Embed Size (px)
Citation preview

Postgrad. med. J. (October 1967) 43, 647-655.
Casualty fractures
GORDON HADFIELDF.R.C.S.
Consultant Orthopaedic Surgeon to St Peter's Hospital, Chertsey,and Rowley Bristow Orthopaedic Hospital, Pyrford
PrinciplesFor the purpose of this article casualty frac-
tures are defined as those which may be treatedtotally in the Accident Department, or treatedthere initially and then referred to a fractureclinic. The exact definition varies with differenthospitals and the seniority of the casualty officer.The casualty officer generally has not the know-ledge or experience to treat many fractures, andif he is in doubt should not hesitate to call in theorthopaedic surgeon.
HistoryWith any fracture the history is important; the
patient may often not be able to give an exacthistory of the injury, but slight trauma makes onesuspect a pathological fracture. The nature anddirection of the force may indicate that a limb
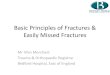
with an apparently simple fracture has sustainedsevere damage to the soft tissues, which maynecrose later. The age of the patient has a bearingon the fracture sustained; similar injuries indifferent age groups may cause different fractures(Fig. 1).
ExaminationA patient with a suspected fracture should be
examined carefully but thoroughly. If handledgently the patient will gain confidence and allowa much more thorough examination. Skin damage,swelling and deformity are all looked for beforethe patient is touched. Note the exact site oftenderness, to be later correlated with the X-rayexamination; both sensation and the pulses distalto the fracture are examined. Movement at thefracture must not be attempted as the elicitation
FIG. 1. Fracture separation of the radial epiphysis (adolescent), fractured scaphoid (young adult) and Colles' fracture(elderly). The same causal force, but the patient's age determines the fracture.
copyright. on M
ay 7, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.43.504.647 on 1 O
ctober 1967. Dow
nloaded from

Gordon Hadfield
of crepitus is an uncivilized method of diagnosis,but the patient is asked to move the limb distal tothe fracture to determine any muscle or tendondamage.
X-rayThe final diagnosis of a fracture is made on the
X-ray. Any suspect limb must be X-rayed. Filmsmust be taken in at least two planes and cover awide enough area. Remember the pitfalls ofX-rays: (1) The fracture may not show up on theoriginal film, only later, as with many scaphoidfractures. (2) Where a forearm fracture is sus-pected both upper and lower radio-ulnar jointsmust be included to make sure there is no disloca-tion of either joint. (3) If you are not sure ofepiphyses in children X-ray the other limb forcomparison.When looking at the X-rays you should try to
correlate any tender point and examine this partof the bone carefully. Remember that the casualtyofficer has an advantage over the radiologist, ashe sees both patient and X-ray. Even so, it isimportant that some system exists in the depart-ment to connect X-ray reports with casualtyrecord cards so that any 'missed' fracture may be'discovered' and the patient treated.
Description of the fractureIt is important for the casualty officer to des-
cribe a fracture accurately: the situation in thebone, whether the fracture is transverse, spiral oroblique, and the displacement of the distal frag-ment relative to the proximal fragment. Accuratedescription means sound advice on the telephone.
TREATMENT-Introductory remarksImmobilization does not make fractures unite,
and not every fractured bone requires treatment,but every fractured limb requires some sort oftreatment even if only reassurance of the patient.A fracture is reduced, splinted in the reduced posi-tion until consolidated, and the soft tissues treated.An undisplaced fracture obviously does notrequire reduction, but may need splinting to pre-vent displacement. If it is impossible to holdreduction, as with a fractured os calcis, then it isfutile to reduce it. If it is impossible to reduce afracture then holding it in the unreduced positionin plaster is only perpetuating malunion andencouraging stiffness. There is, however, softtissue damage which must be treated, and treatedearly before oedema coagulates and soft tissues'consolidate', causing permanent pain and stiff-ness. This method of fracture treatment may becalled supervised neglect, in that the fractured
bone is not treated but the soft tissues are; itshould not be taken to mean neglect of the limbas a whole.
ReductionA fracture may be reduced by traction, mani-
pulation or operation. Manipulation is a scientificprocess reversing the causal force of the fracture,done under an adequate anaesthetic, not a smashand grab raid under anoxia.
Holding reductionThis may be by continuous traction, plaster of
Paris or operation. In Casualty fractures tractionapplies only to the upper limb. The uses and mis-uses of plaster will be discussed later. How long afracture requires to be held varies, but splintageshould not be removed until consolidation hasoccurred. This must be confirmed clinically andradiologically. A useful guide is that a spiral frac-ture in the upper limb takes 6 weeks to con-solidate. A fracture in the lower limb takes twiceas long, and with a transverse fracture the time isalso doubled because of the smaller area of con-tact. A child will need half as long as an adult(Table 1).
TABLE 1
The expected time for fracture consolidation
Upper limb Lower limb
Spiral 6 weeks 12 weeksTransverse 12 weeks 24 weeks
Soft tissuesThe tissues around a fractured bone are swollen
and oedematous; to prevent the oedema fluidcausing adhesions and stiffness it must be elimin-ated before it solidifies. To get rid of fluid eleva-tion helps; bandaging resists further fluid, butonly activity can pump it away. Compressionbandaging is with a crepe or Bisgaarde bandage.Elastic adhesive bandages should never be used;as the oedema varies, so does the size of the limb,and any bandage should be reapplied as soon as itfails to give the necessary support to the limb. Ifan adhesive bandage is used changing it causesunnecessary suffering to the patient. All unsplintedjoints should be actively exercised.
Plaster of ParisAny plaster used to splint a fracture must be
adequate to prevent displacement without splint-ing joints unnecessarily. Before applying anyplaster one should consider: (1) Is it needed at
648
copyright. on M
ay 7, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.43.504.647 on 1 O
ctober 1967. Dow
nloaded from

Casualty fractures
all? (2) Is it effective? (3) Is it too extensive?Often in the upper limb a plaster slab is adequateto maintain reduction.No plaster applied to a recent fracture should
be complete, but should be padded and split insuch a way that when the limb inside swells theplaster does not act as a constricting force. Whenthe initial swelling has settled the plaster may becompleted or replaced with safety.Any patient sent away from hospital with a
plaster on must be warned of the symptoms, signsand dangers of general or local pressure. Generalpressure, from too tight a plaster, will cause painin the limb, with pins and needles and later numb-ness in the fingers or toes. The patient may alsonotice that the extremities have become blue andswollen. He should be told that if this happens thelimb should be elevated, and if the symptoms donot subside in 1 hr he should return to hospital.The patient with localized pressure feels painunder the plaster at one point, usually over a bonyprominence. This is because the skin is beingcompressed between the bone and the plaster. Thepain will persist until pressure necrosis of thenerve endings in the skin has occurred, after whichlittle or no pain is experienced. It is important inthese patients to relieve the pressure as soon aspossible, either by elevating an edge of the plasteror by cutting a window over the painful point. Ifthis is neglected a pressure sore will result.
The use of the Physiotherapy DepartmentThe physiotherapist can play a very useful role
in the treatment of fractures if the patient isreferred early enough. She can encourage activemovements of an injured limb and therebyeliminate stiffening oedema, and she is also trainedto teach patients how to use crutches. Any patientsent home with crutches, i.e. almost all leginjuries, should be referred to the PhysiotherapyDepartment to be shown how to use them (Fig. 2).
TREATMENT-Individual fractures commonlytreated in CasualtyClavicle
This is usually fractured by a fall on the pointof the shoulder or the outstretched arm. Union isnever a problem but malunion is almost invariable.Reduction can be attempted by bracing theshoulders back and held with a figure-of-eightbandage. This causes axillary discomfort, and thebandage rarely stays tight for more than 10 min.It is adequate to support the arm in a sling forcomfort for a few days and encourage early move-ment of the shoulder. Sporting activities are for-bidden for 6 weeks.
FIG. 2. Use the physiotherapist.
ScapulaThe body of the scapula may be fractured by a
direct injury, or the glenoid neck by a fall on thepoint of the shoulder. In neither case is reductionnecessary or possible, excessive movement of thefracture being prevented by the surroundingmuscles; the best treatment is a sling for comfortand early mobilization of the shoulder joint.
Neck of humerusAdults fracture through the surgical neck; in
children fracture-separation of the epiphysisoccurs. These fractures follow a direct injury or afall on the hand, usually with the arm abducted.The fracture is often impacted and may be misseduntil the bruise appears. Even with gross displace-ment spontaneous reduction will follow by sup-porting the wrist in a sling, the weight of the armexerting traction. This traction also maintainsreduction. The sling is retained for up to 6 weeksdepending on the discomfort present. Gravity-assisted shoulder exercises (Fig. 3) are startedimmediately to prevent shoulder stiffness, butexercises with the giant wheel, beloved of old-fashioned physiotherapists, only achieve passivemovement and are, therefore, forbidden.
If there is an associated nerve lesion or disloca-tion refer the patient to the Orthopaedic Depart-ment. The only other complication is shoulderstiffness which is prevented by activity.
649
copyright. on M
ay 7, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.43.504.647 on 1 O
ctober 1967. Dow
nloaded from

Gordon Hadfield
FIG. 3. Gravity assisted exercises. Routine treatmentfor most shoulder injuries.
Greater tuberosityThis is due to a direct injury or to avulsion from
resisted action of the supraspinatus tendon. Thepatient is unable to initiate abduction of theshoulder, and the arm should be supported in asling for comfort. Early gravity exercises areneeded to prevent long-standing stiffness of theshoulder.Shaft of humerusA direct injury causes a transverse fracture and
an indirect injury a spiral fracture. Remember toexamine the radial nerve before you start treat-ment. You need not reduce the fracture, gravitywill do it for you. Accurate reduction is unneces-sary, only correct general alignment. A wrist slingallows gravity to reduce the fracture, and with themuscles surrounding the humerus further splintageis not needed. Occasionally the arm feels veryunstable and the patient feels more confident witha plaster U-slab from the axilla, under the flexedelbow and up the outer side of the arm to thepoint of the shoulder. This is held on with a crepebandage. At 3 weeks the fracture is united and thepatient may wear the sling outside his clothesinstead of inside; at 6 weeks it is consolidated, thesling being discarded at this time. Gravity exer-cises of the shoulder and gentle active movementsof the elbow are started early.
Supracondylar fracture of the humerusThis child's fracture is caused by a fall on the
hand with the elbow flexed. The state of the radialpulse and the nerves must also be assessed at the
clinical examination, as these may be damaged bythe sharp distal end of the proximal fragment.
If there is displacement the fracture must bereduced under general anaesthetic. The least dis-placement, that of backward tilt, can be correctedby flexion of the elbow, but where contact is lostbetween the bone ends the manipulation must besystematic. In the Apley method the oppositehumeral shaft is grasped firmly and the shoulderexternally rotated, the relationship of the epicon-dyle and forearm being noted. The affectedhumerus is then fully externally rotated, and afterreduction of the lateral displacement of the distalfragment the epicondyles and forearm are placedin the correct rotation. If the rotation deformityis not corrected an ugly varus deformity follows.Traction is applied to the forearm with the elbowslightly flexed, and the lower end of the humerusis pulled onto the upper. The elbow is then flexedas far as it will go without obliterating the radialpulse. Provided the fracture has been reduced, thisbeing confirmed by X-ray, and the elbow heldflexed, the stretched triceps splints the fracture.Reduction is held with a collar and cuff sling inthe flexed position; as swelling subsides the collarand cuff is tightened daily maintaining full flexionbut still ensuring the pulse is palpable. The arm iskept inside the vest and the collar and cuff neverremoved (Fig. 4). The use of plaster is an admis-sion of failure of reduction. Repeated plasterchange as flexion is increased is liable to causedisplacement of the fracture. Discomfort due tosweating in the axilla and elbow flexure is pre-vented by blowing powder into these sites.
FIG. 4. Collar and cuff. Three weeks inside the clothesand 3 weeks outside is routine treatment for most elbowinjuries.
650
copyright. on M
ay 7, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.43.504.647 on 1 O
ctober 1967. Dow
nloaded from

Casualty fractures
At 3 weeks the patient is allowed to have thecollar and cuff outside the clothes, only removingit for washing, dressing and eating. At all othertimes the collar and cuff is maintained in fullflexion. The child with a fractured elbow regainsfull movement unless a physiotherapist or anxiousparent tries to force the pace.
Failure to correct the rotation deformity willcause malunion. The serious complications aremyositis ossificans, which is increased by exercise,and the dreaded complication of Volkmann'sischaemia, of which excessive pain is the cardinalsymptom. A patient with any of these complica-tions should be referred to the Orthopaedic De-partment forthwith.
T- or Y-shaped fracture of the humerusThis is due to a fall on the point of the elbow.
The olecranon is driven as a wedge into the lowerhumerus and the condyles are split off. Closedreduction cannot be accurate and if the elbow isput in plaster permanent stiffness is inevitable.Operative reduction is no less unsuccessful. It isbest to make the patient reduce his own fractureassisted by gravity. A collar and cuff is applied,and early active elbow movement encouraged. Bythis means the lower humerus is moulded to a nearnormal shape by the bones with which it has toarticulate and a surprising range of movementresults.
Medial epicondyleThis is due to a valgus strain in children, and
may be associated with a dislocated elbow. Themedial epicondyle is pulled off and if, as occa-sionally happens, it is trapped in the joint or thereare ulnar nerve symptoms, operation is needed.When the epicondyle lies outside the joint and
there is no evidence of an ulnar nerve lesion allthat is required is a sling until the arm is comfort-able. The medial epicondyle is only for muscleattachment, and even with displacement will uniteby fibrous tissue which will give adequate originfor the wrist flexor muscles.
Lateral condyleThis is another childs' injury, caused by a
valgus strain of the elbow pushing off the lateralcondyle. It is very unstable, usually needs opera-tion, and is not really in the province of thecasualty officer.
CapitellumThis is the adult equivalent of the fractured
lateral condyle. The front half of the capitellumand part of the trochlea shear off vertically andthe fragment comes to lie in front of the lower
humerus. Manipulative reduction may be achievedby extending the elbow under general anaesthetic,and while putting a varus strain on the elbow thefragment is replaced by thumb pressure. If thissucceeds flexing the elbow fully holds reduction, acollar and cuff maintaining the flexed position. Ifclosed reduction fails open reduction is necessary.
Radial headA fall on the outstretched hand putting a valgus
strain on the elbow drives the head of the radiusonto the capitellum. The radial head may sustain:(1) a chisel fracture, which is simply a verticalcrack, (2) a marginal fracture where a segment isdisplaced, usually downwards, or (3) a com-minuted fracture.A patient with any of these fractures has a
haemarthrosis of the elbow which will require acollar and' cuff to rest it. Failure to do this leadsto stiffness. With a comminuted fracture excisionof the head may be necessary, and the decisionshould be made by the orthopaedic surgeon. Thecollar and cuff sling is maintained with the elbowfully flexed, as it is flexion which is difficult toregain after an elbow injury. After 3 weeks theelbow is allowed out of the sling for meals, wash-ing and dressing, and at 6 weeks gentle use willallow extension to return.
Neck of radiusThis is the equivalent injury in a child, the head
of radius being tilted distally, forwards andlaterally. Rotation of the forearm is limited if thedeformity is left, and reduction can be achievedby pressing proximally, medially and backwardson the head. If the forearm is also rotated theorbicular ligament may assist reduction. Reductionis held by a collar and cuff for 6 weeks, 3 weeksinside the clothes and 3 weeks outside. If closedreduction fails open reduction must be done unlessthe deformity is slight.
OlecranonThis is due to a fall direct onto the elbow or a
fall on the hand with the elbow flexed, theolecranon being fractured by muscle pull. With adirect injury, the triceps expansion may be intactin spite of the stellate fracture. Such a fractureonly needs treatment of the soft tissues with restin a sling. If there is separation of the fragmentsand the triceps does not act on the forearm opera-tion is necessary. No patient is too old for opera-tion; the elderly patient may need to use crutcheswhich require good triceps action.
Fractures of the radial and ulnar shaftsA fracture of either the radius or ulna, or of
both bones together, may be caused by a direct
651
copyright. on M
ay 7, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.43.504.647 on 1 O
ctober 1967. Dow
nloaded from

Gordon Hadfieldinjury or a rotational force. Beware of the un-displaced fracture of one bone; almost certainlythere is dislocation of one of the radio-ulnar jointswhich requires expert treatment. All adult fore-arm fractures should be referred to the Ortho-paedic Department as perfection of reduction isessential, and is usually by open treatment.
In children, slight sideways shift or angulationwill eventually grow straight, so perfect reductionis not essential. Many of these fractures are green-stick in type with angulation deformity only, andreduction under anaesthetic is achieved by bend-ing the bones back to the straight position. Fre-quently a complete fracture of one of the bones isproduced; this is unimportant so long as contactis kept between the bone ends. If the fracture iscomplete and displaced a careful manipulationaimed at getting apposition of the bone ends isusually successful. Rotation of the forearm is im-portant. If the fracture is in the upper third theforearm should be supinated; in the middle thirdthe forearm is in the position of mid-rotation, andin the lower third the forearm is fully pronated.The reduced fracture is held in a split plaster fromabove the elbow to the metacarpal necks for 8weeks. Although according to the table a childonly needs 6 weeks for consolidation of an upperlimb fracture we know that as soon as a child isreleased from paster he will do all the things hecould not do in plaster, and is then liable torefracture. We are not worried by joint stiffness ina child and an extra 2 weeks in plaster safeguardsthe child from his own folly.
Coles' fractureThis is a transverse fracture of the lower end
of the radius 1 in. from the joint line and notinvolving the joint. The fragment is displaced andtilted backwards, displaced and tilted radially,the fracture is usually impacted and the ulnarstyloid fractured. It is caused by a supinationforce, and reduced under general anaesthetic bypronating the hand on the forearm, followed byflexing and ulnar-deviating the wrist. The fractureis held in this position with a plaster back-splintwhich extends from just below the elbow to themetacarpal necks. The back-slab is made so thatit almost encircles the limb, leaving a gap downthe front of the forearm. It is held on with a crepebandage which will give with any swelling, andnot with a wet cotton bandage which is guaranteedto shrink and may cause ischaemia. Any ringsshould be removed before or during the anaes-thetic. The patient should not go home until ableto raise the arm and touch the opposite ear. Thisdemonstrates to her that although the limb isinjured it can be used. Shoulder, elbow and finger
movements are encouraged, and a sling shouldonly be used for 24 hr. The day after manipula-tion the patient is reviewed and movements againencouraged. One week later a check X-ray istaken; if the fracture has slipped to an unaccept-able position manipulation under anaesthetic isrepeated. The plaster is removed after 6 weeks, anX-ray taken to confirm union and a crepe bandageapplied. This is kept on for a further 2 weeksexcept for washing, and the patient told to usethe hand for light duties. If there is any doubtabout shoulder or finger movements refer thepatient to a physiotherapist.The commonest complications of Colles' frac-
ture are slight malunion, which is almost invariablebut not significant, shoulder or finger stiffnesswhich should be prevented by early movement,and persistent pain on the ulnar side of the wristdue to the fractured ulnar styloid; this usuallysettles as the wrist movement returns.
Other lower radial fracturesFracture separation of the radial epiphysis is
the child's version of a Colles' fracture and istreated in the same way. Do not miss the slightdisplacement which may occur in these fracturesand which can cause quite marked limitation ofwrist movement if not reduced.A comminuted fracture may occur, and as it
involves the joint the plaster is removed at about4 weeks to try to get the joint moving a bit earlierthan in a Colles' fracture.The radial styloid may fracture, and again this
involves the joint surface. There is usually littledisplacement, and a crepe bandage is all that isrequired for comfort, joint movement beingencouraged from the start. Smith's fracture is anoblique fracture of the lower radius so that thefront of the joint surface is sheared off and thehand displaced forwards. It is usually very un-stable and is treated by internal fixation.
ScaphoidThe scaphoid fractures by a fall on the hand,
and causes pain on the radial side of the wrist.pain on forced dorsiflexion and weakness of grip.There is tenderness in the anatomical snuff box.If these signs are present treat the wrist as ascaphoid fracture regardless of the X-ray whichmay not reveal the fracture until 3 weeks later.Plaster is applied from below the elbow to themetacarpal necks, and including the proximalphalanx of the thumb. The wrist is dorsiflexed, thethumb opposed, and the plaster well moulded inthe palm but allowing full metacarpo-phalangealflexion of the fingers. If the original X-ray did notreveal the fracture the plaster is removed at 2
652
copyright. on M
ay 7, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.43.504.647 on 1 O
ctober 1967. Dow
nloaded from

Casualty fractures
weeks and the wrist X-rayed. Again, if the threesigns are present but the X-ray does not show afracture replace the plaster and re-X-ray at 3weeks. If no fracture is demonstrable the wrist isfreed. If there is a fracture the plaster is kept onfor a total time of 6 weeks and the wrist examined.There should be no tenderness in the snuff-box orweakness of grip, but there may be pain ondorsiflexion because the wrist is stiffish. X-ray atthis stage rarely shows union, but if there is notenderness or weakness it is reasonable to leave offthe plaster and apply a crepe bandage. The patientis advised not to do heavy work and is re-examined 3 weeks later. If there are then no signsof a fracture the patient is discharged. If at eitherof these examinations there are still the clinicalsigns of fracture the plaster is reapplied and thepatient referred to the orthopaedic surgeon.
TriquetralWhen there is tenderness on the dorsum of the
wrist and an X-ray shows a flake of bone off theback of the carpus this is usually called a chipfracture of the triquetrum. It does not requirereduction or splintage, but the patient may feelmore comfortable in a crepe bandage for about 2weeks.
MetacarpalsThe base of the first metacarpal may fracture
into the joint as a Bennett's fracture. This may betreated by abducting the thumb and holding it inplaster, or by operation and screwing or wiringthe fragments. A quicker and equally good resultmay be obtained by disregarding the fracture andtreating the soft tissues by a crepe bandage andearly active movement. Despite malunion thefunction of the thumb is as near normal as withany other method of treatment. The metacarpalshafts may fracture, but are supported by thesurrounding muscles and neighbouring meta-carpals; a crepe bandage and early movementgives the best functional result. Some malunion isinevitable but does not affect the function of thehand. The metacarpal necks may fracture andangulate forwards. The orthodox treatment is toreduce the fracture and hold it by flexing thefinger to 900 at the metacarpo-phalangeal joint.This frequently causes permanent or at least long-standing joint stiffness. If you look at any pro-fessional boxer's hands you will find malunitedmetacarpal neck fractures with excellent function.Go for early function and disregard the fracture.Whatever happens do not use plaster.
PhalangesThe phalanges may fracture transversely or
obliquely. Angulation may occur with the trans-
verse ones, but there is usually little displacementof the spiral fractures other than some overlap.With an angulated fracture it is reasonable to restthe finger on a splint in some flexion for 2 weeks,followed by splinting it to the neighbouring fingerwith a garter on the proximal and intermediatephalanges for a further 2 weeks. This will encour-age joint movement. All other phalangeal fracturesare treated with the garters from the start, andonly need 3 weeks' splintage.
The trunkThe only trunk fracture which can be con-
sidered a casualty fracture is a stable crush-fracture of a thoracic or lumbar vertebral body.Such an injury may be caused by a fall or a flexioninjury. -The criteria for stability are clinical andradiological: (1) no symptoms or signs of nerveinvolvement, (2) an intact interspinous ligamentdemonstrated by absence of widening of the intra-spinous space on the lateral X-ray, (3) no fractureof the vertebral facets, (4) no lateral shift of eitherthe spinous process or vertebral body, and (5) theanterior height of the vertebral body is not lessthan one-third of the posterior height. If all thesecriteria are satisfied without any doubt the fractureis disregarded and the patient treated by heat andspinal extension exercises to eliminate the haema-toma in the muscles. Although it is much better toadmit these patients for a few days to get themmobilized, if the hospital bed situation is veryacute they can be treated as out-patients.
Fractured patellaA direct injury may fracture the patella in a
stellate manner without disruption of the quad-riceps expansion. If the patient can lift his legstraight the extensor mechanism is intact. Thefracture needs neither reducing nor holding, butthe haemarthrosis of the knee is treated byaspiration if tense, and early active exercises. Aplaster back splint may be needed to give supportto the knee for about 10-14 days. Do not use thismethod of treatment unless you are sure there isno separation of the fracture.
Fractures of the tibial shaftAll tibial fractures, with or without fibular
fractures, are best treated by hospitalization asthey swell a lot, but in certain cases out-patienttreatment may be used initially if the bed statedemands it. A spiral fracture of the tibia in achild may require reduction by rotation, and isheld in a plaster from above the knee to themetatarsal necks. As the leg will swell the plastermust be padded and split, and crutches supplied.
653
copyright. on M
ay 7, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.43.504.647 on 1 O
ctober 1967. Dow
nloaded from

Gordon Hadfield
An undisplaced transverse fracture in an adult canbe treated in the same way. Early reference to thefracture clinic is essential, as the complications oftibial fractures are many.
Fractures of the fibula shaftA direct injury to the fibular shaft causes a
transverse or comminuted fracture. Make surethere is no associated ankle injury. The fracturerequires no reduction or splintage, but the softtissues are treated by a crepe bandage until theswelling subsides and active movements, withelevation when not walking.
Ankle fracturesThese are fractures of the mortice and displace-
ments of the talus. There are only two anklefractures which can be classified as Casualtyfractures, the external rotation type and theabduction type, and these are only Casualty frac-tures if the medial malleolus is intact. An externalrotation injury causes a spiral fracture of thelower end of the fibula, best seen on the lateralX-ray. An abduction injury causes a transversefracture of the fibula 2-3 in. from the tip of thelateral malleolus. Except for the undisplacedexternal-rotation type of injury these fracturesrequire reduction, and this is carried out byreversing the causal force which can be ascer-tained from the fracture pattern on X-ray. Thereduction is done under a full general anaestheticwith relaxation, and less than perfect is unaccept-able. The external rotation fracture is reduced byinternally rotating the foot, the abduction fractureby adducting the foot. The reduction is held by asplit below-knee plaster from just below the kneeto the necks of the metatarsals. It is wrong tosplint the toes. The ankle is held at a right anglewith the foot neither varus nor valgus, any devia-tion from this position causing stiffness andnecessitating prolonged physiotherapy. When theswelling has subsided the plaster is changed,usually under general anaesthetic with X-raycontrol. The plaster is retained for 6 weeks for anexternal rotation injury and twelve for the abduc-tion injury.The soft tissues are treated by elevating the leg
when not actually walking, and exercising the toesand knee. When the definitive plaster has beenapplied a plaster overboot with a rockered sole isused and the patient is taught to walk normally(Fig. 5). By using the toes when walking he will'milk away' the oedema. After removal of theplaster a crepe bandage is used, again from toes tobelow knee, until there is no swelling.
FIG. 5. A leg plaster prevents ankle movement. Therockered overboot replaces this movement and allowsa normal heel-toe gait.
Fracture-separation of the lower tibial epiphysisis not really an ankle fracture but is treated in asimilar way. The fracture is reduced by reversingthe causal force of the injury, as shown by thedisplacement on X-ray, and held in a plaster for6 weeks.
Fractured calcaneumA fall on the heel may crush the calcaneum.
This bone is essentially an egg-shell containingstale bread crumbs, and even if reduction is pos-sible, however long it is held it will redisplace onweight bearing. The functional treatment is todisregard the fracture and treat the gross swellingby elevation, firm elastic bandaging and exercises.The maximum displacement takes place at thetime of impact, so ordinary weight bearing willnot displace it further. Weight bearing is allowedas soon as the patient feels able to put his foot onthe ground. Permanent sub-talar stiffness may pre-vent the patient returning to his usual occupationin the building or window-cleaning trades.
Metatarsal fracturesThese are caused by dropping a weight on the
foot, or the fifth metatarsal base may be pulled offby an inversion injury. Like the metacarpals, thesefractures are splinted by their neighbours. Mal-union is invariable, but so is good function unlessthe fractures are splinted externally. The fracturesare not treated but the soft tissues must bevigorously treated by firm bandaging, elevationand active exercises. Crutches are required initiallyas the foot will be painful for weight bearing, butthey should be discarded within a few days.
654
copyright. on M
ay 7, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.43.504.647 on 1 O
ctober 1967. Dow
nloaded from

Casualty fractures
Toe fracturesThese painful injuries are notable for their
swelling; only movement and elevation caneliminate this. Splintage in a firm shoe and normalwalking will produce the same malunion as plasteror collodion splints, without the stiffness.
Follow upAll patients with fractures treated in Casualty
and sent home must be seen the following day.At this review the patient is checked for pain,swelling and function. Activity should be en-couraged. A decision should now be made as tothe follow up. Most fractures will be referred to afracture clinic, but if it is decided to continuetreatment in the Casualty Department the fre-quency of attendance is determined by the type offracture.
The earliest possible return to work, even if onlylight work, must be the aim of treatment. If thefracture has rendered the patient incapable of hisown work for a long time the Disabled Registermay help. Do not let a patient stay away fromwork unnecessarily because of an impendinginsurance claim, and if the patient in your opinioncan reasonably work but will not for this reasonwrite this in your notes.With any Casualty fracture, if in doubt call for
more senior help.
For further readingAPLEY, A. GRAHAM (1963) A System of Orthopaedics and
Fractures, 2nd edn. Butterworths, London.PERKINS, G. (1958) Fractures and Dislocations. Athlone
Press, London.WATSON-JONES, R. (1955) Fractures andJoint Injuries, 4th edn.
Livingstone, Edinburgh.
655
copyright. on M
ay 7, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.43.504.647 on 1 O
ctober 1967. Dow
nloaded from