for supraventricular tachycardia. Am J Car-
Coplen SE, Antman EM, Berlin JA, et al. Efficacy and safety of quinidine therapy for maintenance of sinus rhythm after cardioversion: A meta-analysis of randomized control trials. Circulation 1990;82:1106-1116. Creamer JE, Nathan AW, Camm AJ. The proanhythmic ef- fects of antianhythmic drugs. Am Heart J 1987;2:397-406. Menasche P, Leclercq JF, Cauchemez B, et al. Surgery for the Wolff-parkinsow White syndrome in 73 consecutive patients: What have we learned from intraoperative mapping? Eur J Cardiothorac Surg 1989;3:387-390. Bieze J. Regulatory watch: Radiation exposure risks haunt interventionalists. Diagn h a g 1993;8:68-79. de Buitleir M, Sousa J, El-Atassi R, et al. The reduction in medical care costs associated with radiofrequency catheter ab- lation of accessory pathways. Am J Cardiol 1990;66:189-192. Kalbfleisch SJ, Calkins H. Langberg JJ. et al. Comparison of the cost of radiofrequency catheter modification of the atrio- ventricular node and medical therapy for drug-refractory atrio- ventricular node reentrant tachycardia. JACC 1992;19: 1583- 1587. Survey of attendants of the EP Technologies RF Ablation Sem- inar preceding the Annual Meeting of the North American Society of Pacing and Electrophysiology. Chicago, Illinois 1992.
di01 1992;70:218-223.
Vol. 8, No. 1, 1995 Journal of Interventional Cardiology 67