Embed Size (px)
Citation preview

Cataract
By
Col Rana Intisarul Haq
MCPS, FCPS (AFIO)

Lens
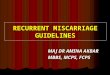
The lens is a biconvex structure located directly behind the posterior chamber and pupil It is the lesser of the two refractive elements in the dioptric system The equatorial diameter in adult is about 9-10 mm The anteroposterior width of the lens is about 6 mm The lens has certain unusual features. It lacks innervation and is avascular.

Detail view of the anatomy of the eye

cataract
DefinitionAny congenital or acquired opacity in the
lens capsule or substance of the lens , irrespective of the effects on vision is called cataract.

Classification of Cataract
According to Age
According to Morphology
According to Etiology
According to maturity
Congenital and acquired

6
Age Related Senile Cataract
Age related cataract is universal in persons over 70 years of age. Both sexes are involved equally.
There is considerable genetic influence.
Average age of onset of cataract is approximately 10 years earlier in tropical countries.

Age Related Cataracts senile
Presenile Cataracts
Diabetes Mellitus
Myotonic Dystrophy
Atopic Dermatitis
Neurofibromatosis-2
Traumatic Cataract
Direct Penetrating Injury
Concussion
Electric Shock & Lightening
Ionizing Radiation

Toxic Cataracts
Steroids
Chlorpromazine
Miotics
Busulphan
Amiodarone
Gold
Secondary Cataracts
Ch Ant Uveitis
Ac Congestive Glaucoma
High Myopia
Hereditary Fundus Dystrophy

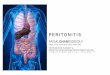
According to Morphology
Posterior Subcapsular Cataract
Ant Subcapsualr Cataract
Nuclear Cataract
Cortical Cataract
Mature Cataract

This diagram illustrates the different morphological characteristics of cataract together with their depth and location within the lens. The following illustrations demonstrate clinical examples of these anatomical entities.
CATARACT
THE LENS

CLASSIFICATION ON BASIS OF MATURITY
IMMATURE CATARACT
MATURE
HYPERMATURE
MORGAGNIAN

Causes
Hereditary
Age
DM
Steroids
UV Rays
Poor Nutrition
Smoking

Epidemiology
Cataract surgery is the most commonly performed surgery in elderly patient
Any Age
Two peaks
<10 Years
>65 Years

Pathology
Depends on type of Cataract
Early Changes – tiny areas of liquefaction called morgagnian degeneration seen as cortical spokes
Progress to involve entire cortex
Later on homogeneous appearance

15
Etiopathogenesis of Cataract
Caused by degeneration and opacification of existing lens fibres, formation of aberrant fibres or deposition of other material in their place.Loss of transparency occurs because of abnormalities of lens protein and consequent disorganization of the lens fibres

16
Etiopathogenesis of Cataract
Any factor that disturbs the critical intra and extra cellular equilibrium of water and electrolytes or deranges the colloid system within the fibres causing opacification.
Fibrous metaplasia of lens fibres occurs in complicated cataract.
Epithelial cell necrosis occurring in angle closure glaucoma leads to focal opacification of the lens epithelium (Glaucomflecken)

17
Etiopathogenesis of Cataract
Abnormal products of metabolism, drugs or metals can be deposited in storage diseases (Febry), metabolic diseases (Wilson) and toxic reactions (Siderosis)

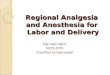
Nuclear Cataract

Mature Cataract

Hypermature Cataract

Traumatic Cataract(Penetrating Trauma)

Vossius Ring

PSC in Atopic Dermatitis

Congenital Cataract

Stellate PSC in Myotonic Dystrophy

Shield Anterior Subcapsular Cataract
(Atopic Dermatitis)

PSC in Atopic Dermatitis

Progression of Steroid-induced Cataract

Anterior Subcapsular Opacities (Ch Ant Uveitis)

Adv Cataract & Posterior Synechiae
(Ch Ant Uveitis)

31
Symptoms of Cataract
1. Blurring of vision2. Frequent change of glasses due to rapid
change in refractive index of the lens 3. Painless, progressive, gradual diminution
of vision due to reduction in transparency of the lens
4. Second sight or myopic shift in case of nuclear cataract causing index myopia, improving near vision.

32
Symptoms of Cataract
5. Loss or marked diminution of vision in bright sunlight or bright light beam in central posterior sub-capsular cataract.
6. Monocular diplopia or polyopia in presence of cortical spoke opacities
7. Glare in posterior sub-capsular cortical cataract due to increased scattering of light

33
Symptoms of Cataract
8. Colored haloes around the light as seen in cortical cataract due to irregular refractive index in different parts of the lens.
9. Color shift , reds are accentuated
10. Visual field loss, generalized reduction in sensitivity due to loss of transparency

34
Signs of senile cataract
Positive findings
1. Diminution of vision
2. Anterior chamber is shallow in cases of intumescent cataract and deep in cases of hypermature (shrunken) cataract
3. Tremulousness of iris in cases of hypermature shrunken cataract

35
Signs of senile cataract
4. Lenticular opacity , grey or white opacity in lens. Iris shadow in immature cataract. No iris shadow in mature cataract
5. Morgagnian Cataract- is characterized by liquefied cortex, which is milky and nucleus is seen as brown mass, seen as semicircular line, altering its position with change in position of head

36
Signs of senile cataract
6. Distant direct ophthalmoscopy will reveal black shadow against red background in cases of immature cataract.

Thank you

Management of Cataract

HISTORYAge of Onset
Decreased Vision Painless, effecting daily routine? If the patient is bothered
about his decreased vision. Trauma
Any Ophthalmological Problems
Drugs Intake
Exposure to Radiations
Systemic Diseases Skin disease, joint pains, etc.
Family History

Examination GPE
SYSTEMIC EXAMINATION
OCULAR EXAMINATIONVISUAL ACUITYADNEXACORNEAANTERIOR CHAMBERPUPILVITROUSRETINA

Investigations
Blood Glucose
ECG
Chest x-rays (PA view)
Blood Complete Picture
Any specific relevant investigation (if indicated)

Indication for Surgery
Visual Improvement When the patient is bothered.
Medical IndicationsWhen cataract is adversely affecting the
health of the eye e.g.:Phacolytic Glaucoma Intumescent CataractDiabetic Retinopathy
Cosmetic IndicationsTo restore black pupil

Optimal Post Op Refraction
If monocular correction is reqd. e.g.
in contralateral dense or amblyopia
best post op refraction is -1DS.
If binocular correction is reqd
difference between the two eyes should not be more than 3DS.

SURGICAL TECHNIQUES
ICCE
ECCE
ECCE with posterior chamber IOL implant
Phacoemulcification

ECCE

IOL Implantation

Phacoemulcification

Operative Complications Complications of Local AnaesthesiaRetrobulbar HemorrhagePerforation of the globe, optic nerve
or sheath
Operative Complications:Bridle Suture Perforation of the globeStripping of Descemet’s MembraneDamage to ciliary body

Operative Complications(Contd)
Rupture of the Posterior CapsuleCapsular Rupture without Vitreous Loss
Small TearLarge Tear or Zonular Tear
Capsular Rupture with Vitreous Lossvitrectomy
Posterior Loss of Lens FragmentsSmall FragmentsLarge Fragments

Nuclear Material in Vitreous

Operative Complications(Contd)
Suprachoroidal HemorrhageSource
long or short ciliary arteryContributing Factors
sudden in IOPcoughing Valsalva ManoeuvreVitreous LossSudden rise in B.P.Retrobulbar anaesthetic without adrenaline

Operative Complications(Contd)
Suprachoroidal Hemorrhage(Contd)Presentation
after lens delivery, progressive shallowing of anterior chamber, increased IOP & iris prolapse, vitreous extrusion, loss of red reflex. In severe cases all intraocular contents may be extruded
Immediate TreatmentClosure of the IncisionAdministration of Hyperosmotic Agent

Operative Complications(Contd)
Suprachoroidal Hemorrhage(Contd)Subsequent Treatment
Topical & Systemic SteroidsBetween 7 & 14 Day drainage of the blood,
pars plana vitrectomy & air-fluid exchange

Early Post-Operative Complications
Iris Prolapse Cause - inadequate
suturing Complications -
defective wound healing, ch ant uveitis, epithelial ingrowth, cystoid macular edema, excessive astigmatism.
Treatment

Early Post-Operative Complications
Striate KeratopathyCause - damage to
corneal endothelium
Hyphema

Early Post-Operative Complications
Acute Bacterial EndophthalmitisPathogenesis
Causative Organisms Staph Epidermidis, Staph Aureus, Pseudomonas sp etc
Source of InfectionPrevention
Treatment of local infections of the Patients Preoperative instillation of Povidine-iodine Meticulous draping Technique Postoperative injection

Draping of Eyes

Early Post-Operative Complications
Acute Bacterial Endophthalmitis(contd)Clinical Features
severityTime Interval
Staph Aureus - 1st to 3rd day Staph Epidermidis - 4rth to 10th day
Differential Diagnosis Retained Lens Matter Toxic Reaction Difficult or Prolonged surgery

Fibrinous Exudation in Severe Acute Endophthalmitis

Small Hypopyon

Acute Bacterial Endophthalmitis(contd)Clinical Features
Differential Diagnosis Retained Lens Matter Toxic Reaction Difficult or Prolonged surgery

Early Post-Operative Complications
Acute Bacterial Endophthalmitis(contd) Management
Identification of causative organism aqueous samples vitreous samples
Antibiotics Vitrectomy Steroids Subsequent therapy

Late Post-Operative Complications
Opacification of the Posterior Capsule Types
Elschnig’s Pearls Capsular Fibrosis
Indications for Treatment Visual Acuity Impaired Visualization of Fundus Monocular Diplopia or severe glare
Nd:YAG Laser Capsulotomy Complications

Elschnig Pearls

Fibrosis of Posterior Capsule

Technique of Nd:YAG Laser capsulotomy

Late Post-Operative Complications
Malposition of IOL Tilting Decentration Treatment
Corneal Decompensation Causes Treatment

Late Post-Operative Complications
Retinal Detachment Risk Factors
Disruption of Posterior Capsule
Vitreous Loss Lattice Degeneration
Sunset Syndrome Cause Traetment

Late Post-Operative Complications
Chronic Endophthalmitis Causative Organism
Propionibacterium Acnes Staph Epidermidis
Clinical Features Treatment Strategy
steroids & antibiotics Removal of IOL,
remaining cortex
& entire capsular bag