Embed Size (px)
Citation preview
Cast Care
OBJECTIVES:
After hours of classroom discussion, the Level 3 students will be able to:
1. define what cast is.
2. enumerate the purposes of having (a) cast/s.
3. identify the different types of cast materials and padding materials.
4. differentiate the different types of casts.
5. relate how complications arise when patient/s have casts.
6. compose appropriate and practical methods to counter complications that may arise when patient/s have casts.
Casts
A cast is an immobilizing device made up of layers of plaster or fiberglass (water-activated polyurethane resin) bandages molded to the body part that it encases.
Purposes:1. To immobilize and hold bone fragments in reduction2. To apply uniform compression of soft tissues
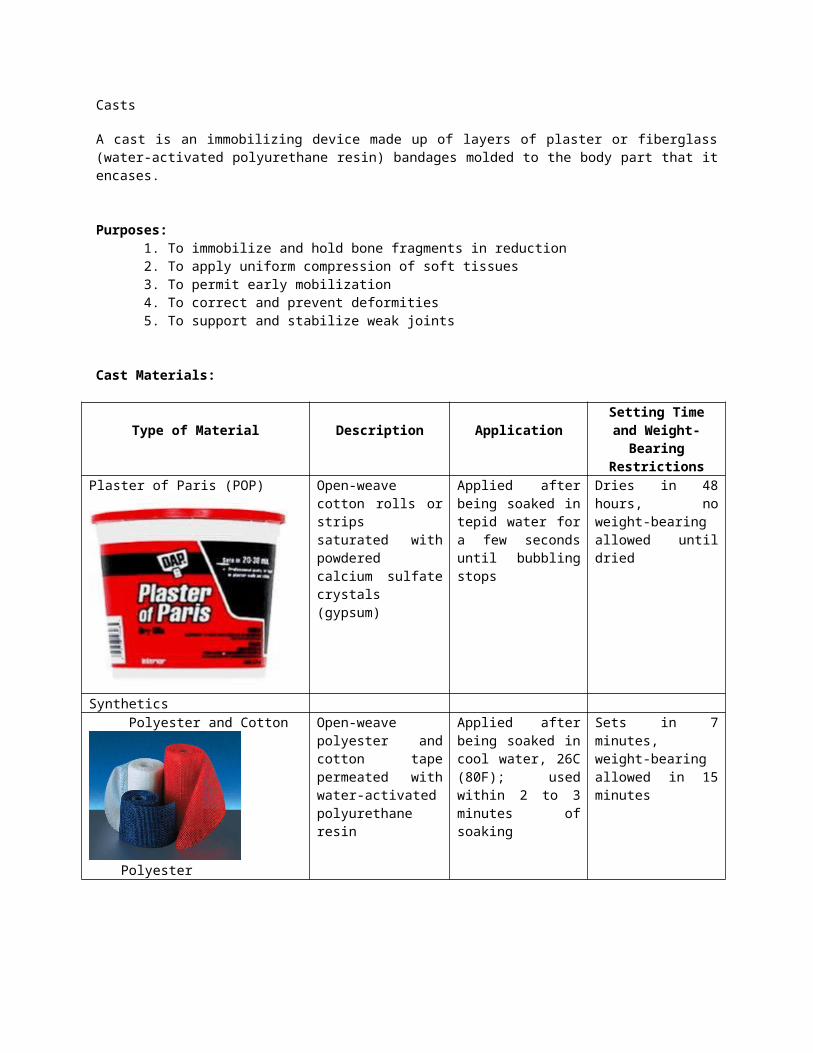
3. To permit early mobilization4. To correct and prevent deformities5. To support and stabilize weak joints
Cast Materials:
Type of Material Description ApplicationSetting Time and Weight-
Bearing Restrictions
Plaster of Paris (POP) Open-weave cotton rolls or strips saturated with powdered calcium sulfate crystals (gypsum)
Applied after being soaked in tepid water for a few seconds until bubbling stops
Dries in 48 hours, no weight-bearing allowed until dried
Synthetics Polyester and Cotton
Polyester
Cotton
Open-weave polyester and cotton tape permeated with water-activated polyurethane resin
Applied after being soaked in cool water, 26C (80F); used within 2 to 3 minutes of soaking
Sets in 7 minutes, weight-bearing allowed in 15 minutes
Fiberglassa. Water-activated
(Scotchcast, Deltalite)
Open-weave fiberglass tape impregnated with water-activated polyurethane resin (Scotchcast) or photosensitive polyurethane resin (Lightcast II)
Applied after being immersed in tepid water for 10 to 15 seconds (Scotchcast); applied with silicone type hand cream to keep it from sticking
Sets in 15 minutes, weight-bearing allowed in 30 minutes (Scotchcast); sets after being exposed for 3 minutes to a special ultraviolet
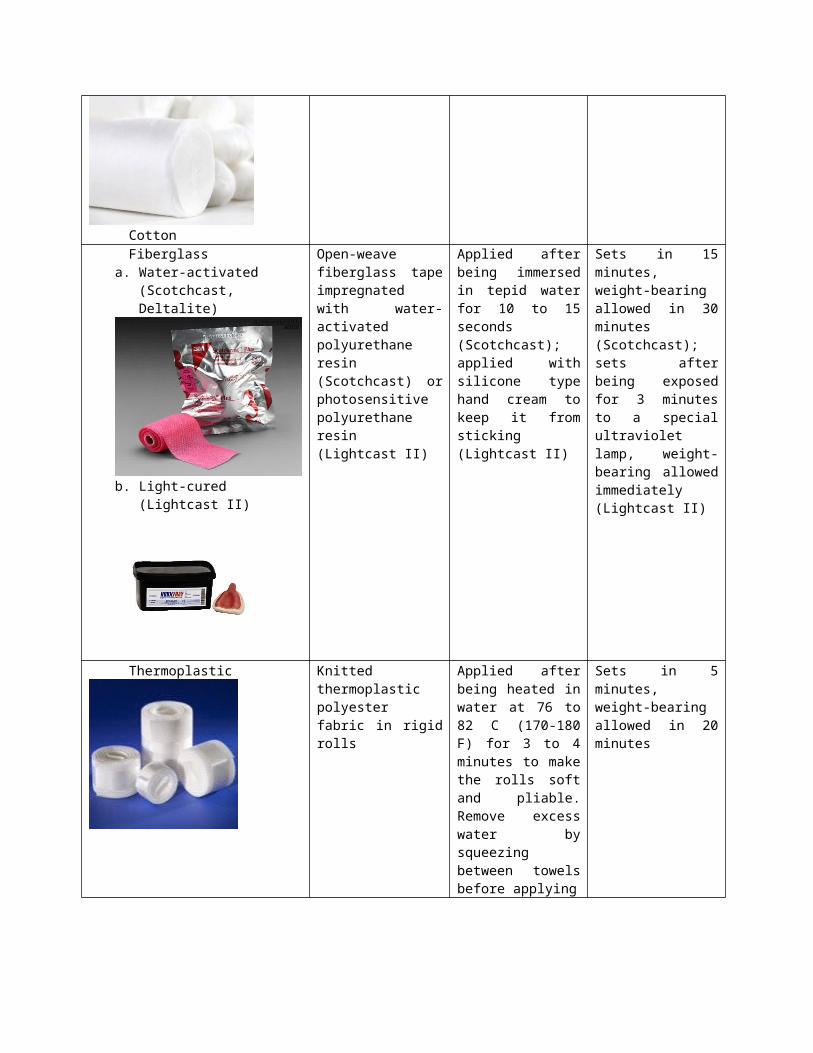
b. Light-cured (Lightcast II)
(Lightcast II) lamp, weight-bearing allowed immediately (Lightcast II)
Thermoplastic Knitted thermoplastic polyester fabric in rigid rolls
Applied after being heated in water at 76 to 82 C (170-180 F) for 3 to 4 minutes to make the rolls soft and pliable. Remove excess water by squeezing between towels before applying
Sets in 5 minutes, weight-bearing allowed in 20 minutes
Padding Materials:Before the plaster of Paris or synthetic casts are applied, the affected area must be
padded.
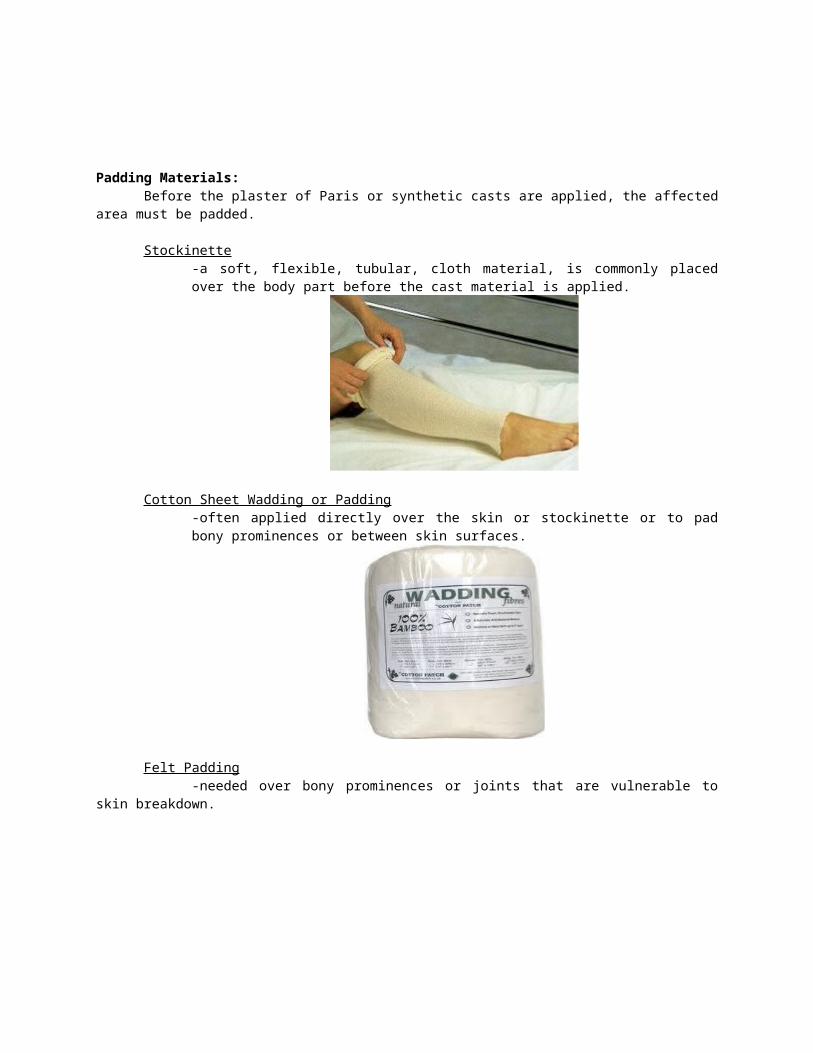
Stockinette-a soft, flexible, tubular, cloth material, is commonly placed over the body part before the cast material is applied.
Cotton Sheet Wadding or Padding-often applied directly over the skin or stockinette or to pad bony prominences or between skin surfaces.
Felt Padding-needed over bony prominences or joints that are vulnerable to skin
breakdown.
Plaster Splints-used to add strength over areas susceptible to breakage
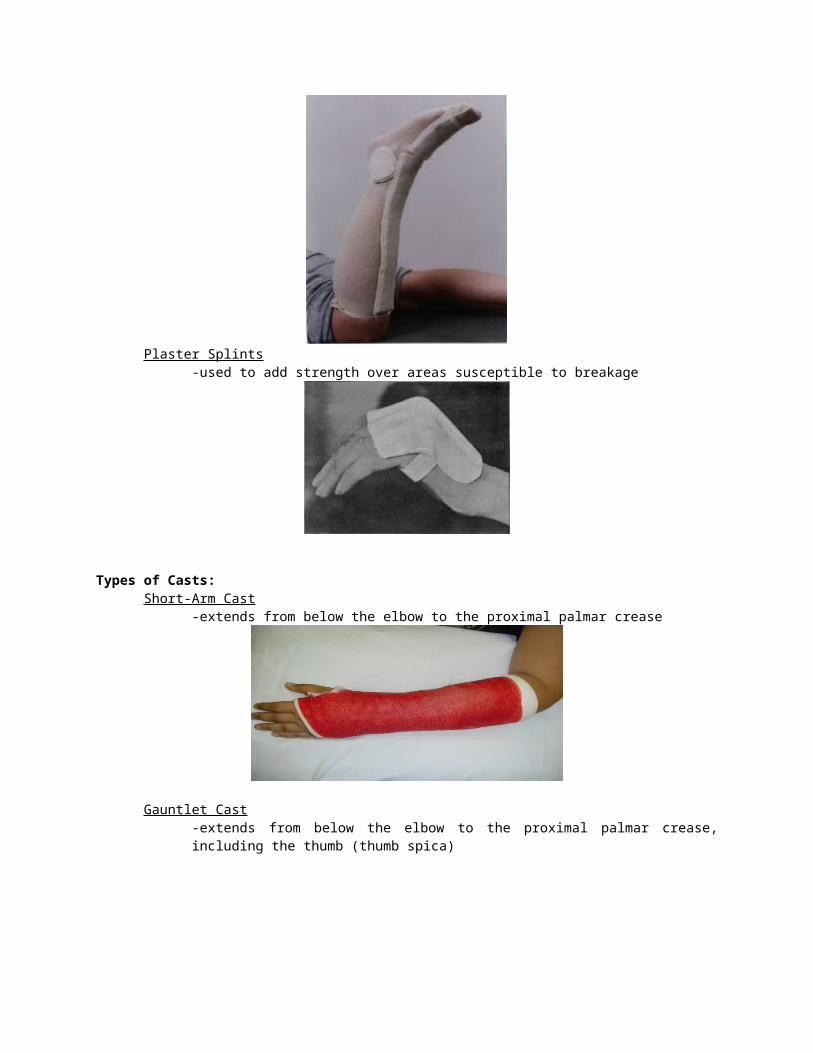
Types of Casts:Short-Arm Cast
-extends from below the elbow to the proximal palmar crease
Gauntlet Cast-extends from below the elbow to the proximal palmar crease, including the thumb (thumb spica)
Long-Arm Cast-extends form upper level of axillary fold to proximal palmar crease; elbow usually immobilized at right angle
Short-Leg Cast-extends from below knee to base of toes

Long-Leg Cast-extends from upper thigh to the base of toes; foot is at right angle in a
neutral position
Body Cast-encircles the trunk stabilizing the spine
Spica Cast-incorporates the trunk and extremity
1. Shoulder Spica Cast-a body jacket that encloses trunk, shoulder and elbow
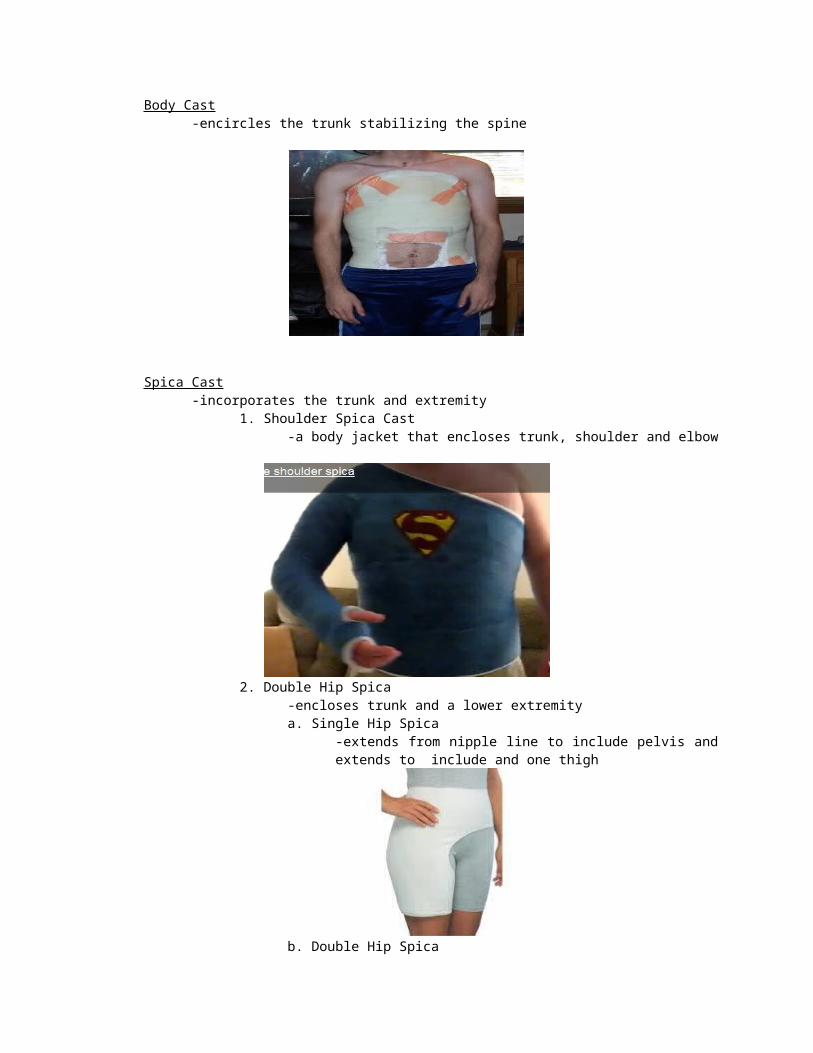
2. Double Hip Spica-encloses trunk and a lower extremitya. Single Hip Spica
-extends from nipple line to include pelvis and extends to include and one thigh
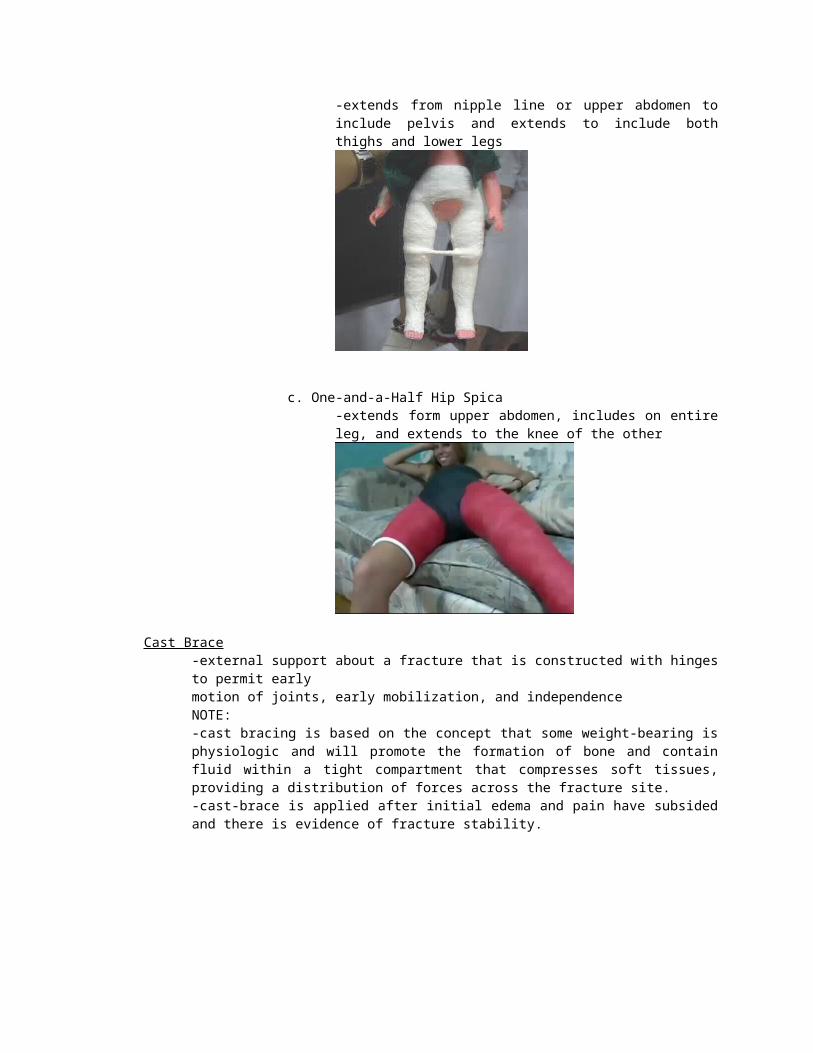
b. Double Hip Spica-extends from nipple line or upper abdomen to include pelvis and extends to include both thighs and lower legs
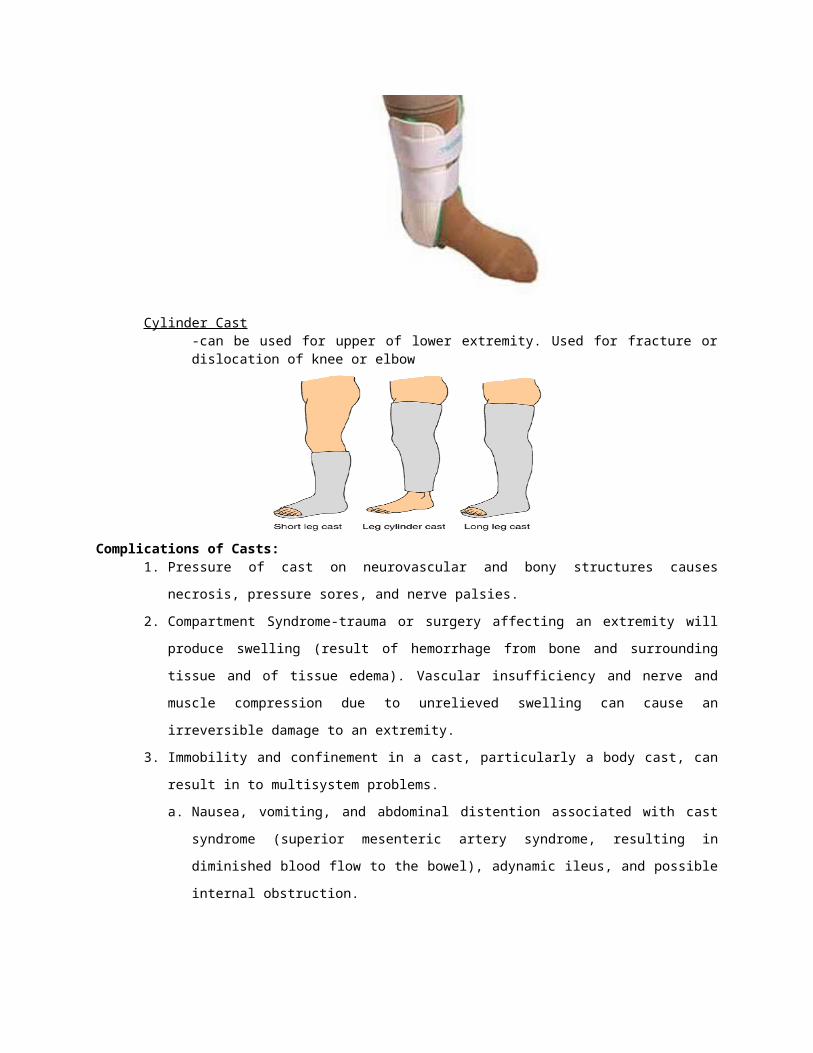
c. One-and-a-Half Hip Spica-extends form upper abdomen, includes on entire leg, and extends to the knee of the other
Cast Brace-external support about a fracture that is constructed with hinges to permit early motion of joints, early mobilization, and independenceNOTE:-cast bracing is based on the concept that some weight-bearing is physiologic and will promote the formation of bone and contain fluid within a tight compartment that compresses soft tissues, providing a distribution of forces across the fracture site.-cast-brace is applied after initial edema and pain have subsided and there is evidence of fracture stability.
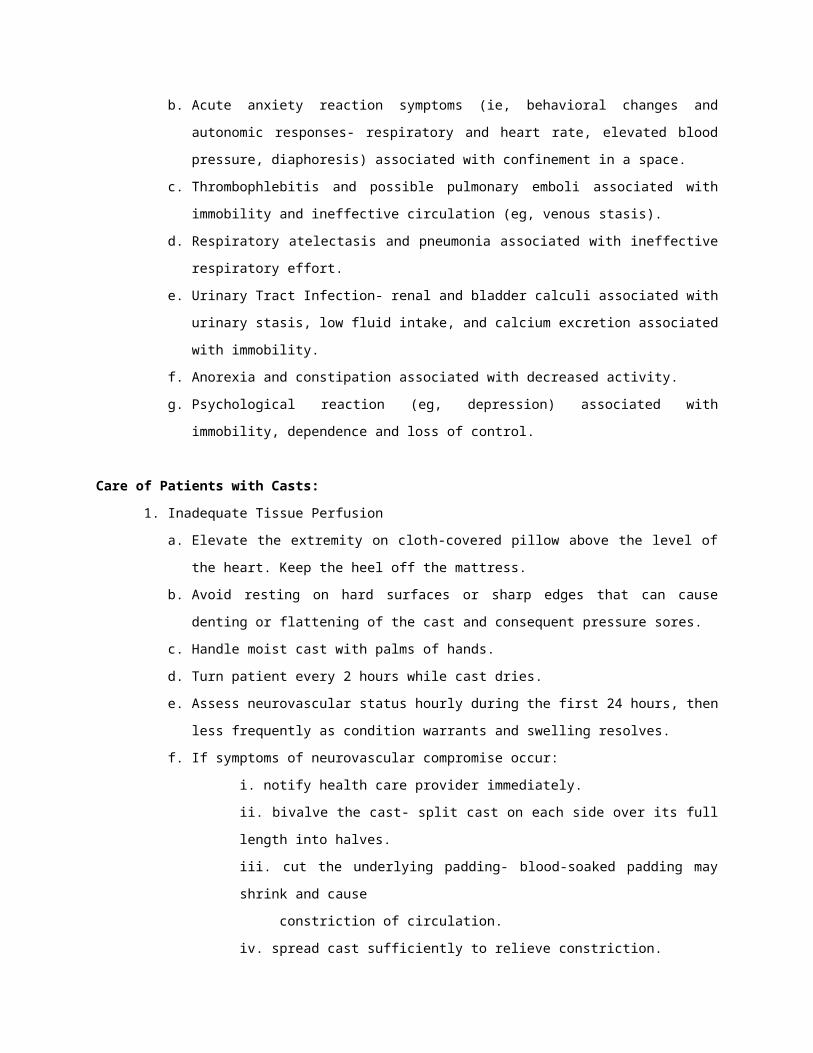
Cylinder Cast-can be used for upper of lower extremity. Used for fracture or dislocation of knee or elbow
Complications of Casts:1. Pressure of cast on neurovascular and bony structures causes necrosis, pressure
sores, and nerve palsies.
2. Compartment Syndrome-trauma or surgery affecting an extremity will produce swelling (result of hemorrhage from bone and surrounding tissue and of tissue edema). Vascular insufficiency and nerve and muscle compression due to unrelieved swelling can cause an irreversible damage to an extremity.
3. Immobility and confinement in a cast, particularly a body cast, can result in to multisystem problems.a. Nausea, vomiting, and abdominal distention associated with cast syndrome
(superior mesenteric artery syndrome, resulting in diminished blood flow to the bowel), adynamic ileus, and possible internal obstruction.
b. Acute anxiety reaction symptoms (ie, behavioral changes and autonomic responses- respiratory and heart rate, elevated blood pressure, diaphoresis) associated with confinement in a space.
c. Thrombophlebitis and possible pulmonary emboli associated with immobility and ineffective circulation (eg, venous stasis).
d. Respiratory atelectasis and pneumonia associated with ineffective respiratory effort.
e. Urinary Tract Infection- renal and bladder calculi associated with urinary stasis, low fluid intake, and calcium excretion associated with immobility.
f. Anorexia and constipation associated with decreased activity.g. Psychological reaction (eg, depression) associated with immobility,
dependence and loss of control.
Care of Patients with Casts:1. Inadequate Tissue Perfusion
a. Elevate the extremity on cloth-covered pillow above the level of the heart. Keep the heel off the mattress.
b. Avoid resting on hard surfaces or sharp edges that can cause denting or flattening of the cast and consequent pressure sores.
c. Handle moist cast with palms of hands.d. Turn patient every 2 hours while cast dries.e. Assess neurovascular status hourly during the first 24 hours, then less
frequently as condition warrants and swelling resolves.f. If symptoms of neurovascular compromise occur:
i. notify health care provider immediately.ii. bivalve the cast- split cast on each side over its full length into halves.
iii. cut the underlying padding- blood-soaked padding may shrink and cause constriction of circulation.iv. spread cast sufficiently to relieve constriction.
g. If symptoms of pressure area occur, cast may be “windowed” (hole cut in it) so the skin at the pain point can be examined and treated. The window must be replaced so the tissue does not swell and cause additional pressure problems at window edge.
2. Immobilitya. Encourage the patient to move about as normally as possible.b. Encourage compliance with prescribed exercises to avoid muscle atrophy and
loss of strength.i. active ROM for every joint that is not immobilized at regular and frequent intervals.ii. isometric exercises for the muscles of the casted extremity. Instruct patient to alternately contract and relax muscles without moving affected part.
c. Reposition and turn patient frequently.d. Avoid pressure behind knees, which reduces venous return and predisposes to
thromboembolism.e. Use antiembolism stockings as prescribed.f. Administer prophylactic anticoagulants as prescribed.g. Encourage deep breathing exercises and coughing at regular intervals to
prevent atelectasis and pneumonia.h. Observe for symptoms of cast syndrome- nausea, vomiting, abdominal
distention, abdominal pain, and decreased bowel sounds.i. Encourage patient to drink liberal quantities of fluid- to avoid urinar infection
and calculi secondary to immobility.
3. Patient in Spica or Body CastPOSITIONINGa. Place a bedboard under the mattress for uniform support of the body.b. Support the curves of the cast with cloth-covered flexible pillows- prevents
cracking and flat spots while cast is drying.i. place 3 pillows crosswise on bed for body cast.
ii. place one pilllw crosswise at the waist and two pillows lengthwise for affected leg for spica cast. If both legs are involved, use 2 additional pillows.
c. Encourage the patient to maintain physiological position by:i. using the overhead trapeze.ii. placing good foot flat on bed and pushing down while lifting himself or herself up on the trapeze.iii. avoiding twisting motions.iv. avoiding positions that produce pressure on groin, back, chest and abdomen.
TURNINGa. Move the patient to the side of the bed using a steady, even pulling motion.b. Place pillows along the other side of the bed- one for the chest and two
(lengthwise) for the legs.c. Instruct patient to place arms at side or above head.d. Turn the patient as a unit. Avoid twisting the patient in the cast.e. Turn the patient toward the leg not encase in plaster or toward the
unoperated side if both legs are in plaster.i. one nurse stands at other side of bed to receive the patient’s shoulder.ii. second nurse supports leg in plaster while the third nurse supports the patient’s back as he or she is turned.
f. Turn the patient in body cast to a prone position twice daily- provides postural drainage of bronchial tree; relieves pressure on back.
g. Keep the cast leel by elevating the lumbar sacral area with a small pillow when the head of the bed is elevated.
4. Hygienic Carea. Protect the cast form soiling.
i. cover perineum with a towel and apply spray (lacquer-type) to preineal area of cast. Tuck 10 cm strips of thin polyethylene sheeting under perineal area of cast and tape to cast exterior. Replace when soiling occurs.ii. clean outside of cast with dry cleanser on almost-dry cloth.
b. Roll the patient onto fracture bedpan; use small pillow in lumbosacral area for support.
5. Skin Carea. Inspect skin for signs of irritation:
i. around cast edge.ii. under cast- pull skin taut and inspect under cast, using a penlight for illumination.
b. Reach up under cast, and massage accessible skin.c. Protect the toes form the pressure of the bedding.
6. Additional CareDIETa. Assess the patient’s food preferences. Serve small meals.b. Provide natural bowel stimulants (eg. Fiber).c. Monitor bowels, and use a bowel program if necessary.
CAST SYNDROMEa. If symptoms of cast syndrome develop, report immediately.b. Place patient in prone position, if tolerated to relieve pressure symptoms.c. Use nasogastric suction as prescribed.d. Maintain electrolyte balance by intravenous replacement of fluids as
prescribed.e. Prepare the patient for removal of the cast or surgical relief of duodenal
obstruction if necessary.
7. Cast is Removeda. Instruct to cleanse skin with mild soap and water, blot dry, and apply
emollient lotion to dry skin.b. Warn against scratching the skin.c. Advise to continue prescribed exercises. Gradually resume activities, and
elevate extremity to control swelling.
CARE FOR PATIENT WITH TRACTION
TRACTION
-is a means by which a part of the body is immobilized.
-it involves a pulling force that is applied to a part of the body while a second force, called countertraction, pulls in the opposite direction.
-the pulling force of traction is provided through a system of pulleys, ropes, and weights attached to the client; countertraction is often achieved by elevating the foot or head of the bed and therefore is supplied by the client’s body.
Balanced Traction
-the amount of force in the traction is equal to the amount of force in the countertraction
Suspension
-is a mechanism that suspends a body part by using traction equipment, but it does not involve a pulling force.
Straight or Running Traction
-the traction force is pulled against the long axis of the body, and the countertraction is supplied by the client’s body.
PURPOSE OF TRACTION
1.to reduce and/or immobilize a bone fracture for healing
2.to maintain proper bone alignment
3.to prevent soft tissue injury
4.to correct, reduce, or prevent deformities
5.to decrease muscle spasm and pain
6.to treat inflammatory conditions by immobilizing a joint, e.g for arthritis or tuberculosis of a joint
TYPES OF TRACTION
1.Manual Traction
-is applied by the hands
-the nurse holds the limb while exerting pulling force.
-it is a temporary measure used while skin traction is prepared (e.g when a cast is being applied) or in an emergency (e.g when a traction rope breaks)
2.Skin Traction
-is a pulling force applied to the skin and soft tissues through the use of tape or traction straps and a system of ropes, pulleys and weights.
-the traction tape or strap is often made of vented foam rubber or cloth, and it may have either adhesive or nonadhesive backing
-adhesive skin traction is used only for continuous traction
-nonadhesive skin traction is used intermittently; it easily be removed and reapplied
-the tape is applied lengthwise along a limb and attached to a spreader bar, which is designed to spread the tape away from the bony prominences of the involved body part
-the bar must be wider than the involved part
3.Skeletal Traction
-is applied by inserting metal pins, wires or tongs directly into or through a bone. The metal device is then attached to a system of ropes, pulleys, and weight by means of a metal frame attached to the bed.
4.Encircling Traction
-a halter or sling is placed around a body part and attached by means of a rope and pulley to a weight that pulls in a straight line.
-examples are cervical head halter traction and pelvic traction
Traction can be either continuous or intermittent. Continuous traction (skeletal or skin) is applied and released by a physician, who is responsible for handling the
affected part when it is not in traction. Intermittent traction (nonadhesive skin traction) can be applied and released by nursing personnel with the appropriate order. However, the amount of weight to be applied is prescribed by the physician.
TRACTION EQUIPMENT
Overhead Frame-is attached to the hospital to the hospital bed and provides a means for attachment of the traction apparatus
-there are numerous kinds of overhead frames, which attach to the bed in different ways; each frame, however, has at least two upright bars (one at each of the bed), and one overhead bar.
Trapeze-attached to the overhead frame, the trapeze can be used by the client for moving in bed, unless contraindicated by the client’s health
Firm Mattress-to maintain body alignment and efficiency of the traction, a girm mattress is essential.
Ropes, pulleys, weight hangers and weights-for the halo-thoracic vest traction
GUIDELINES FOR TRACTION
All traction should have countertraction to prevent the client from being pulled by the force of traction against the pulleys or the bed, thus negating the traction.
To apply and maintain the correct amount of traction, all traction weights should not touch any part of the bed.
The traction force should follow an established line of pull. The line of pull determines the position and alignment of the body as prescribed by the physician. All ropes should be on the center track of a pulley, and the line of pull should always be from (a) the point of attachment to the client to (b) the first pulley.
Traction should always be applied while the client is in proper body alignment in a supine position
To be effective, traction should be maintained continuously unless ordered otherwise.
SKIN TRACTION
TYPES:
1. BUCK’S EXTENSION-is a simple traction used to immobilize fracture of the hip and reduce muscle spasm before surgical repair.
-it can be applied to one leg (unilateral) or both legs (bilateral)
-may be use either adhesive or non-adhesive tape.
-sometimes commercially made foam rubber boot-type splints with self-adhering straps are used.
-countertraction is applied by elevating the foot of the bed.
2. RUSSELL TRACTION-is commonly used to immobilize fractures of the femur before surgical repair.
-a sling under the thigh is used to suspend the limb, and the knee is slightly flexed.
-the pull on the limb is both vertical (through the sling) and horizontal (through the footplate)
-the degree of flexion of the knee depends on the angle needed as determined by the physician.
-the placement of the overhead pulley and the pulley on the foot of the bed varies.
-the latter may be raised so that it is line with the pulley on the footplate.
-the foot of the bed may or may not be elevated for the countertraction.
-the head of the bed should remain flat.
-a pillow may or may not be ordered to support the lower leg.
3. PELVIC BELTS or GIRDLES-provide traction around the client’s hips and relieve lower back, hip and leg pain.
-the belts is fitted directly on the skin over the iliac crests (i.e., the top margin is at the level of the umbilicus) and fastened over the abdomen.
-the straps, which attach to the pulley and weight system, may be attached either at the client’s sides, so that the pull of the traction is toward the foot of the bed, or at the back (under the client), so that the traction pull is downward and toward the foot of the bed.
-countertraction is provided by elevating the foot of the bed or by placing the client in William’s position, i.e, elevating the head of the bed and the knee gatch to approximately the same angle
4. CERVICAL HEAD HALTER TRACTION-provides skin (encircling) traction on the cervical spine.
-it relieves muscle spasms and nerve compression in the neck, upper arms or shoulders that may be associated with cervical injuries, e.g., “whiplash.”
-the head halter is attached to a spreader bar that is wide enough to prevent the halter from pressing on the client’s ears, jaws, or sides of the head.
-countertraction from the client’s body weight is provided by elevating the head of the bed
-head halter traction may be applied intermittently or continuously.
-if traction is required for a long period of time; however, the skeletal traction is applied.
5. BRYANT’S TRACTION-is an adaptation of a bilateral Buck’s extension
-is used to stabilized fractured femurs or correct congenital hip dislocations in young children under 18kg (40lbs)
-skin traction is applied to both the affected and unaffected leg to maintain the position of the affected leg.
-a spreader bar attached to the strips maintains leg alignment.
-unless otherwise ordered, the hips are flexed at right angle (90degrees) to the body, and the buttocks raised about 2.5cm (1in) off the mattress
-the weight of the child’s torso provides countertraction
-a jacket or belt restraints may be necessary to prevent the child from turning and to supplement countertraction.
6. SIDE-ARM or DUNLOP’S TRACTION-is a combined horizontal and vertical adaptation of Buck’s extension to the humerus and forearm
-the traction pull outward from the upper arm is used to align fractures of the humerus , and then pull upward from the forearm maintains the forearm in the desired alignment relative to the humerus (e.g., a 45 or 90 degrees)
-countertraction is provided by the positioning of the body; e.g., a folded blanket placed under the mattress on the side of the traction frame augments countertraction
SKELETAL TRACTIONS
TYPES:
1. BALANCED SUSPENSION TRACTION-allows the client some degree of movement when skeletal traction is applied to the femur to prevent muscle spasm and overriding of bone fragments before surgical fixation
A.)Thomas leg splint –consists of a full ring or half ring around the thigh with two rods on either side of the legs
-the distal end is attached to a weighted rope for suspension.
B.)Pearson attachment-is a sling appliance that joins the Thomas splint at knee level.
-it supports the lower leg off the bed and permits the knee to be flexed
-the pin or wire drilled through the bone is attached to a spreader, which in turn, is attached to ropes, pulleys, and weights.
-countertraction is supplied mostly by the body’s weight
-the suspension weight, however, is counterbalanced by a weighted rope attached to the proximal end of the Thomas splint.
2. SKULL TONGS (Crutchfield, Burton, Gardner-Wells, or Vinke)-immobilize fractures of the cervical and upper thoracic vertebrae.
-the tongs are secured to each side of the skull
-the center metal bar is attached to ropes, pulleys, and weights and creates a traction pull along the long axis of the spine.
3. HALO RING TRACTION-an adaptation of the skull tong
-is a circular metal band secured by two anterior and two posterior pins that penetrate the skull only a fraction of an inch.
-the ring can be attached to a weighted rope, a plaster cast or a molded plastic vest
-the latter method is referred to as a Halo-thoracic vest traction, which the halo is attached to the plaster cast or a plastic vest by metal rods. Some vest extends to the client’s pelvic girdle. The vest, which is padded with sheepskin, supports and suspends the weight of the entire apparatus around the chest.
CARE OF A CLIENT IN TRACTION
1. PIN SITE CARE-when pins are used for fixation, pin sites must be cared for to remove any secretions or crusts and to prevent infection.
-a common approach to pin site care is cleaning each pin site separately three times a day.
-use sterile cotton-tipped applicators soaked with sterile saline solution to clean away all crusts and drainage.
-the skin around the pin may be massaged gently to bring any drainage to the surface, where it can be cleaned away.
-a dressing may be applied while drainage continues.
-when there is no drainage, the dressings are usually omitted.
-after healing occurs, the pin sites are cleansed carefully with soap and water and rinsed thoroughly.
NOTE: whatever the type of pin site care used, you should constantly assess for infection at the pin sites.
Indications of infection at the sites include redness, heat, drainage, swelling and pain. Fever is a non-specific indicator that may not be present for a localized tissue infection.
2. EXTERNAL FIXATION DEVICE CARE-must also be kept clean
-the device may become soiled in the process of daily living
-a cloth with soap and water may be used to clean the device
-be sure to rinse off any soap
-do not allow water to run from the device into pin sites because it may carry bacteria into the pin sites.