Embed Size (px)
Citation preview
CASN/ACESI CLINICAL PLACEMENT PROJECTS
Project 3: Inventory of the Use of Simulated Clinical Learning Experiences and Evaluation of their Effectiveness
March 1st, 2007
Acknowledgement of Contribution and Disclaimer Results and opinions expressed in this report are those of the researchers and do not necessarily represent the views and policies of Health Canada or the Canadian Association of Schools of Nursing. Production of this material has been made possible through a financial contribution from Health Canada.
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
1
CASN/ACÉSI Clinical Placement Projects
Project 3: Inventory of the Use of Simulated Clinical Learning Experiences and Evaluation of their Effectiveness
Executive Summary
Background The use of simulation in professional health care educational programming has expanded as opportunities for clinical placements become more difficult and the challenge to provide a safe environment for patients and students during training increases as patient acuity and complexity increase. Methods of teaching clinical skills to health professionals is gradually evolving and innovative approaches for teaching and testing skills are being explored. The use of simulation technology is at the forefront of this movement. The use of simulation in nursing education has increased as educators are seeking ways to replace some elements of the high risk components of the physical experience of a clinical placement. Educators are seeking new learning strategies that will support the ability of the student to learn complex skills in a safe environment. However, it is necessary to establish the evidence base and best practices for the use of simulated learning for health care professionals. The purpose of this project is to develop an inventory of simulation use for healthcare professional preparation in Canada and explore the evidence base for its use, cost effectiveness and possibilities for multi-professional collaboration. The possibilities for simulation to provide alternatives to traditional clinical experience for nurse education, and its limitations are also explored.
The Study This project sought to:
1. Establish current practices in using simulated learning experiences for nursing and other health care professional students in Canada, and explore the potential for collaboration;
2. Identify the types of simulated learning resources and experiences used, for professional healthcare education and identify which professional groups are using them, and at which levels;
3. Establish the evidence for the effectiveness of using simulated learning experiences; 4. Explore what evidence is available from economic evaluations of simulated learning experiences to support their
use or otherwise; 5. Identify areas from the literature specific content areas that are more appropriate for the use of simulated
experiences; 6. Explore the feasibility, utility, and effectiveness of using simulated learning experiences as an augmentation to
more traditional clinical placements; 7. Investigate the potential for using a collaborative framework for implementing clinical simulations using e-
learning technologies for professional healthcare education and training in Canada. There were several components to this study. First, a literature review was conducted of background materials and documents obtained from health care professional educators related to use of clinical simulation. Second, an assessment was conducted to determine the types of simulated learning resources used and the experience of the educators in using simulated learning experiences. This study used web based technology (on-line surveys), telephone focus groups and a Delphi technique consensus survey to obtain primary source data from schools of nursing and other health care professional educational institutions to identify their perspectives and experiences in using simulation based activities. Site visits to three major simulation centres were also undertaken, and interviews with educators managing simulation-based training at these
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
2
sites were conducted. One of these was a nursing and health professional educational site (The McGill Medical Simulation Centre in Montreal), and the two others being to sites for other professions that used simulation intensively (The Air Canada Simulation Centre in Vancouver, and the Canadian Forces Trauma Training Centre in Vancouver). The target audience for the survey were all Canadian Schools of Nursing with undergraduate educational programs and schools for other health care professionals, including medicine and allied health professions. Large hospital centres offering continuing professional development were also included.
Findings: The key findings are summarised as follows:
• There remains some lack of standardization in the use of terminology in simulation (e.g. what is considered high fidelity)
• 70% of respondents indicated they used simulation learning as an augmentation to clinical learning experience, • 17/64 programs reporting used simulations as a formal requirement in their curriculum; • Undergraduate and professional development programs used simulation more than graduate programs; • Nursing and respiratory therapy programs used the highest number of mean hours of simulation while
physiotherapy programs used the lowest; • 44% of professional programs provided interdisciplinary training opportunities using simulation, with nursing
providing more than the average; • Tools used to evaluate student performance in simulations included OSCEs, video feedback, and reflective papers; • Team building was seen as a particularly valuable use of simulation technique; • Access to simulation technology is an issue due to cost or lack of access to appropriate devices; • Devices are in the early stages of development and continued improvements are seen as valuable and required; • Improved client safety and better prepared practitioners are accepted as the key reason for using simulation in
health professional education and training • Few studies exploring the cost-effectiveness or efficiency of simulation for health education exist • There were mixed responses by educators on the ability of simulation to completely replace clinical practical
experiences. The majority felt this was inappropriate, whilst some felt 10-20% could be replaced; • Actual clinical hours currently replaced by simulation were low; • Educational Institutional and Provincial Government funding accounts for most of the setup funding sources for
simulation; • There is increasing interest in using simulation for inter-professional training; • There was clear support for sharing simulation initiatives and resources.
Conclusions: Simulated clinical learning offers significant advantages over traditional educational methods. Benefits include the provision of a safe environment for both patient and student during training in high risk procedures, unlimited exposure to rare but complicated clinical events, the ability to manipulate training opportunities rather than wait for a suitable situation to arise, the ability to provide immediate feedback, the opportunity to standardize and evaluate performance, the opportunity to repeat performance, and the ability to efficiently organize team training. It also may present opportunity for lower costs in certain instances. Currently, the ability of simulation to meet the needs of practice education remains limited.
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
3
Recommendations: The empirical evidence to support the use of clinical simulation for nursing education remains somewhat sparse, particularly in terms of economic performance. Because of increasing pressure to find alternatives for clinical practical experience there is a danger of seeing simulation as a panacea for all shortages of clinical experience. Currently, we do not have the evidence to support that presumption, and with the current state of the art, it would be more appropriate to seek to resolve these particular difficulties by other means. The nature of clinical practice with highly–complex client needs, and unpredictable nature of much of real-world health care practice means that currently the ability of simulation to meet the needs of practice education remains limited. That does not mean that simulation has a large role to play in professional healthcare education, but that we need more information to seek the optimum balance between simulated and actual practice. The biggest question that remains has been identified as:
“Does a comprehensive strategy of competency-based training, using multiple modalities including simulation and supervised client care yield better outcomes for patients, fewer errors, or more efficient patient care and education than does the current system of mostly apprenticeship-based training?”
Dutta et al (2006)
Future simulation research should be undertaken to address the following issues:
• Validate the cost-effectiveness and cost efficiency of specific types of simulation; • Validate the cost-effectiveness and cost-efficiency of clinical simulation practices in specific programs; • Establish a focus on highly specific outcomes measures, with specific target populations and large numbers of
subjects in simulation research; • Establish the value of inter-professional simulation-based education; • Establish the pedagogic dimensions of simulation use in terms of established learning theory.
In addition, nurse educators have the opportunity to drive the development of simulation technologies to meet their particular needs. Manufacturers need to facilitate more nursing focused scenarios for client groups within and beyond the acute medical surgical environment. Educational Institutions and Provincial Government funding accounts for most of the setup funding sources for simulation initiatives, and there is a clear need to maximize the efficiency of using simulation in more multi-disciplinary centres and using inter-disciplinary learning activities. Simulation and particularly high fidelity simulation is a costly investment for education providers and it is important to gain benefit from economies of scale, and making best-use of these resources. Education providers should develop these resources with these points in mind, and existing centres should explore ways to open up access for inter-disciplinary education to publicly funded providers of professional healthcare education. Finally, there was clear support amongst the participants in this study for improved collaboration. We need to examine better ways of sharing resources between different institutions, and Canadian healthcare education providers should engage in the sharing of tools and practices to promote a community of healthcare simulation users for the benefit of all.
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
4
Table of Contents
Introduction .............................................................................................................................................................................. 5 Background .............................................................................................................................................................................. 5 Project Goal and Objectives ..................................................................................................................................................... 5 Researchers, Partners and Funding........................................................................................................................................... 6 Methodology ............................................................................................................................................................................ 6
Design .............................................................................................................................................................................. 6 Target Audience ............................................................................................................................................................... 7 Instruments ....................................................................................................................................................................... 7 Ethical Review ................................................................................................................................................................. 8 Participants ....................................................................................................................................................................... 8 Themes in the Literature................................................................................................................................................... 9
Findings.................................................................................................................................................................................. 15
A. Trends in Use by Profession, Level, and Type ................................................................................................... 15 B. Types of Simulation Use and Access ................................................................................................................. 27 C. Planning and Organizing Simulation in the Curriculum..................................................................................... 35 D. Meeting the Needs of Practice............................................................................................................................ 47 E. Investment in Simulation.................................................................................................................................... 60 F. Additional Information....................................................................................................................................... 68 G. Pedagogic Dimension Mapping Exercise........................................................................................................... 69
Conclusions ............................................................................................................................................................................ 71 Recommendations .................................................................................................................................................................. 74 Acknowledgements ................................................................................................................................................................ 73 References .............................................................................................................................................................................. 77 Appendices............................................................................................................................................................................. 84
Report Prepared by: Dr. Bernie Garrett, Assistant Professor, UBC School of Nursing Dr. Elizabeth Tench, Statistician Rena van der Wal, Professional Practice Director, Nursing & Allied Health, Vancouver Coastal Health Pascale Fretier; Graduate Research Assistant (French translation) Front cover photograph courtesy of Laerdal Medical Corporation.
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
5
Introduction The aim of this project was to explore the use of simulated clinical learning experiences in healthcare professional education and training in Canada and evaluate the effectiveness of this approach based on the existing evidence. With diminishing opportunities for clinical placements, it is necessary to consider alternate models of clinical learning experience, including simulation. It is therefore necessary to establish the evidence base and best practices for the use of simulated learning for healthcare professional education and training. The overall aim was to develop an inventory of simulation use for healthcare professional preparation in Canada, and explore the evidence base for its use, cost-effectiveness and possibilities for multi-professional collaboration. The possibilities for simulation to provide alternatives to traditional clinical experience for nurse education, and its limitations are also explored.
Background The use of simulation in professional health care teaching has expanded with the development of technologies providing more complex interactive platforms to support highly realistic simulations (Grenvik & Schaefer, 2004; Patow, 2004). The latest technologies include interactive computer linked mannequins (patient simulators) and digital multimedia utilizing artificial intelligence (AI) techniques (Xia et al, 2005; Shim, 2005; Pham et al, 2005;Garrett & Callear, 2001; Novak, 1993). Methods of teaching health professionals clinical skills are gradually evolving, and novel approaches to imparting and testing these skills have been sought. At the forefront of this movement is the use of simulation technology. In medical education, there has been increasing use of high-fidelity simulation devices for skills base training, particularly in the fields of surgery, anaesthesiology, and trauma (Barsuk et al., 2005; Brinchmann-Hansen; Grenvik & Schaefer, 2004; Thistlethwaite, 2004; Weller, Robinson, et al, 2004; Qayumi et al, 2004). The use of simulation in nursing education, has also been employed in a number of areas over the years, including intensive care (Henry & Waltmire, 1992), child health (Krawczak & Bersky, 1995; Lauri, 1992), physical assessment (White, 1995), medical-surgical nursing (Garrett & Callear, 2001; Hjelm-Karlson & Stenbeck, 1997; Medley & Horne, 2005) and also in midwifery (Lyons, Miller, & Milton, 1998; Woodson, 1997; Cioffi et al. 2005). Computer-based simulations have been employed as a valuable tool in contemporary problem-based learning approaches, particularly in the development of complex clinical skills such as clinical decision-making. The use of high-fidelity simulations of specific clinical practices for education and training is now a practical reality and has a range of applications across a wide range of healthcare professions. By providing practice in clinical skills in realistic settings, simulations can provide effective educational tools that may actually be able to replace some elements of actual physical experience, and allow for the evaluation of students in these skills, thereby augmenting clinical practice and possibly even replacing some elements of it.
Project Goal and Objectives This project sought to: 1. Establish current practices in using simulated learning experiences for nursing and other health professional students in Canada, and explore the potential for collaboration; 2. Identify the types of simulated learning resources and experiences used, for professional healthcare education and identify which professional groups are using them, and at which levels; 3. Establish the evidence for the effectiveness of using simulated learning experiences; 4. Explore what evidence is available from economic evaluations of simulated learning experiences to support their use or otherwise; 5. Identify, from the literature specific content areas that are more appropriate for the use of simulated experiences;
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
6
6. Explore the feasibility, utility and effectiveness of using simulated learning experiences as an augmentation to more traditional clinical placements; 7. Investigate the potential for using a collaborative framework for implementing clinical simulations using e-learning technologies for professional healthcare education and training in Canada.
Researchers, Partners and Funding Bernard M. Garrett, RN, PhD was the overall project manager responsible for all aspects of the project. Jo-Anne Swanson and Pat Griffin were responsible for overseeing the project on behalf of CASN/ACESI. An Advisory Committee appointed by CASN/ACESI liaised with their organization, promoting the project and providing advice and feedback to the project manager. The project was funded by the Canadian Association of Schools of Nursing/ Association Canadienne des Écoles de Sciences Infirmières (CASN/ACESI), with in-kind support from the University of British Columbia (UBC) School of Nursing and Vancouver Coastal Health (VCH).
Methodology Time frame for Implementation of activities Implementation of the project occurred in three phases. The first phase, preparation and data collection, comprised the first four months. The project employed an online survey methodology for obtaining primary source data from schools of nursing and faculty members involved in simulation-based activities. The second phase focused on data management, including data cleaning and analyses. The third phase consisted of interpretation, recommendation and evaluation, using further referent group discussions at the national and level, and visits to several simulation centres.
Phase 1: September 2005 to April 2006 Phase 2: April 2006 to December 2006 Phase 3: December 2006 to March 2007
Design The following describes the design of the study: 1. An inter-professional advisory committee was struck by CASN/ACESI to oversee the entire project from its inception
to its completion, and offer assistance and advice as the project progressed. This committee consisted of representation from major nursing, health professional and other stakeholder groups. This committee included representation from:
Canadian schools of nursing Canadian schools of regulated nursing bodies (e.g. LPNs, RPNs) Other health professional education providers for physicians, physiotherapists, occupational therapists, paramedics,
operating department practitioners, nurse–practitioners, midwives and social workers. The Academy of Canadian Executive Nurses (ACEN) The Association of Canadian Academic Healthcare Organizations (ACAHO) the Canadian Healthcare Association
(CHA).
2. A local project management team was established at UBC consisting of a project manager, two research assistants and a French translator to undertake the work.
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
7
3. A literature review of background material, and related documents regarding the use of clinical simulation in healthcare professional education was undertaken by the project team.
4. A sample base for the survey was developed, to include all schools of nursing and medical schools in Canada, and
education providers for the allied health professionals (as previously listed), clinical health care agencies providing continuing professional development for health care professionals, preceptors of newly qualified health care professionals and students.
5. A research strategy and tools were developed, included 3 data collection methods: a) A Web based survey questionnaire exploring usage, costs and perceptions of the
value of clinical simulation (for pre-licensure education providers and post qualifying education providers and health care agencies) b) A Delphi technique consensus survey of the pedagogic value of clinical simulation for clinical education providers, and
c) Telephone Focus groups (for educators/trainers, and preceptors using simulation). 6. Site visits to three major simulation centres were organized. One being a nursing and health professional educational
site and the two others being to sites for other professions that used simulation intensively (aviation and military). Interviews with educators managing simulation-based training at these sites were planned.
7. Ethical review of the study design was obtained from the UBC Behavioural Ethics Review Board. 8. Data was collected using the approaches/tools outlined above. 9. These data were analyzed, using descriptive statistics and content analysis of performance indicators, simulation usage
patterns, trends and perceptions of the value of clinical simulation in professional healthcare education. 10. A final written report was collated for dissemination of the findings.
Target Audience All Canadian Schools of Nursing with undergraduate education programs comprised the primary target audience for the survey, giving the potential number of schools of nursing participating at 81. In addition, all Canadian Medical Schools were included, as well as institutions offering pre-registration Dentistry, Physiotherapy, Occupational Therapy, Paramedic, Social Work, Midwifery, and Operating Department Practitioner education and training. Lastly, large hospital centres offering continuing professional development courses were also included. Referent Groups were comprised of volunteers from the original respondents to the survey and additionally members of two other professions (civilian aircrew and military medical technicians) engaged in professional simulation based training/educational activities. All potential participants were invited to participate.
Instruments An online questionnaire, in English, was developed and pilot tested with five experts from simulation-based healthcare education practice and the CASN/ACESI Advisory Committee. As well, pilot testers and the Advisory Committee reviewed the cover letter and a document of definitions, and provided feedback on their clarity, relevance and comprehensiveness. Documents were revised to reflect this input and the final questionnaires and other study documents were then translated into French. The online French questionnaire and other materials were reviewed by native French speaking Canadians from the Advisory Committee to ensure accuracy, as well as suitability of translation for technical

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
8
terms. Copies of the English version of the three questionnaires, cover letters and definition document are found in Appendix B. For the Delphi consensus survey, a pedagogic mapping tool was required. Several were explored including David Gabba’s excellent “Dimensions of Simulation” tool (Gaba, 2004). However, the broader pedagogic dimension mapping tool created by Reeves & Laffey (1999) was selected as it clearly delineates the pedagogic dimensions of interactive learning (see Appendix B for details of this tool). Each of the eight dimensions mapped represents a bipolar continuum of values for a single pedagogic factor. This was chosen as they provide a simple and practical tool to describe the instructional design of a high-fidelity clinical simulation application. The tool allows the delineation of the pedagogic dimensions involved and identification of the instructional design in terms of learning theory (Reeves & Laffey, 1999).
Ethical Review A submission was made to the University of British Columbia Behavioural Ethics Review Board (http://www.ors.ubc.ca/ethics/index.htm for ethical review of the study design and data collection methodologies. The project was subsequently approved and once this had been granted the data collection proceeded as planned. The letters and consent form for participation can be found in Appendix B)
Participants There were 71 respondents who agreed to complete the survey of which 11 respondents also took part in the telephone interviews. There were a also 8 respondents who took part in the pedagogic mapping exercise. Overall, 71 questionnaires were completed of 195 sent out giving an overall response rate of 36%. Of the 71 individuals that participated in the survey, 5 respondent’s data were incomplete. This resulted in a total N of 64 respondents being retained in the study. Twelve of those indicated they did not use simulations, leaving 59 individuals who completed the full questionnaire. Participants were asked a question regarding whether they used or intended to use simulations in their training programs. Of the 12 who did not use simulation, two of them indicated that they intended to start using simulations in the next year; and five of these individuals indicated that they intended to begin use of simulations in the next two years. Of the 11 respondents who took part in the telephone focus group interviews, 10 currently used simulations. The respondent who did not use simulations was retained in the study as their input provided some useful additional information. The numbers of participants and proportions of profession, level, and type of simulation represented can be found in Figure A.1.1. For example, 43 of the 64 respondents (67%) represented Nursing Programs. A cautionary note about the category totals: because respondents can legitimately represent more than one profession, level or type, overlap can occur. For example, one respondent might represent Nursing and Paramedic programs, undergraduate and graduate programs, and utilize High, Medium and Low Fidelity Simulations. Due to overlap, totals by various categories may be skewed, for example, totaling amounts invested by profession exceeds the total amount invested over the 64 respondents as some are counted more than once. These totals are useful when comparing professions but do not accurately reflect the overall totals. The reader is cautioned to take this into account when reading this article.
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
9
Themes in the Literature The Increased Use of Simulation in Professional Education and Training The application of abstract theory to practical situations is an area where simulation can be particularly useful (Laurillard 1997), and as health care professional education is practice based, simulation techniques offer particular appeal here. The aviation industry has successfully been using computer-based simulation techniques to train pilots for a number of years, and the military have successfully used simulations for tactical training (Fletcher 1999). Simulation based training has also proved valuable in areas where experiential learning may not be possible due to time, cost or operational constraints such as in the training of police to respond to bomb threats (Chung & Huda 1999). The types of simulation used in health care education include:
• System facsimile: the training of staff to operate computerised interfaces identical to the real thing under safe conditions, e.g. a simulated computer controlled dialysis control interface.
• Apparatus and procedural operations: the use of actual representations of equipment requiring human
manipulation to operate, e.g. an endoscopy simulator for training physicians.
• Practical scenario-based simulation and decision-making exercises: Individual client focused clinical simulation exercises or large-scale simulations, such as trauma team exercises or management exercises.
• Process modelling: demonstrating the effects of all characteristics of a phenomenon in a computerized model, e.g.
modelling a molecular structure.
(after Dean &Whitlock,1992; Ziv & Berkenstadt 2004). This demonstrates the wide range of applications for simulation, and many of the more complex modern simulation tools offer complex multi-faceted simulations incorporating more than one of these categories. Many modern health professional educational applications involve a combination of practical scenario-based simulation and apparatus operation. The use of simulations as learning tools has been growing in many areas of health care education. Originally pioneered in the fields of anaesthesiology and emergency medicine (Buck, 1991; Gaba, 2004; Vardi et al, 2003), other areas of more recent use include surgery (Ro et al, 2005; Susuki et al, 2005; Xia et al, Spicer et al, 2005; Qayumi & Qayumi 1999) and dentistry (Wierinck et al 2005; Abbey, 2002), critical care nursing (Hravnak, 2005; Lavell, 2006; Vaughan, 2006), paediatrics (Krawczak & Bersky, 1995; Tsai 2004), medical-surgical nursing (Wood, 2006; Shaw, 2006; Schoening et al, 2006), midwifery (Robertson, 2006; Rennie & Main, 2006). In 2006, Simulation in Healthcare was established as the first journal devoted entirely to the topic of simulation and the field continues to promote research interest with over 100 papers published on this subject over the last 3 years in the discipline of nursing alone. The use of simulation in nurse education is an area where it may hold significant promise for further development. Physical or computer-based simulation provides a valuable tool for contemporary problem-based learning approaches, particularly in the development of skills such as clinical decision-making (Docherty et al, 2005; Garrett and Callear 2001). Immersion and Fidelity Simulation involves techniques and technologies that create guided, interactive, and often immersive activities mimicking experiences of a real-world environment (Gaba, 2004). The immersive nature of simulation refers to its ability to evoke or

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
10
replicate substantial aspects of the real world in a way that engages the student in the simulation. Immersive simulations convey the sense that participants are immersed in the activity, as they would be in real life. “The ideal example of full immersion (admittedly fictional) would be the Star Trek holodeck, in which one literally cannot tell the difference between the simulated experience and real life” (Gaba, 2004). Experience with simulation tends to suggest that the more immersive simulations are for the participants, the more value they have in the learning process (Gaba, 2004; Niermyer et al, 2004; Mastrangelo et al; 2002).Various techniques have been employed to assist with immersion of students in the simulation, such as adding real world props (equipment, actors etc) to practical simulations, or by adding multimedia to computer-based simulations or time limits based on real world events to provide stressors, and all of these provide a way in which the student’s experiences can be made more active and involved (Gaba, 2004; Garrett and Callear 2001; Wang et al, 1998; White 1995; Bustio et al. 1996). Fidelity in simulation generally refers to the degree to which a simulation recreates the characteristics of the real world (Beaubien and Baker, 2004). Fidelity is the degree to which a simulation provides an accurate and truthful representation of the original phenomenon. High Fidelity Simulations represent reality to a very high degree. E.g. full motion flight simulators and complex human patient simulators. The use of the latter has increased over the last five years with the implementation of more advanced and realistic patient simulators (Gaba, 2004). Low fidelity simulations represent some limited aspect of reality E.g. classroom role play exercises. Simulation fidelity is not one-dimensional (Beaubien and Baker, 2004), and fidelity may involve the environment of the simulation, the equipment in use or psychological fidelity (the
degree to which the trainee perceives the simulation to be a believable surrogate (Rehmann et al, 1995). The experience in the health professional education setting suggests high-fidelity simulation has an increasing role to play in the attainment of more complex psycho-motor skills (e.g. with apparatus or procedural operations), and may help with immersion (Dutta et al, 2006). However, other forms of lower fidelity simulation have been found to be effective in health professional education, including role play, case studies, and task-trainers, and these have a long established base of research to support their effectiveness for training in communication skills and team work (Goldenberg et al, 2005; Marsh, 2005; Yee et al, 2005; Beaubien and Baker, 2004; Lowdermilk & Fishel, 1991; McArthur,et al, 1989; Novack et al, 1992; Sutnick & Carroll, 1981; Lowe 1975). There is inconsistent use of the terms, low, intermediate and high fidelity in the literature, which can cause some confusion. Some authors refer to high fidelity simulation where the simulator models responses to environmental or physiological changes automatically (e.g. McIntyre, 2004; Qayumi & Qayumi, 1999), whilst others suggest broader definitions. Low-fidelity simulation is generally used to describe screen-based computer program simulators and basic mechanical models. The Canadian Patient Safety Institute used the following definition in 2005 (CPSI/ICSP 2005), and this has been adopted for use in this study:
• High-fidelity simulation: Combines highly sophisticated, life-like mannequins with computer programs driven by complex models of respiratory and cardiovascular physiology and extensive pharmacological modeling of drugs. The result is a dynamic, integrated system with opportunity for multidisciplinary training. This includes both computer model-driven simulators and instructor-driven simulators (e.g. METI® Human Patient Simulator, Laerdal SimMan® and MedSim Eagle Patient Simulator). Also standardized patients can be considered in this context for modelling normal physiology, or easily mimicked conditions.
• Intermediate-fidelity simulation: Replicates only part of the environment, enabling simulation of a subset of
functionality. This category includes virtual reality and haptic systems as well as part task trainers that are used to train both basic and complex technique related to psychomotor skills. Examples include the MedSim UltraSim, AccuTouch endoscopy simulator, laparoscopic simulators, and the 'Harvey' cardiology simulator. Note that this category does not include basic mechanical models that lack functionality for feedback or varying of scenarios.

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
11
The use of high-fidelity simulation in healthcare has expanded in line with the development of increased computer processing power, and performance as well as reduced costs to support the control of simulation devices in compact and affordable units. High-fidelity is now proving its value in the simulation of activities where experiential learning is expensive, undesirable, or even dangerous. High fidelity computer controlled patient simulators have been used increasingly in nurse education and many centres have set up high fidelity clinical laboratories (Shoening et al, 2006; Fletcher, 2005; Lavell et al, 2006; Hravnak, et al, 2005). Using Simulation to Develop Clinical Decision-making Skills Problem solving ability has been recognized as central to nursing practice (del Bueno, 2005; Roberts et al. 1993) and this requires the development of critical thinking and decision-making skills. The solutions to clinical problems arise from complicated cognitive processes and require critical thinking skills. The use of simulation to test clinical problem solving skills developed in the late 1960's with basic paper-based simulations to test the problem solving skills of nursing students (de Tornyay 1968). These simulation exercises, however, were complex, unwieldy, and difficult to manage with large groups of students. Another problem was that nurse teachers carried out the assessment of student performance giving summative scores whilst this type of assessment has since been shown to have limited value in helping students develop skills (Gipps 1988, Gipps & Murphy 1995; Torrance 1995). Students find learning from simulations most beneficial when there is formative feedback immediately following an event (Shoening et al 2006; Laurillard 1995, 1997; Johannson & Wertenberger 1996; Lyons, Miller & Milton 1998). Such immediate individualized feedback requires the analysis of an experienced tutor or some form of artificial intelligent system to provide this. Nevertheless, the use of simulated patient based experiences using real data have shown great promise in developing clinical decision making skills, and student self-efficacy in this area. For example, simulations using anonymised patient data from clinical information systems, and computerized clinical decision support systems have been used to structure effective scenarios for developing nurse’s clinical decision making skills (O’Neil et al, 2006; Watkinson et al, 2005). Bremner & Brannan (2000), Garrett & Callear (2001) and Hjelm-Karlson & Stenbeck, (1997) all reported positive effects in using computer-based simulations to develop nurses clinical decision making skills. Lasater (2005) and Medley & Horne (2005) reported success with using high-fidelity exercises for students to enhance their clinical decision making skills in acute care. In midwifery studies, Cioffi (2006) and Baker (1997) also indicated that simulated clinical activities improved clinical decision making skills. Medical education and dentistry have also found simulation effective here (Docherty et al, 2005; Allen & Moore, 2004; Bond & Spillane, 2002). Steadman et al (2006) even suggest simulation-based training is superior to problem-based learning for the acquisition of critical assessment and management skills. Client Safety Client safety remains a key issue in health care provision. Research into adverse events (AEs) has highlighted the need to improve patient safety. A recent Canadian study demonstrated an AE rate of 7.5 per 100 hospital admissions and amongst clients with AEs, events judged to be preventable occurred in 36.9% of cases and death in 20.8% (Baker, 2004), Physician reviewers also estimated that 1521 additional hospital days were associated with AEs (Baker et al, 2004). The Canadian Patient Safety Institute (CPSI) identified the value of simulation in helping prevent AEs in its 2005 study (CPSI, 2005), and many authors have identified the contribution of simulation based education and training in improving client safety. In the critical care environment, Lavele et al (2006) and Henneman & Cunningham (2005) suggested improved safety can be achieved using high-fidelity mannequins and simulated exercises. In nursing, Herold (2005), and Van Sell et al (2006) identify a clear role for high-fidelity simulation in pre-registration nurse education. Recently Spencer (2006), Fried et al (2004), and Gaba (2004) have all identified value in using surgical simulation for improved client safety. In a recent study exploring the impact of video simulations on training surgeons, Ziv et al (2005, 2003) and Scerbo (2004) have also highlighted simulation as an ethical imperative for medical education in order to reduce AEs. In resuscitation simulation using medium and low fidelity mannequins has a long history (Long, 2005), and the use of role-play based simulation in

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
12
managing violence and aggression has also been successful (Gates et al, 2005). Effectiveness of Using Simulation The value of simulation as an effective educational tool for health professional education has been demonstrated in many areas, particularly in the fields of medicine and anaesthesiology, although it still remains to be conclusively demonstrated as best practice. A literature review of 18 articles from 1991 to 2005 on the use of human patient simulators (HPS®) in teaching suggests evidence of faster skill acquisition and performance improvements. In a randomized trial comparing performance in simulator-trained versus moulage-trained physicians in initial trauma assessment, a significantly improved performance in the simulator-trained cohort was demonstrated (Lee et al., 2003). Additional investigations, predominantly in the anaesthesia literature, support the use of HPS® for skill acquisition (Deanda & Gaba, 1991; Hotchkiss, Biddle, & Fallacaro, 2002), and throughout the literature, participants in HPS® scenarios have expressed positive learning experiences. Abrahamson et al (2004) reported the effectiveness of high fidelity simulation in training anaesthesiology residents. Costanza, et al (1999) reported the effectiveness of using standardized patients (SPs) to improve community physician skills in mammography counselling and clinical breast examination. Standardized patients are actors who have been carefully coached to simulate an actual patient, and have taken over from real patients in many areas of medical education. Berg et al (2001) undertook a study that reported computer-based virtual-reality simulation provided a valid method for teaching surgical suturing skills. Similar results have also been reported using simulation with nursing students (Alliner et al, 2006; Becker et al, 2006), combat medical technicians (Heman, 2005), midwives (Wilford et al, 2006; Cioffi, 2005) and dentists (Welk et al, 2004). A number of comparative studies have been undertaken to validate the effectiveness of simulation as a teaching tool compared with traditional methods. Becker et al (2006) undertook a comparative study of undergraduate nursing students. In critical care and resuscitation, there is good evidence of the effectiveness of simulation. Wood (2006), Grenvik (2004) Hammond (2004) and Ali (1998) have all identified positive effects of simulated practice. Likewise, Bowyer, (2005) reported similar outcomes for intravenous therapy skills and also Holzman, (1995) documented positive results in the field of anaesthesiology. Schwid et al reported positive results in their multi-institutional study evaluating anaesthesia residents using mannequin-based simulation (2002). In the field of surgical education, Carter et al identified the effectiveness of SPs in surgical student’s clerkships (2005), and Ahlberg et al also identified that virtual reality simulation was an effective surgical training tool (2002). Sedlack et al (2004) identified computer based simulation training enhanced the competency of gastroenterology fellows colonoscopy skills. Dentists have also found positive outcomes in comparative studies (Amano, 2004; Schittek Janda, 2004). In nursing education Ravert (2004), Garrett & Callear (2001), and Burrows (1989) have also reported positive outcomes for simulation in comparative studies. In medicine using virtual reality simulations, Burdea (1999) reported less conclusive findings, however, noting that a virtual prostate palpation simulator used with medical students, while promising, needed significant improvement in both model realism and interface hardware. Sutherland et al (2006) reviewed 30 randomized controlled trials and found that surgical simulation was overall no more effective than other training methods. Computer simulation generally showed better results than no training at all (and better than physical trainer/model training in one RCT), but was not convincingly superior to standard training. The study did not find evidence for the superiority of any specific type of surgical simulation (eg, video, computer, or cadaver-based). There is also very little evidence exploring the degree to which simulation can be used to replace actual clinical practice. Jeffries, 2005 and Gaba (2004) note that this is still an unknown quantity. In terms of exploring costs associated with simulation, it is useful to differentiate between cost-benefit, cost-effectiveness and cost-efficiency:

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
13
• Cost-benefit: a measure in economic terms of the benefits of the education to the individual and society in terms of the rate of return to the individual and to society as a whole. A cost-benefit analysis is useful when both cost and effects can be measured in monetary terms.
• Cost-effectiveness: a measurement of the extent to which an educational system produces outputs that are relevant to the needs and demands of its clients. Cost-effectiveness is useful when costs are expressed in monetary terms and effects are measured in non-monetary terms.
• Cost-efficiency: a relative measure of comparison to another system; where the output costs less than the other system per unit of input. An educational system increases its cost-efficiency when it maintains output with a less than proportional increase in input" (Rumble 2001).
Several recent studies exploring the cost-benefits of simulation report positively on the use of these techniques in specific areas, although this subject is poorly represented in the literature. Hanchett (2002) found that training simulators for IV education provided significant cost-benefits and improved opportunities. McGovern & Johnston (1996) suggested that the use of computer-based simulation for training surgeons was cost-beneficial. Dr. David Gaba, in his 2004 paper exploring the future of simulation, notes that the costs and benefits of simulation are difficult to determine, especially for the most challenging applications, and long term use may be required to establish these. The cost-effectiveness of simulation has been explored in several areas. Grenvik et al (2004) suggest that clinical simulation offers advantages over traditional medical education methods that include lower costs, both direct and indirect. Rosengren et al (2005) identified that simulation showed promise as a cost-effective alternative for use with motivational interviewing skill assessment with medical students interviewing substance abusers. In the surgical arena, the use of simulators to teach microsurgical suturing techniques has demonstrated cost-effectiveness (Lahiri et al 2005). This has also been demonstrated in arthroscopic knee surgery (Heng et al 2004). Samsel et al (1994), in a study using computer-based simulation for teaching first year medical students cardiovascular physiology, found computer simulations more cost-effective than animal demonstrations. Hemman (2005) also found that improving combat medic training was more cost effective when a computer-based virtual training simulator was used. Theroux & Pearce (2006) suggested that for nurse practitioners, learning pelvic examination simulation was less cost effective compared with voluntary peer examination, but that the latter was a less effective teaching method. Studies exploring the cost-efficiency of simulation are also rather sparse in the literature. Wong, et al (2004) explored the use of full scale computer simulators in anesthesia training and evaluation, and found that their cost-efficiency was at least questionable. Haluck & Krummel (2000) explored the value of computers and virtual reality and suggested that simulation might be more cost-efficient compared to the current system of surgical resident education. In the use of simulation for distance education, it seems there is more evidence, and von Lubitz et al (2003) indicated that, in medical education, preliminary data on distance-based high-fidelity human patient simulation indicates it is more cost-efficient that current methods. The Validity of Using Simulation to Evaluate Performance
Many studies have been undertaken demonstrating the value of simulation in the evaluation of student’s clinical skills, and this is a commonplace practice in many professions. It has been suggested that the near-random clinical experiences of students do not provide consistent, repeated practice for objective performance evaluation (Petrusa, 2004). Forker & McDonald (1996) identified a clear trend in evaluation methodologies moving towards using computer adaptive and computer simulation testing in healthcare professional education. Often SPs (usually actors or more recently high-fidelity

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
14
mannequins) are used in structured simulation exercises in medical education. Bartfay et al (2004) undertook a meta-analysis of Objective Structured Clinical Examination (OSCE) practices in medical education and supported the use of this simulated approach in reducing variation in the student’s experiences, and in the marking by different assessors. Beaulieu et al (2005) reported similar results with the use of SPs (actors) with qualified physicians. Structured simulations using SPs have been reported as effective for training in communication and interviewing skills for physicians (Blake et al, 2000), and for providing remedial support (Blake et al, 2001). Devitt et al (2001) identified that simulation based training of medical and anaesthesiology students using a high-fidelity anaesthetic simulator provided evidence that the simulation based method could discriminate between practice categories and provided a valid performance assessment tool. Weller et al (2003) also reported similar results with high-fidelity simulation and anaesthesiology students. Hatala et al (2005) also supported the use of SPs and simulated exercises as an evaluation tool in the Canadian internal medicine speciality examination. Bartfay et al (2004) and Konkle-Parker et al (2002) suggest the implementation of OSCE would also be appropriate in nursing education, whilst Ebbert, D. W., & Connors, H. (2004) and O’Connor et al (1999) support this approach for nurse-practitioner education, and Baez (2005) for social worker education. The use of simulation based testing has also been explored in other professions. For the training of surgical laparoscopy skills, Aucar et al (2005) suggested that, although imperfect, there is an emerging body of evidence establishing the validity of simulation techniques for assessing surgical skills. Likewise in anaesthesiology, Gaba et al (1998) report the successful use of practical simulations in assessing clinical performance during simulated crises using both technical and behavioural ratings. However, Wong (2004) suggested that, although there is some preliminary evidence of reliability and validity in using the simulator to evaluate clinical competence, the development of such techniques has not progressed enough to justify its use in formal, summative evaluation of competence in anesthesia at this time. Tomlin (2005) reported success using interactive video client simulation scores to predict clinical performance of occupational therapy students. Simulation to Support Inter-Disciplinary Team Work The aviation industry has used team-based simulation activities (crew resource management – CRM) for a number of years, and it is accepted as an essential part of crew training, although the evidence of its contribution to safety remains difficult to quantify (Salas et al, 2001). There is a growing body of literature exploring the use of simulation in team based training for health professional education, and more recently for interdisciplinary team based education and training. Grenvik et al (2004) described the effectiveness of team based training in critical care medical training, noting that The Institute of Medicine in its book “To Err is Human” (IOM, 2001) recommended establishing interdisciplinary team training programs incorporating efficient methods such as simulation. Moorthy et al (2005) reported that team-building skills training for surgical trainees using procedural simulations in a simulated operating room, proved effective. Mueller et al (2005) found that teaching anti-arrhythmic therapy and ECG interpretation in simulator-based interdisciplinary undergraduate education improved teamwork skills. Blum et al (2005) explored criteria for measuring the effectiveness of simulation-based team training for improving communication skills, and reported positive outcomes. In undergraduate nursing education, Medley & Horne (2005) noted that team based exercises provide an important area for the use of practical simulations. Larew et al (2006) found that high-fidelity simulation provided a positive learning experience in which students refined their patient management skills while collaborating with multidisciplinary team members to resolve common postoperative problems. Rodehorst et al (2005) suggested that the use of interdisciplinary simulation activities could be positive in helping health care professional team members understand each others’ roles. Likewise, Siktberg et al (2005) support the use of interdisciplinary simulations with this perspective. Kyrkjebø et al (2006) also support the role of interprofessional simulation for nursing education in improving client safety.
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
15
Findings
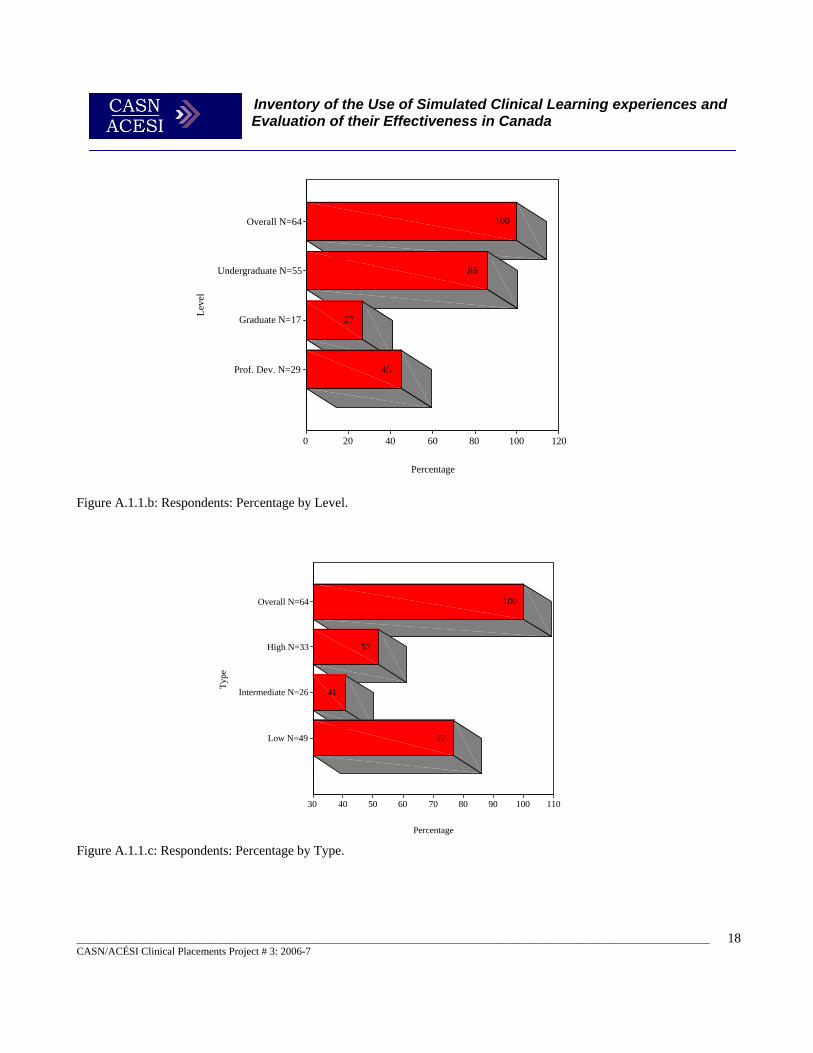
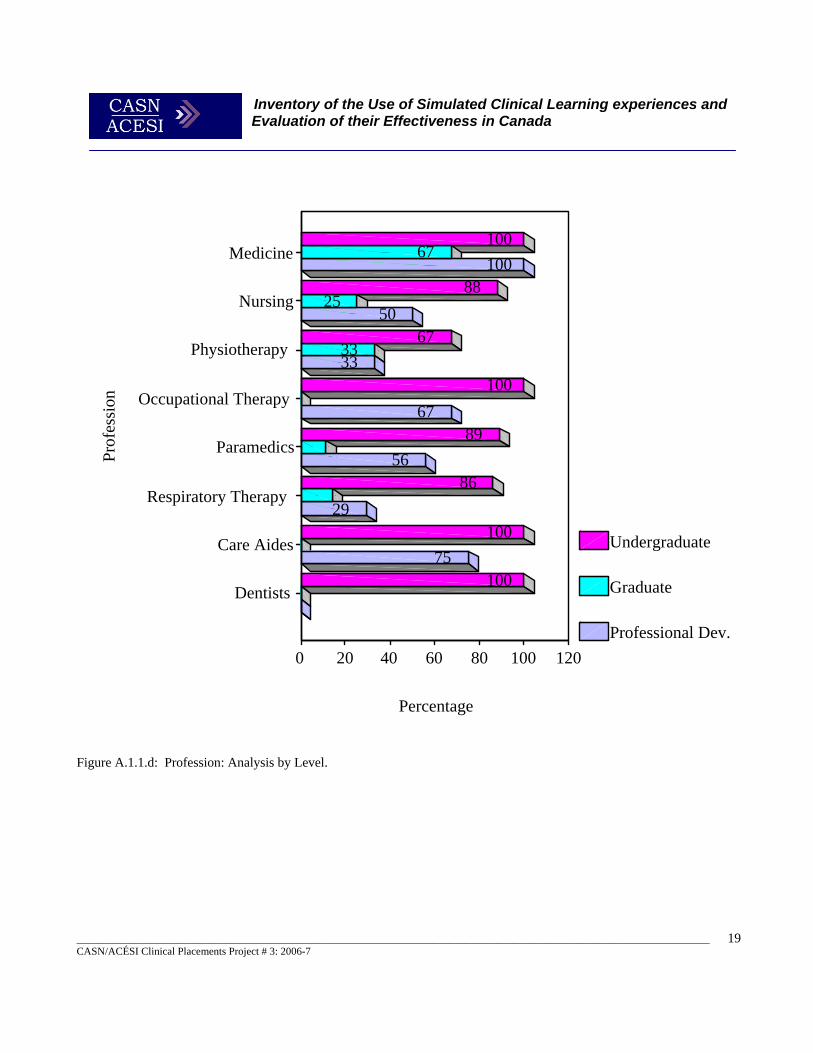
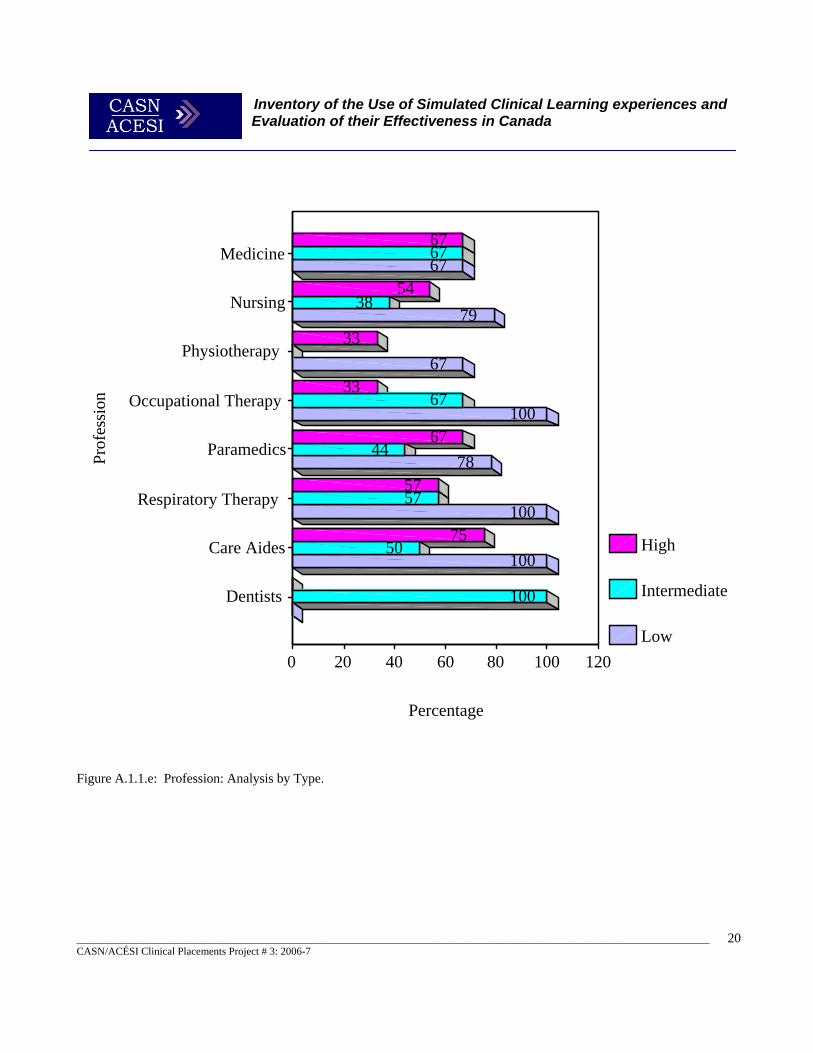
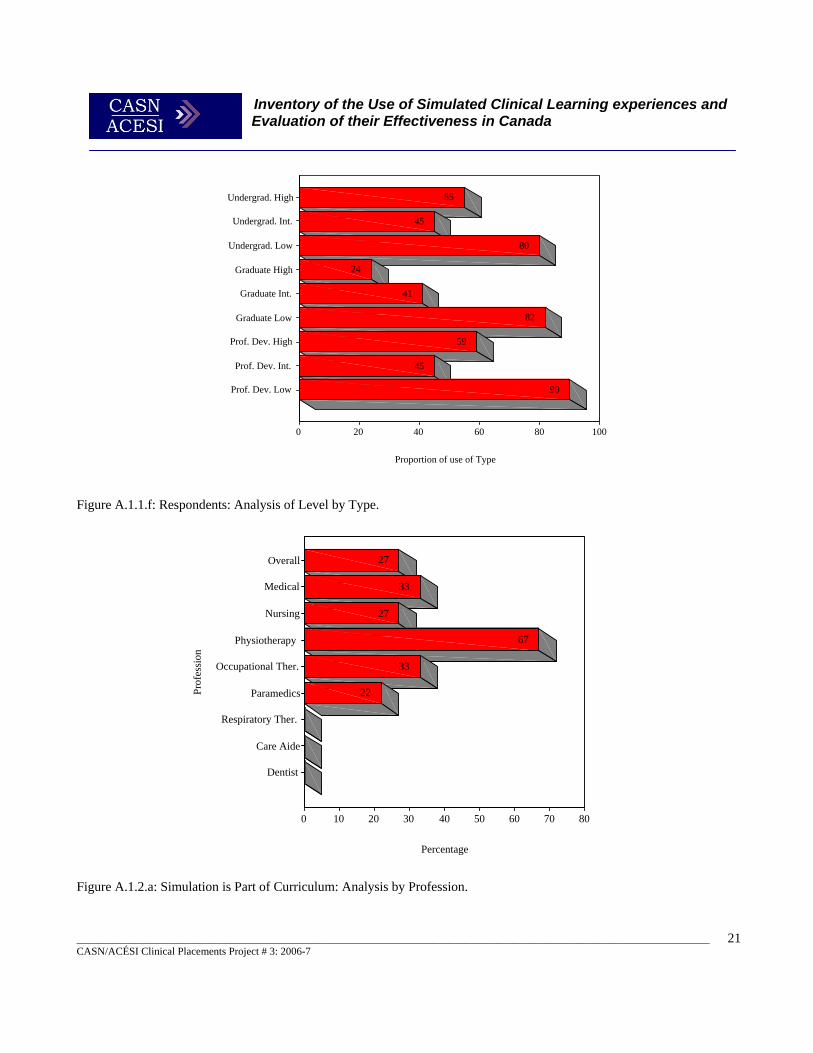
A. Trends in Use by Profession, Level, and Type The number of programs represented for each profession can be found in Figure A.1.1. Although only 64 respondents were included in the study, the total number of different professional Programs they represented was 79 (as some respondents represented multiple professions). Eight professions in total were represented in the study including Medicine, Nursing, Physiotherapy, Occupational Therapy, Respiratory Therapy, and Dentistry. Paramedics and Care Aides were also represented. There were more respondents representing Nursing than any other profession (75%). The next highest representation was of Paramedics (14%). Dentists were the least well-represented (3%). Counts and percentage of the total N for each Profession can be found in Figure A.1.1.a Level Respondents were asked to define their simulation utilisation by Level, which included either non-professional Undergraduate or Graduate training use, or Professional Development applications. Undergraduate programs that used simulations were comparatively well-represented (86%), while Professional Development (47%) and Graduate Level Programs (25%) were not as prevalent. Counts and proportion of the total N for each Level can be found in Figure A.1.1.b. Simulation Type Respondents were given the opportunity to identify the types of simulation (catagorized as Low, Intermediate or High Fidelity) that were in use by their institutions and in their programs. The most common Type of simulation used was Low Fidelity (77%), followed by High (52%), and Intermediate Fidelity (41%). Counts and percentage of total N for each Type can be found in Figure A.1.1.c. Profession, Level and Type All Medical, Occupational, Paramedic, Care Aide, and Dental Programs had Undergraduate Programs. The highest percentages of Graduate Programs were in Medicine, Physiotherapy, and Nursing (67%, 33%, and 25%, respectively). The prevalence of Professional Development Programs in each Profession ranged between 29% and 75%, except for Medicine for which respondents indicated 100%. For proportions of Undergraduate, Graduate, and Professional Programs using simulations in each Profession see Figure A.1.1.d. When type of simulation use by each Profession was analysed (low, medium or high fidelity), it was found that all Occupational Therapist, Respiratory Therapist, Care Aide, and Dental Programs used Low Fidelity simulations the most. Representatives of Medical, Paramedic, and Care Aide Professions reported the highest proportion of High Fidelity simulation use. Undergraduate and Professional Development Programs made the greatest use of Low Fidelity simulations, but respondents reported about half as much use of High Fidelity Simulations. Graduate Programs also used a high percentage of Low Fidelity Simulations, but utilised much less of the High Fidelity Type of simulations (55%, 59% and 24%, respectively, for Undergraduate, Professional Development, and Graduate Level). For percentages of use of Type of Fidelity for each Profession, see Figure A.1.1.e. Proportions of Type of Fidelity use for each Level appear Figure A.1.1.f. Efforts to Promote Simulation to Other Groups. Forty-eight of the 64 respondents indicated whether efforts had been made to promote simulation use to other groups. Responses indicated that 25 of the 48 Programs were promoting the use of simulations to other groups, while 23 were not.

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
16
Some examples of other groups to which simulations were being promoted were early national integration programs, occupational health and safety, and local agencies. Responses were too fragmented to divide by Profession, Level, and Type. For a full listing of other groups see Table A.1.1.
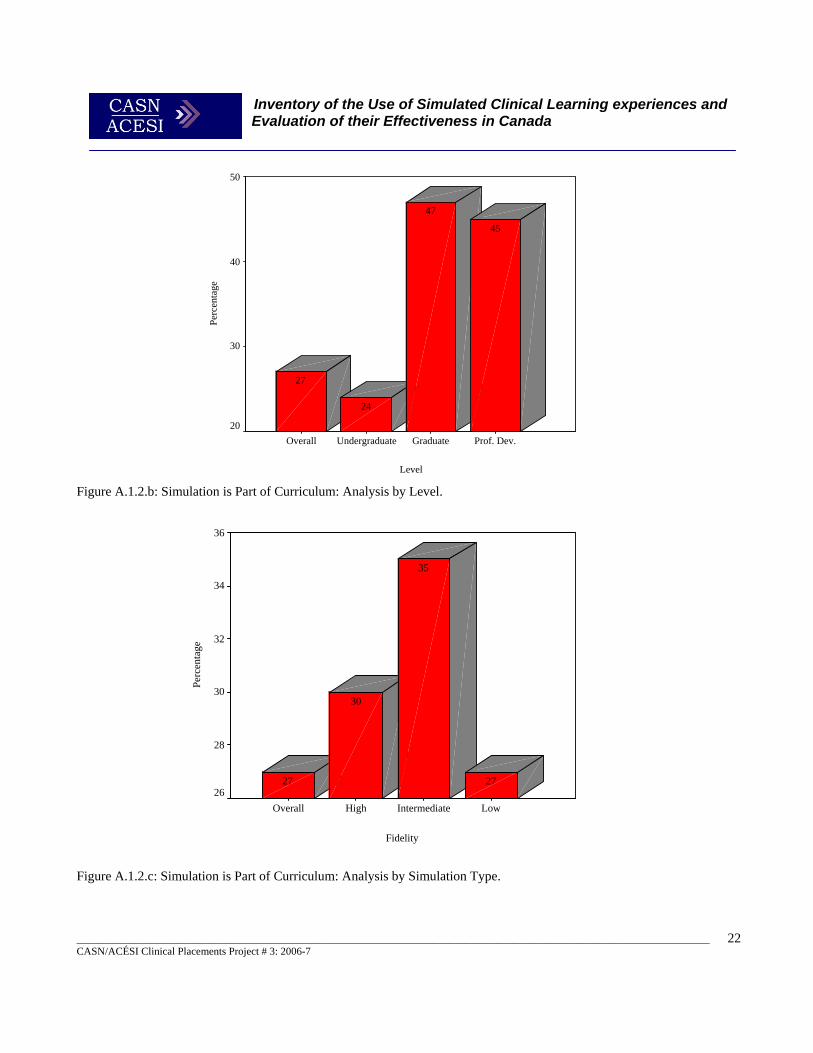
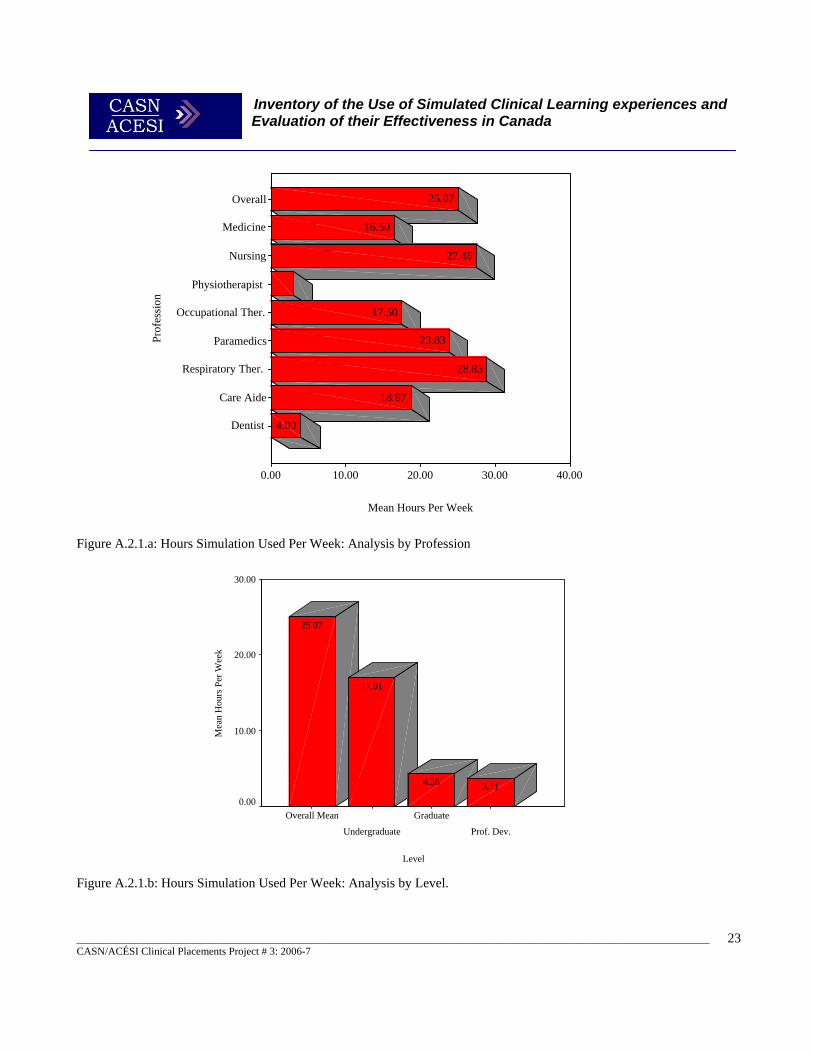
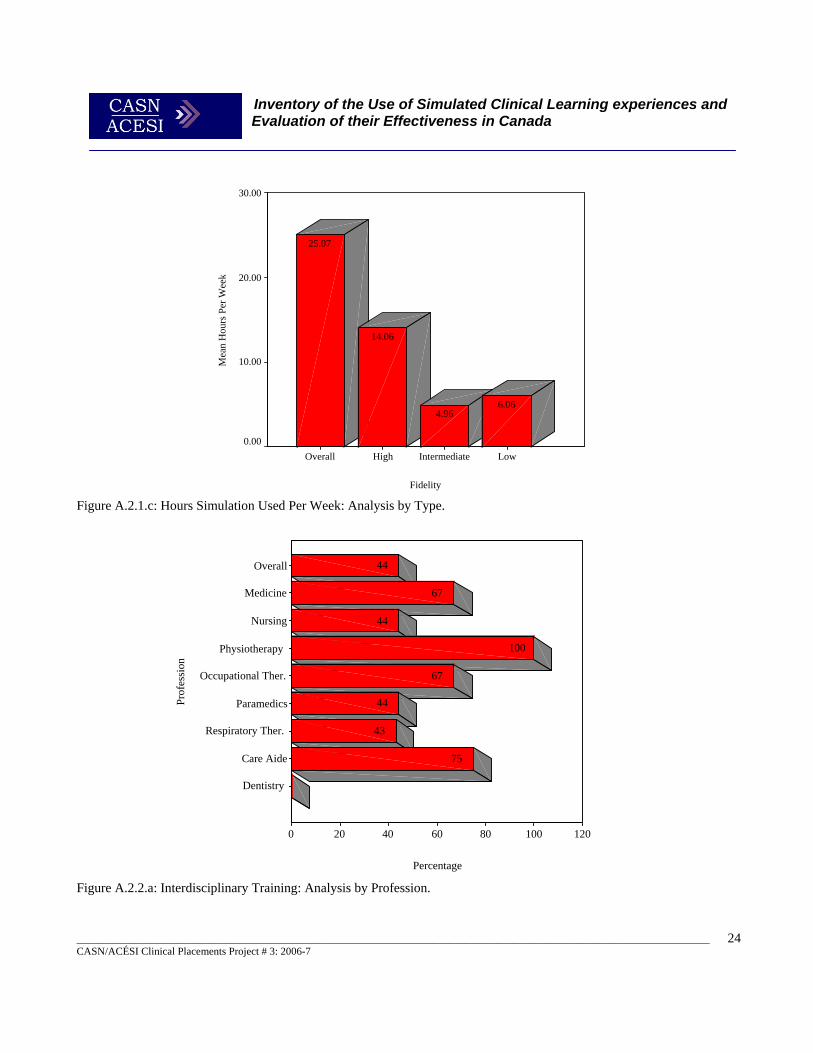
Simulation as a Formal Requirement of Programs Respondents from 17 of the 64 Programs represented (27%) indicated that simulations were used as a formal requirement in their curriculum. Physiotherapists used simulation for this purpose the most (76%). For most Professions, the percentage of reported use of simulations as a formal part of their curriculum ranged between 22-33%. An exception to this was Respiratory Therapists, Care Aides, and Dentists that did not use simulations at all in training Programs (See Figure A.1.2.a). Of the three Levels, Undergraduates used simulations almost half as much as Graduate and Professional Development Programs (See Figure A.1.2.b). Simulations were found to be a formal requirement more for Intermediate than for High and Low Fidelity users (See Figure A.1.2.c). Activities Supported By Simulation Activities supported by simulation were analysed by Undergraduate and Graduate Level, and Type of simulation used. Examples of such activities included competency evaluation, equipment testing, and certification maintenance. Differences in the use to which simulations were put can be seen between Undergraduate and Graduate Programs. Undergraduate Programs used simulations for such things as injections and transfer/lifts. Interestingly, Graduate Programs did not utilise simulations for these skills, possibly because Graduate students have already mastered these tasks. For a full listing of activities see Table A.2.1. Table A.2.2 provides percentages of use of simulations for each Type. For example, within Undergraduate Programs, 53.8% of users of High Fidelity employed simulations for competency evaluation, compared to 89.7% of users of Low Fidelity. Respondents from Graduate Programs reported some interesting differences between application of simulation by users of Low, Intermediate, and High Fidelity for neurological procedures. Users of Low Fidelity employed simulations for such procedures twice as much as users of Intermediate simulations, and four times as much as users of High Fidelity simulations. When this is compared to Undergraduate usage, users of Low Fidelity simulations used simulations only twice as much as users of Intermediate and High Fidelity simulations (see Table A.2.2). Simulation applications for the eight professions are in Table A.2.3, A.2.4 and A.2.5. These tables provide percentages for how much each Profession uses simulation for particular applications. Some notable variation between Professions and Levels was found. For example, Undergraduate Nursing Programs used simulation for competency evaluation almost three times as much as Graduate Nursing Programs did (69.8% and 25.6%, respectively). Undergraduate Occupational Therapists used simulation for certification maintenance four times as much as did Undergraduate Paramedics (100% and 25%, respectively). Percentages of simulation use for specific applications appear in Table A.2.4. Care Aide and Dental Programs did not use simulations for Graduate Level Programs. Dentists used simulations for a limited number of applications compared to Care Aide Programs in their Undergraduate Programs (See Table A.2.5). Hours per Week Simulations Used The overall mean number of hours simulation centres were used per week by different professions (M = 25.07) is given in Figure A.2.1.a. Simulation Programs for Nursing and Respiratory Therapists reflected the highest use. The least number of hours of use reported was by Physiotherapy Programs. Undergraduate Programs utilised over four times as many hours of simulations (M = 12.01) than Graduate or Professional Development Programs. The latter had similar hours of application per week. Mean hours per week of simulation usage by Undergraduate, Graduate and Professional Development Programs appear in Figure A.2.1.b. Users of High Fidelity employed simulations almost three times as much as users of Low or Intermediate Fidelity simulations (see Figure A.2.1.c).
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
17
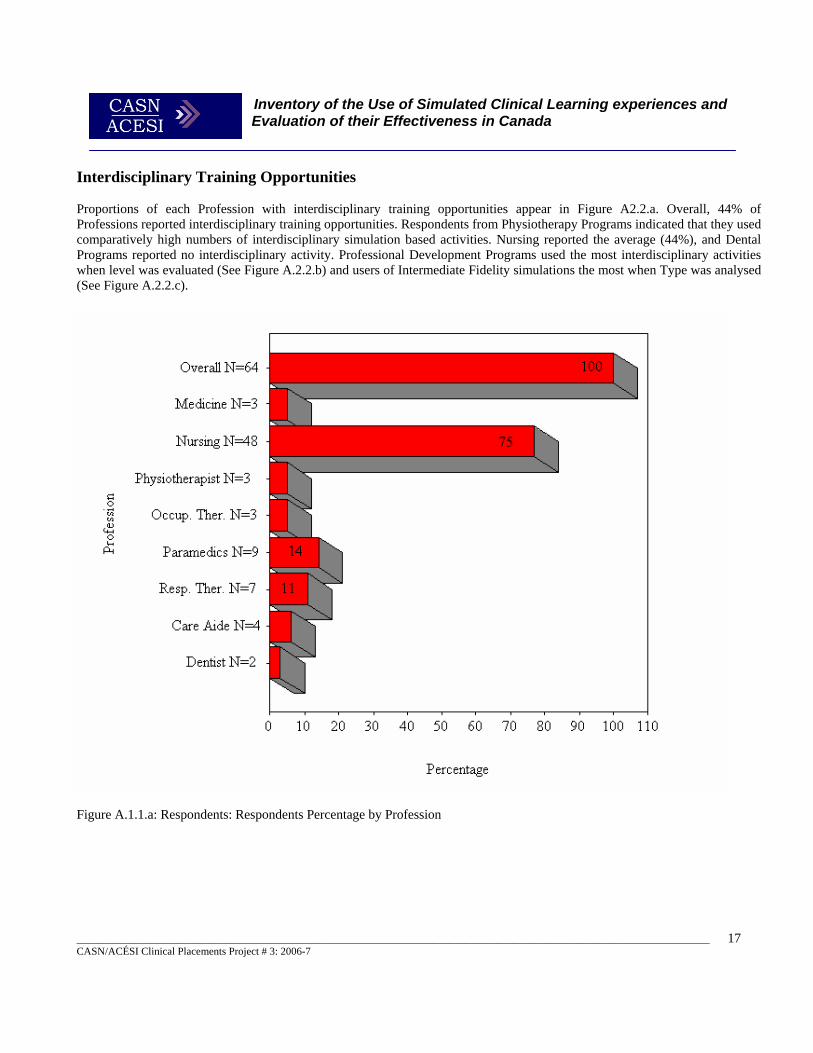
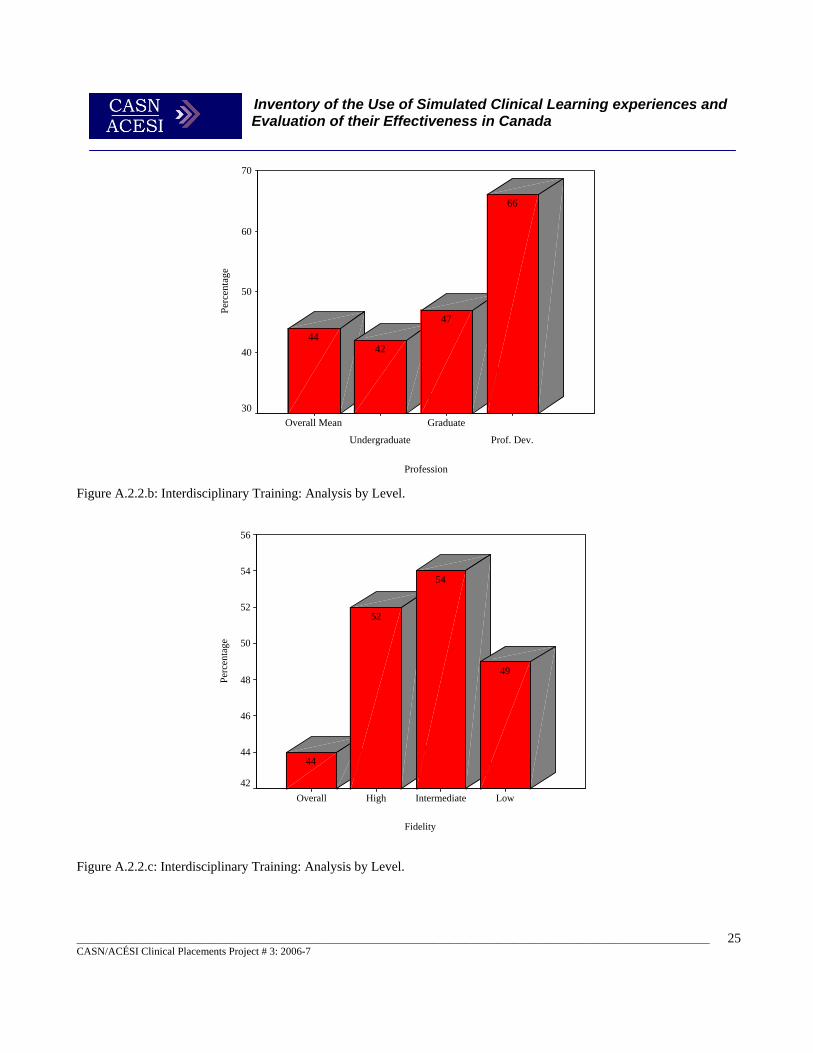
Interdisciplinary Training Opportunities Proportions of each Profession with interdisciplinary training opportunities appear in Figure A2.2.a. Overall, 44% of Professions reported interdisciplinary training opportunities. Respondents from Physiotherapy Programs indicated that they used comparatively high numbers of interdisciplinary simulation based activities. Nursing reported the average (44%), and Dental Programs reported no interdisciplinary activity. Professional Development Programs used the most interdisciplinary activities when level was evaluated (See Figure A.2.2.b) and users of Intermediate Fidelity simulations the most when Type was analysed (See Figure A.2.2.c).
Figure A.1.1.a: Respondents: Respondents Percentage by Profession
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
18
Figure A.1.1.b: Respondents: Percentage by Level.
Figure A.1.1.c: Respondents: Percentage by Type.
Leve
l
Overall N=64
Undergraduate N=55
Graduate N=17
Prof. Dev. N=29
Percentage
120100806040200
45
27
86
100Ty
pe
Overall N=64
High N=33
Intermediate N=26
Low N=49
Percentage
11010090807060504030
77
41
52
100
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
19
Prof
essi
on
Medicine
Nursing
Physiotherapy
Occupational Therapy
Paramedics
Respiratory Therapy
Care Aides
Dentists
Percentage
120100806040200
Undergraduate
Graduate
Professional Dev.
75
29
56
67
33
50
100
33
25
67
100
100
86
89
100
67
88
100
Figure A.1.1.d: Profession: Analysis by Level.
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
20
Prof
essi
on
Medicine
Nursing
Physiotherapy
Occupational Therapy
Paramedics
Respiratory Therapy
Care Aides
Dentists
Percentage
120100806040200
High
Intermediate
Low
100
100
78
100
67
79
67
100
50
57
44
67
38
67
75
57
67
33
33
54
67
Figure A.1.1.e: Profession: Analysis by Type.
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
21
Figure A.1.1.f: Respondents: Analysis of Level by Type.
Figure A.1.2.a: Simulation is Part of Curriculum: Analysis by Profession.
Undergrad. High
Undergrad. Int.
Undergrad. Low
Graduate High
Graduate Int.
Graduate Low
Prof. Dev. High
Prof. Dev. Int.
Prof. Dev. Low
Proportion of use of Type
100806040200
90
45
59
82
41
24
80
45
55Pr
ofes
sion
Overall
Medical
Nursing
Physiotherapy
Occupational Ther.
Paramedics
Respiratory Ther.
Care Aide
Dentist
Percentage
80706050403020100
22
33
67
27
33
27
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
22
Figure A.1.2.b: Simulation is Part of Curriculum: Analysis by Level.
Figure A.1.2.c: Simulation is Part of Curriculum: Analysis by Simulation Type.
Fidelity
LowIntermediateHighOverall
Perc
enta
ge
36
34
32
30
28
2627
35
30
27
Level
Prof. Dev.GraduateUndergraduateOverall
Perc
enta
ge
50
40
30
20
45
47
24
27
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
23
Level
Prof. Dev.
Graduate
Undergraduate
Overall Mean
Mea
n H
ours
Per
Wee
k
30.00
20.00
10.00
0.003.714.36
17.01
25.07
Figure A.2.1.a: Hours Simulation Used Per Week: Analysis by Profession Figure A.2.1.b: Hours Simulation Used Per Week: Analysis by Level.
Prof
essi
on
Overall
Medicine
Nursing
Physiotherapist
Occupational Ther.
Paramedics
Respiratory Ther.
Care Aide
Dentist
Mean Hours Per Week
40.0030.0020.0010.000.00
4.00
18.67
28.83
23.83
17.50
27.46
16.50
25.07
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
24
Fidelity
LowIntermediateHighOverall
Mea
n H
ours
Per
Wee
k
30.00
20.00
10.00
0.00
6.064.96
14.06
25.07
Prof
essi
on
Overall
Medicine
Nursing
Physiotherapy
Occupational Ther.
Paramedics
Respiratory Ther.
Care Aide
Dentistry
Percentage
120100806040200
75
43
44
67
100
44
67
44
Figure A.2.1.c: Hours Simulation Used Per Week: Analysis by Type. Figure A.2.2.a: Interdisciplinary Training: Analysis by Profession.
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
25
Profession
Prof. Dev.
Graduate
Undergraduate
Overall Mean
Perc
enta
ge
70
60
50
40
30
66
47
4244
Fidelity
LowIntermediateHighOverall
Perc
enta
ge
56
54
52
50
48
46
44
42
49
54
52
44
Figure A.2.2.b: Interdisciplinary Training: Analysis by Level. Figure A.2.2.c: Interdisciplinary Training: Analysis by Level.

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
26
A couple of themes in this area emerged from the open ended question responses, focus group interviews and site visits. Frequently inconsistent terminology was used when discussing the level of fidelity of simulation. For example:
“We just recently got a high definition simulator…” “Our partners both X and Y Universities both have high and low tech, that’s how you probably call it…” “From my perspective, we mostly use it for the psychomotor skills development and have limited uses for communication skills. What I consider moderate fidelity there’s limited interactions.”
“We have 2 high fidelity, we call high fidelity, the other person called them moderate fidelity SimMan®.”
One clear theme was the increase in perceived need for high-fidelity simulation to support clinical practical education. High-fidelity simulation appeared to be consistently valued in all professions:
“Any faculty who will be using our low-fidelity simulators, are coached on the capabilities and given an opportunity to work with it prior to classes. Our plan for introduction of HPS® systems is to have instructional sessions for any faculty involved with using the simulators.” “We have very limited simulation tools in house and have to use external high fidelity settings. the access to intermediate fidelity tools is limited by resource allocation priorities.” “Only low-fidelity available; we require new labs with high- and intermediate-fidelity simulation tools.” “Curriculum changes are taking place and we are hoping to develop new lab resources including high fidelity simulators.” “High fidelity and additional intermediate is needed.” “There are a range of scenarios used in our OT and PT programs. Other programs at the University also use simulation e.g.: Dentistry has high fidelity equipment.”
When asked about the value of these resources for interdisciplinary education there was an overall consensus that this is a good use of these techniques and technology. Some centres were already running inter-disciplinary simulation sessions, and this was common practice in aircrew and military healthcare personnel training.
“I see so much opportunity it’s just coordinating all of these disciplines, bring their timetables together. Figure out what is the learning objectives you want in that scenario but, you could bring in nursing students RTs, physicians, all kinds of people. It doesn’t even have to be just the teachers you could do a community home environment focus as well. There is a huge opportunity; it’s just the planning part that has to happen first.” “Its just the logistics that are challenging to work out. But when I watch the people who have been renting the simulator, that’s exactly what they’re doing, that’s bringing in people from different fields who have to work together in different situations and they’re practicing working together as a team.”
“A lot of places already do that, involving their paramedics and their firefighters and policemen. We are

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
27
looking at that because I think there is a real need for that and I think it will help the people having a better understanding of what each one’s role is and hopefully if we know that and look at our inter-professional people and how we all work together and get a clear understanding with the students working in a common simulated experience and hopefully in the future will see that there is a better understanding what each group of people do, what services we do provide, how we can work together and it should in the long term make it better for the public because the more we know about each other the better that will be. And we are planning on doing something like that on this campus.”
B. Types of Simulation Use and Access Respondents were asked who and what they used their simulations for. These were categorised in terms of Medical Simulation Users, Nursing Simulation Users or Other Users. The total number of Typical Users of Simulations split by these categories appears in Figure B.1.1. Nursing users made up the bulk of simulation users in the survey, mainly due to the large proportion of Nursing Programs represented. Nursing Program users accounted for 222 of 354 of users of simulations (63%). The largest single group of users of Nursing Program simulations were Undergraduate Students (40 of the 48 Nursing Programs). This was followed by Acute Surgical Nurses (N = 18), Acute Medical Nurse (N = 17), and CCU Nurses (N = 17). Responses were divided into
• Medical Users by Simulation Fidelity (See Figure B.1.2 below and Table B.1.1 in Appendix E) and by Level (See Figure B.1.3 below and Table B.1.4 in Appendix E),
• Nursing Users by Simulation Fidelity (See Figure B.1.2 below and Table B.1.2 in Appendix E) and by Level (See Figure B.1.3 below and Table B.1.5 in Appendix E), and
• Other Users by Simulation Fidelity (See Figure B.1.2 below and Table B.1.3 in Appendix E) and by Level (See Figure B.1.3 and Table B.1.6).
Table B.1.1 in Appendix E gives the actual numbers and percentages for Medical users of simulations, analysed by Type of use (low, intermediate or high fidelity). Forty-three percent of Medical users of Intermediate Fidelity simulations were Undergraduate students, whilst only ten-percent of Medical users of Low Fidelity simulations were ER Residents. Most doctor and resident pairings showed identical simulation type use patterns. For example, anaesthetists and anaesthesia residents both represented exactly the same proportions amongst high, intermediate, and low fidelity groups. One variation from this pattern was evident among ER physicians and ER residents where ER residents use higher proportions of all simulation types than ER physicians. Table B.1.2 in Appendix E gives total numbers and percentages analysed by Type of use for Nursing users of simulations. Substantial percentages of Nursing users of all types of simulation were Undergraduate students (93% of 43 Nursing Programs reporting) followed by Acute Medical Nurses (40%), Acute Surgical Nurses (42%) and Cardiac Care Unit (CCU) Nurses (40%), see Figure B.1.4. Table B.1.3 gives numbers and percentages by Type for Other users of simulations. Approximately 22% of Other Users were respiratory therapists, and paramedics were also well-represented in this group. Variations amongst Users of Simulations were more pronounced by Level than when usage is compared by type. Medical simulation use was highest in undergraduate education, then continuing professional development, followed by least use in graduate programs. This user profile was also similar for both Nursing and Other users. Table B.1.4 in Appendix E provides numbers and percentages for Medical users analysed by Level of User. Overall, 23 out of 64 Medical users of simulation (36%) were Undergraduate students. Table B.1.5 in Appendix F also shows the numbers and percentages for Nursing users explored by Level of user, and Table B.1.6 in Appendix F shows numbers and percentages of Other Users of simulations analysed by Level of User. Thirty-one percent of Other Users of simulation in Professional Development
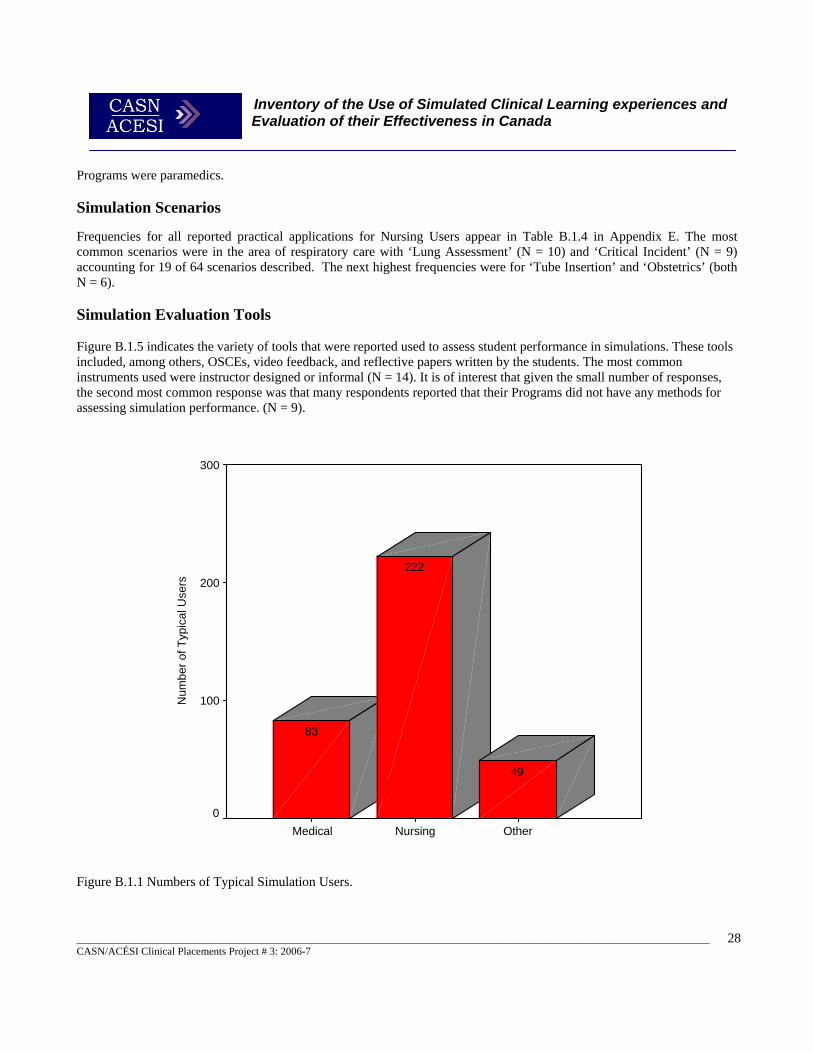
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
28
OtherNursingMedical
Num
ber o
f Typ
ical
Use
rs
300
200
100
0
49
222
83
Programs were paramedics. Simulation Scenarios Frequencies for all reported practical applications for Nursing Users appear in Table B.1.4 in Appendix E. The most common scenarios were in the area of respiratory care with ‘Lung Assessment’ (N = 10) and ‘Critical Incident’ (N = 9) accounting for 19 of 64 scenarios described. The next highest frequencies were for ‘Tube Insertion’ and ‘Obstetrics’ (both N = 6). Simulation Evaluation Tools Figure B.1.5 indicates the variety of tools that were reported used to assess student performance in simulations. These tools included, among others, OSCEs, video feedback, and reflective papers written by the students. The most common instruments used were instructor designed or informal (N = 14). It is of interest that given the small number of responses, the second most common response was that many respondents reported that their Programs did not have any methods for assessing simulation performance. (N = 9). Figure B.1.1 Numbers of Typical Simulation Users.
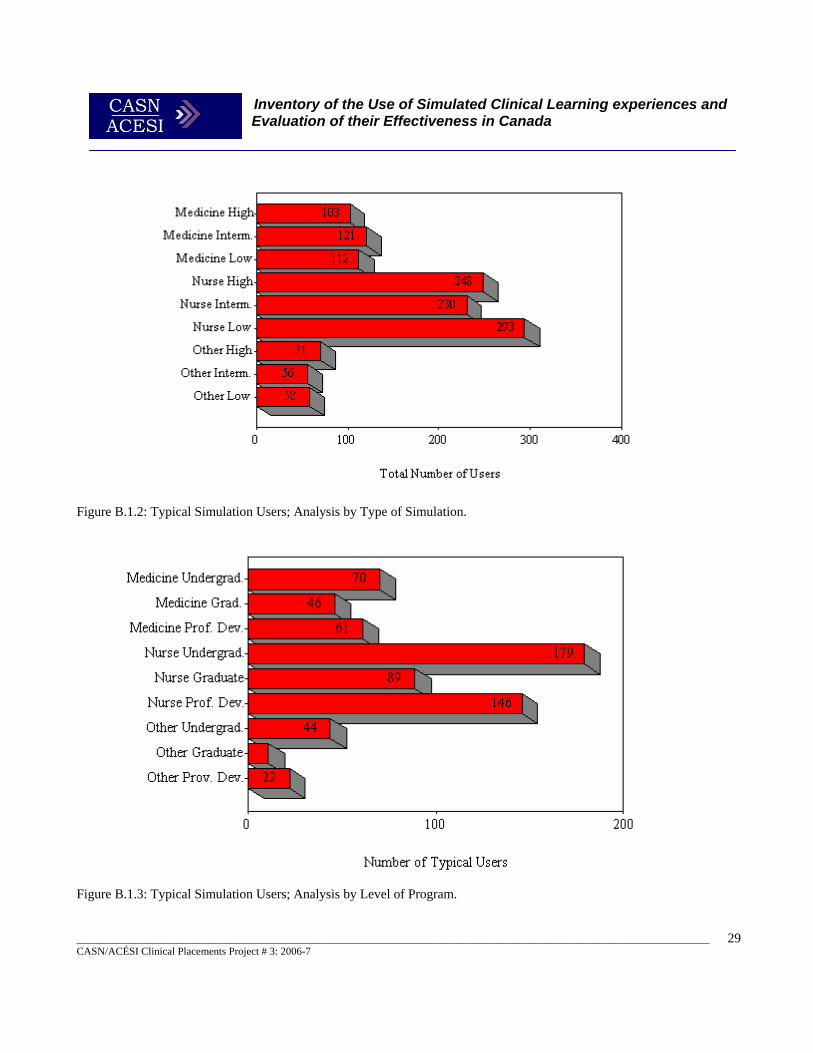
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
29
Figure B.1.2: Typical Simulation Users; Analysis by Type of Simulation. Figure B.1.3: Typical Simulation Users; Analysis by Level of Program.
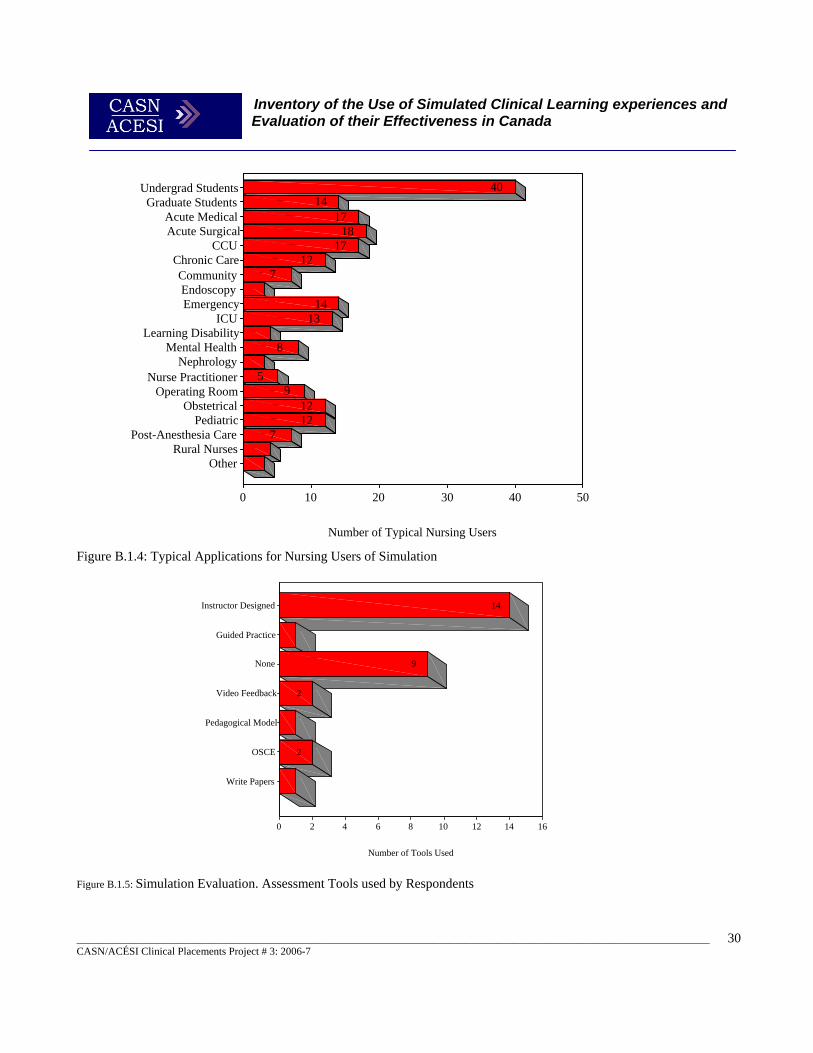
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
30
Instructor Designed
Guided Practice
None
Video Feedback
Pedagogical Model
OSCE
Write Papers
Number of Tools Used
1614121086420
2
2
9
14
Figure B.1.4: Typical Applications for Nursing Users of Simulation Figure B.1.5: Simulation Evaluation. Assessment Tools used by Respondents
Undergrad StudentsGraduate Students
Acute MedicalAcute Surgical
CCUChronic CareCommunityEndoscopyEmergency
ICULearning Disability
Mental HealthNephrology
Nurse PractitionerOperating Room
ObstetricalPediatric
Post-Anesthesia CareRural Nurses
Other
Number of Typical Nursing Users
50403020100
71212
95
8
1314
712
1718
1714
40
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
31
More themes in this area emerged from the open ended question responses, focus group interviews and site visits. The use of high-fidelity simulation to simulate high-acuity critical incidents, new procedures or procedures with a high-risk of injury or failure was a recurring theme. The Air Canada simulation Centre use equipment failures or emergences taken from real-life events in most simulation sessions. The Trauma Training Centre also focuses on simulations based on the very latest combat casualties that they have experienced. Their instructors rotate through active deployment in-between returning to the centre. They then use direct experience of the situations they have been exposed to in order to recreate authentic simulations to prepare military health care personnel (Doctors, Nurses, Medical Technicians and Physicians Assistants).
“…see how it works the first time not with real people. Given that, we deal with very vulnerable populations and we’re dealing with very high acute stuff. So I would like to be able to do that in a simulation area, before doing it for real.”
“We use simulation to expose students to high risk, low incidence events. To give all students equal opportunity to care for specific patient concerns/situations. To expose students to emergency situations, where in clinical practice they would be side lined or removed from the situation.” “We did develop a scenario for high risk care with nursing students last spring around blood transfusion reactions.”
A few areas reported using low-fidelity computer-based simulations in their education programs e.g. computer interactive simulations. Two centres identified that although they had this type of resource, they were limited by licensing and internet bandwidth in their ability to make them more widely available.
“The access to low fidelity tools is limited by the number of computers available in the organization and the lack of a multi-media server for our intranet.”
There were many similarities in the use of simulation between different health care professions, and some disagreement of the best use of high fidelity simulation. Many centres reported using simple simulation for psycho-motor clinical skills training, and most that did so also used high fidelity simulators for more advanced skills training in this domain.
“Early technical skills and eye-hand coordination are routinely taught using dental simulators.” "We mostly use it for the psychomotor skills… We use primarily behaviorally driven types of learning for students. Step by step for the psychomotor skills…” “Specific tasks could benefit from simulations. That would help developing more secure techniques.” “We use simulation for technical programs - airway management, crico-thyroid puncture, IV access…” “Mainly it [simulation] allows the user to develop the psycho-motor skills needed to do the procedure the right way and gain confidence executing the procedure. “ “Predominantly we use it [high-fidelity simulation] for clinical skills and overall assessment and then the follow-through. I think it allows them to do the assessment of the patient and I think it does also assist them in the process of critical thinking.” “From my perspective, we mostly use it [simulation] for the psychomotor skills development and have limited uses for communication skills.”

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
32
“We use the high fidelity SimBaby® for them [midwifery students] to do vitals and neonatal assessment on.” “My experience is that for actual skills: insertion of tubes its use [high-fidelity simulation] is minimal, other than for assessments. For technical skills like insertion, it doesn’t give you the environment for that.”
Many sites also reported a move towards using simulation in helping develop more complex practice skills such as teamwork and communication skills.
“I really think there is going to be a bigger approach to use it not only to develop psychomotor skills but the decision making and the communication skills.”
“I think its [simulation] for everything: decision making, clinical skills, communicating with clients or other staff.” “Although in 1st year we use simulation a lot for psychomotor skill development, in 2nd year in both programs it is more for decision making, cognitive skills and communication and looking into developing some mental health scenarios where the prime factor they would be learning would be communication.” “People have to have practice their communication skills, decision making, work together as a team and the whole complex skills altogether as well as some clinical skills.”
“The community has expressed an interest in using simulation to build team skills as well as to master proficiency in clinical skills.” “It improves critical thinking skills including decision making troubleshooting, negotiation, and improves teamwork skills such as leadership and communication.” “We can simulate a difficult communication issue [with high-fidelity simulators].”
Team building was seen as particularly valuable use of these techniques and technologies.
“The community has expressed an interest in using simulation to build team skills as well as to master proficiency in clinical skills” “I see the gross potential really being in the interaction piece the assessment, the judgment and the team interaction. And I really like the idea of recording where the team can afterward look at how it worked, how they functioned. “ “I think more and more in the health care field we see a movement here on the West Coast toward team development as far as managing health care, in-patient and out-patient. And simulation is one way we can facilitate that.”
Several areas, particularly those supporting medical education, used SPs as their main use of simulation for developing these higher-order skills. For example the McGill Medical Simulation Centre made extensive use of SPs with its undergraduate medical students. The Trauma Training Centre used actors in its Field Hospital simulations, but a high-

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
33
fidelity simulator for the actual client. For normal and easily mimicked conditions SPs provided excellent functionality in this area, whilst for more difficult to simulate physiological conditions the high-fidelity simulators came into their own.
“Standardized patients simulate normal changes and psychosocial communication skills.” “We will be using the simulators with our standardized patient program.”
The majority of centres used simulation for practicing acute medical-surgical procedures, but also several used simulation in other settings such as to recreate hospital or community clinical environments.
“We also use simulation to orientate learners and faculty to newly acquired settings - clinics, community etc.”
Some sites found great value in simulating the particular health care environment for students early in their educational programs before they went into actual practice. In this way they could acclimatise their students as to what to expect in the clinical environment. The Air Canada Simulation Centre uses this practice in training aircrew for new aircraft types. Great effort is taken to produce an ultra-high-fidelity copy of the aircraft cockpit in the simulator so flight crew students become acclimatised to the environment, including alarms and noises before they operate in the real aircraft. The Vancouver Trauma Training Centre uses a similar approach, making their Field Hospital (surgical units) simulations as realistic as possible. This includes having camouflage netting hung around, identical equipment found in the field present and taped sound effects (e.g. helicopters, gunfire) and also using actors to simulate various non-medical personnel (e.g. stressed officers or other military personnel). The following comment from a School training nurses, physiotherapists (PT) and occupational Therapists (OT) illustrates this point.
“We have been using our sim labs with our OTs and PTs as well as nursing and we found it very helpful with our OTs students in orienting them in a clinical setting. Most of them have never set foot in an hospital before so we have run a couple of orientation sessions just to get them to get used to what it would be like to walk into an hospital setting, with all the bells and whistles going off, and have an opportunity to figure out how to work the beds and look at all the equipment and things, before they actually get in and start messing around with real patients. They found that really helpful in boosting their confidence.”
Access to simulation technology was also noted as an issue by several of the respondents, and this is a theme also evident in Section D. Several respondents noted they had limited access to high-fidelity simulation technology because of the cost, or that its use was outside of their control.
“We have very limited simulation tools in house and have to use external high fidelity settings. the access to intermediate fidelity tools is limited by resource allocation priorities.” “We really support the incorporation of higher fidelity simulation into our program, but as yet, the cost has been prohibitive. We will venture into this within the year.” “We need to borrow task trainers (i.e. palpation models for Leopold's Maneuvers) from other departments. We have none of the intermediate- or high-fidelity simulation tools that our students need.” “Only low-fidelity available; we require new labs with high- and intermediate-fidelity simulation tools.”
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
34
“We have 1 sim lab currently very heavily physician controlled and design to meet the needs of the physician trainees.” “Our labs are only equipped with low-fidelity simulators for basic nursing skills. FYI - the labs in many Ontario Schools of Nursing are better equipped than some of the clinical placement agencies in Nova Scotia.”
The improvements in the technology arose as a consistent theme amongst respondents. Whilst the improvements in high-fidelity simulation were seen as valuable, there was consensus that we are at an early stage of development in this field. Compared to aircrew training where equipment can be simulated so it is indistinguishable from the real thing (in many cases it is the actual equipment) the simulation of human physiology and interaction is a far more complex undertaking.
“Still not as real life as we would like it to be, we’re getting there. And some of the assessments on the manikin aren’t quite landmark in the right position, pulses may be hard to find so the technical aspects are not as refine as a real human being. And I guess we’re getting spoil in technology because we are expecting that already. So students having used all other kinds of technology that’s so wonderful kind of go wow, it’s just plastic.” “It enhances the learning, it allows for certain styles of learners to be more engaged I think so students find technology fascinating.” “Even if we have the technology, it is more important to teach them how to think- It is a question that is closely monitored right now especially in the paramedical and medical fields.” “There is more communication involved with the high fidelity simulators because we have the ability to talk on the fly for that. I bought a voice modulator so that my voice can be male or female.” “One of the most useful features they have added is the ability to remotely talk for the mannequin, and the voice come from the patient. Vocalizing for the patient enables us to run real-time interactive simulations with an added dimension of realism. The technology and interface is improving all the time”
A range of other low-fidelity activities were also reported using classroom exercises for such things as role-play for communication skills, and simulated management exercises.
“We often use simple classroom based role-play to simulate communication skills, such as breaking bad news.” “We have used simulations in the classroom in management exercises and for managing aggression.”
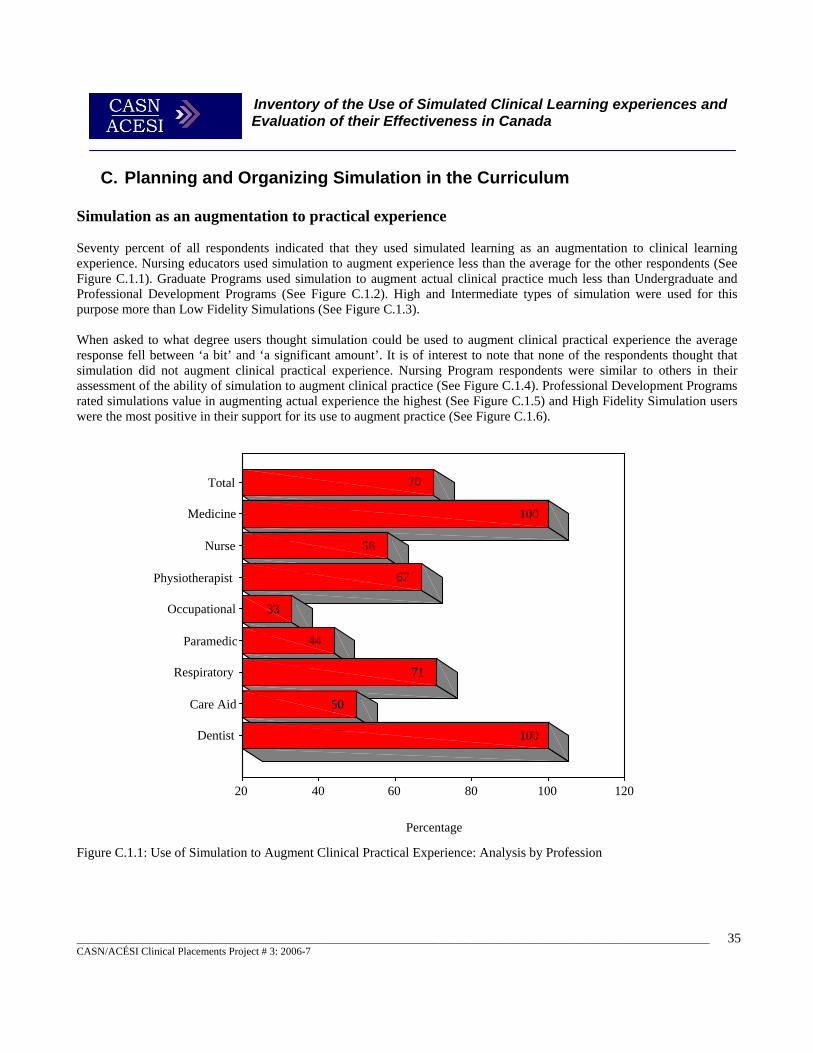
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
35
C. Planning and Organizing Simulation in the Curriculum Simulation as an augmentation to practical experience Seventy percent of all respondents indicated that they used simulated learning as an augmentation to clinical learning experience. Nursing educators used simulation to augment experience less than the average for the other respondents (See Figure C.1.1). Graduate Programs used simulation to augment actual clinical practice much less than Undergraduate and Professional Development Programs (See Figure C.1.2). High and Intermediate types of simulation were used for this purpose more than Low Fidelity Simulations (See Figure C.1.3). When asked to what degree users thought simulation could be used to augment clinical practical experience the average response fell between ‘a bit’ and ‘a significant amount’. It is of interest to note that none of the respondents thought that simulation did not augment clinical practical experience. Nursing Program respondents were similar to others in their assessment of the ability of simulation to augment clinical practice (See Figure C.1.4). Professional Development Programs rated simulations value in augmenting actual experience the highest (See Figure C.1.5) and High Fidelity Simulation users were the most positive in their support for its use to augment practice (See Figure C.1.6).
Figure C.1.1: Use of Simulation to Augment Clinical Practical Experience: Analysis by Profession
Total
Medicine
Nurse
Physiotherapist
Occupational
Paramedic
Respiratory
Care Aid
Dentist
Percentage
12010080604020
100
50
71
44
33
67
58
100
70
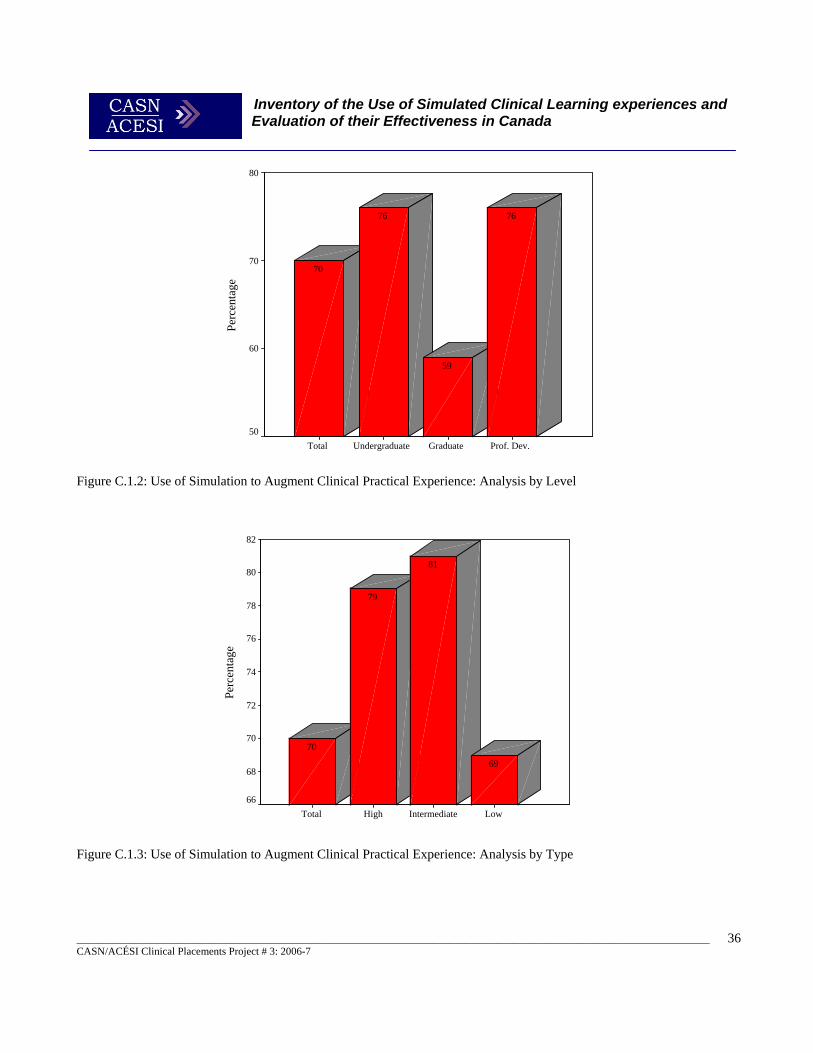
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
36
Prof. Dev.GraduateUndergraduateTotal
Perc
enta
ge
80
70
60
50
76
59
76
70
Figure C.1.2: Use of Simulation to Augment Clinical Practical Experience: Analysis by Level
Figure C.1.3: Use of Simulation to Augment Clinical Practical Experience: Analysis by Type
LowIntermediateHighTotal
Perc
enta
ge
82
80
78
76
74
72
70
68
66
69
81
79
70
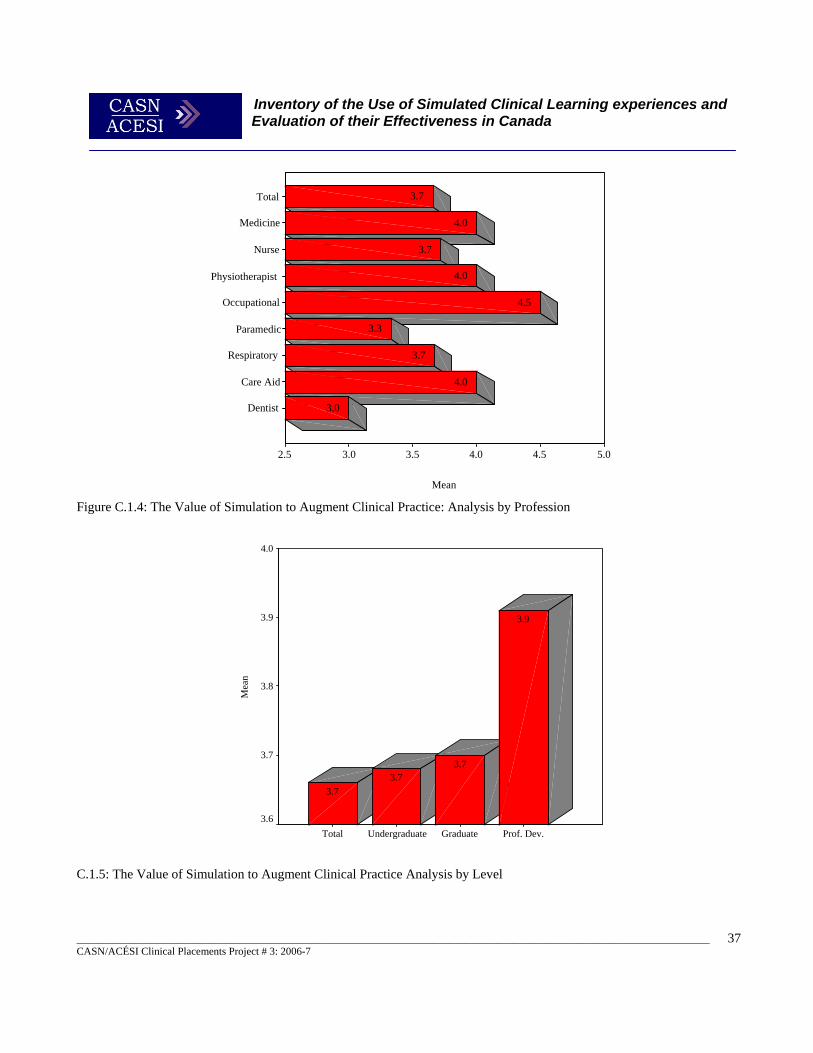
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
37
Figure C.1.4: The Value of Simulation to Augment Clinical Practice: Analysis by Profession
C.1.5: The Value of Simulation to Augment Clinical Practice Analysis by Level
Total
Medicine
Nurse
Physiotherapist
Occupational
Paramedic
Respiratory
Care Aid
Dentist
Mean
5.04.54.03.53.02.5
3.0
4.0
3.7
3.3
4.5
4.0
3.7
4.0
3.7
Prof. Dev.GraduateUndergraduateTotal
Mea
n
4.0
3.9
3.8
3.7
3.6
3.9
3.73.7
3.7
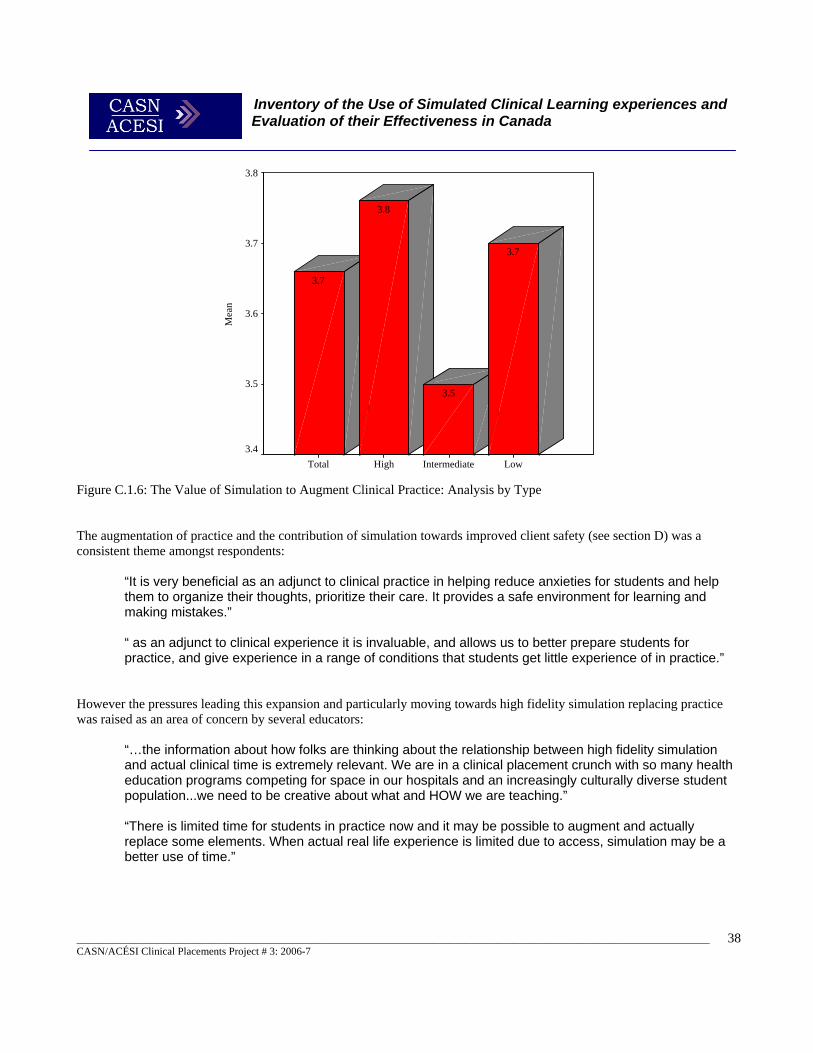
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
38
Figure C.1.6: The Value of Simulation to Augment Clinical Practice: Analysis by Type The augmentation of practice and the contribution of simulation towards improved client safety (see section D) was a consistent theme amongst respondents:
“It is very beneficial as an adjunct to clinical practice in helping reduce anxieties for students and help them to organize their thoughts, prioritize their care. It provides a safe environment for learning and making mistakes.” “ as an adjunct to clinical experience it is invaluable, and allows us to better prepare students for practice, and give experience in a range of conditions that students get little experience of in practice.”
However the pressures leading this expansion and particularly moving towards high fidelity simulation replacing practice was raised as an area of concern by several educators:
“…the information about how folks are thinking about the relationship between high fidelity simulation and actual clinical time is extremely relevant. We are in a clinical placement crunch with so many health education programs competing for space in our hospitals and an increasingly culturally diverse student population...we need to be creative about what and HOW we are teaching.” “There is limited time for students in practice now and it may be possible to augment and actually replace some elements. When actual real life experience is limited due to access, simulation may be a better use of time.”
LowIntermediateHighTotal
Mea
n
3.8
3.7
3.6
3.5
3.4
3.7
3.5
3.8
3.7

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
39
Total
Medicine
Nurse
Physiotherapy
Occupational
Paramedic
Respiratory
Care Aid
Dentist
Mean
4.03.53.02.52.01.51.0
2.5
2.3
2.8
2.5
1.7
1.3
2.3
3.5
2.4
Simulation as a replacement for practical experience Only seven out of 64 (11%) respondents indicated that they currently used simulation as an alternative to clinical practical experience. No respondents reported that they completely replaced any practical experiences with simulation, and the hours replaced ran from 8 to 40 hours per program. Six respondents (9%) indicated that the mean number of hours of clinical practical experience replaced by simulation was 12.5 hours. Of the few that did replace practice with simulation, most reported using simulation to replace less than two days of actual practical experience. Respondents were also asked to what degree they thought simulation could be used to replace clinical practical experience, and were given five choices ranging from ‘none’ ‘to a large degree.’ It is of interest to note that none of the respondents indicated ‘to a large degree’ and 21% of respondents stated “none.” The overall mean was 2.4, this indicated a score about midway between ‘somewhat’ and ‘a bit.’ Medical educators gave simulation the highest rating in their perception of its ability to replace practice out of all the professions (See Figure C.2.1.a), and ranked this between ‘a bit’ and ‘a significant amount’. When categorized by level of use Professional Development educators gave simulation the lowest rating for its ability to replace clinical practical experience (See Figure C.2.1.b). Intermediate Fidelity Programs gave simulation the highest rating for its ability to replace clinical experience (See Figure C.2.1.c). Details of the types of experience replaced by simulation can be found in Figure C.2.2, although responses were sparse. Examples include ‘Central Line Access Skill Certification’ and ‘Yearly Skills Maintenance’. Ways in which simulation can replace clinical practical experience appear in Table C.2.3. Example include ‘Integrate/Upgrade Knowledge Base’, Improve Clinical Reasoning/Judgement/Critical Thinking’, “Provide Training in Skills where there is Limited Clinical Access,” “Build Confidence,’ and “Meeting Licensing Requirements”. It is of note that 13 (32%) of 41 respondents did not think that simulation could replace clinical practical experience at all. Figure C.2.1.a: The Value of Simulation to Replace Clinical Practice: Analysis by Profession
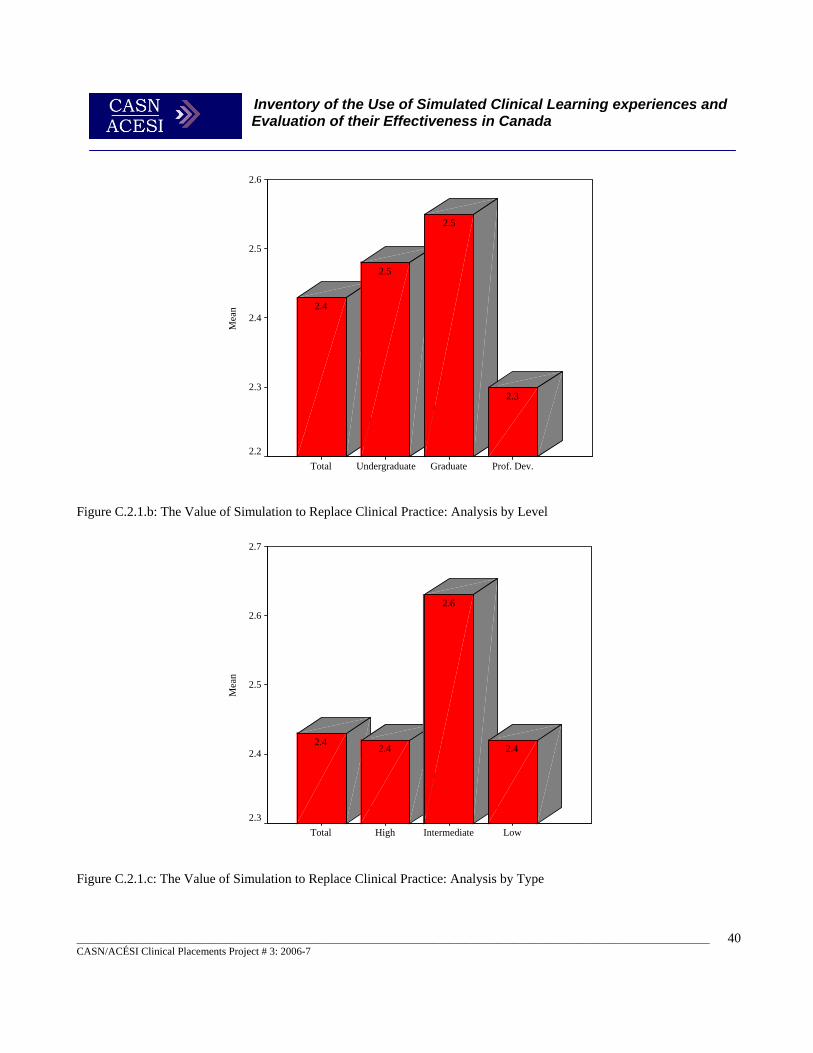
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
40
Figure C.2.1.b: The Value of Simulation to Replace Clinical Practice: Analysis by Level Figure C.2.1.c: The Value of Simulation to Replace Clinical Practice: Analysis by Type
LowIntermediateHighTotal
Mea
n
2.7
2.6
2.5
2.4
2.3
2.4
2.6
2.42.4
Prof. Dev.GraduateUndergraduateTotal
Mea
n
2.6
2.5
2.4
2.3
2.2
2.3
2.5
2.5
2.4
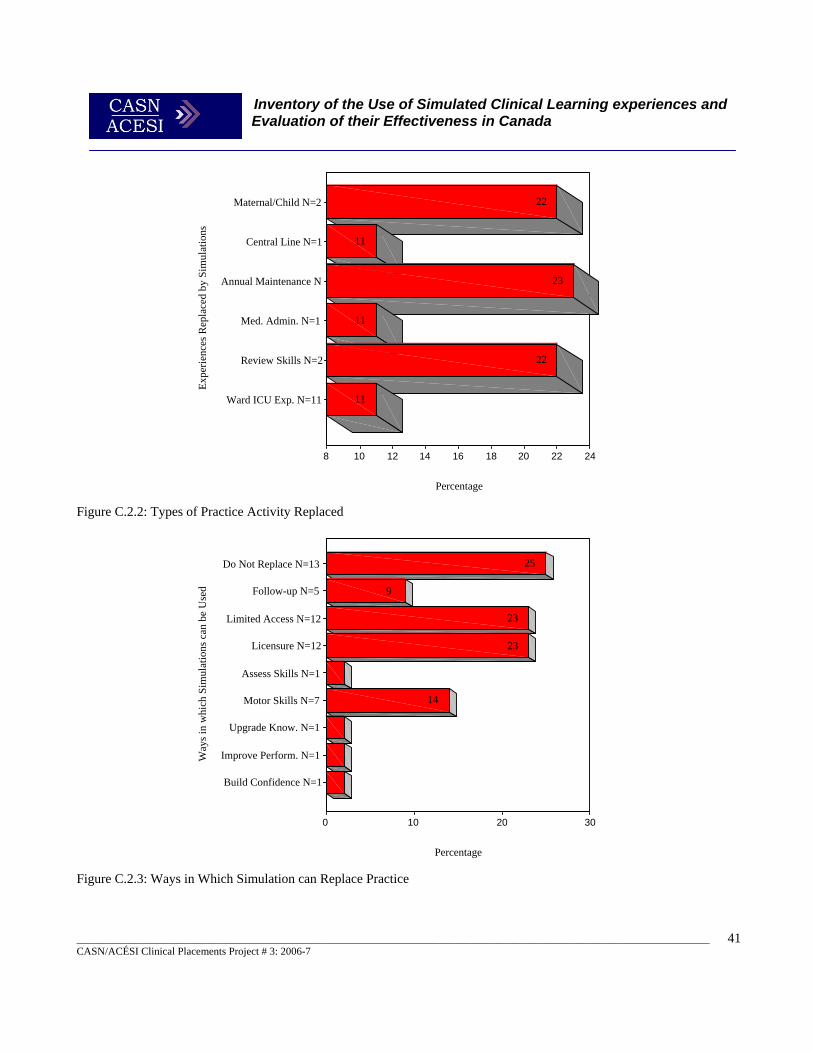
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
41
Way
s in
whi
ch S
imul
atio
ns c
an b
e U
sed
Do Not Replace N=13
Follow-up N=5
Limited Access N=12
Licensure N=12
Assess Skills N=1
Motor Skills N=7
Upgrade Know. N=1
Improve Perform. N=1
Build Confidence N=1
Percentage
3020100
14
23
23
9
25
Expe
rienc
es R
epla
ced
by S
imul
atio
nsMaternal/Child N=2
Central Line N=1
Annual Maintenance N
Med. Admin. N=1
Review Skills N=2
Ward ICU Exp. N=11
Percentage
24222018161412108
11
22
11
23
11
22
Figure C.2.2: Types of Practice Activity Replaced Figure C.2.3: Ways in Which Simulation can Replace Practice

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
42
The idea of simulation being used to replace practical elements of programs was a controversial issue. It raised a range of responses in the focus groups and open-ended responses. The majority of responses was critical of such a move and suggested that this would be a retrograde step for health care professional education:
“I see simulation as an adjunct to clinical practice but not a replacement for it. I believe that simulation is useful for certain early phases of the learning process but not application.” “I think the faculty and the nursing clinical educators don’t think it is as valuable as the real thing and neither do I. So it shouldn’t be a replacement, although in terms of remedial or missed clinical time I think it has great value there. “ “I would not really want to see simulation completely replace clinical in any way, I think it is a very good way to augment and support what’s being done in a clinical setting but I don’t think we’ll ever see it so much as a real replacement because there is just something that happens that, no matter how good your sim lab is, there are just some things that you just absolutely can’t do in that kind of an environment where people actually need to be in the real clinical setting.”
Elements that were considered difficult for simulation to replace by nursing educators included psycho-social and spiritual dimensions of care, and professional socialization.
“I think one of the pieces that is missing having simulation instead of clinical experiences is the emotive and relational pieces missing in the sim manikins. So I don’t think it can ever replace the real life scenarios.” “One of the things that concerns me is the whole socialization of students into their professional roles and that is something that I think is somewhat difficult to engage in a simulation lab.” “The only way it can replace clinical practical experience is in the development of specific skills such as enemas, catheterization, wound care etc.; cannot anticipate the complexity of real life patient/family interactions.”
There were however, also several positive responses in this area suggesting that there were some areas that simulation could replace some elements of practical experience, and in some fields is already doing so:
“We teach in BSN and LPN programs with those and we have developed scenarios for a variety, probably about 8, COPD, post-op assessment, a diabetic client with ulcers, hypoglycemic reactions. That was one that was to replace a clinical experience that was missed.” “My experience in watching it is that I think it could be the equivalent of, and we need to determine what’s a good balance, what’s the equivalency I am not even saying 50% but I think it could probably be 10 or 20% [replacement]. Just because you can create such a rich learning environment in a simulated environment where basically every minute of that 2-3 hours whatever you want to create is a learning opportunity and every minute of a 3 hours situation on a hospital unit might not be a learning opportunity. …If you want to go minute by minute, we probably get a better bang for our buck in a simulation environment.” “A 10 to 20% replacement of practice. I think I would be comfortable with that.”
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
43
The site visits to other professional centres revealed different practices in this area. For example The Air Canada Simulation Centre uses simulation extensively to replace actual air-time when converting pilots to different aircraft types. Over 95% of their conversion time is spent in the simulator. However, although these are ultra-high fidelity full-motion simulators virtually indistinguishable from the real aircraft, human simulators have yet to reach that level of sophistication. However, they did also use simulation extensively for crew resource management and other inter-disciplinary activities.
“Line Oriented Flight Training- The “LOFT” concept is that everything will happen as the result of a series of various events. And it is this series of events that will be built into a real-life scenario. You can build this into a 4 hours scenario, various events will happen (meteorological event, a passenger gets sick, a system failure...). It is handled in a way that is closer to real-world situation”.
The use of crew resource management was seen as an important part of maintaining safety and this type of training was not done in actual aircraft due to the costs. Low-fidelity classroom-based exercises (such as a complete 4 hour flight) and simulator exercises were used to replace in-flight training. The Vancouver Trauma Centre did not aim to replace practice with its simulation based training, but acknowledged that it was not always possible or desirable to expose their personnel to actual front-line environments for practical and safety issues.
“We simulate based on actual practical problems seen in the field, as we need to prepare our personnel to meet those conditions when they are out there.”
Supporting Simulation The number of full-time simulation supporting staff, centre/unit managers, technicians and clerical staff can be found in Figure C.3.1.a. Overall, the average number of full-time simulation support workers was 1.94 per institution reporting. Nursing had slightly below average with 1.74 full-time workers supporting their simulation programs. Dentistry had the most support while Physiotherapy had the least. Graduate Programs had more support than Professional Development and Undergraduate Programs who had the least (See Figure C.3.1.b). Users of Intermediate Fidelity reported approximately 50% more support than High or Low Fidelity Simulation Programs (See Figure C.3.1.c).
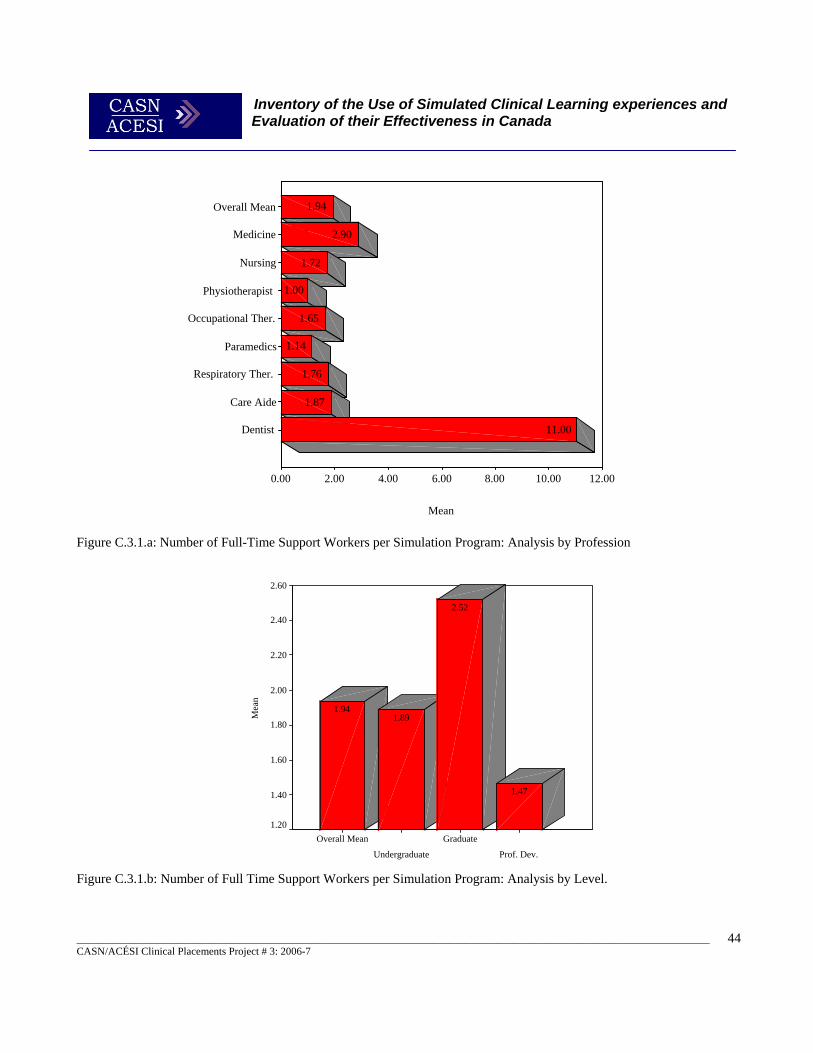
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
44
Prof. Dev.
Graduate
Undergraduate
Overall Mean
Mea
n
2.60
2.40
2.20
2.00
1.80
1.60
1.40
1.20
1.47
2.52
1.891.94
Overall Mean
Medicine
Nursing
Physiotherapist
Occupational Ther.
Paramedics
Respiratory Ther.
Care Aide
Dentist
Mean
12.0010.008.006.004.002.000.00
11.00
1.87
1.76
1.14
1.65
1.00
1.72
2.90
1.94
Figure C.3.1.a: Number of Full-Time Support Workers per Simulation Program: Analysis by Profession Figure C.3.1.b: Number of Full Time Support Workers per Simulation Program: Analysis by Level.
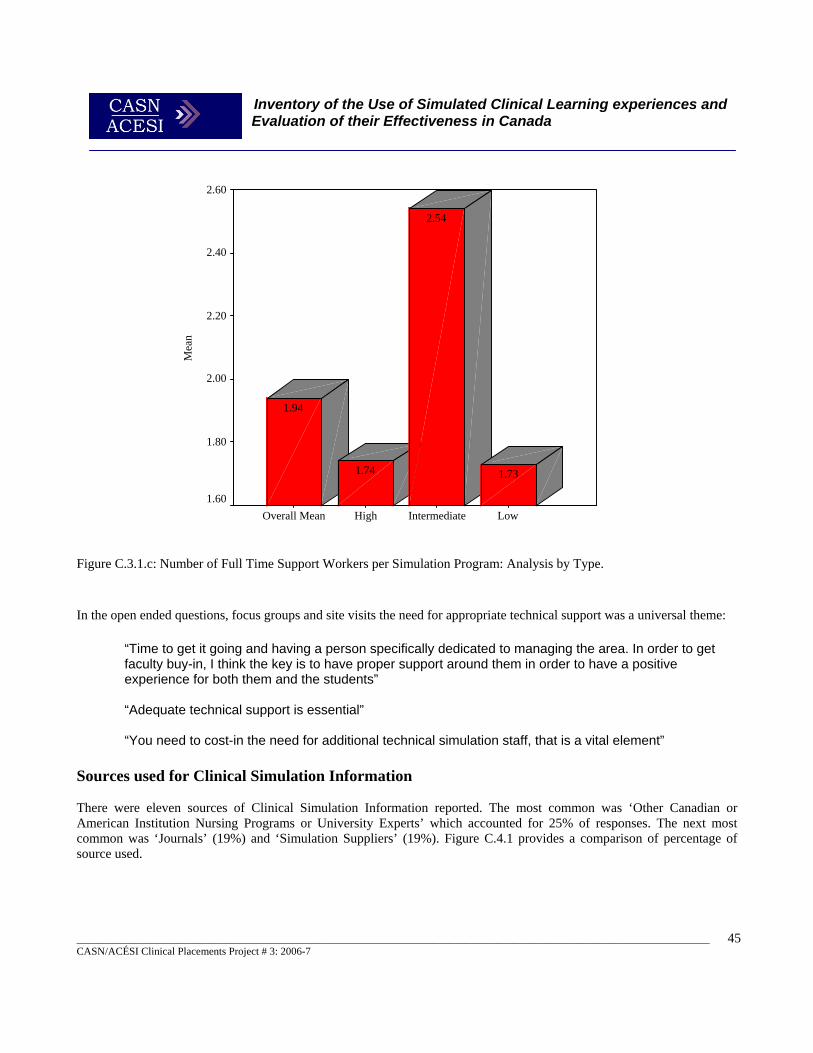
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
45
LowIntermediateHighOverall Mean
Mea
n2.60
2.40
2.20
2.00
1.80
1.60
1.73
2.54
1.74
1.94
Figure C.3.1.c: Number of Full Time Support Workers per Simulation Program: Analysis by Type. In the open ended questions, focus groups and site visits the need for appropriate technical support was a universal theme:
“Time to get it going and having a person specifically dedicated to managing the area. In order to get faculty buy-in, I think the key is to have proper support around them in order to have a positive experience for both them and the students” “Adequate technical support is essential” “You need to cost-in the need for additional technical simulation staff, that is a vital element”
Sources used for Clinical Simulation Information There were eleven sources of Clinical Simulation Information reported. The most common was ‘Other Canadian or American Institution Nursing Programs or University Experts’ which accounted for 25% of responses. The next most common was ‘Journals’ (19%) and ‘Simulation Suppliers’ (19%). Figure C.4.1 provides a comparison of percentage of source used.
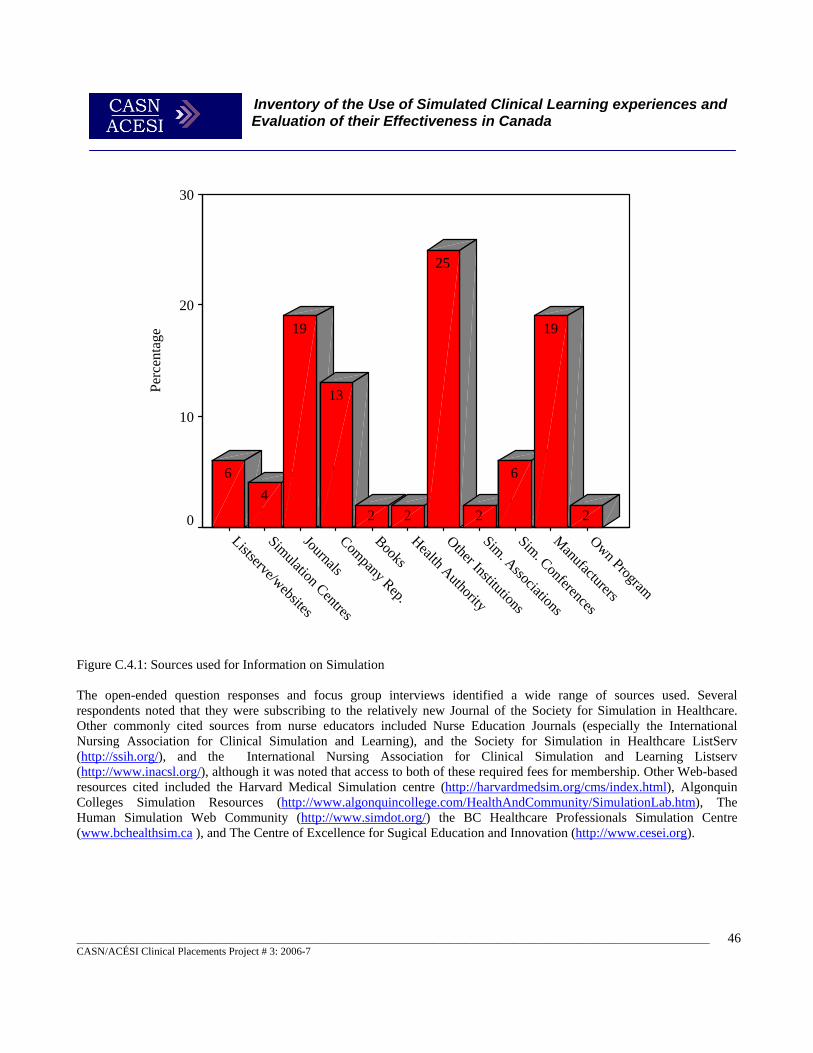
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
46
Figure C.4.1: Sources used for Information on Simulation The open-ended question responses and focus group interviews identified a wide range of sources used. Several respondents noted that they were subscribing to the relatively new Journal of the Society for Simulation in Healthcare. Other commonly cited sources from nurse educators included Nurse Education Journals (especially the International Nursing Association for Clinical Simulation and Learning), and the Society for Simulation in Healthcare ListServ (http://ssih.org/), and the International Nursing Association for Clinical Simulation and Learning Listserv (http://www.inacsl.org/), although it was noted that access to both of these required fees for membership. Other Web-based resources cited included the Harvard Medical Simulation centre (http://harvardmedsim.org/cms/index.html), Algonquin Colleges Simulation Resources (http://www.algonquincollege.com/HealthAndCommunity/SimulationLab.htm), The Human Simulation Web Community (http://www.simdot.org/) the BC Healthcare Professionals Simulation Centre (www.bchealthsim.ca ), and The Centre of Excellence for Sugical Education and Innovation (http://www.cesei.org).
Own Program
Manufacturers
Sim. Conferences
Sim. Associations
Other Institutions
Health Authority
BooksCompany Rep.
Journals
Simulation Centres
Listserve/websites
Perc
enta
ge
30
20
10
0 2
19
6
2
25
22
13
19
46

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
47
D. Meeting the Needs of Practice Respondents were asked to indicate to what level simulation met their training needs for clinical education and training. Percentages for whether simulation meets training needs, analyzed by profession, appear in Figure D.1. All physician respondents, and a significant portion of nurses (54%), respiratory therapists (43%), and those representing educational institutions (50%) indicated that simulations somewhat met these needs. There were no respondents that indicated simulation exceeded their training needs; however, 21% of nurses, 25% of paramedics and 19% of those representing educational institutions noted that simulations were inadequate as training aids. The professions whose learning needs that were least met by simulations were Occupational Therapists, Paramedics and Care Aides (See Figure D.1.a). Those individuals representing medical professions and also Physiotherapists, in particular, indicated that simulation only somewhat met their needs (See Figure D.1.b). An examination of Figure D.1.c, however, reveals that about one third of Occupational Therapists, Paramedics, and Respiratory Therapists believed that simulation fully met their needs. When averaged over all nine professions, most participants considered that simulation somewhat met their needs. Analysis by Level is indicative of the fact that for 21% of participants, simulation did not meet their training needs. For 54% of respondents, simulations somewhat fulfilled clinical training needs, while for another 15%, these learning tools aided in fully meeting training requirements. Undergraduate educators were less optimistic than their Graduate and Professional Development counterparts, when responding to this question (28%, compared to 31% and 31% on average, respectively). See Figures D.2 to D.2.c for breakdowns by Level. Division by Type reveals that users of Intermediate Fidelity simulations had the highest opinion of simulations with respect to meeting their learning needs (See Figure D.3), followed by Low Fidelity, and then High Fidelity. For details on analysis by type see Figures D.3.a to D.3.c. Study participants were given the option to provide their responses to an open-ended question that addressed the concern of whether simulations met their clinical education and training needs. The main reasons given why simulation did not meet their needs are tabulated in figure D.4. The most common response expressed was that the level of simulation was too low (21 responses), and 6 Respondents Indicated that they felt simulations should only fill a supplemental role in educational programs. With regard to cost-effectiveness and cost-efficiency ninety-six percent of respondents had not conducted any formal evaluations or cost-benefit/cost-effectiveness/cost-efficiency evaluations of the simulation resources, and only eighteen percent thought that simulation was Very Cost Effective (see Figure D.5). Four percent of respondents thought that simulation was Not Cost Effective, but thirty eight percent thought it was Reasonably Cost Effective, and over thirty five percent stated it was Cost Effective. Six percent of respondents felt that simulation was Not Cost Efficient, forty four percent Reasonably Cost Efficient and thirty one percent Cost Efficient, and only four percent Very Cost Efficient (Figure D.6). Generally there was a perception that simulation was cost-effective and cost-efficient. This probably reflects the perception identified that simulation is a significant contributor to client safety, and is therefore judged as an effective learning technique, although possibly in terms of efficiency respondents were a little less certain.
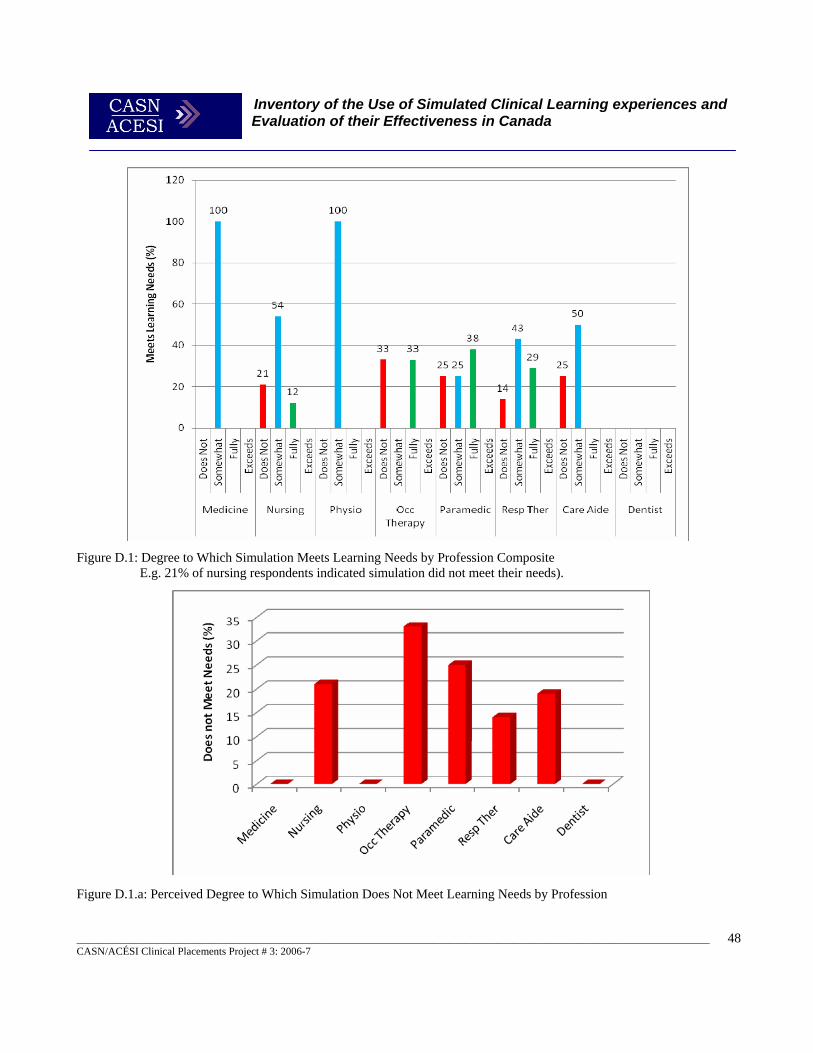
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
48
Figure D.1: Degree to Which Simulation Meets Learning Needs by Profession Composite E.g. 21% of nursing respondents indicated simulation did not meet their needs). Figure D.1.a: Perceived Degree to Which Simulation Does Not Meet Learning Needs by Profession
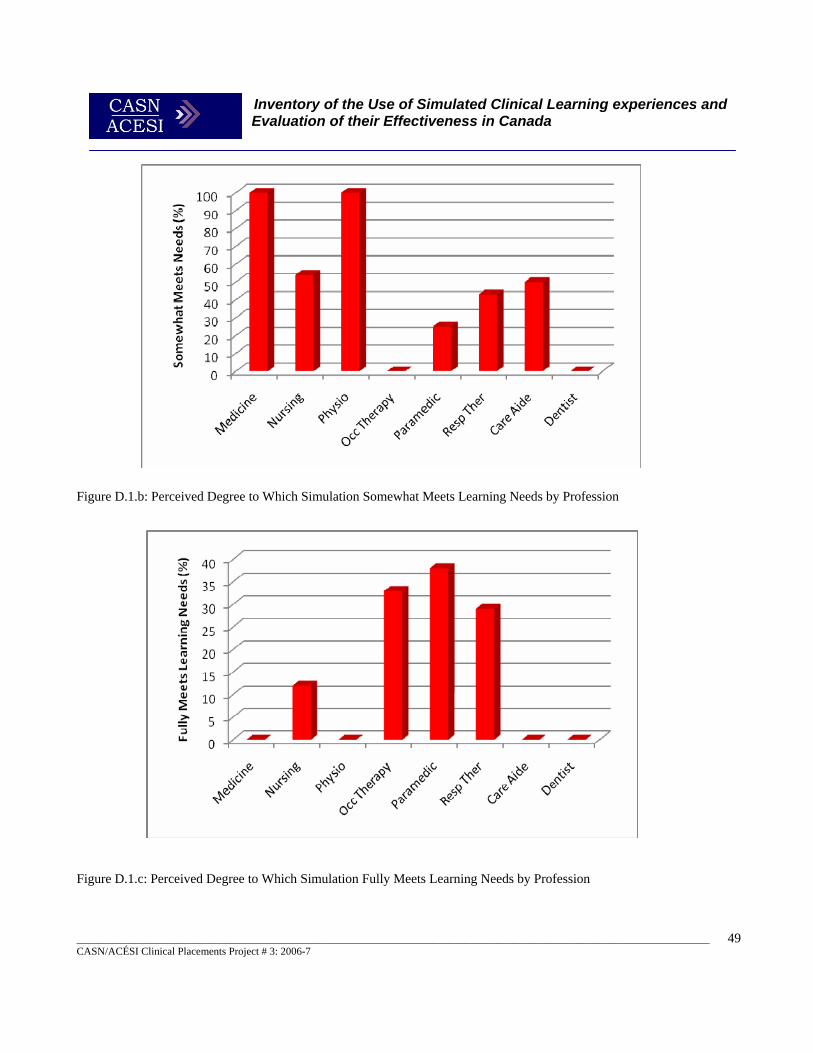
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
49
Figure D.1.b: Perceived Degree to Which Simulation Somewhat Meets Learning Needs by Profession Figure D.1.c: Perceived Degree to Which Simulation Fully Meets Learning Needs by Profession
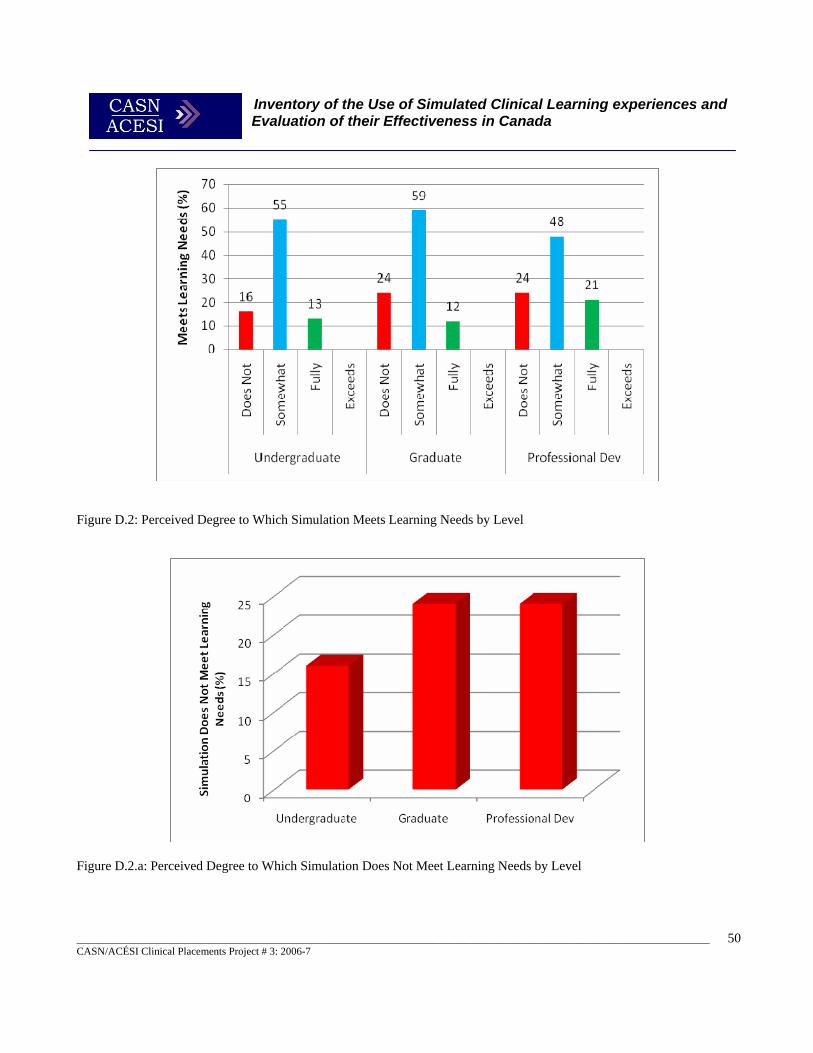
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
50
Figure D.2: Perceived Degree to Which Simulation Meets Learning Needs by Level
Figure D.2.a: Perceived Degree to Which Simulation Does Not Meet Learning Needs by Level
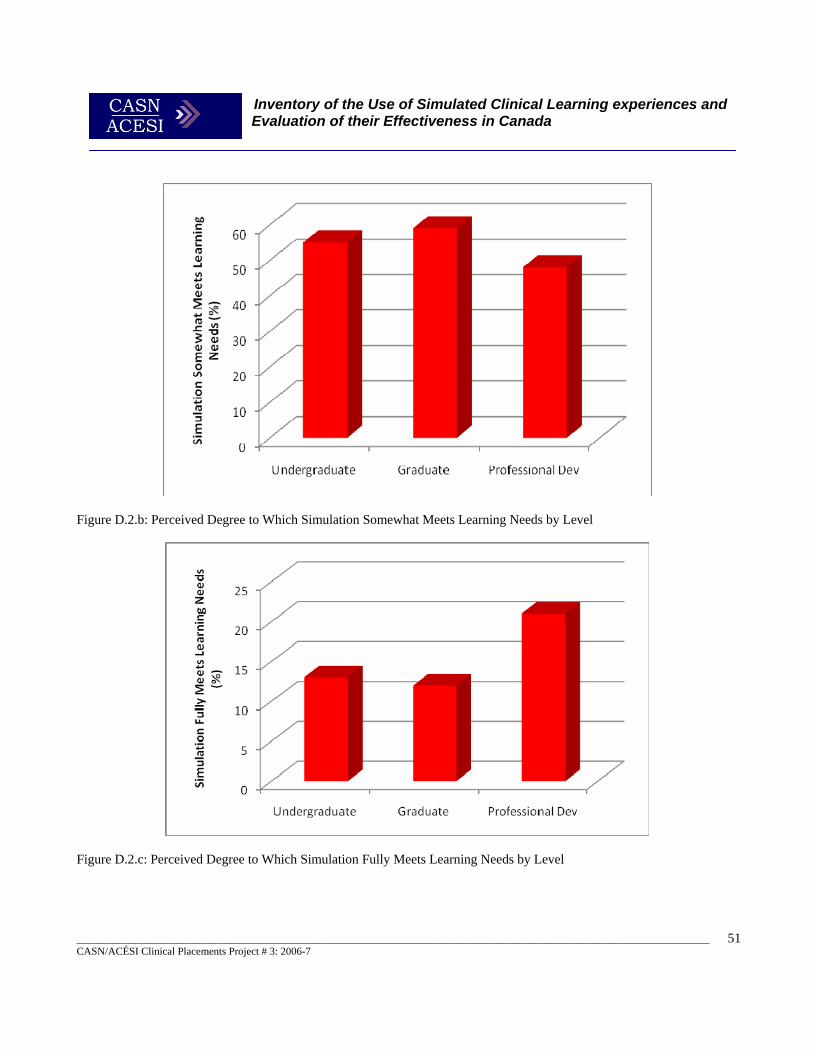
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
51
Figure D.2.b: Perceived Degree to Which Simulation Somewhat Meets Learning Needs by Level
Figure D.2.c: Perceived Degree to Which Simulation Fully Meets Learning Needs by Level
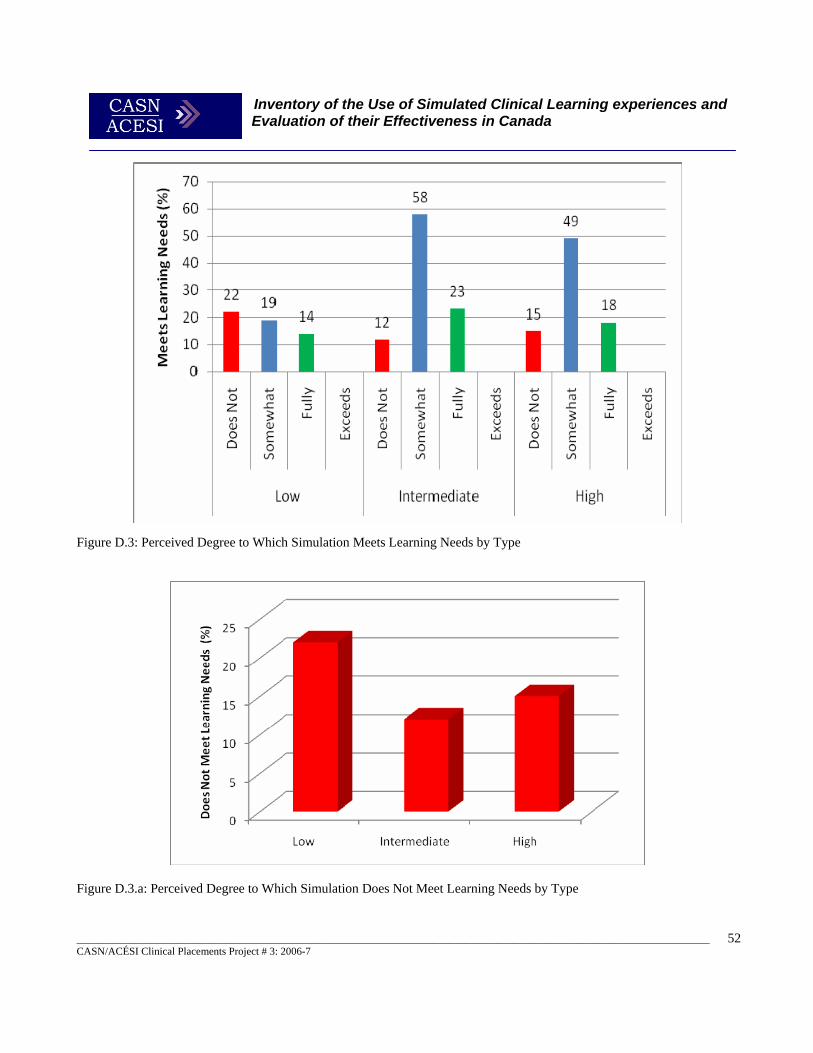
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
52
Figure D.3: Perceived Degree to Which Simulation Meets Learning Needs by Type
Figure D.3.a: Perceived Degree to Which Simulation Does Not Meet Learning Needs by Type
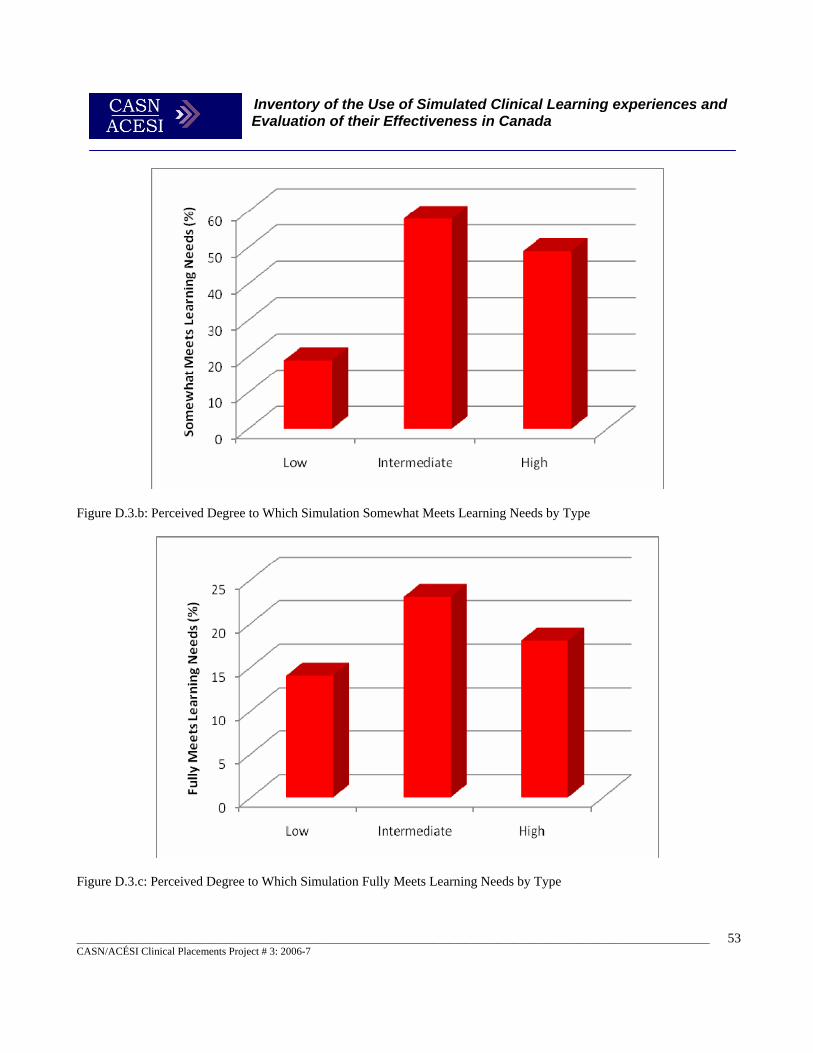
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
53
Figure D.3.b: Perceived Degree to Which Simulation Somewhat Meets Learning Needs by Type
Figure D.3.c: Perceived Degree to Which Simulation Fully Meets Learning Needs by Type
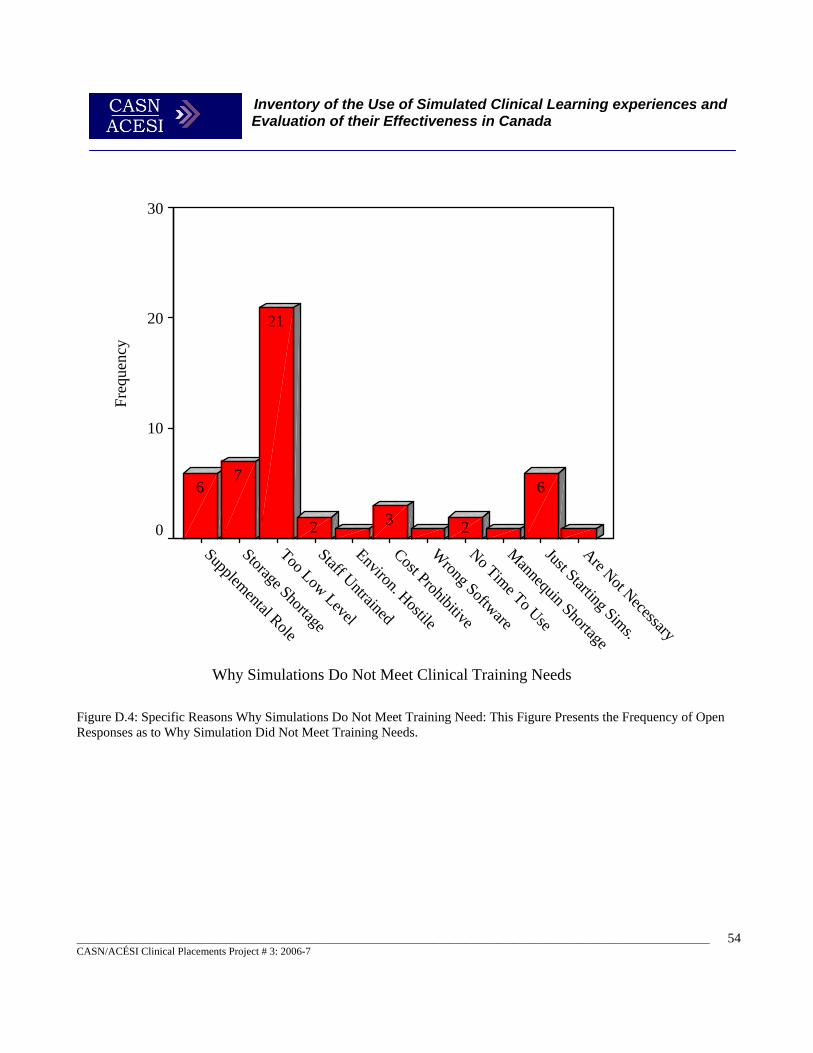
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
54
Why Simulations Do Not Meet Clinical Training Needs
Are Not Necessary
Just Starting Sims.
Mannequin Shortage
No Time To Use
Wrong Software
Cost Prohibitive
Environ. Hostile
Staff Untrained
Too Low Level
Storage Shortage
Supplemental Role
Freq
uenc
y
30
20
10
0
6
232
21
76
Figure D.4: Specific Reasons Why Simulations Do Not Meet Training Need: This Figure Presents the Frequency of Open Responses as to Why Simulation Did Not Meet Training Needs.
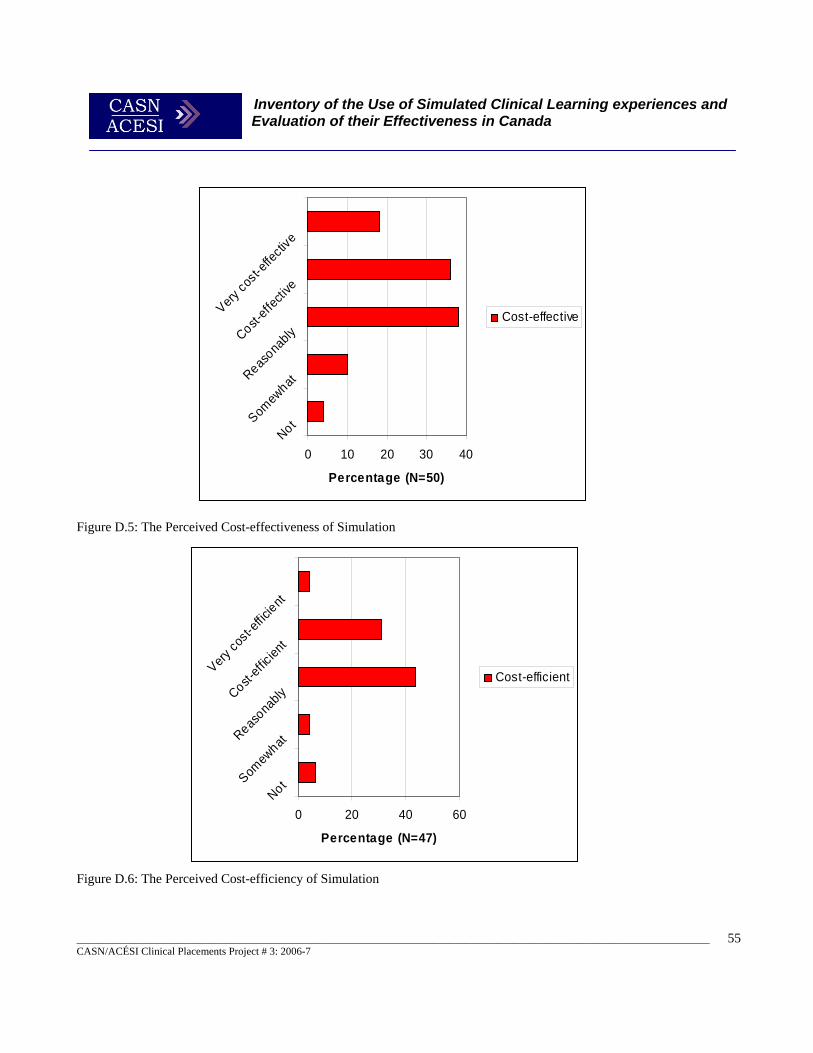
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
55
0 10 20 30 40NotSom
ewhatReas
onablyCost-
effec
tive
Very co
st-eff
ectiv
e
Percentage (N=50)
Cost-effective
0 20 40 60NotSom
ewhatReas
onablyCost-
efficie
nt
Very co
st-eff
icient
Percentage (N=47)
Cost-efficient
Figure D.5: The Perceived Cost-effectiveness of Simulation Figure D.6: The Perceived Cost-efficiency of Simulation
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
56
An opportunity was provided to respond to an open-ended question concerning whether simulations met the training needs of study participants. In Figure D.1.14, some of the major problems that respondents had getting simulations to adequately meet their training needs are highlighted. Other major themes from these questions, the focus group interviews and site visits are discussed below. Of the 49 responses to this open-ended question, 22 dealt with the theme of inadequate simulation equipment. The difficulties reported were that either high fidelity simulations were unavailable, or if high fidelity simulations were available they were still inadequate. For example, when administering IVs, the variety of vein placements and anatomical variation in live patients was not reproducible even in high fidelity simulations.
“Simulation efforts have met many training needs, however there are limitations some of which are technical directly related to the simulators. “ “The functionality could still be improved in some aspects. We are investigating and purchasing augmenting equipment to increase realism etc. We have and will continue to discuss upgrades with vendors. “ “We would like to see a better range of gender age, and ethnic characteristics as enhancements, female voices for example, in the simulators [high-fidelity] to increase realism.” “It is still not as real life as we would like it to be, we’re getting there. And some of the assessments on the manikin aren’t quite landmarked in the right position, pulses may be hard to find so the technical aspects are not as refined as a real human being.”
One recurrent encompassed suggestions such as the need for better training of instructors. There were also statements concerning the need for more direct feedback to instructors and students, and getting faculty “on-board.”
“…you have to spend time with faculty and, I’m sure you have heard before, not everyone is on-board with simulations and depending on individual faculty’s orientation around that, there is a lot of time that needs to be spent encouraging people to look at change and how nursing education can implement new things. And there are a lot of people who want it to remain traditional, stay with what they know.”
Several participants indicated that the simulations take time to integrate into curriculum. Construction of curriculum-specific scenarios is time-consuming. Also, many simulation programs were new and had not had enough time to develop their resources yet. “We are new at this and finding that it takes a lot of time to create useful scenarios.”
“We have purchased scenarios for the nursing program, from METI® but, when the outside group is doing the critical care team, the physician who has working with simulation does his own scenarios.” “I know here we don’t have the resources to be creating our own simulation scenarios so having purchased the ones from METI® is a big advantage.”
Negative faculty attitudes towards simulation were another factor raised by a few respondents and how that affected the integration of simulation into the curriculum:
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
57
“We are just getting started and some of it’s actually kind of attitude from the faculty in that they feel that it’s impotent and strange to actually be working on simulators, even having the student being with [simulated] patients on their own. That was one of the barriers I think we had so far.”
“You have to spend time with faculty and, I’m sure you have heard before, not everyone is on board with simulations and depending on individual faculty’s orientation around that, there is a lot of time that needs to be spent encouraging people to look at change and how nursing education can implement new things. There are a lot of people who want it to remain traditional, stay with what they know.”
Surprisingly reliability and technical issues were not overly expressed as concerns although a couple of respondents did indicate they had experienced technical problems. However when discussed these were generally related to support issues (see section C).
“Technical is a concern when a stuff goes down in the middle of a scenario it doesn’t make a very positive experience for the students, and certainly not all nursing labs have an IT at their immediate school. If the technology goes awry, when you are in the middle of a scenario, and troubleshooting that and not losing the interest of student's [sic].”
In exploring the advantages of simulation the role of high-fidelity clinical simulation in helping improve client safety through better prepared practitioners was expressed by most of the professional educators. The Air Canada Simulation Centre expressed safety as a key reason for using flight simulation as opposed to actual experience.
“Improving safety is a key issue. We have to establish a training matrix that must be approved by Transport Canada, a recurrent training matrix which extends over a 3 years period (every 6 months mandatory simulation based recurrent training occurs). It will cover essential issues like engine failure, hydraulic systems failure.”
Other comments from health care educators reflected a strong belief that simulation provided benefits in improvements in client safety are given below.
“…how do you measure the long-term effects? Do we prevent errors from being made at the actual bedsides with real live human beings? We don’t know that yet. We just know that instructors and nurses in the agencies are saying that these students can prioritize and react more quickly than what’ve seen in the past.” “Increasing patient safety, better prepared students and, I hope a long range spin-off would be that patient safety in the practicum settings would be increased.”
“One of the big advantages is that nobody should be dying in a sim lab.”
“You can create an almost real life situation in a very safe environment versus being a real patient situation. So let’s say the student nurse team doesn’t quite do the right thing that should be happening you can intervene and make a difference in what the outcomes are going to be ; and it’s a huge learning thing for them, without the result of something critical happening. So it’s safe and you can create quite a safe learning environment as well just through the debriefing process of how you approach it. “
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
58
“I think the clients are more acutely ill and as a result the expectations of [clinical] staff and some faculty are that the students perform at a higher level than we may have seen historically before in the nursing programs. Simulation can help that.”
A theme related to this and very frequently raised was that of increased levels of student confidence in those engaged in simulated activities, particularly with high-fidelity simulation. This went alongside a theme of lowered stress in the teaching environment.
“Using our simulators students will have the opportunity to participate in a code blue and develop confidence and competence so that once they graduate and are involved in a true code they will have already had the experience and have practiced in a safe environment.” “…it allows the user to develop the psycho-motor skills needed to do the procedure the right way and gain confidence executing the procedure.” “…improved confidence, improved skills, provide familiarity and practice with unusual or rarely utilized skills.” “Students have increased confidence going into clinical areas due to exposure in the [simulation] lab.” “Those programs are good for skills development because you repeat the right gestures over and over. Students get to know their strengths and weaknesses in regard of different care procedures situations: stress, shaking, sterility. This in turn will help them gain self-confidence. The more the students simulate a situation, the easier it will be for them to visualize and integrate it. “ “It creates a realistic environment with a lower stress level“ “With simulation there is a lower stress learning environment as compared to a patient.”
Another theme that arose was the ability to standardize student’s experiences and use standardized evaluations in assessing student’s performance. The McGill Medical Simulation Centre used SPs and videotaped simulations significantly in the evaluation of student performance.” Competency evaluation with tasks and simulation (e.g. CPR) was very common in most areas.
“We use standardized scripts along with that so they administer medications to the manikins, and all get the same experience." “Standardized patients help us give predictable experiences to our students for evaluation. They all get the same experience." “We have developed evaluation grids, for standardized simulations to assess our student’s performance.” “We evaluate our students with scenarios we have developed simulating the ones on ECOS [examen clinique objectif structure] therefore much alike the OIIQ exam [examen professionnel d'admission à la profession in Quebec] in certain area of health care procedures.”

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
59
“Simulation provides opportunity to have unbiased evaluation based on predetermined objectives and evidence based guidelines permits a clearer "view" of students critical thinking and problem solving strategies and abilities (particularly if scenarios and debriefings are videotaped) “ “We use formal evaluation forms for each specific skill that is critiqued e.g. wound care, medication administration”
With regard to cost-benefit, cost-effectiveness and cost-efficiency the evidence from the open-ended questions, focus groups and site visits suggested a range of views. The areas where simulation was perceived as most cost-beneficial included restorative dentistry, undergraduate nursing, and for continuing professional education, and client safety was also identified. Several respondents noted it was too early to tell. For cost-effectiveness a similar range of activities were suggested but also several participants suggested it would be more effective where high numbers of complex procedures were required and when used for students who need to make up clinical hours due to illness or family emergencies. Cost-efficiency did not appear to be perceived any differently, and additional responses in this category suggested simulation would also be efficient for use in rural clinical placements at a distance from main centres, and only would really be demonstrated when product durability, use with multiple applications, and larger number of users could be established.
“We anticipate it will be cost-beneficial when it is used for our continuing education programs” They have the potential to be extremely cost-effective. We’re looking at curriculum revisions within our own consortium of colleges and that is going to change the clinical practice areas. We’re looking at and I think in our health authority they are looking at probably downsizing so I really think there is going to be a bigger approach to use it not only to develop psychomotor skills but the decision making and the communication skills and developing the confidence and competence prior putting our students into the clinical settings.” “One of the things we have found in terms of cost is that this takes an incredible amount of human resources to mount a scenario and to do it correctly. We had 121 students in their 2nd year that we ran through the simulation lab last week and we did it over 2 days and there were 5 instructors in there…but certainly the learning that went on was well worth the investment in the cost of the human resources.” “I would think the effectiveness is going to be down the line in terms of improving readiness to practice and competence and confidence and ultimately patient safety in quality care.” “I guess it depends on what criteria you want to use for cost-effectiveness and who’s going to be evaluating that criteria. The person who does our budget doesn’t think it’s cost-effective at all because it’s a big budget item.” “I don’t know, I wouldn’t say that it is more efficient. I think it’s going to turn up to be more costly but in terms of the maintenance and the time it is going to take to use the simulations well. There is a lot human resource time that goes in where before, with more traditional ways, they practice blood pressure on each other, the other ways that we did it I would think of the top would be more cost-effective.”

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
60
E. Investment in Simulation Sources of funding, and amounts of funding from each source, were explored in the survey. However, proportions and counts for funding sources for both Set-up and Ongoing funding were based on how many sources respondents indicated they had received support from, rather than how much support they had received from each. Therefore, only a general overview is given. The ten possible sources of set-up funding were as follows; Federal Government Grants, Provincial Government Grants, Educational Institutions, Healthcare Institutions, Private Donors, Municipal Government, Student Education Resource Funds, In Kind Equipment Funds, Clinical Revenue, and Tuition Fees. The main sources for Set-Up Funding, if rated by the number of sources, were Educational Institutions and Provincial Governments (See Figure E.1). These two accounted for 76% of set-up funding sources for all simulation programs. Set Up Funding The average number of set-up funding sources was 3.7 per profession. Nursing programs had the broadest base of funding for set-up costs, having 7 of 10, compared to only two for Physiotherapy (See Figure E.2). Undergraduate Programs utilized all ten sources followed by Professional Development and graduate programs (See Figure E.2). Graduate programs had a much shallower funding base, being only half that of undergraduate programs. High Fidelity programs covered 90% of possible sources, while Intermediate and Low Fidelity ones utilized only 70% each (Figure E.2). An examination of the Nursing Profession in Figure E.3 reveals a similar pattern to set-up funding for all programs with Educational Institutions and Provincial Government funding accounting for 79% of its funding sources. Healthcare Institutions and Private or Donor Support accounted for 15% of set-up funding, and the remaining 6% came from Municipal Governments, Student Education Resource Funds, and In Kind Equipment. For complete details on set-up funding for the other professions see Table E.2 in Appendix E. Ongoing Funding Sources The sources for ongoing funding are somewhat different than for set-up funding. They are as follows: Provincial Governments, Federal Governments, Regional Governments, Educational Institutions, Healthcare Institutions, Private or Donor Support, Municipal Governments, Rental to Outside Sources, Private Sources, and Clinical Revenues. Educational Institutions provide 57% of funding sources for ongoing simulations. This is unlike set-up funding where two bodies provide the bulk of funding sources. Frequencies for all of the sources appear in Figure E.4. Figure E.5 displays the frequencies for number of sources for professions, levels, and types. The average number of sources of ongoing funding by profession was 3.8. This is comparable to the average of 3.7 for set-up funding. A comparison of the nine Profession groups demonstrated that, as with set-up funding, Nursing had the broadest base of funding and Physiotherapy the least variety of funding sources. When split by level the Undergraduate and Professional Development categories led the way with 100% and 80% of the identified funding sources respectively, followed by graduate programs with funding from only 60% of the sources identified. Division by type demonstrates that High Fidelity programs had the broadest funding base. High Fidelity had access to 90% of the funding sources, while Intermediate Fidelity had 70% and Low Fidelity only 60%. The average number of funding sources accessed was 7.7. When proportion of sources is considered for the Nursing Profession it follows a similar pattern to the overall ongoing funding profile. The majority (62%) of funding sources for Nursing Programs came from Educational Institutions, while Healthcare Institutions and other sources accounted for only ten percent or less. For details on the other professions see Table 11.6 in Appendix F.
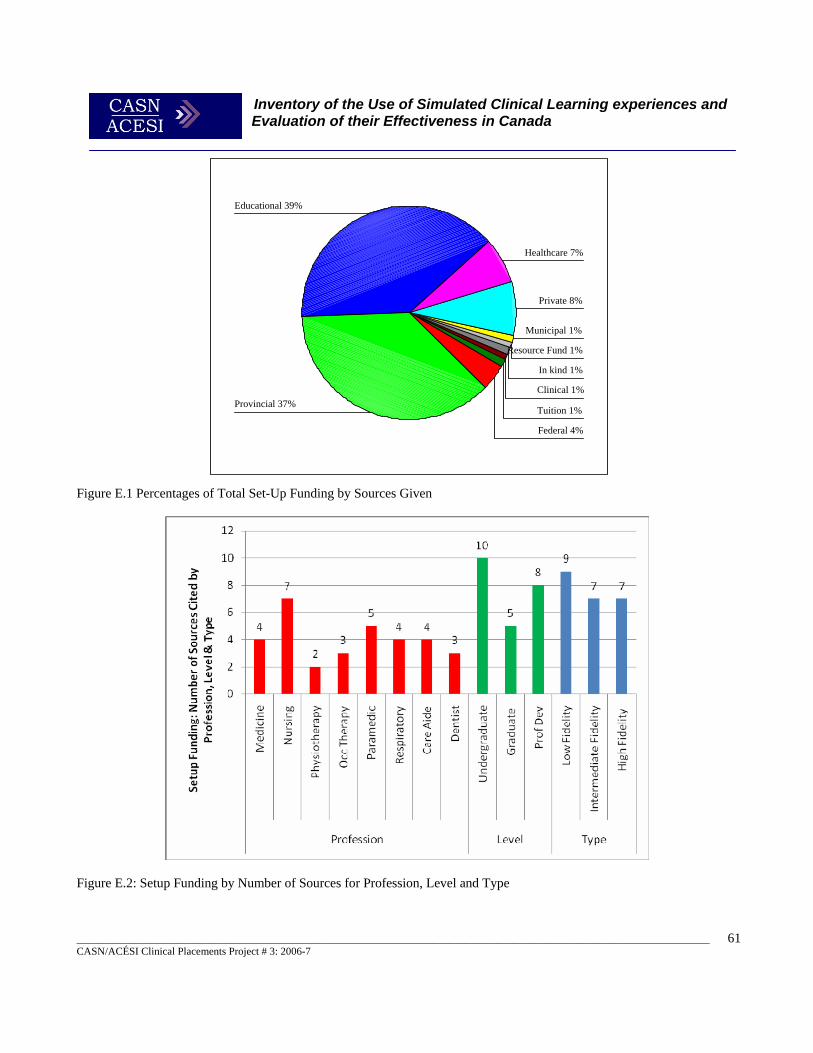
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
61
Tuition 1%
Clinical 1%
In kind 1%
Resource Fund 1%
Municipal 1%
Private 8%
Healthcare 7%
Educational 39%
Provincial 37%
Federal 4%
Figure E.1 Percentages of Total Set-Up Funding by Sources Given
Figure E.2: Setup Funding by Number of Sources for Profession, Level and Type
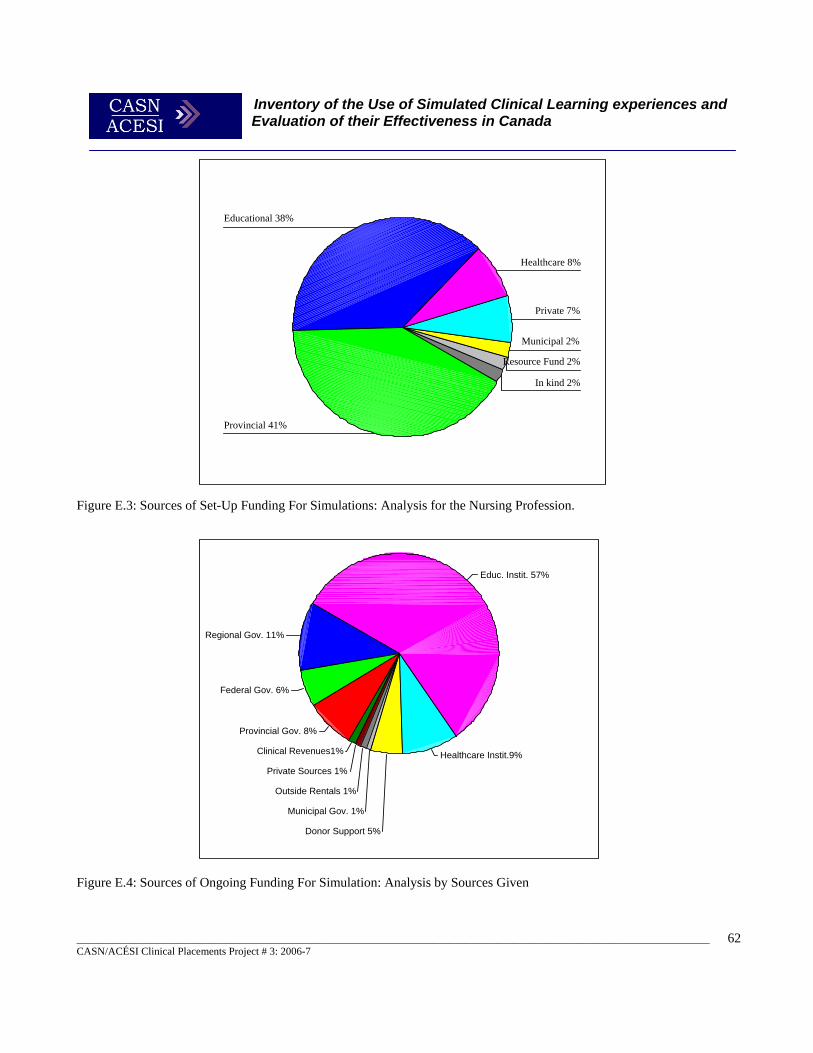
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
62
In kind 2%
Resource Fund 2%
Municipal 2%
Private 7%
Healthcare 8%
Educational 38%
Provincial 41%
Clinical Revenues1%
Private Sources 1%
Outside Rentals 1%
Municipal Gov. 1%
Donor Support 5%
Healthcare Instit.9%
Educ. Instit. 57%
Regional Gov. 11%
Federal Gov. 6%
Provincial Gov. 8%
Figure E.3: Sources of Set-Up Funding For Simulations: Analysis for the Nursing Profession.
Figure E.4: Sources of Ongoing Funding For Simulation: Analysis by Sources Given
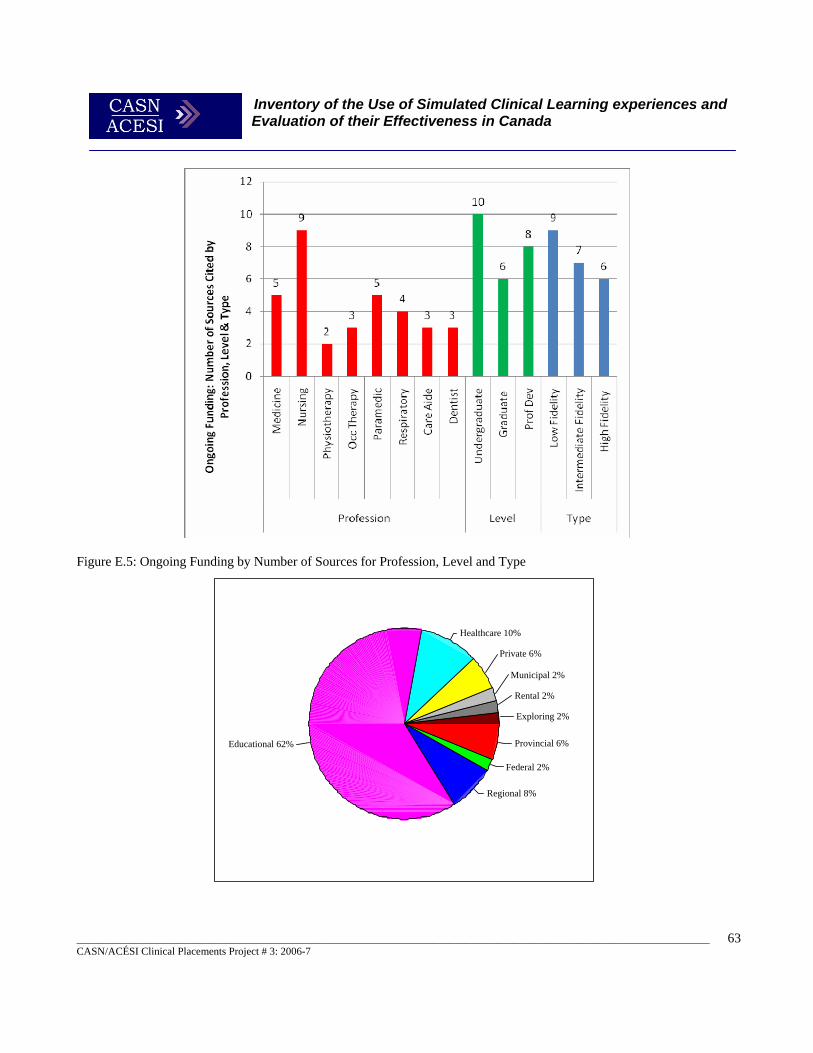
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
63
Exploring 2%
Rental 2%
Municipal 2%
Private 6%
Healthcare 10%
Educational 62%
Regional 8%
Federal 2%
Provincial 6%
Figure E.5: Ongoing Funding by Number of Sources for Profession, Level and Type

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
64
Figure E.6 Sources of Ongoing Funding: Analysis for the Nursing Profession.
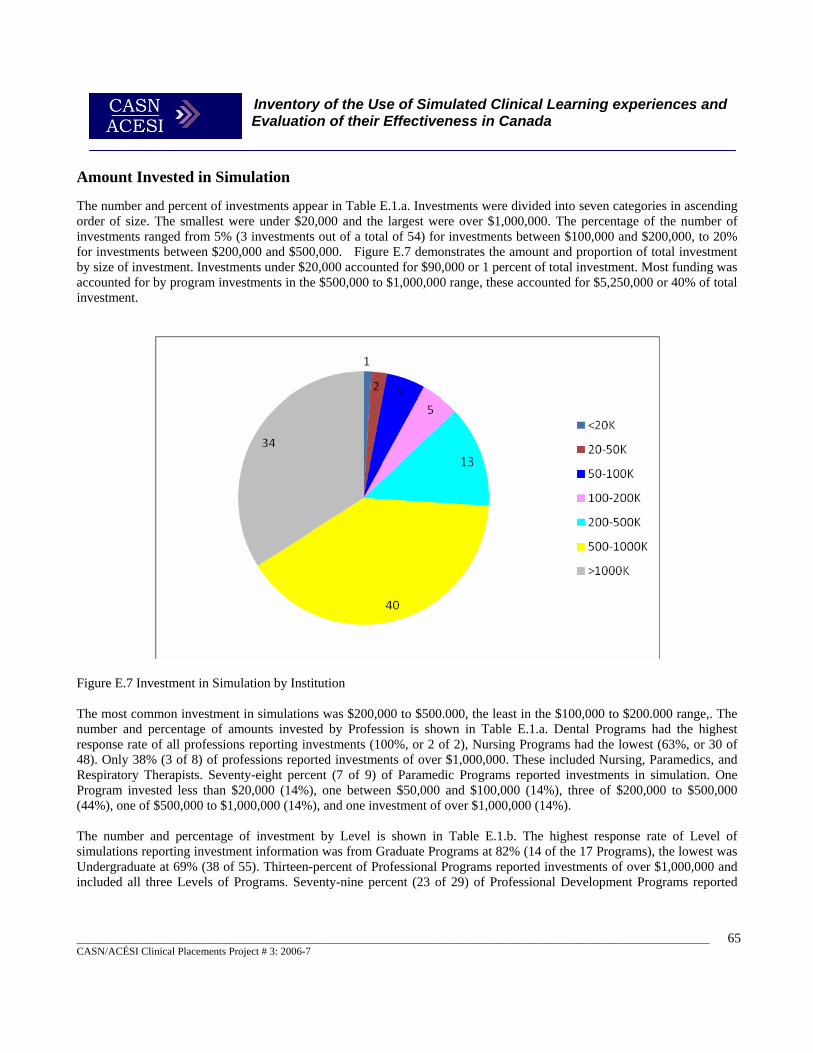
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
65
Amount Invested in Simulation The number and percent of investments appear in Table E.1.a. Investments were divided into seven categories in ascending order of size. The smallest were under $20,000 and the largest were over $1,000,000. The percentage of the number of investments ranged from 5% (3 investments out of a total of 54) for investments between $100,000 and $200,000, to 20% for investments between $200,000 and $500,000. Figure E.7 demonstrates the amount and proportion of total investment by size of investment. Investments under $20,000 accounted for $90,000 or 1 percent of total investment. Most funding was accounted for by program investments in the $500,000 to $1,000,000 range, these accounted for $5,250,000 or 40% of total investment.
Figure E.7 Investment in Simulation by Institution The most common investment in simulations was $200,000 to $500.000, the least in the $100,000 to $200.000 range,. The number and percentage of amounts invested by Profession is shown in Table E.1.a. Dental Programs had the highest response rate of all professions reporting investments (100%, or 2 of 2), Nursing Programs had the lowest (63%, or 30 of 48). Only 38% (3 of 8) of professions reported investments of over $1,000,000. These included Nursing, Paramedics, and Respiratory Therapists. Seventy-eight percent (7 of 9) of Paramedic Programs reported investments in simulation. One Program invested less than $20,000 (14%), one between $50,000 and $100,000 (14%), three of $200,000 to $500,000 (44%), one of $500,000 to $1,000,000 (14%), and one investment of over $1,000,000 (14%). The number and percentage of investment by Level is shown in Table E.1.b. The highest response rate of Level of simulations reporting investment information was from Graduate Programs at 82% (14 of the 17 Programs), the lowest was Undergraduate at 69% (38 of 55). Thirteen-percent of Professional Programs reported investments of over $1,000,000 and included all three Levels of Programs. Seventy-nine percent (23 of 29) of Professional Development Programs reported
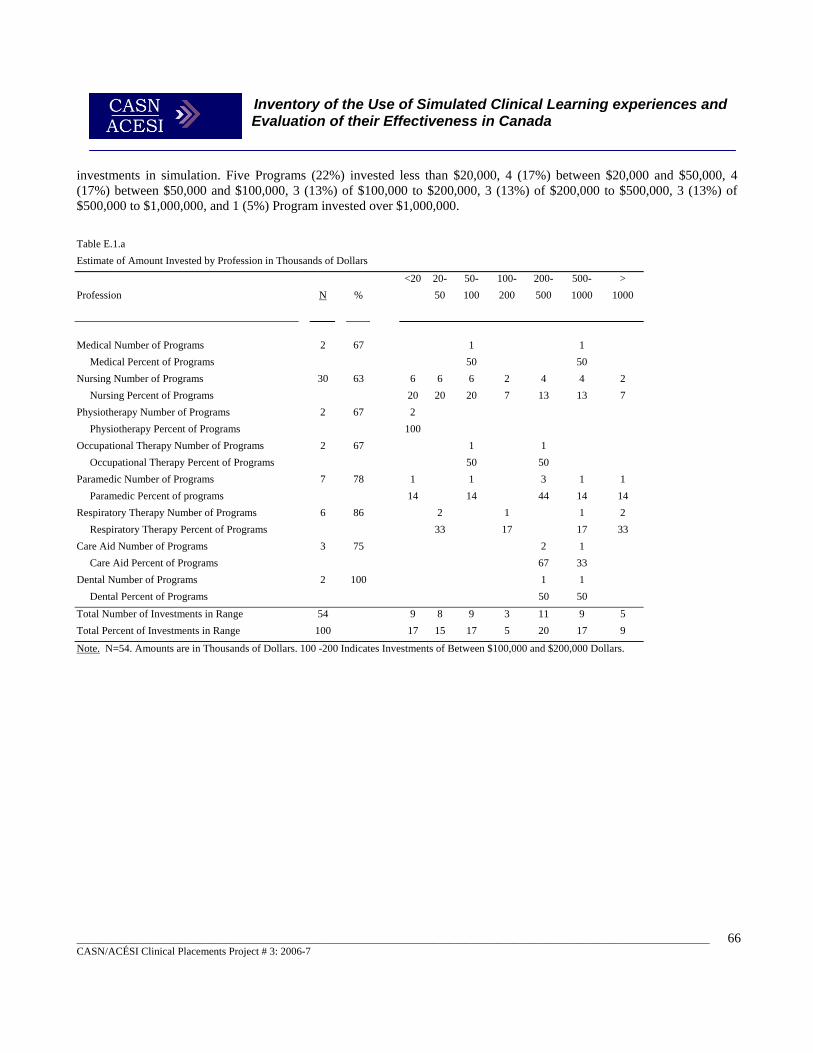
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
66
investments in simulation. Five Programs (22%) invested less than $20,000, 4 (17%) between $20,000 and $50,000, 4 (17%) between $50,000 and $100,000, 3 (13%) of $100,000 to $200,000, 3 (13%) of $200,000 to $500,000, 3 (13%) of $500,000 to $1,000,000, and 1 (5%) Program invested over $1,000,000. Table E.1.a Estimate of Amount Invested by Profession in Thousands of Dollars
<20 20- 50- 100- 200- 500- > Profession N %
50 100 200 500 1000 1000
Medical Number of Programs 2 67 1 1 Medical Percent of Programs 50 50 Nursing Number of Programs 30 63 6 6 6 2 4 4 2 Nursing Percent of Programs 20 20 20 7 13 13 7 Physiotherapy Number of Programs 2 67 2 Physiotherapy Percent of Programs 100 Occupational Therapy Number of Programs 2 67 1 1 Occupational Therapy Percent of Programs 50 50 Paramedic Number of Programs 7 78 1 1 3 1 1 Paramedic Percent of programs 14 14 44 14 14 Respiratory Therapy Number of Programs 6 86 2 1 1 2 Respiratory Therapy Percent of Programs 33 17 17 33 Care Aid Number of Programs 3 75 2 1 Care Aid Percent of Programs 67 33 Dental Number of Programs 2 100 1 1 Dental Percent of Programs 50 50 Total Number of Investments in Range 54 9 8 9 3 11 9 5 Total Percent of Investments in Range 100 17 15 17 5 20 17 9
Note. N=54. Amounts are in Thousands of Dollars. 100 -200 Indicates Investments of Between $100,000 and $200,000 Dollars.
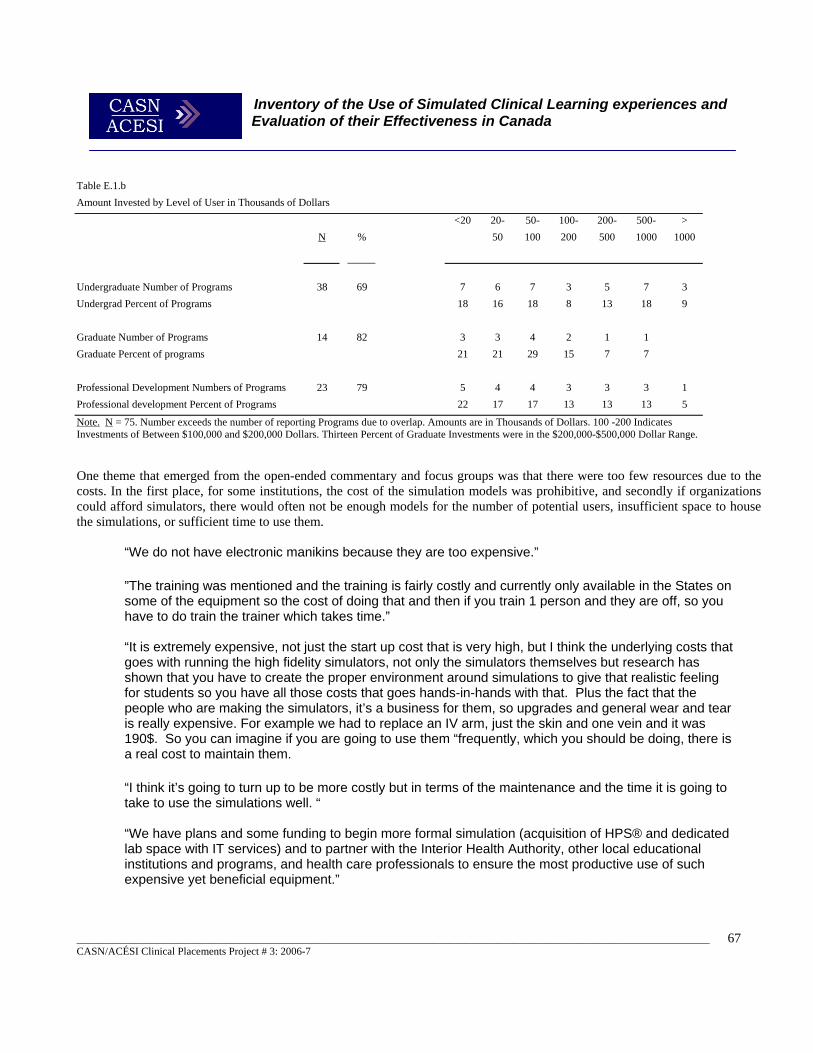
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
67
Table E.1.b Amount Invested by Level of User in Thousands of Dollars
<20 20- 50- 100- 200- 500- > N %
50 100 200 500 1000 1000
Undergraduate Number of Programs 38 69 7 6 7 3 5 7 3 Undergrad Percent of Programs 18 16 18 8 13 18 9 Graduate Number of Programs 14 82 3 3 4 2 1 1 Graduate Percent of programs 21 21 29 15 7 7 Professional Development Numbers of Programs 23 79 5 4 4 3 3 3 1 Professional development Percent of Programs 22 17 17 13 13 13 5
Note. N = 75. Number exceeds the number of reporting Programs due to overlap. Amounts are in Thousands of Dollars. 100 -200 Indicates Investments of Between $100,000 and $200,000 Dollars. Thirteen Percent of Graduate Investments were in the $200,000-$500,000 Dollar Range. One theme that emerged from the open-ended commentary and focus groups was that there were too few resources due to the costs. In the first place, for some institutions, the cost of the simulation models was prohibitive, and secondly if organizations could afford simulators, there would often not be enough models for the number of potential users, insufficient space to house the simulations, or sufficient time to use them.
“We do not have electronic manikins because they are too expensive.”
”The training was mentioned and the training is fairly costly and currently only available in the States on some of the equipment so the cost of doing that and then if you train 1 person and they are off, so you have to do train the trainer which takes time.” “It is extremely expensive, not just the start up cost that is very high, but I think the underlying costs that goes with running the high fidelity simulators, not only the simulators themselves but research has shown that you have to create the proper environment around simulations to give that realistic feeling for students so you have all those costs that goes hands-in-hands with that. Plus the fact that the people who are making the simulators, it’s a business for them, so upgrades and general wear and tear is really expensive. For example we had to replace an IV arm, just the skin and one vein and it was 190$. So you can imagine if you are going to use them “frequently, which you should be doing, there is a real cost to maintain them.
“I think it’s going to turn up to be more costly but in terms of the maintenance and the time it is going to take to use the simulations well. “ “We have plans and some funding to begin more formal simulation (acquisition of HPS® and dedicated lab space with IT services) and to partner with the Interior Health Authority, other local educational institutions and programs, and health care professionals to ensure the most productive use of such expensive yet beneficial equipment.”
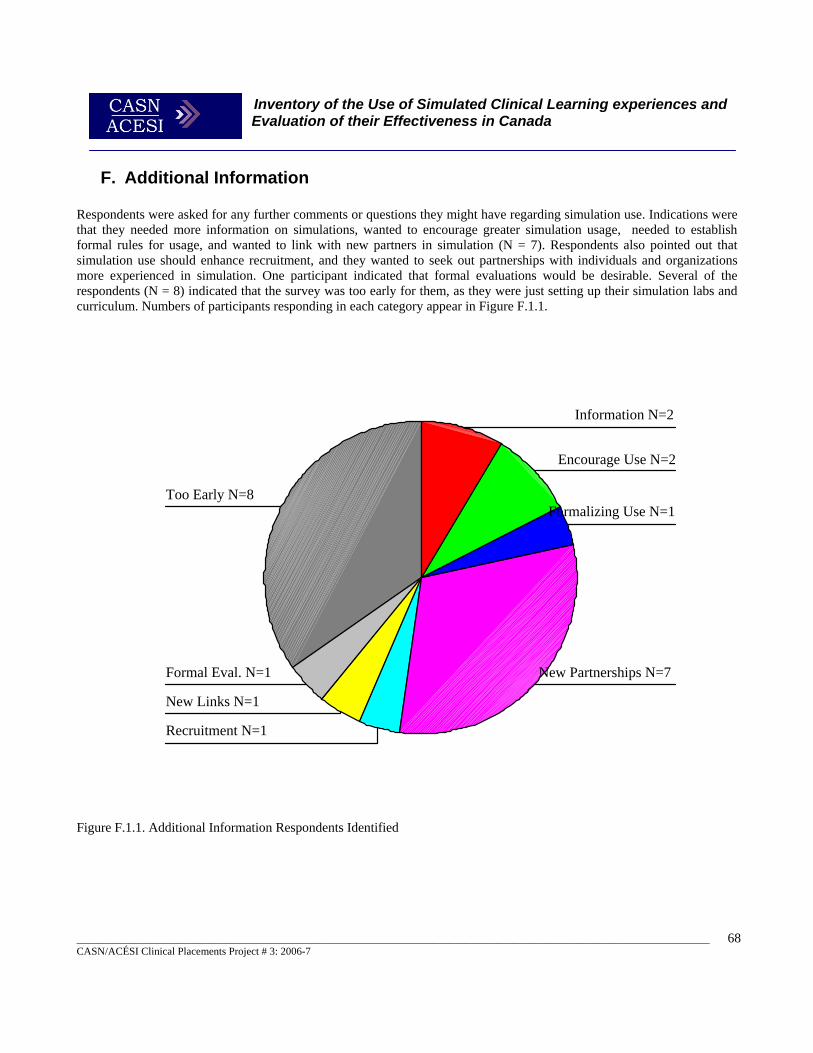
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
68
F. Additional Information Respondents were asked for any further comments or questions they might have regarding simulation use. Indications were that they needed more information on simulations, wanted to encourage greater simulation usage, needed to establish formal rules for usage, and wanted to link with new partners in simulation (N = 7). Respondents also pointed out that simulation use should enhance recruitment, and they wanted to seek out partnerships with individuals and organizations more experienced in simulation. One participant indicated that formal evaluations would be desirable. Several of the respondents (N = 8) indicated that the survey was too early for them, as they were just setting up their simulation labs and curriculum. Numbers of participants responding in each category appear in Figure F.1.1.
Figure F.1.1. Additional Information Respondents Identified
Too Early N=8
Formal Eval. N=1
New Links N=1
Recruitment N=1
New Partnerships N=7
Formalizing Use N=1
Encourage Use N=2
Information N=2
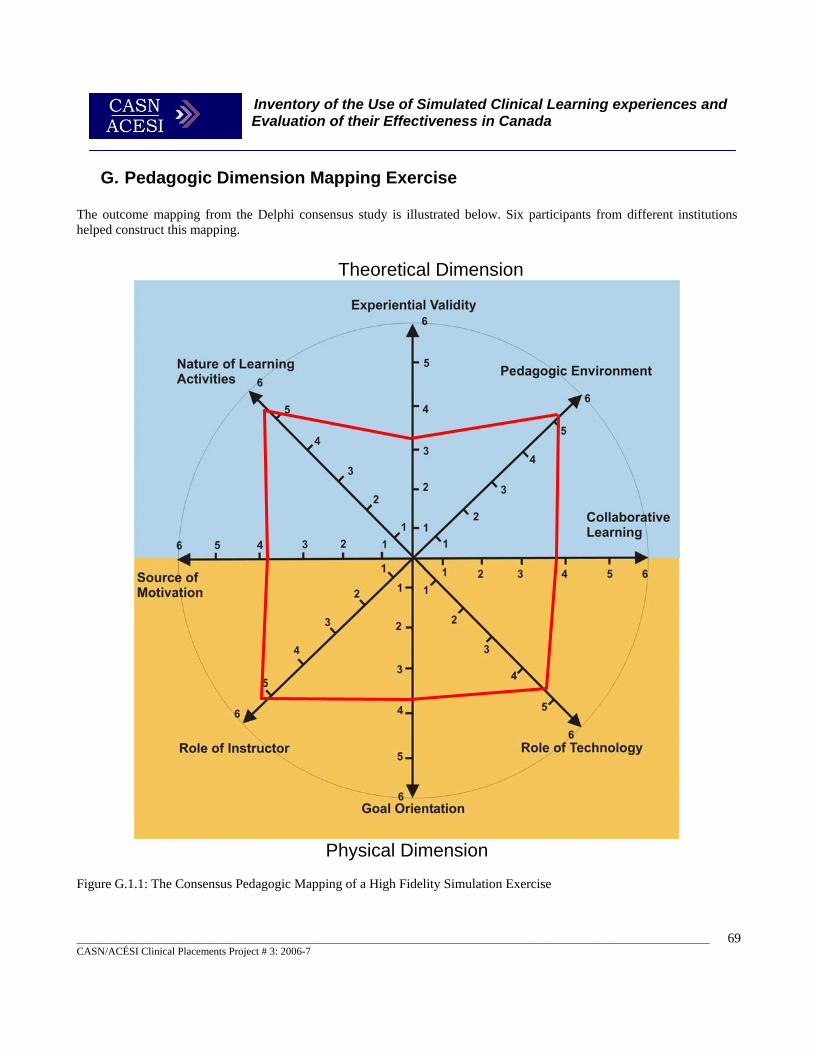
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
69
G. Pedagogic Dimension Mapping Exercise The outcome mapping from the Delphi consensus study is illustrated below. Six participants from different institutions helped construct this mapping.
Theoretical Dimension
Physical Dimension
Figure G.1.1: The Consensus Pedagogic Mapping of a High Fidelity Simulation Exercise

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
70
Summary of the Pedagogic Mapping Exercise A consensus mapping of a high-fidelity clinical simulation scenario (acute medical care of a young adult with dyspnoea) was undertaken by a group of educators. This simulation was one of the standard nursing simulations produced by METI® for use with their simulators, and was used with their permission. This resulted in the mapping in figure G1.1 above. The mapping was split into two dimensions, firstly the physical dimension to represent the more practical pedagogic themes and secondly the theoretical dimension to represent the more conceptual pedagogic dimensions. In the physical domain the mapping identified that the instructor’s role was highly facilitative, supporting the students in heuristic learning rather than providing didactic instruction. The role of the technology in the simulation was seen as providing a cognitive learning tool rather than as a surrogate for instruction. There was a clear consensus of ideas here, in both of these dimensions in that simulation was seen as a valuable tool for developing higher level skills with facilitated experiences rather than being used to replace instruction with exercises or drills. This was somewhat reflected in the Goal Orientation dimension whereby the simulation was scored as being slightly more generalizable than specific in its application. Educators felt that although the simulation was geared to the development of problem-solving and clinical critical thinking skills, (as transferable skills), the simulation also provided some highly specific clinical psycho-motor skills as goals. The source of motivation was seen as somewhat varied in that it could be extrinsic or intrinsic, depending if the simulation was being used for evaluation of performance. The overall consensus was that this simulation provided slightly more intrinsic motivation to the student. Likewise the Collaborative Learning dimension could be varied depending if the simulation were run as an individualised activity (or team activity with minimal interaction), or team based collaborative exercise. It was suggested that the activity held a slightly more collaborative focus as the student would need to engage other healthcare professionals to complete it effectively. In the theoretical dimension there was a clear consensus that the Nature of Learning Activity was highly process rather than product focused. This again reflected the heuristic nature of the simulation exercise and the intense resource based nature of the learning experience. Students were seen as being encouraged to discover solutions in this exercise rather than directed to a specific solution by the instructor. One interesting finding from this exercise was that Experiential Validity was seen as only marginally abstract, and that the application of the learning from this experience in practical real-life situations was not seen as very high. This may have been a product of some disagreement between the educators in this area resulting in a neutral overall score for this aspect. Lastly, the Pedagogic Environment was viewed as highly constructivist as opposed to instructivist, clearly indicating that this simulation exercise was seen as an active engaging learning experience.

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
71
Conclusions This study has revealed several interesting trends in simulation usage within education for nursing and other health professions in Canada, and there are a number of areas where there is a lack of evidence, and conflicting views amongst professional educators. 1. What is the current practice in using simulated learning experiences for nursing and other health professional students
in Canada?
There is a clear trend of rapidly increasing use of simulation in professional healthcare education practice evident from both the literature and survey results. This seems to have been driven in part by improved technologies and the availability of higher-fidelity simulation equipment. Overall, 70% of all respondents are using simulation and 52% are using high fidelity simulation in their provision of education. Another major factor influencing growth here is the increased pressures on educators to deliver training of ever more complex technical skills with limited opportunities for actual real-life clinical practical experience within short time frames. Some institutions are considering the replacement of some clinical elements with simulated learning activities, although none currently reported completely replacing any practicum with a simulated experience. Nursing education has a long history of using low and intermediate fidelity simulation in education. It is now rapidly adopting high-fidelity simulation as a significant component in its practice. Simulation forms a significant part of the curriculum in undergraduate, graduate and continuing professional education provision for most health professionals in Canada.
2. What types of simulated learning experiences are used, for what purposes, and by whom?
There are a wide range of simulation activities being engaged in, at all levels of educational practice. Simulation appears to be used the most in undergraduate education, followed by continuing professional development, and the least use in graduate programs. This likely reflects the nature of these programs and activities being simulated. Classroom based simulation was widely prevalent, being used for such things as role-play exercises for communication skills, and simulated care management exercises. The use of high-fidelity clinical simulation is most well developed in medical professional education (particularly anaesthesia, surgery, and ER practice), dentist, paramedic and respiratory therapist preparation. It is also now becoming highly prevalent in nursing, occupational therapy, physiotherapy, midwifery, and care aide preparation. Intermediate level simulation represents a significant part of the nursing curriculum in both time and numbers involved. This was reflected by the highest use in terms of time spent on simulation activities reported (approximately 28 hours a week of simulation use per nursing institution reporting), and most users reported accessing simulation resources. Acute client care forms the main focus for simulated learning activities. The types of activities most commonly simulated ranged widely from psycho-motor skills practice, to interdisciplinary team based activities. In medical education, high-fidelity simulators are used to train students in a wide range of clinical procedures such as suturing, intubation, laparoscopic surgery and endoscopy. They are also used for complex team based scenarios, including complete surgical simulations in a simulated Operating Room. Many centres were using Standardised Patients (scripted actors) to simulate normal and easily mimicked conditions, and using the new high-fidelity electro-mechanical patient simulators for simulating more complex patho-physiological changes and conditions. Nurse educators were using simulation for a similar wide range of activities from respiratory assessment and CPR to care management in acute emergencies. The use of intermediate level simulation was a common theme with most institutions describing “Skills Lab” activities for task training in this domain (such as practicing wound care, or catheterization). The trends in the use of high-fidelity simulation in nursing suggest these are now being used for higher order skills development such as critical thinking/clinical problem solving exercises and team work involving

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
72
complete client centred simulations, rather than task training activities. The use of simulations to orientate students to new and unfamiliar acute health care environments was also reported.
3. What is the evidence for the effectiveness of using simulated learning experiences? The effectiveness of simulation has been most clearly argued from the perspective of improved client safety. This is a generally accepted principle, but not conclusively proven. In a recent study exploring the impact of video simulations on training surgeons, Ziv et al (2005, 2003) and Scerbo (2004) highlighted simulation as an ethical imperative for medical education in order to reduce adverse events. In other professions (such as aircrew training), safety remains a key reason for utilizing simulation-based training. Simulations’ effectiveness still remains to be conclusively demonstrated in nursing. In professions outside of nursing, literature suggests evidence of faster skill acquisition and performance improvements. Several comparative studies have been undertaken to validate the effectiveness of simulation as a teaching tool compared with traditional methods. These generally suggest simulation is more effective, but in many areas it has yet to be established as superior to traditional methods. All physician respondents, and a significant portion of nurses (54%), respiratory therapists (43%), and those representing educational institutions (50%) indicated that simulations somewhat met their needs for practice education. There were no respondents that indicated simulation exceeded their training needs; however, 21% of nurses, 25% of paramedics and 19% of those representing educational institutions noted that simulations were inadequate as training aids. In many cases, the current level of technology available was identified as inadequate. For example, when administering IVs, the variety of vein placements and anatomical variation in live patients was not considered reproducible even in the latest high fidelity simulators.
4. What evidence is available from economic evaluations of simulated learning experiences?
The cost-effectiveness of simulation remains a contentious issue in the literature and amongst participants in this study. Cost-benefit is difficult to determine as many of the benefits of simulation are not easily quantifiable in monetary terms (e.g. improved client safety, or better prepared students). It may be easier to establish cost-effectiveness and cost-efficiency, but currently this also remains unclear. Studies exploring the efficiency of simulation are rather sparse in the literature. Wong, et al (2004) explored the use of full scale computer simulators in anesthesia training and evaluation, and found that their cost-efficiency was at least questionable. Haluck & Krummel (2000) exploring the value of computers and virtual reality and suggested that simulation might be more cost-efficient compared to the current system of surgical resident education. In the use of simulation for distance education, it seems there is more evidence. Von Lubitz et al (2003) indicated that in medical education, preliminary data on distance-based high-fidelity human patient simulation indicates it is more cost-efficient that current methods. Studies have suggested that clinical simulation offers advantages over traditional medical education methods that include lower costs, both direct and indirect (Grenvik et al, 2004) but in specific instances simulation has been shown to be more cost effective, but a less effective teaching method (Theroux & Pearce, 2006). Ninety-six percent of respondents had not conducted any formal cost-benefit/cost-effectiveness/cost-efficiency evaluations of their simulation practices, and only eighteen percent thought that simulation was very cost effective. Generally there was a perception that simulation was cost-effective and cost-efficient. This probably reflects the perception that simulation is a significant contributor to client safety, and is therefore judged as an effective learning technique, although possibly in terms of efficiency, respondents were a little less certain.
5. What content areas have been identified in the literature as more appropriate to simulated experiences?
Simulation based training has proved valuable in areas where experiential learning may not be possible due to time, cost or operational constraints such as client/student safety and accessing experience presents problems (Chung &

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
73
Huda 1999). The use of simulations as learning tools has been growing in many areas of health care education, and is proving its value in the simulation of complex psycho-motor tasks (such as surgical procedures, airway intubation, insertion of central lines, arterial lines, chest tubes and emergency tracheostomies), assessment of abnormal physiological responses, and in clinical decision making practice. The experience in the health professional education setting suggests high-fidelity simulation has an increasing role to play in the attainment of more complex psycho-motor skills, e.g. with apparatus or procedural operations, (Dutta et al, 2006). However, other forms of lower fidelity simulation have also been found to be very effective in health professional education, including role play, case studies, and task-trainers, and these have a long established base of research to support their effectiveness for training in communication skills and team work (Beaubien et al, 2004). The use of simulated patient based experiences using real data have shown great promise in developing clinical decision making skills, and student self-efficacy in this area. For example Steadman et al (2006) even suggest simulation-based training is superior to problem-based learning for the acquisition of critical assessment and management skills.
6. What clinical simulation learning activities, including inter-professional learning experiences, exist in Canada?
The range of clinical experiences in Canada mirrors those available in other developed counties. There is a wide range of resources available and there are several large established centres engaged in using simulations for multi-disciplinary use. For example the McGill Medical Simulation Centre in Quebec, the University of Toronto’s Faculty of Nursing’s Clinical Simulation Learning Centre and Canadian Simulation Centre for Human Performance and Crisis
Management Training in Ontario, the Algonquin College Health Studies Simulation Lab in Ontarion, the Alberta Centre for Emergency Medical Services Simulation at Grant MacEwan College, and the Centre of Excellence for Surgical Education and Innovation in Vancouver, British Columbia. When asked about the value of these resources for interdisciplinary education, there was an overall consensus that this is a good use of these techniques and technologies. Some centres were already running inter-disciplinary simulation sessions, and this was common practice in aircrew and military healthcare personnel training. Proportions of each profession using interdisciplinary training varied considerably and forty four percent of all professions reported using some interdisciplinary training. Physiotherapy educators indicated that they had comparatively high numbers of interdisciplinary opportunities. Forty nine percent of nursing educators surveyed responded that they were involved in interdisciplinary simulation based education, whilst dental programs had the least activity in this area. Professional development programs seem to be engaged in most interdisciplinary opportunities and intermediate and high fidelity simulations seemed to be used the most for this type of activity.
7. What is the feasibility, utility and effectiveness of simulated learning experiences as an augmentation to more traditional clinical placements?
As an augmentation to current clinical practice, there is good evidence that simulation has significant benefits. The most cited ones being improved client safety and better prepared practitioners (Dutta et al, 2006; Lavele et al, 2006; Henneman & Cunningham (2005). Simulation was seen as very beneficial as an adjunct to clinical practice in helping reduce anxieties for students, assisting them to organize their thoughts, and prioritize their care. It was characterized as providing a safe environment for learning and making mistakes. As an adjunct to clinical experience, it was valued by educators for better preparing students for practice, and giving experience in a range of conditions that students would get little opportunity to engage in real world practice. Augmentation of clinical practice appeared the most favourable reason for using simulation, and was cited as the most appropriate use of these techniques and technologies. Seventy percent of all respondents in this study indicated that they used simulated learning as an augmentation to clinical learning experience. Nursing educators reported using simulation to augment experience slightly less than the average compared to other health care professions. High and intermediate fidelity simulations were used to augment practice more than low fidelity simulations. When asked to what degree users thought simulation could be used to augment

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
74
clinical practical experience, the average response fell between ‘a bit’ and ‘a significant amount’. None of the respondents thought that it was not feasible to augment clinical practical experience with simulation. However, the pressures leading this expansion, and particularly moving towards high fidelity simulation replacing practical experience, appear to be seen as areas of concern by many educators. Only 11% of respondents indicated that they currently used simulation as an alternative to clinical practical experience. No respondents reported that they completely replaced any practical experiences with simulation, and the hours replaced ran from 8 to 40 hours per program. Medical educators gave simulation the highest rating in their perception of its ability to replace practice out of all the professions. Of the few that did report replacing practice with simulation, most reported used simulation to replace less than two days of actual practical experience. Respondents were also asked to what degree they thought simulation could be used to replace clinical practical experience, and were given five choices ranging from ‘none’ ‘to a large degree.’ It is of interest to note that none of the respondents indicated ‘to a large degree’ and 21% of respondents stated “none.” When categorized by level of use, Professional Development educators gave simulation the lowest rating for its ability to replace clinical practical experience. Activities that educators thought simulation could be used to replace included central venous line placement, and specific skills certification/recertification (e.g. CPR). It is of note that thirty two percent of respondents did not think that simulation could replace clinical practical experience at all.
Recommendations Simulated clinical learning offers significant advantages over traditional educational methods including the provision of a safe environment for both patient and student during training in high risk procedures; unlimited exposure to rare but complicated clinical events; the ability to manipulate training opportunities rather than wait for a suitable situation to arise; the ability to provide immediate feedback; the opportunity to standardize and evaluate performance; the opportunity to repeat performance; and the ability to efficiently organize team training (including interdisciplinary team training (after Grenvik et al, 2004). It also, arguably, presents the opportunity to lower costs in certain instances. There are then, significant reasons for health professional educators to embrace the use of simulation in our clinical education activities, and we should do so. However, there also remain many unanswered questions and the empirical evidence to support the use of clinical simulation for nursing education remains somewhat sparse, particularly in terms of economic performance. Because of increasing pressure to find alternatives for clinical practical experience, there is a danger of seeing simulation as a panacea for all shortages of clinical experience. Currently, we do not have the evidence to support that presumption, and with the current state of the art, it would be more appropriate to seek to resolve these particular difficulties by other means. The nature of clinical practice with highly–complex client needs, and the unpredictable nature of events mean that currently, the ability of simulation to meet the needs of practice education remains limited. That does not mean that simulation has a large role to play in professional healthcare education, but that we need more information to seek the optimum balance between simulated and actual practice. The biggest question that remains has been identified as:
“Does a comprehensive strategy of competency-based training, using multiple modalities including simulation and supervised client care yield better outcomes for patients, fewer errors, or more efficient patient care and education than does the current system of mostly apprenticeship-based training?”
Dutta et al (2006)
The specific recommendations related to these issues, as derived from this project are summarised in the table overleaf:
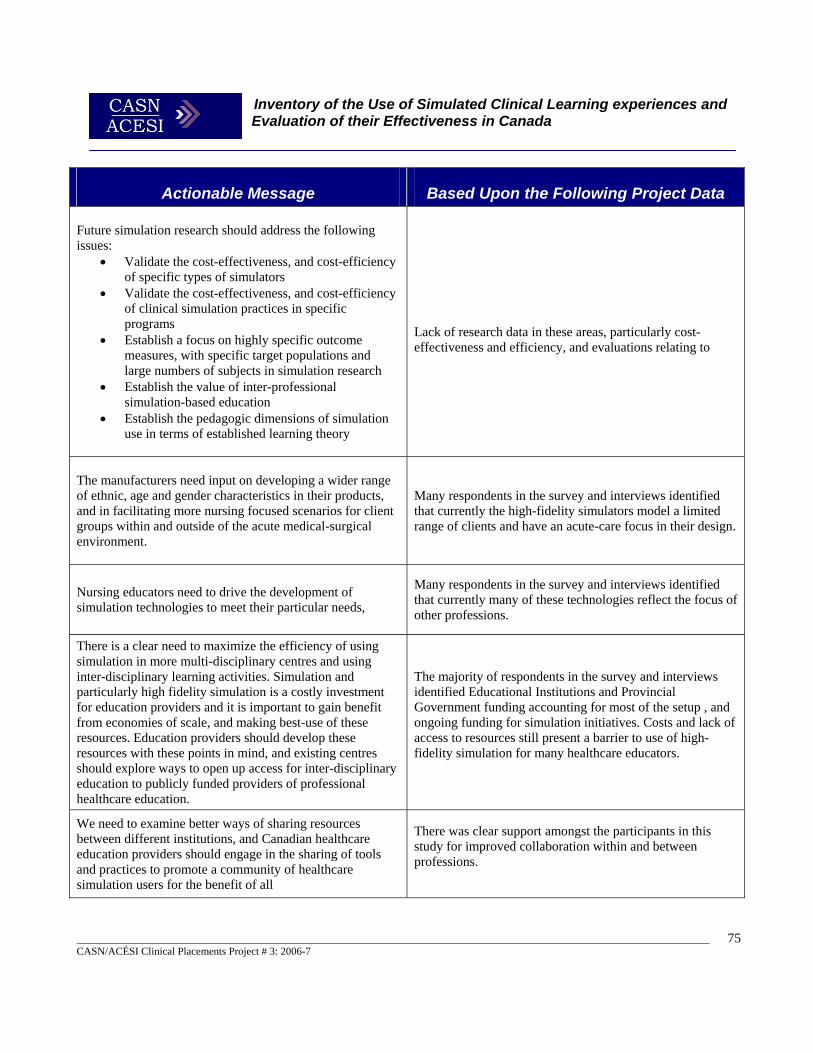
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
75
Actionable Message Based Upon the Following Project Data Future simulation research should address the following issues:
• Validate the cost-effectiveness, and cost-efficiency of specific types of simulators
• Validate the cost-effectiveness, and cost-efficiency of clinical simulation practices in specific programs
• Establish a focus on highly specific outcome measures, with specific target populations and large numbers of subjects in simulation research
• Establish the value of inter-professional simulation-based education
• Establish the pedagogic dimensions of simulation use in terms of established learning theory
Lack of research data in these areas, particularly cost-effectiveness and efficiency, and evaluations relating to
The manufacturers need input on developing a wider range of ethnic, age and gender characteristics in their products, and in facilitating more nursing focused scenarios for client groups within and outside of the acute medical-surgical environment.
Many respondents in the survey and interviews identified that currently the high-fidelity simulators model a limited range of clients and have an acute-care focus in their design.
Nursing educators need to drive the development of simulation technologies to meet their particular needs,
Many respondents in the survey and interviews identified that currently many of these technologies reflect the focus of other professions.
There is a clear need to maximize the efficiency of using simulation in more multi-disciplinary centres and using inter-disciplinary learning activities. Simulation and particularly high fidelity simulation is a costly investment for education providers and it is important to gain benefit from economies of scale, and making best-use of these resources. Education providers should develop these resources with these points in mind, and existing centres should explore ways to open up access for inter-disciplinary education to publicly funded providers of professional healthcare education.
The majority of respondents in the survey and interviews identified Educational Institutions and Provincial Government funding accounting for most of the setup , and ongoing funding for simulation initiatives. Costs and lack of access to resources still present a barrier to use of high-fidelity simulation for many healthcare educators.
We need to examine better ways of sharing resources between different institutions, and Canadian healthcare education providers should engage in the sharing of tools and practices to promote a community of healthcare simulation users for the benefit of all
There was clear support amongst the participants in this study for improved collaboration within and between professions.

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
76
Acknowledgements The authors would like to make special thanks and acknowledgement to the following for their help in facilitating the completion of this study: Ms. Madeline Buck B.Sc.(N), M.Sc.(A), Faculty Lecturer, B.Sc.(N.) Assistant Director School of Nursing & McGill Medical Simulation Centre, McGill University, Montreal, Quebec Mr. John Benham, Snr. Flight Simulation Instructor, The Air Canada Simulation Centre, Vancouver International Airport, Vancouver, British Columbia Lt. Gordon Peckham, A/OC, The Canadian Forces Trauma Training Centre (West), Vancouver, British Columbia

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
77
References Abbey, L. M. (2002). Interactive multimedia patient simulations in dental and continuing dental education. Dental Clinics of North America, 46(3), 575-587.th experts and novices. Studies in Health Technology & Informatics, 111, 414-417. Abrahamson, S., Denson, J. S., & Wolf, R. M. (2004). Effectiveness of a simulator in training anesthesiology residents. Quality & Safety in Health Care, 13(5), 395-397. Alinier, G., Hunt, B., Gordon, R., & Harwood, C. (2006). Effectiveness of intermediate-fidelity simulation training technology in undergraduate nursing education. Journal of Advanced Nursing, 54(3), 359-369. Allen, K. L., & More, F. G. (2004). Clinical simulation and foundation skills: an integrated multidisciplinary approach to teaching. Journal of Dental Education, 68(4), 468-474. Aucar, J. A., Groch, N. R., Troxel, S. A., & Eubanks, S. W. (2005). A review of surgical simulation with attention to validation methodology. [Review] [50 refs]. Surgical Laparoscopy, Endoscopy & Percutaneous Techniques, 15(2), 82- 89. Baez, A. (2005). Development of an objective structured clinical examination (OSCE) for practicing substance abuse intervention competencies: an application in social work education. Journal of Social Work Practice in the Addictions, 5(3), 3-20. Baker, C., Norton, P., Flintoft, V., Blais, R., Brown, A., Cox, J., Etchells, E., Ghali, W., Herbert, P., Majumdar, S., O'Beirne, M., Palacios-Derflingher, L., Reid, R., Sheps, S., & Tamblyn, R. (2004). The Canadian Adverse Events Study: the incidence of adverse events among hospital patients in Canada. CMAJ: Canadian Medical Association Journal, 170(11), 1678-1686. Barsuk, D., Ziv, A., Lin, G., Blumenfeld, A., Rubin, O., Keidan, I., et al. (2005). Using advanced simulation for recognition and correction of gaps in airway and breathing management skills in prehospital trauma care. Anesthesia & Analgesia, 100(3), 803-809. Bartfay, W. J., Rombough, R., Howse, E., & Leblanc, R. (2004). Evaluation. The OSCE approach in nursing education. Canadian Nurse, 100(3), 18-23. Beaubien J.M. and Baker D.P. (2004) The use of simulation for training teamwork skills in health care: how low can you go? Quality & Safety in Health Care, 13, 51-56 Beaulieu, M. D., Rivard, M., Hudon, E., Saucier, D., Remondin, M., & Favreau, R. (2003). Using standardized patients to measure professional performance of physicians. International Journal for Quality in Health Care, 15(3), 251-259. Becker, K., Rose, L., Berg, J., Park, H., & Shatzer, J. (2006). The teaching effectiveness of standardized patients. Journal of Nursing Education, 45(4), 103-111. Berg, D., Raugi, G., Gladstone, H., Berkley, J., Weghorst, S., Ganter, M., & Turkiyyah, G. (2001). Virtual reality simulators for dermatologic surgery: measuring their validity as a teaching tool. Dermatologic Surgery, 27(4), 370-374.

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
78
Blake, K. D., Mann, K. V., & Kaufman, D. M. (2001). Using standardized patients to identify students needing extra training in interviewing skills. Academic Medicine, 76(5), 537-538. Blake, K., Mann, K. V., Kaufman, D. M., & Kappelman, M. (2000). Learning adolescent psychosocial interviewing using simulated patients. Academic Medicine, 75(10 Suppl), S56-58. Bond, W. F., & Spillane, L. (2002). The use of simulation for emergency medicine resident assessment... presented at the Council of Emergency Medicine Residency Directors (CORD) Consensus Conference on the ACGME Core Competencies: "Getting Ahead of the Curve," March 2002, Washington, DC. Academic Emergency Medicine, 9(11), 1295-1299. Bremner, M. N., & Brannan, J. D. (2000). A computer simulation for the entry-level RN: enhancing clinical decision making. Journal for Nurses in Staff Development, 16(1), 5-9. Brinchmann-Hansen, A., Wisborg, T., & Brattebo, G. (2004). [Simulation- an efficient way of learning in graduate and continuous medical education]. Tidsskrift for Den Norske Laegeforening, 124(16), 2113-2115. Buck, G. H. (1991). Development of simulators in medical education. Gesnerus, 48(1), 7-28. Cioffi, J., Purcal, N., & Arundell, F. (2005). A pilot study to investigate the effect of a simulation strategy on the clinical decision making of midwifery students. Journal of Nursing Education, 44(3), 131-134. Costanza, M. E., Luckmann, R., Quirk, M. E., Clemow, L., White, M. J., & Stoddard, A. M. (1999). The effectiveness of using standardized patients to improve community physician skills in mammography counselling and clinical breast exam. Preventive Medicine, 29(4), 241-248. CPSI/ICSP. (2005). Current State Report on Patient Simulation in Canada ,Edmonton, AB, Canada: Canadian Patient Safety Institute. Deanda, A., & Gaba, D. M. (1991). Role of Experience in the Response to Simulated Critical Incidents. Anesthesia & Analgesia, 72(3), 308-315. del Bueno, D. (2005). A crisis in critical thinking. Nursing Education Perspectives, 26(5), 278-282. Docherty, C., Hoy, D., Topp, H., & Trinder, K. (2005). eLearning techniques supporting problem based learning in clinical simulation. International Journal of Medical Informatics, 74(7-8), 527-533. Dunn, W. (Ed.). (2004). Simulators in Critical Care Medicine and Beyond. Society for Critical Care Medicine (SCCM) Press Publishers. Dutta S., Gaba D., Krummel T.M.(2006) To simulate of Not to Simulate: What is the Question.? Annals of Surgery, 243(3). Ebbert, D. W., & Connors, H. (2004). Standardized patient experiences: evaluation of clinical performance and nurse practitioner student satisfaction. Nursing Education Perspectives, 25(1), 12-15. El-Jardali, F., & Lagacé, M. (2005). Making hospital care safer and better: the structure-process connection leading to adverse events. Healthcare Quarterly, 8(2), 40-48.

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
79
Fletcher, M. (2005). Simulation: unique lab broadens education options. Canadian Nurse, 101(2), 10. Fried, M. P., Satava, R., Weghorst, S., Gallagher, A. G., Sasaki, C., Ross, D., Sinanan, M., Uribe, J. I., Zeltsan, M., Arora, H., & Cuellar, H. (2004). Identifying and reducing errors with surgical simulation. Quality & Safety in Health Care, 13(1). Gaba D.M. (2004) The future vision of simulation in health care, Quality & Safety in Health Care, 13(suppl 1), 2-10 Gallagher, A. G., & Cates, C. U. (2004). Virtual reality training for the operating room and cardiac catheterisation laboratory. Lancet, 364(9444), 1538-1540. Garrett, B. M., & Callear, D. (2001). The value of intelligent multimedia simulation for teaching clinical decision-making skills. Nurse Education Today, 21(5), 382-390. Gates, D., Fitzwater, E., & Succop, P. (2005). Reducing assaults against nursing home caregivers. Nursing Research, 54(2), 119-127. Goldenberg, D., Andrusyszyn, M., & Iwasiw, C. (2005). The effect of classroom simulation on nursing students' self- efficacy related to health teaching. Journal of Nursing Education, 44(7), 310-314. Grenvik, A., & Schaefer, J. (2004). From Resusci-Anne to Sim-Man: the evolution of simulators in medicine. Critical Care Medicine, 32(2 Suppl). Grenvik, A., Schaefer, J. J., 3rd, DeVita, M. A., & Rogers, P. (2004). New aspects on critical care medicine training. Current Opinion in Critical Care, 10(4), 233-237. Hatala, R., Kassen, B. O., Nishikawa, J., Cole, G., & Issenberg, S. B. (2005). Incorporating simulation technology in a Canadian internal medicine specialty examination: a descriptive report. Academic Medicine, 80(6), 554-556 Hemman, E. A. (2005). Improving combat medic learning using a personal computer-based virtual training simulator. Military Medicine, 170(9), 723-727. Heng, P. A., Cheng, C. Y., Wong, T. T., Xu, Y., Chui, Y. P., Chan, K. M., & Tso, S. K. (2004). A virtual-reality training system for knee arthroscopic surgery. IEEE Transactions on Information Technology in Biomedicine, 8(2), 217-227. Henneman, E., & Cunningham, H. (2005). Using clinical simulation to teach patient safety in an acute/critical care nursing course. Nurse Educator, 30(4), 172-177. Herold, G. (2005). Test flight: human simulation increases safety in nurse training. NurseWeek California, 18(21), 14-15. Hjelm-Karlson, K., & Stenbeck, H. (1997, 1997). A simulation that teaches clinical decision making in nursing. Proceedings of Nursing Informatics 1997: International Medical Informatics Association. Hotchkiss, M. A., Biddle, C., & Fallacaro, M. (2002). Assessing the authenticity of the human simulation experience in anesthesiology. American Association of Nurse Anesthetists Journal, 70(6), 470-473. Hravnak, M., Beach, M., & Tuite, P. (2007). Simulator technology as a tool for education in cardiac care. Journal of Cardiovascular Nursing, 22(1), 16-24.

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
80
Hravnak, M., Tuite, P., & Baldisseri, M. (2005). Expanding acute care nurse practitioner and clinical nurse specialist education: invasive procedure training and human simulation in critical care. AACN Clinical Issues: Advanced Practice in Acute & Critical Care, 16(1), 89-104. IOM. (2000). To Err Is Human: Building a Safer Health System. The Institute of Medicine (USA). Retrieved 28th February, 2007, from the World Wide Web: http://www.nap.edu/openbook/0309068371/html/ Konkle-Parker, D. J., Cramer, C. K., & Hamill, C. (2002). Standardized patient training: a modality for teaching interviewing skills. Journal of Continuing Education in Nursing, 33(5), 225-230. Krawczak, J., & Bersky, A. K. (1995). The development of automated client responses to computerized clinical simulation testing. Computers in Nursing, 13(6), 295-300. Kyrkjebø, J. M., Brattebø, G., & Smith-Strøm, H. (2006). Improving patient safety by using interprofessional simulation training in health professional education. Journal of Interprofessional Care, 20(5), 507-516. Lasater, K. (2005). The impact of high fidelity simulation on the development of clinical judgment in nursing students: an exploratory study. Unpublished Ed.D Thesis. 227 p., (Portland State University). Lauri, S. (1992). using a computer simulation program to assess the decision making process in child health care. Computers in Nursing, 10(40), 171-177. Lavele, B., Denning, S., Ihnken, L., Benney, A. & Loberg, N. (2006). Accelerated orientation of nurse-paramedic critical care flight crews using high-fidelity simulation. Critical Care Nurse, 26(2), S28. Lavell, B., Sullivan, D., & Dahl, W. (2006). He's real! Using high-fidelity simulation in critical care and progressive care orientation. Critical Care Nurse, 26(2), S28-29. Long, R. E. (2005). Using simulation to teach resuscitation: an important patient safety tool. Critical Care Nursing Clinics of North America, 17(1), 1-8. Lowdermilk, D. L., & Fishel, A. H. (1991). Computer simulations as a measure of nursing students' decision-making skills. Journal of Nursing Education, 30(1), 34-39. Lyons, J., Miller, M., & Milton, J. (1998). Learning with technology: use of case based physical and computer simulations in professional education. Contemporary Nurse:- A journal for the Australian nursing profession, 7(2), 98-102. Mastrangelo, M. J., Jr., Stich, J., Hoskins, J. D., Witzke, W., George, I., Garrison, J., Nichols, M., & Park, A. E. (2002). Advancements in immersive VR as a tool for preoperative planning for laparoscopic surgery. Studies in Health Technology & Informatics, 85, 274-279. McArthur, J. R., Bolles, J. R., Fine, J., Kidd, P., & Bessis, M. (1989). Interactive computer-video modules for health sciences education. Methods of Information in Medicine, 28(4), 360-363. Medley, C. F., & Horne, C. (2005). Educational innovations. Using simulation technology for undergraduate nursing education. Journal of Nursing Education, 44(1), 31-34.

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
81
Niemeyer, G., Kuchenbecker, K. J., Bonneau, R., Mitra, P., Reid, A. M., Fiene, J., & Weldon, G. (2004). THUMP: an immersive haptic console for surgical simulation and training. Studies in Health Technology & Informatics, 98, 272-274. Novack, D. H., Dube, C., & Goldstein, M. G. (1992). Teaching medical interviewing. A basic course on interviewing and the physician-patient relationship. Archives of Internal Medicine, 152(9), 1814-1820. Novak, S. (1993). Multimedia in Simulation and Training. Proceedings of the British computer Society Conference: multimedia applications, Leeds, London, UK. O'Connor, F. W., Albert, M. L., & Thomas, M. D. (1999). Incorporating standardized patients into a psychosocial nurse practitioner program. Archives of Psychiatric Nursing, 13(5), 240-247. O'Neill, E., Dluhy, N., Hansen, A., & Ryan, J. (2006). Coupling the N-CODES system with actual nurse decision-making. CIN: Computers, Informatics, Nursing, 24(1), 28-36. Patow, C. A. (2004). Improving patient safety through simulation technology. AHIP Cover, 45(3), 74-77. Petrusa, E. R. (2004). Taking standardized patient-based examinations to the next level. Teaching & Learning in Medicine, 16(1), 98-110. Pham, T., Roland, L., Benson, K. A., Webster, R. W., Gallagher, A. G., & Haluck, R. S. (2005). Smart tutor: a pilot study of a novel adaptive simulation environment. Studies in Health Technology & Informatics, 111, 385-389. Qayumi, A., Kurihara, Y., Imai, M., Pachev, G., Seo, H., Hoshino, Y., Cheifetz, R., Matsuura, K., Momoi, M., Saleem, M., Lara Guerra, H., Miki, Y., & Kariya, Y. (2004) Comparison of computer-assisted instruction (CAI) versus traditional textbook methods for training in abdominal examination (Japanese experience). Medical Education, 38(10), 1080-1088. Qayumi K, & Qayumi T. (1999). "Computer-assisted learning: cyberPatient--a step in the future of surgical education." Journal of investigative surgery 12(6): 307-17.Quality & Safety in Health Care, 13: 2-10 Reeves, T. C., & Laffey, J. M. (1999). Design assessment, and evaluation of a problem based learning environment in undergraduate engineering. Higher Education Research and Development Journal, 18(2), 219-232. Rehmann A , Mitman R, Reynolds M. A (1995) Handbook of flight simulation fidelity requirements for human factors research. Technical Report No. DOT/FAA/CT-TN95/46. Wright-Patterson AFB, OH: Crew Systems Ergonomics Information Analysis Center, 1995. Rennie, A., & Main, M. (2006). Student midwives' views of the objective structured clinical examination. British Journal of Midwifery, 14(10), 602-607. Ro, C. Y., Toumpoulis, I. K., Ashton, R. C., Jr., Jebara, T., Schulman, C., Todd, G. J., Derose, J. J., Jr., & McGinty, J. J. (2005). The LapSim: a learning environment for both experts and novices, Studies in Health Technology and Informatics, 111, 414-7 Robertson, B. (2006). An obstetric simulation experience in an undergraduate nursing curriculum. Nurse Educator, 31(2), 74-78.

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
82
Salas E., Burke C.S., Bowers C.A., Wilson K.A. (2001) Team training in the skies: does crew resource management (CRM) training work? Human Factors, 43, 641–74 Saleem M. Lara-Guerra H. Miki Y. Kariya Y. (2004) Comparison of computer-assisted instruction (CAI) versus traditional textbook methods for training in abdominal examination (Japanese experience). Medical Education. 38(10):1080-8. Scerbo, M. W. (2004). Medical virtual reality simulation: enhancing safety through practicing medicine without patients. Biomedical Instrumentation & Technology, 38(3), 225-228. Schendel, S., Montgomery, K., Sorokin, A., & Lionetti, G. (2005). A surgical simulator for planning and performing repair of cleft lips. Journal of Cranio-Maxillo-Facial Surgery, 33(4), 223-228. Schoening, A., Sittner, B., & Todd, M. (2006). Simulated clinical experience: nursing students' perceptions and the educators' role. Nurse Educator, 31(6), 253-258. Shaw, J. (2006). Nursing students use life-size mannequins to gain practical experience. Registered Nurse Journal, 18(1), 23-25. Shemer, S., & Shoenfeld, Y. (2003). Terror and Medicine - Medical Aspects of Biological, Chemical and Nuclear Terrorism, PABST Science Publishers. Spencer, K. (2006). Patient simulation to enhance patient safety. Plastic Surgical Nursing, 26(4), 195-197. Spicer, M. A., van Velsen, M., Caffrey, J. P., & Apuzzo, M. L. (2004). Virtual reality neurosurgery: a simulator blueprint. Neurosurgery, 54(4), 783-797; Discussion 797-788. Steadman, R. H., Coates, W. C., Huang, Y. M., Matevosian, R., Larmon, B. R., McCullough, L., & Ariel, D. (2006). Simulation-based training is superior to problem-based learning for the acquisition of critical assessment and management skills. Critical Care Medicine, 34(1), 151-157. Sutherland L.M., Middleton P.F., Anthony A., Hamdorf J., Cregan P., Scott D., Maddern G.J.(2006) Surgical simulation: a systematic review. Annals of Surgery, 243, 291-300. Sutnick, M. R., & Carroll, J. G. (1981). Using patient simulators to teach clinical interviewing skills. Journal of the American Dietetic Association, 78(6), 614-616. Thistlethwaite, J. (2004). Simulated patient versus clinician marking of doctors' performance: which is more accurate? Medical Education, 38(4). Van Sell, S., Johnson-Russell, J., & Kindred, C. (2006). The teaching power of high-tech dummies. Registered Nurse, 69(4), 30-35, 32p. Vaughan, D. (2006). Simulated NICU helps RNs hone skills. Nursing Spectrum - New England Edition, 10(16), 10-11. Wang Y , Chui C, Lim H, et al. (1998) Real-time interactive simulator for percutaneous coronary revascularization procedures. Computer Aided Surgery 3, 211–27.

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
83
Watkinson, G., Spencer, A., Monger, E., Weaver, M., Gobbi, M., Lathlean, J., & Bryant, S. (2004). Virtual interactive practice: utilizing healthcare information systems to contextualize the skills associated with clinical decision making within nurse education. Medinfo, 11(1), 746-752. Welk, A., Splieth, C., Rosin, M., Kordass, B., & Meyer, G. (2004). DentSim - a future teaching option for dentists. International Journal of Computerized Dentistry, 7(2), 123-130. Weller, J. M., Bloch, M., Young, S., Maze, M., Oyesola, S., Wyner, J., Dob, D., Haire, K., Durbridge, J., Walker, T., & Newble, D. (2003). Evaluation of high fidelity patient simulator in assessment of performance of anaesthetists. British Journal of Anaesthesia, 90(1), 43-47. Weller, J., Robinson, B., Larsen, P., & Caldwell, C. (2004). Simulation-based training to improve acute care skills in medical undergraduates. New Zealand Medical Journal, 117(1204), 22. White, J. E. (1995). Using interactive video to add physical assessment data to computer-based patient simulations in nursing. Computers in Nursing, 5, 233-235 Wierinck, E., Puttemans, V., Swinnen, S., & van Steenberghe, D. (2005). Effect of augmented visual feedback from a virtual reality simulation system on manual dexterity training. European Journal of Dental Education, 9(1), 10-16. Wilford, A., & Doyle, T. (2006). Product focus. Integrating simulation training into the nursing curriculum. British Journal of Nursing, 15(17), 926. Wood, D. (2006). Fake it to make it. Nursing Spectrum - Florida Edition, 16(11), 24-25. Yee, B., Naik, V. N., Joo, H. S., Savoldelli, G. L., Chung, D. Y., Houston, P. L., Karatzoglou, B. J., & Hamstra, S. J. (2005). Nontechnical skills in anesthesia crisis management with repeated exposure to simulation-based education. Anesthesiology, 103(2), 241-248. Ziv, A., Ben-David, S., & Ziv, M. (2005). Simulation based medical education: an opportunity to learn from errors. Medical Teacher, 27(3), 193-199.
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
84
Appendices Appendix A: Participants ....................................................................................................................................................... 85 Appendix B: Documents& Instruments ................................................................................................................................. 87 Appendix C – Project Advisory Committee Membership.................................................................................................... 119 Appendix D – Ethical Approval ........................................................................................................................................... 120 Appendix E – Detailed Statistical Findings.......................................................................................................................... 122
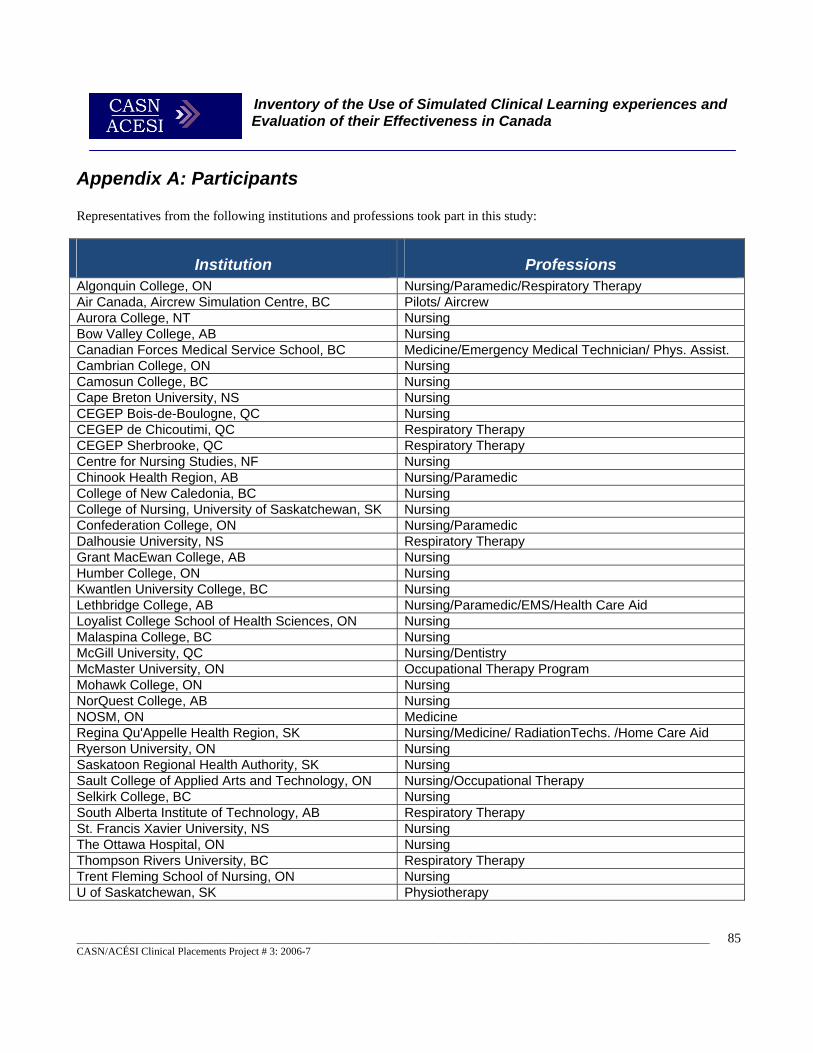
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
85
Appendix A: Participants Representatives from the following institutions and professions took part in this study:
Institution Professions Algonquin College, ON Nursing/Paramedic/Respiratory Therapy Air Canada, Aircrew Simulation Centre, BC Pilots/ Aircrew Aurora College, NT Nursing Bow Valley College, AB Nursing Canadian Forces Medical Service School, BC Medicine/Emergency Medical Technician/ Phys. Assist. Cambrian College, ON Nursing Camosun College, BC Nursing Cape Breton University, NS Nursing CEGEP Bois-de-Boulogne, QC Nursing CEGEP de Chicoutimi, QC Respiratory Therapy CEGEP Sherbrooke, QC Respiratory Therapy Centre for Nursing Studies, NF Nursing Chinook Health Region, AB Nursing/Paramedic College of New Caledonia, BC Nursing College of Nursing, University of Saskatchewan, SK Nursing Confederation College, ON Nursing/Paramedic Dalhousie University, NS Respiratory Therapy Grant MacEwan College, AB Nursing Humber College, ON Nursing Kwantlen University College, BC Nursing Lethbridge College, AB Nursing/Paramedic/EMS/Health Care Aid Loyalist College School of Health Sciences, ON Nursing Malaspina College, BC Nursing McGill University, QC Nursing/Dentistry McMaster University, ON Occupational Therapy Program Mohawk College, ON Nursing NorQuest College, AB Nursing NOSM, ON Medicine Regina Qu'Appelle Health Region, SK Nursing/Medicine/ RadiationTechs. /Home Care Aid Ryerson University, ON Nursing Saskatoon Regional Health Authority, SK Nursing Sault College of Applied Arts and Technology, ON Nursing/Occupational Therapy Selkirk College, BC Nursing South Alberta Institute of Technology, AB Respiratory Therapy St. Francis Xavier University, NS Nursing The Ottawa Hospital, ON Nursing Thompson Rivers University, BC Respiratory Therapy Trent Fleming School of Nursing, ON Nursing U of Saskatchewan, SK Physiotherapy
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
86
Université de Moncton, NB Respiratory Therapy Université du Québec à Chicoutimi, QC Nursing Université du Québec à Trois-Rivières, QC Nursing Université du Québec, QC Paramedic Université Laval, QC Dentistry, Nursing Université Sainte-Anne, NS Paramedic University Health Network, Toronto Gen. Hosp., ON Medicine University of Alberta, AB Nursing University of British Columbia Okanagan, BC Nursing University of British Columbia, BC Nursing University of Calgary, AB Nursing University of Lethbridge, AB Nursing University of Manitoba, MB Physiotherapy/ Respiratory Therapy/ Occupational T. University of Manitoba, MB Nursing University of Northern British Columbia, BC Nursing University of Ontario Institute of Technology, ON Nursing University of Toronto, ON Physiotherapy University of Victoria, BC Nursing University of Western Ontario, ON Nursing University of Windsor, ON Nursing York University, ON Nursing
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
87
Appendix B: Documents& Instruments
Inventory of the Use of Simulated Clinical Learning Experiences and Evaluation of their Effectiveness. Principal Investigator: Dr Bernie Garrett, Assistant Professor. Monday, May 05, 2006 Dear Colleague, I will shortly be writing to you to you to ask you to participate in a survey to investigate the use of simulated learning experiences for clinical health professional education in Canada. The Project The aim of this project is to explore the use of simulated clinical learning experiences in healthcare professional education and training in Canada and evaluate the effectiveness of this approach. We wish to establish the range, evidence base and best practices in the use of simulated learning for healthcare professional education and training. The overall aim is to develop an inventory of simulation use for healthcare professional preparation in Canada, and explore the evidence base for its use, cost-effectiveness and possibilities for multi-professional collaboration. In this way the possibilities for simulation to provide alternatives to traditional clinical experience for nurse education, and its limitations may be established. This project has been commissioned by the CASN/ACESI. This project seeks to: 1. Establish current practices of using simulated learning experiences for nursing and other health professional students in Canada, and explore the potential for collaboration 2. Identify the types of simulated learning resources and experiences used, for professional healthcare education and identify which professional groups are using them, and at which levels 3. Establish evidence of the effectiveness of using simulated learning experiences 4. Explore what evidence is available from economic evaluations of simulated learning experiences to support their use or otherwise 5. Identify areas from the literature of specific content areas that are more appropriate for the use of simulated experiences 6. Explore the feasibility, utility and effectiveness of using simulated learning experiences as an augmentation to more traditional clinical placements
The University of British Columbia School of Nursing T201-2211, Wesbrook Mall Vancouver, B.C. V6T 2B5 Phone: (604) 822-7417 Fax: (604) 822-7466
REQUEST TO PARTICIPATE IN A STUDY

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
88
7. Investigate the potential for using a collaborative framework for implementing clinical simulations using e-learning technologies for professional healthcare education and training in Canada. Yours faithfully, We would very much value your participation in this survey, or if you feel you are not the appropriate person to contribute, perhaps you could identify a suitable colleague at your institution who could participate in this important work. Many thanks for considering this request, Yours faithfully, Dr Bernie Garrett Assistant Professor University of British Columbia School of Nursing
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
89
Inventory of the Use of Simulated Clinical Learning Experiences and Evaluation of their Effectiveness. Principal Investigator: Dr Bernie Garrett, Assistant Professor. Tuesday, June 06, 2006 Dear Colleague, I am writing to you to ask you to participate in a survey to investigate the use of simulated learning experiences for clinical health professional education in Canada. The Project The aim of this project is to explore the use of simulated clinical learning experiences in healthcare professional education and training in Canada and evaluate the effectiveness of this approach. We wish to establish the range, evidence base and best practices in the use of simulated learning for healthcare professional education and training. The overall aim is to develop an inventory of simulation use for healthcare professional preparation in Canada, and explore the evidence base for its use, cost-effectiveness and possibilities for multi-professional collaboration. In this way the possibilities for simulation to provide alternatives to traditional clinical experience for nurse education, and its limitations may be established. This project has been commissioned by the CASN/ACESI. This project seeks to: 1. Establish current practices of using simulated learning experiences for nursing and other health professional students in Canada, and explore the potential for collaboration 2. Identify the types of simulated learning resources and experiences used, for professional healthcare education and identify which professional groups are using them, and at which levels 3. Establish evidence of the effectiveness of using simulated learning experiences 4. Explore what evidence is available from economic evaluations of simulated learning experiences to support their use or otherwise 5. Identify areas from the literature of specific content areas that are more appropriate for the use of simulated experiences 6. Explore the feasibility, utility and effectiveness of using simulated learning experiences as an augmentation to more traditional clinical placements 7. Investigate the potential for using a collaborative framework for implementing clinical simulations using e-learning technologies for professional healthcare education and training in Canada.
The University of British Columbia School of Nursing T201-2211, Wesbrook Mall Vancouver, B.C. V6T 2B5 Phone: (604) 822-7417 Fax: (604) 822-7466
INVITATION TO PARTICIPATE IN A STUDY

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
90
Why am I being asked? I am inviting you to be involved as a health care professional educator who may be using simulated learning to support clinical education and training. What is involved? Participation is quite straightforward and completely voluntary. All that is asked is that you or an appropriate colleague from your institution completes a short online questionnaire. This questionnaire should take no more than 30 minutes at maximum to complete. To access the questionnaire, simply go to http://www.surveymonkey.com/s.asp?u=267482100855 on the Web and start the questionnaire you will find there. For those institutions currently using simulation here is also an opportunity to be involved in two further research activities (a short Delphi consensus questionnaire on the pedagogic value of simulation, and a telephone interview). All participants will be sent a copy of the final report resulting from the study by e-mail. The Survey needs to be completed before the end of July. Confidentiality Summary findings from questions 1 to 12 explore basic information on the use of simulation and range of use in your institution and will be used to produce a national simulation inventory. Survey results from questions 13 to 35 explore views and practices and data will be aggregated for those questions, and for institutions or individuals will not be identifiable from their responses in any analysis, published or shared materials. All survey data will be kept secure on the Web-server and at the University of British Columbia. Contact for information about the study If you have any questions or desire further information with respect to this study, please contact Dr. Bernie Garrett at 604-822-7443 or by e-mail at [email protected]. Contact for concerns about the rights of research subjects: If you have any concerns about your treatment or rights as a research subject, you may contact the Research Subject Information Line in the UBC Office of Research Services at 604-822-8598. Consent: Participation or non-participation in the survey will not affect any relationships you or your institution may have with the investigators, CASN/ACESI or the University of British Columbia. By completing and submitting the questionnaire you will be certifying that you have read and understood the information presented here and have consented to take part in the study. Unfortunately, we cannot offer any remuneration for your participation in this study but would very much appreciate your input. Thank you very much for your time in considering this invitation and participating, if you choose to do so. Yours faithfully, Dr Bernie Garrett
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
91
Web Survey
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
92
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
93
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
94
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
95
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
96
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
97
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
98
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
99
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
100
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
101
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
102
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
103
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
104
Inventory of the Use of Simulated Clinical Learning Experiences and Evaluation of their Effectiveness. Principal Investigator: Dr Bernie Garrett, Assistant Professor. Tuesday, July 28, 2006 Dear Colleague, A short while ago wrote to you to invite you to participate in a survey being undertaken to investigate the use of simulated learning experiences for clinical health professional education in Canada. I just wanted to take this opportunity to see if you had any questions about the process or would like to respond, as we have not yet received a submission from your institution. If you would like to participate, there is still time as we have extended the deadline for submission,and we would very much value your input. I attach our original letter of invitation in case you do not have a copy. Thank you very much for your time in considering this invitation. Yours faithfully, Dr Bernie Garrett Assistant Professor University of British Columbia School of Nursing
The University of British Columbia School of Nursing T201-2211, Wesbrook Mall Vancouver, B.C. V6T 2B5 Phone: (604) 822-7417 Fax: (604) 822-7466
INVITATION TO PARTICIPATE IN A STUDY
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
105
Inventory of the Use of Simulated Clinical Learning Experiences and Evaluation of their Effectiveness. Principal Investigator: Dr Bernie Garrett, Assistant Professor. Monday August 14th 2006 Dear Colleague, Recently you participated in a survey to investigate the use of simulated learning experiences for clinical health professional education in Canada. Thank you very much for your response. At that time you indicated you would be prepared to participate in a further Delphi survey to explore the pedagogic value of simulation. I am now writing to you to invite you to participate in this additional short survey. The Project The aim of this project is to explore the use of simulated clinical learning experiences in healthcare professional education and training in Canada and evaluate the effectiveness of this approach. We wish to establish the range, evidence base and best practices in the use of simulated learning for healthcare professional education and training. The overall aim is to develop an inventory of simulation use for healthcare professional preparation in Canada, and explore the evidence base for its use, cost-effectiveness and possibilities for multi-professional collaboration. In this way the possibilities for simulation to provide alternatives to traditional clinical experience for nurse education, and its limitations may be established. This project seeks to: 1. Establish current practices of using simulated learning experiences for nursing and other health professional students in Canada, and explore the potential for collaboration 2. Identify the types of simulated learning resources and experiences used, for professional healthcare education and identify which professional groups are using them, and at which
The University of British Columbia School of Nursing T201-2211, Wesbrook Mall Vancouver, B.C. V6T 2B5 Phone: (604) 822-7417 Fax: (604) 822-7466
INVITATION TO PARTICIPATE IN A STUDY

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
106
levels 3. Establish evidence of the effectiveness of using simulated learning experiences 4. Explore what evidence is available from economic evaluations of simulated learning experiences to support their use or otherwise 5. Identify areas from the literature of specific content areas that are more appropriate for the use of simulated experiences 6. Explore the feasibility, utility and effectiveness of using simulated learning experiences as an augmentation to more traditional clinical placements 7. Investigate the potential for using a collaborative framework for implementing clinical simulations using e-learning technologies for professional healthcare education and training in Canada. Why am I being asked? I am inviting you to be involved as a health care professional educator who may be using simulated learning to support clinical education and training. What is involved? Participation is quite straightforward and completely voluntary. All that is asked is that you complete a short pedagogic mapping questionnaire. This questionnaire should take no more than 20 minutes at maximum to complete, and instructions and the questionnaire are attached. If you are prepared to be involved, would you please complete the questionnaire and return it to me in the prepaid envelope by Friday September the 8th 2006All participants will be sent a copy of the final report resulting from the study by e-mail. Confidentiality The personal identity of all participants in this questionnaire will be kept strictly confidential. All documents will be identified only by code number and kept in a locked filing cabinet in a locked office in the School of Nursing at UBC. Any data kept on electronic media at the School of Nursing will not include the name or personal details of the individual subject and will be encrypted. Subjects will not be identified by name in any reports of the completed study. Contact for information about the study If you have any questions or desire further information with respect to this study, please contact Dr. Bernie Garrett at 604-822-7443 or by e-mail at [email protected].

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
107
Contact for concerns about the rights of research subjects: If you have any concerns about your treatment or rights as a research subject, you may contact the Research Subject Information Line in the UBC Office of Research Services at 604-822-8598. Consent: Participation or non-participation in the survey will not affect any relationships you or your institution may have with the investigators, CASN/ACESI or the University of British Columbia. By completing and submitting the questionnaire you will be certifying that you have read and understood the information presented here and have consented to take part in the study. Unfortunately, we cannot offer any remuneration for your participation in this study but would very much appreciate your input. Thank you very much for your time in considering this invitation and participating, if you choose to do so. Yours faithfully, Dr Bernie Garrett Assistant Professor University of British Columbia School of Nursing
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
108
INSTRUCTION SHEET: DELPHI PEDAGOGIC MAPPING STUDY What is a Delphi study? The objective of most Delphi applications is the reliable and creative exploration of ideas or the production of suitable information for decision making. The Delphi Method is based on a structured process for collecting and distilling knowledge from a group of experts by means of a series of questionnaires interspersed with controlled opinion feedback (Adler and Ziglio, 1996). Norman Dalkey (1969) and Olaf Helmer (1975), the techniques original developers, suggest Delphi represents a useful communication device among a group of experts and thus facilitates the formation of a group judgment. Wissema (1982) underlines the importance of the Delphi Method as a mono-variable exploration technique for technology forecasting. He further states that the Delphi method has been developed in order to make discussion between experts possible without permitting a certain social interactive behavior as happens during a normal group discussion and hampers opinion forming. The Delphi method has been widely used to generate forecasts in technology, education, and other fields (Cornish, 1977)." A more detailed explanation of the technique can be found at http://www.iit.edu/~it/delphi.html How do I Participate? There will be three rounds to this Delphi study. Firstly in this round consider the pedagogic mapping form attached and read the descriptions for each of the criteria. Then considering the use of clinical patient simulation in the attached METI® HPS® example place an X on the lines for each of the eight criteria reflecting how you think this dimension applies. For example for Dimension 3 (Role of the Instructor); if you feel that the role of the instructor in clinical patient simulation in the attached example scenario is completely didactive you would mark this at the far left of the line. Once you have completed the mapping please return it to me by either e-mail or post (to the address on the header of this letter). Once I have received the responses I will collate the responses and then send out the second round of short questionnaires. Following that one, there will be one final round of questionnaires to answer.
The University of British Columbia School of Nursing T201-2211, Wesbrook Mall Vancouver, B.C. V6T 2B5 Phone: (604) 822-7417 Fax: (604) 822-7466
INSTRUCTION SHEET & DELPHI QUESTIONNAIRE
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
109
The Pedagogic Dimension Mapping Tool
This tool simply represents a graphical way of representing the pedagogic dimensions of a learning application. A set of eight dimensions (after Reeves & Reeves 1997) is described below to represent the pedagogic dimensions of a learning application (in this case clinical patient simulation). Each dimension represents a bipolar continuum of values for a single pedagogic factor scaled from 1 to 6. They allow the delineation of the pedagogic dimensions involved for the educational resource being examined (in this case a High Fidelity Simulation) and help identify the grounding of the instructional design of the application in terms of learning theory. The dimensions are outlined below:
• Dimension 1: goal orientation
This dimension represents the degree to which the application is highly specific in terms of its outcome focus, or is highly generalizable. For example, is the application concerned with the development of a narrow range of outcomes for a specific purpose, or is it more involved in the development of skills or knowledge that are transferable to a wide range of situations?
• Dimension 2: pedagogical environment
This dimension represents the pedagogical environment in terms of two opposite approaches, instructivist and constructivist. The instructivist approach uses more classical instructional approaches (such as lectures, demonstrations and laboratories) that are more passive in nature. The constructivist approach on the other hand uses heuristic, hands on or collaborative learning and problem solving strategies.
• Dimension 3: role of the instructor
The focus of this dimension is to measure the degree of didactic or facilitative content in the simulation activity. This dimension ranges from a completely didactic approach at one extreme to a completely facilitative approach at the other.
• Dimension 4: role of the technology
The role of the technology is examined in this dimension. Technology can be used as a source of surrogate instruction or as a tool for extending cognitive processes. Therefore these two extremes are represented on a continuum.
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
110
Didactic applications tend to have a more instructional role (such as training for psycho-motor skills), whereas other computer-based learning applications support the development of cognitive skills.
• Dimension 5: nature of learning activities
This dimension ranges from the replication of the taught activities to the generation of new skills. It reflects the pedagogic approach in that the activities contained in the CBL application are either outcome focused or process focused. E.g. A simulation module designed to reinforce a sequence of events to achieve a specific end result (competency in a skill) is product focused, whilst a module designed to develop transferable critical thinking skills is process focused.
• Dimension 6: Source of motivation
Here the dimension ranges between external and internal. External motivation can be viewed as an application which has summative evaluated scores attached to its completion. E.g. resulting in certification, pass/fail or related to a specific job requirement. An example of more intrinsic motivation would be an educational product that is seen as useful by students in itself and which captivates their interest to work through it.
• Dimension 7: Experiential validity
This dimension measures the practical application of the content and processes to real life settings. Reeves (1997) applies a continuum between abstract and concrete, suggesting highly theoretical content remains abstract in terms of experiential validity, whilst practical skills-based content is more concrete.
• Dimension 8: Collaborative learning
This final dimension focuses on the amount of collaborative learning occurring. It ranges from proscribed to integral. Proscribed learning is viewed as highly controlled learning with little or no collaboration between students, whilst integral learning requires students’ collaboration as an integral part of the system.
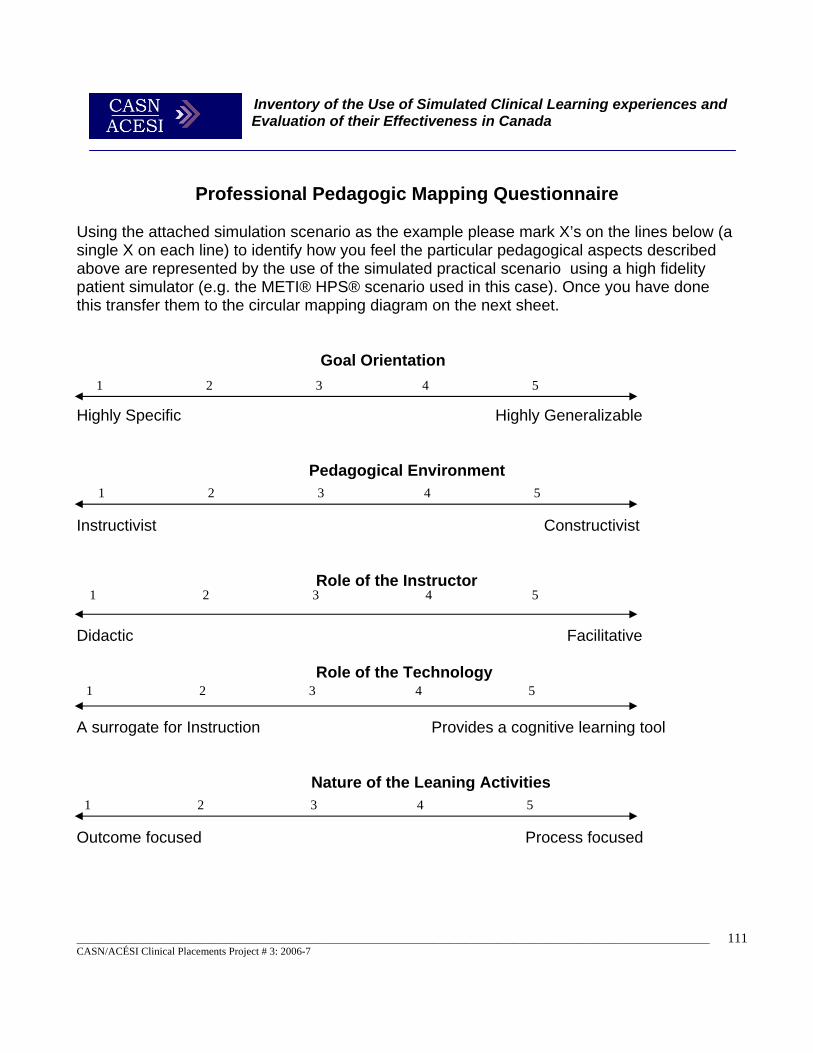
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
111
Professional Pedagogic Mapping Questionnaire
Using the attached simulation scenario as the example please mark X’s on the lines below (a single X on each line) to identify how you feel the particular pedagogical aspects described above are represented by the use of the simulated practical scenario using a high fidelity patient simulator (e.g. the METI® HPS® scenario used in this case). Once you have done this transfer them to the circular mapping diagram on the next sheet. Goal Orientation
Highly Specific Highly Generalizable
Pedagogical Environment
Instructivist Constructivist Role of the Instructor
Didactic Facilitative Role of the Technology
A surrogate for Instruction Provides a cognitive learning tool
Nature of the Leaning Activities
Outcome focused Process focused
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
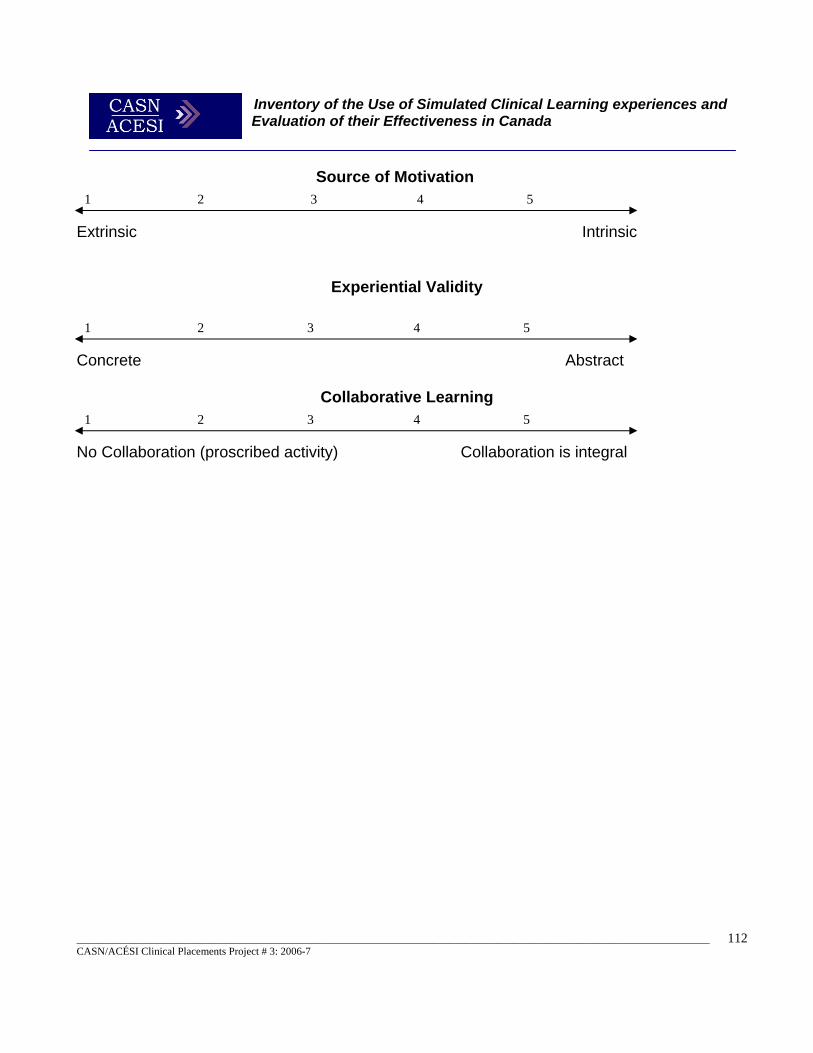
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
112
Source of Motivation
Extrinsic Intrinsic
Experiential Validity
Concrete Abstract
Collaborative Learning
No Collaboration (proscribed activity) Collaboration is integral
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
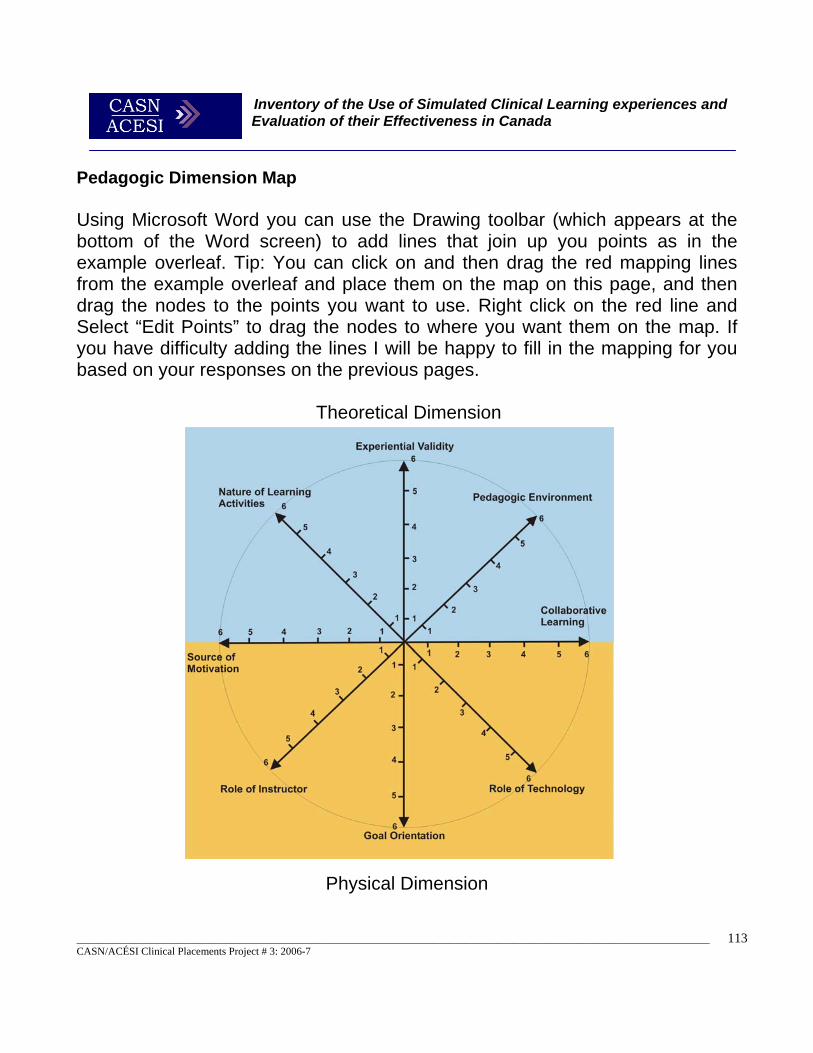
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
113
Pedagogic Dimension Map Using Microsoft Word you can use the Drawing toolbar (which appears at the bottom of the Word screen) to add lines that join up you points as in the example overleaf. Tip: You can click on and then drag the red mapping lines from the example overleaf and place them on the map on this page, and then drag the nodes to the points you want to use. Right click on the red line and Select “Edit Points” to drag the nodes to where you want them on the map. If you have difficulty adding the lines I will be happy to fill in the mapping for you based on your responses on the previous pages. Theoretical Dimension
Physical Dimension
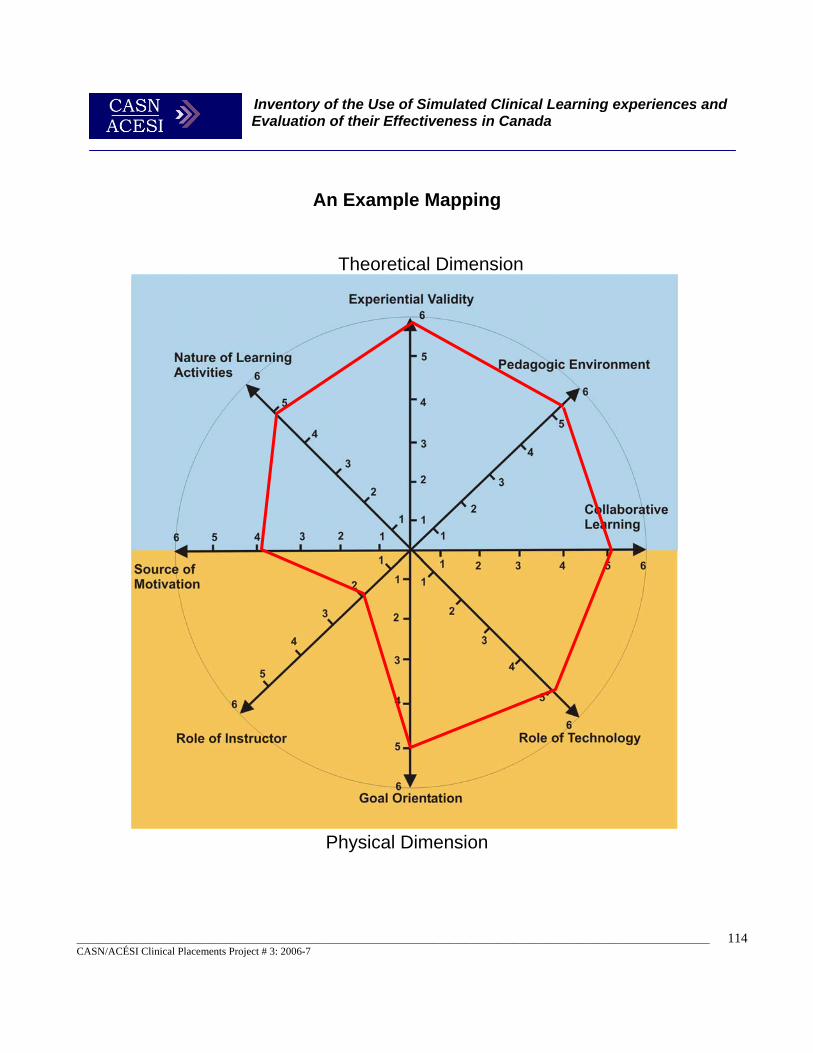
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
114
An Example Mapping
Theoretical Dimension
Physical Dimension
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
115
Inventory of the Use of Simulated Clinical Learning Experiences and Evaluation of their Effectiveness. Principal Investigator: Dr Bernie Garrett, Assistant Professor. Friday, August 17, 2007 Dear Colleague, Recently you participated in a survey to investigate the use of simulated learning experiences for clinical health professional education in Canada. At that time you indicated you would be prepared to participate in a further telephone interview to explore the value of simulation. I am now writing to you to ask if you would still be prepared to participate in this telephone focus group interview. The Project The aim of this project is to explore the use of simulated clinical learning experiences in healthcare professional education and training in Canada and evaluate the effectiveness of this approach. We wish to establish the range, evidence base and best practices in the use of simulated learning for healthcare professional education and training. The overall aim is to develop an inventory of simulation use for healthcare professional preparation in Canada, and explore the evidence base for its use, cost-effectiveness and possibilities for multi-professional collaboration. In this way the possibilities for simulation to provide alternatives to traditional clinical experience for nurse education, and its limitations may be established. This project seeks to: 1. Establish current practices of using simulated learning experiences for nursing and other health professional students in Canada, and explore the potential for collaboration 2. Identify the types of simulated learning resources and experiences used, for professional healthcare education and identify which professional groups are using them, and at which
The University of British Columbia School of Nursing T201-2211, Wesbrook Mall Vancouver, B.C. V6T 2B5 Phone: (604) 822-7417 Fax: (604) 822-7466
INVITATION TO PARTICIPATE IN A STUDY
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
116
levels 3. Establish evidence of the effectiveness of using simulated learning experiences 4. Explore what evidence is available from economic evaluations of simulated learning experiences to support their use or otherwise 5. Identify areas from the literature of specific content areas that are more appropriate for the use of simulated experiences 6. Explore the feasibility, utility and effectiveness of using simulated learning experiences as an augmentation to more traditional clinical placements 7. Investigate the potential for using a collaborative framework for implementing clinical simulations using e-learning technologies for professional healthcare education and training in Canada. Why am I being asked? I am inviting you to be involved as a health care professional educator who may be using simulated learning to support clinical education and training. What is involved? Participation is quite straightforward and completely voluntary. All that is required is that you participate in a short telephone focus group interview with five of your colleagues form other institutions. The interview should take no longer than 30 minutes at maximum to complete, and will be scheduled at you and your colleagues convenience. If you are prepared to be involved, would you please complete the attached consent form and return it to me in the prepaid envelope by Friday September the 8th 2006. I will then contact you and schedule an interview at your convenience. Confidentiality The interview will be taped and transcribed but the personal identity of all participants in will be kept strictly confidential after its conclusion. All individuals and documents will be identified only by code number and kept in a locked filing cabinet in a locked office in the School of Nursing at UBC. Any data kept on electronic media at the School of Nursing will not include the name or personal details of the individual subject and will be encrypted. Subjects will not be identified by name in any reports of the completed study. Contact for information about the study If you have any questions or desire further information with respect to this study, please contact Dr. Bernie Garrett at 604-822-7443 or by e-mail at [email protected].

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
117
Contact for concerns about the rights of research subjects: If you have any concerns about your treatment or rights as a research subject, you may contact the Research Subject Information Line in the UBC Office of Research Services at 604-822-8598. Unfortunately, we cannot offer any remuneration for your participation in this study but would very much appreciate your input. Thank you very much for your time in considering this invitation and participating, if you choose to do so. Yours faithfully, Dr Bernie Garrett Assistant Professor University of British Columbia School of Nursing
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
118
SIMULATION TELEPHONE FOCUS GROUP INTERVIEW SCRIPT Introduction 1. Introduce the telephone focus group session and thank the participants for taking part in the study 2. Outline the objectives of the study and informed them that the interview will be audio-taped. Questions (used to generate discussion)
1) What types of simulated learning resources and experiences are you currently using? 2) Which professional groups are you using them with, and at which levels? 3) How useful do you feel the use of patient simulation is professional health care education? 4) How effective do you think clinical patient education is for the development of clinical skills? 5) What are the cost-benefits and how cost-effective do you think these techniques are compared
to traditional approaches? 6) How cost-efficient do you think these techniques are compared to traditional approaches? 7) What advantages do the offer compared to traditional approaches? 8) What do you think are the disadvantages? 9) What sorts of things (if any) have caused you problems in implementing clinical simulation? 10) What specific content areas do you feel are most suited for the use of simulated experiences 11) Do you think it would be feasible to use simulated learning experiences as an augmentation to
more traditional clinical placement 12) What about as an alternative to an actual clinical placement? 13) Do you think it would be feasible to use simulated learning experiences for inter-professional
education and training? 14) Lastly, what do you think is the potential for using a collaborative framework to share clinical
simulations for professional healthcare education and training across Canada? 15) Any other comments?
Conclusion Thank them for participating in the interview.
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
119
Appendix C – Project Advisory Committee Terms of Reference and Membership With funding from Health Canada, CASN is pleased to sponsor three projects dealing with clinical placements for nursing and other health professional students. Project 1 – Inventory of strategies to deliver nursing and inter-professional clinical placements in Canada; Project 2 – Cost of nursing clinical placements Project 3 – Inventory of the use of simulated clinical learning experiences and the evaluation of their effectiveness. The Advisory Committee will:
• Oversee the entire project from its inception to its evaluation phase. • Review submissions received and select the successful candidates. • Provide independent expert advice on the conduct of the three research projects, the framing of recommendations,
and the dissemination of results. • Consist of representation from major nursing, health professional and other stakeholder groups.
Membership will involve a two-year commitment, ending in April, 2007 when the projects are completed. In addition, there will most likely be two face-to-face meetings and a number of teleconferences over the two-year time period. Travel expenses will be covered for the meetings.
Name Location Email Susan Dawe NBCC [email protected]
George Eisler BC Academic Health Council [email protected]
Jennifer Ellis Canadian Health Services Research Foundation [email protected]
Pat Semeniuk Vancouver Coastal Health [email protected]
Victoria Greenslade Office of Nursing Policy, Health Canada [email protected]
Nora Hammell Canadian Nurses Association [email protected]
Diane Morin Université Laval [email protected]
Michel Tarko Douglas College [email protected]
Ellen Rukholm Laurentian University [email protected] Lynnette Leeseberg Stamler University of Saskatchewan [email protected]
Lise Talbot Université de Sherbrooke [email protected]
Jane Milliken Chair, CASN Task Force on Clinical Education
Pat Smith Northern Ontario School of Medicine – Researcher [email protected]
Michel Morton Lakehead University – Researcher [email protected]
Bernard Garrett UBC – Researcher [email protected]
Pat Griffin CASN [email protected]
Jo-Anne Swanson CASN [email protected]
Dina Idriss CASN [email protected]
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
120
Appendix D – Ethical Approval Consent Form
A Survey of Healthcare Education and Training Professionals To Assess The Use And Effectiveness Of Clinical Simulation. Principal Investigator: Dr Bernie Garrett, Assistant Professor. The University of British Columbia, School of Nursing
T201-2211, Wesbrook Mall, Vancouver, B.C. V6T 2B5 Phone: (604) 822-7417 Fax: (604) 822-7466 E-Mail: [email protected]
Purpose: The aim of this project is to explore the use of simulated clinical learning experiences in healthcare professional education and training in Canada and evaluate the effectiveness of this approach. We wish to establish the range, evidence base and best practices in the use of simulated learning for healthcare professional education and training. The overall aim is to develop an inventory of simulation use for healthcare professional preparation in Canada, and explore the evidence base for its use, cost-effectiveness and possibilities for multi-professional collaboration. In this way the possibilities for simulation to provide alternatives to traditional clinical experience for nurse education, and its limitations may be established. This project has been commissioned by the CASN/ACESI. Study Procedures: Participation in this study will require that you participate in a single short telephone focus group interview with several (up to 5) of your colleagues from other professional health care education institutions. The interview should take no longer than 30 minutes at maximum to complete, and will be scheduled at you and your colleagues’ convenience. The interview will be audio-taped for later transcription, but personal biographical or institutional information will not be recorded. Confidentiality: We encourage all participants to refrain from disclosing the contents of the discussion outside of the focus group; however, we cannot control what other participants do with the information discussed.” However, your personal identity will be kept strictly confidential in all analysis and reports resulting from this interview. No personal biographical information is required during the interview. All documents will be identified only by code number and kept in a locked filing cabinet in a locked office in the School of Nursing. Any data kept on electronic media (computers) at the School of Nursing will not include the name or personal details of the individual subjects and will be encrypted. Subjects will not be identified by name or location in any reports of the completed study. Remuneration/Compensation:
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
121
Unfortunately, we cannot offer any remuneration for your participation in this study but thank you very much for your time and effort in participating. Contact for information about the study: If you have any questions or desire further information with respect to this study, you may contact Dr. Bernie Garrett at 604-822-7443 or by e-mail at [email protected]. Contact for concerns about the rights of research subjects: If you have any concerns about your treatment or rights as a research subject, you may contact the Research Subject Information Line in the UBC Office of Research Services at 604-822-8598. Consent: Participation in this study is entirely voluntary and you may refuse to participate or withdraw from the study at any time without jeopardy to any relationships with the Schools of Nursing at UBC. Your signature below indicates that you have received a copy of this consent form for your own records. Your signature indicates that you consent to participate in this study. ____________________________________________________ Researcher Signature Date ____________________________________________________ Subject Signature Date ____________________________________________________ Printed Name of the Subject ____________________________________________________ Contact Number/E-mail for communication

Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
122
Appendix E – Detailed Statistical Findings Section A Table A.1.1 Other Groups to Which Simulations are Being Promoted Other Groups Being Promoted To
N
Yes - There are currently efforts to promote simulation use to new groups 25Our occupational health and safety 1Local agencies 4Future 5Partnership with FHA 1Medical 2Students 5Anesthesia 2Hospitals 2Early national integration programs 1Paramedic 1Critical care training 1Nurses 2Mentoring 1Pediatric Resuscitation 2Continuing education 2ACLS courses 1Educational institutions 1Faculty 3Interdepartmental communications 1Haptic VR simulations 1Inter-professional Simulations Laboratory 1CCU with monitors 2Sharing 1Note: N = 43.
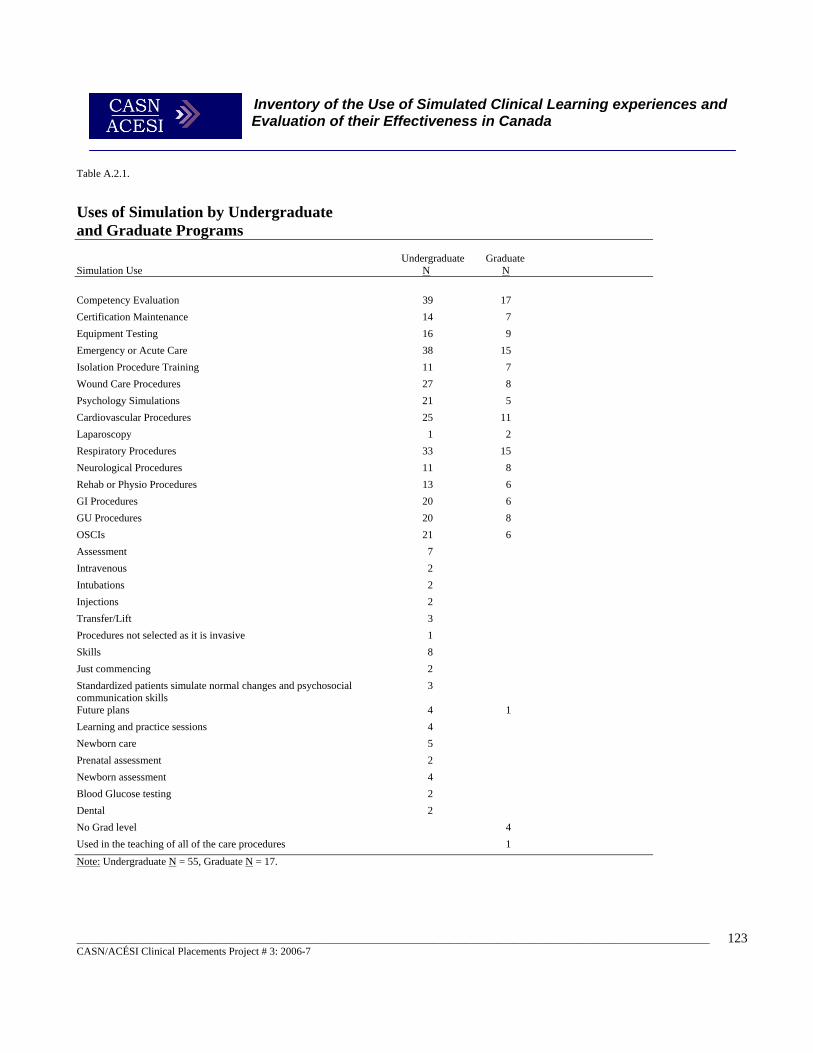
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
123
Table A.2.1.
Uses of Simulation by Undergraduate and Graduate Programs
Undergraduate Graduate Simulation Use N N
Competency Evaluation 39 17 Certification Maintenance 14 7 Equipment Testing 16 9 Emergency or Acute Care 38 15 Isolation Procedure Training 11 7 Wound Care Procedures 27 8 Psychology Simulations 21 5 Cardiovascular Procedures 25 11 Laparoscopy 1 2 Respiratory Procedures 33 15 Neurological Procedures 11 8 Rehab or Physio Procedures 13 6 GI Procedures 20 6 GU Procedures 20 8 OSCIs 21 6 Assessment 7 Intravenous 2 Intubations 2 Injections 2 Transfer/Lift 3 Procedures not selected as it is invasive 1 Skills 8 Just commencing 2 Standardized patients simulate normal changes and psychosocial communication skills
3
Future plans 4 1 Learning and practice sessions 4 Newborn care 5 Prenatal assessment 2 Newborn assessment 4 Blood Glucose testing 2 Dental 2 No Grad level 4 Used in the teaching of all of the care procedures 1 Note: Undergraduate N = 55, Graduate N = 17.
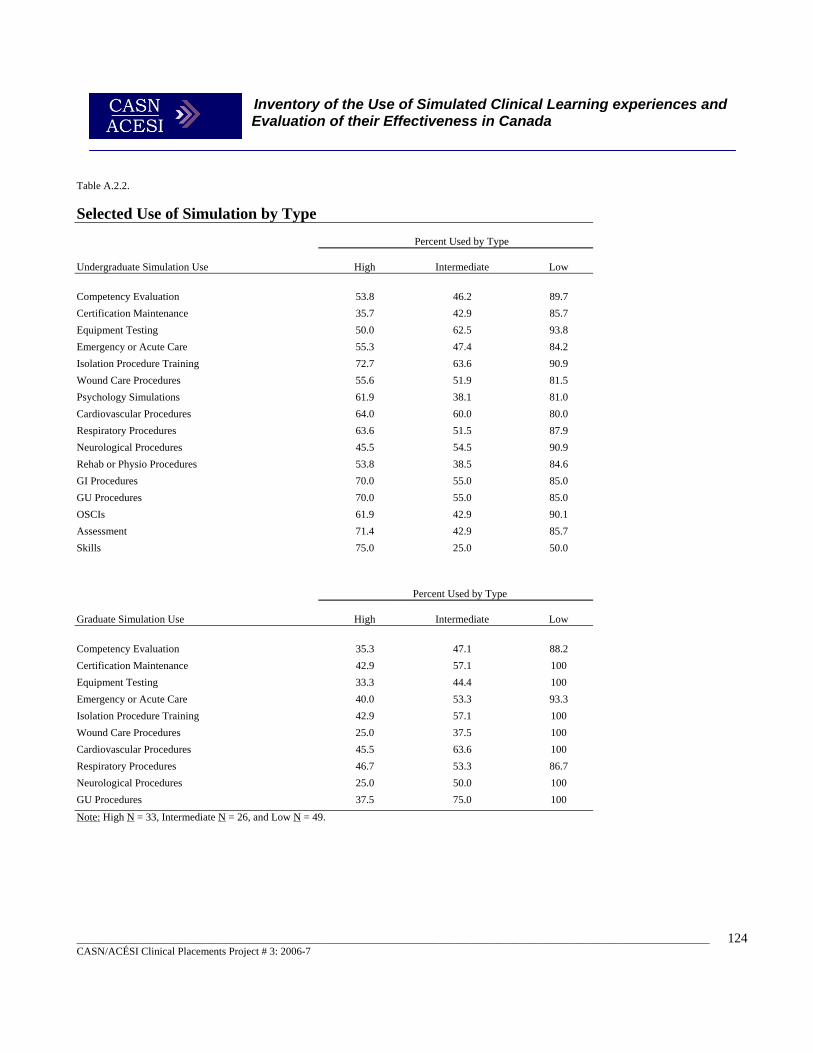
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
124
Table A.2.2. Selected Use of Simulation by Type
Percent Used by Type
Undergraduate Simulation Use
High
Intermediate
Low
Competency Evaluation 53.8 46.2 89.7 Certification Maintenance 35.7 42.9 85.7 Equipment Testing 50.0 62.5 93.8 Emergency or Acute Care 55.3 47.4 84.2 Isolation Procedure Training 72.7 63.6 90.9 Wound Care Procedures 55.6 51.9 81.5 Psychology Simulations 61.9 38.1 81.0 Cardiovascular Procedures 64.0 60.0 80.0 Respiratory Procedures 63.6 51.5 87.9 Neurological Procedures 45.5 54.5 90.9 Rehab or Physio Procedures 53.8 38.5 84.6 GI Procedures 70.0 55.0 85.0 GU Procedures 70.0 55.0 85.0 OSCIs 61.9 42.9 90.1 Assessment 71.4 42.9 85.7 Skills 75.0 25.0 50.0
Percent Used by Type
Graduate Simulation Use
High
Intermediate
Low
Competency Evaluation 35.3 47.1 88.2 Certification Maintenance 42.9 57.1 100 Equipment Testing 33.3 44.4 100 Emergency or Acute Care 40.0 53.3 93.3 Isolation Procedure Training 42.9 57.1 100 Wound Care Procedures 25.0 37.5 100 Cardiovascular Procedures 45.5 63.6 100 Respiratory Procedures 46.7 53.3 86.7 Neurological Procedures 25.0 50.0 100 GU Procedures 37.5 75.0 100 Note: High N = 33, Intermediate N = 26, and Low N = 49.
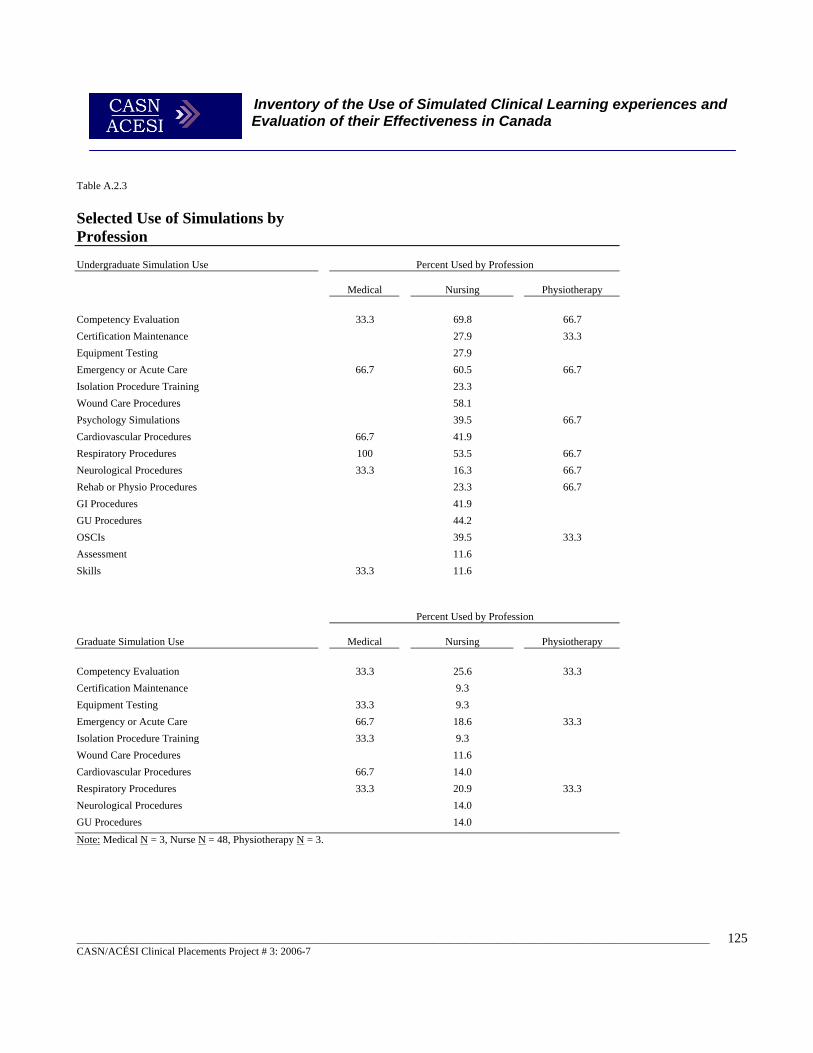
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
125
Table A.2.3
Selected Use of Simulations by Profession
Undergraduate Simulation Use
Percent Used by Profession
Medical
Nursing
Physiotherapy
Competency Evaluation 33.3 69.8 66.7 Certification Maintenance 27.9 33.3 Equipment Testing 27.9 Emergency or Acute Care 66.7 60.5 66.7 Isolation Procedure Training 23.3 Wound Care Procedures 58.1 Psychology Simulations 39.5 66.7 Cardiovascular Procedures 66.7 41.9 Respiratory Procedures 100 53.5 66.7 Neurological Procedures 33.3 16.3 66.7 Rehab or Physio Procedures 23.3 66.7 GI Procedures 41.9 GU Procedures 44.2 OSCIs 39.5 33.3 Assessment 11.6 Skills 33.3 11.6
Percent Used by Profession Graduate Simulation Use
Medical
Nursing
Physiotherapy
Competency Evaluation 33.3 25.6 33.3 Certification Maintenance 9.3 Equipment Testing 33.3 9.3 Emergency or Acute Care 66.7 18.6 33.3 Isolation Procedure Training 33.3 9.3 Wound Care Procedures 11.6 Cardiovascular Procedures 66.7 14.0 Respiratory Procedures 33.3 20.9 33.3 Neurological Procedures 14.0 GU Procedures 14.0 Note: Medical N = 3, Nurse N = 48, Physiotherapy N = 3.
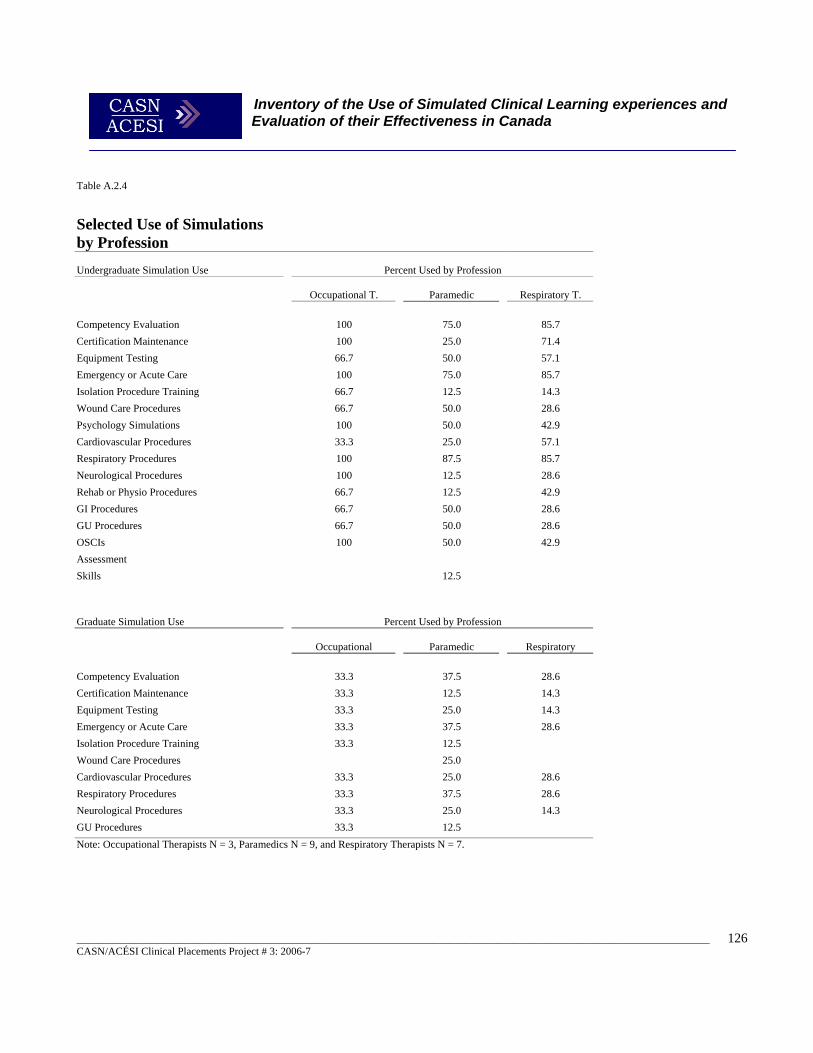
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
126
Table A.2.4
Selected Use of Simulations by Profession
Undergraduate Simulation Use
Percent Used by Profession
Occupational T.
Paramedic
Respiratory T.
Competency Evaluation 100 75.0 85.7 Certification Maintenance 100 25.0 71.4 Equipment Testing 66.7 50.0 57.1 Emergency or Acute Care 100 75.0 85.7 Isolation Procedure Training 66.7 12.5 14.3 Wound Care Procedures 66.7 50.0 28.6 Psychology Simulations 100 50.0 42.9 Cardiovascular Procedures 33.3 25.0 57.1 Respiratory Procedures 100 87.5 85.7 Neurological Procedures 100 12.5 28.6 Rehab or Physio Procedures 66.7 12.5 42.9 GI Procedures 66.7 50.0 28.6 GU Procedures 66.7 50.0 28.6 OSCIs 100 50.0 42.9 Assessment Skills 12.5
Graduate Simulation Use
Percent Used by Profession
Occupational
Paramedic
Respiratory
Competency Evaluation 33.3 37.5 28.6 Certification Maintenance 33.3 12.5 14.3 Equipment Testing 33.3 25.0 14.3 Emergency or Acute Care 33.3 37.5 28.6 Isolation Procedure Training 33.3 12.5 Wound Care Procedures 25.0 Cardiovascular Procedures 33.3 25.0 28.6 Respiratory Procedures 33.3 37.5 28.6 Neurological Procedures 33.3 25.0 14.3 GU Procedures 33.3 12.5 Note: Occupational Therapists N = 3, Paramedics N = 9, and Respiratory Therapists N = 7.
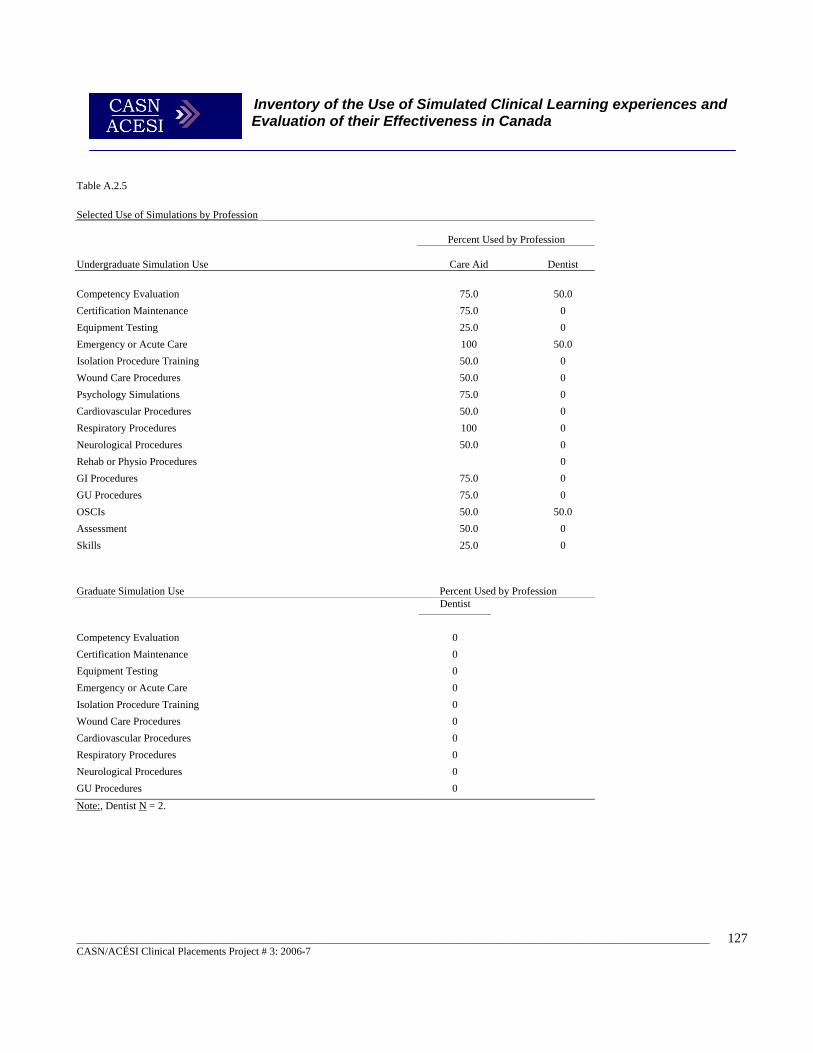
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
127
Table A.2.5 Selected Use of Simulations by Profession
Percent Used by Profession
Undergraduate Simulation Use
Care Aid
Dentist
Competency Evaluation 75.0 50.0 Certification Maintenance 75.0 0 Equipment Testing 25.0 0 Emergency or Acute Care 100 50.0 Isolation Procedure Training 50.0 0 Wound Care Procedures 50.0 0 Psychology Simulations 75.0 0 Cardiovascular Procedures 50.0 0 Respiratory Procedures 100 0 Neurological Procedures 50.0 0 Rehab or Physio Procedures 0 GI Procedures 75.0 0 GU Procedures 75.0 0 OSCIs 50.0 50.0 Assessment 50.0 0 Skills 25.0 0
Graduate Simulation Use
Percent Used by Profession Dentist
Competency Evaluation 0 Certification Maintenance 0 Equipment Testing 0 Emergency or Acute Care 0 Isolation Procedure Training 0 Wound Care Procedures 0 Cardiovascular Procedures 0 Respiratory Procedures 0 Neurological Procedures 0 GU Procedures 0 Note:, Dentist N = 2.
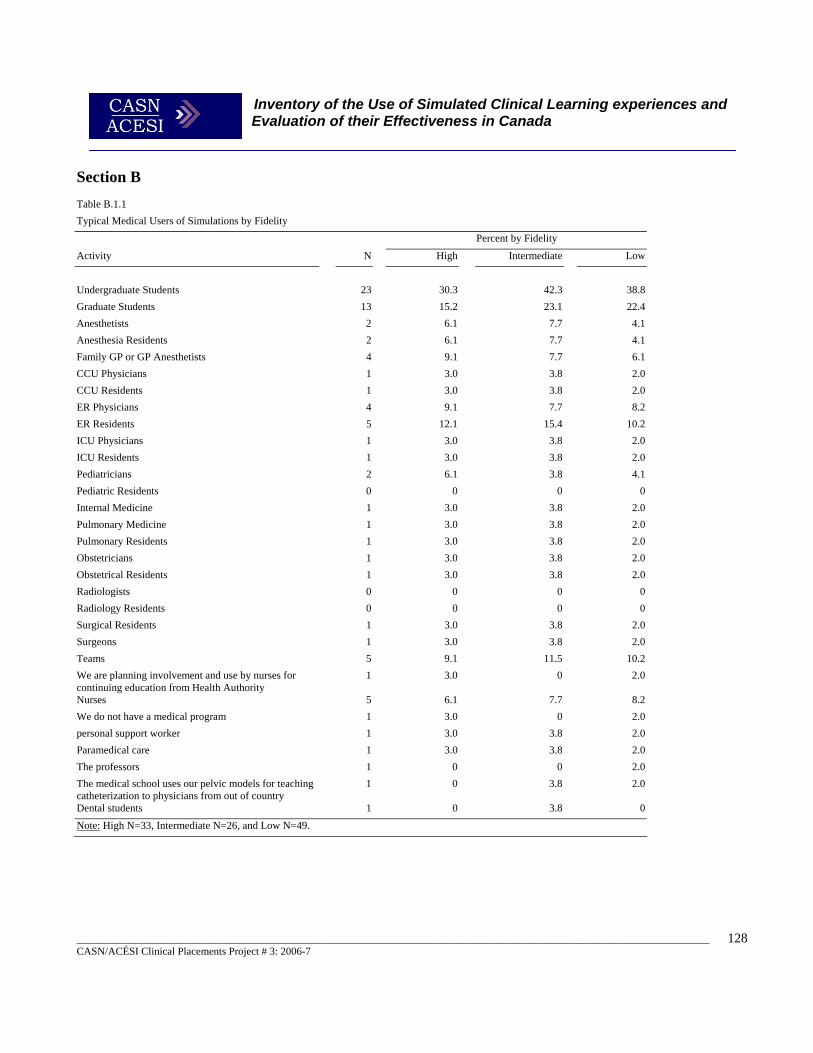
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
128
Section B Table B.1.1 Typical Medical Users of Simulations by Fidelity
Percent by Fidelity
Activity N High Intermediate Low
Undergraduate Students 23 30.3 42.3 38.8 Graduate Students 13 15.2 23.1 22.4 Anesthetists 2 6.1 7.7 4.1 Anesthesia Residents 2 6.1 7.7 4.1 Family GP or GP Anesthetists 4 9.1 7.7 6.1 CCU Physicians 1 3.0 3.8 2.0 CCU Residents 1 3.0 3.8 2.0 ER Physicians 4 9.1 7.7 8.2 ER Residents 5 12.1 15.4 10.2 ICU Physicians 1 3.0 3.8 2.0 ICU Residents 1 3.0 3.8 2.0 Pediatricians 2 6.1 3.8 4.1 Pediatric Residents 0 0 0 0 Internal Medicine 1 3.0 3.8 2.0 Pulmonary Medicine 1 3.0 3.8 2.0 Pulmonary Residents 1 3.0 3.8 2.0 Obstetricians 1 3.0 3.8 2.0 Obstetrical Residents 1 3.0 3.8 2.0 Radiologists 0 0 0 0 Radiology Residents 0 0 0 0 Surgical Residents 1 3.0 3.8 2.0 Surgeons 1 3.0 3.8 2.0 Teams 5 9.1 11.5 10.2 We are planning involvement and use by nurses for continuing education from Health Authority
1 3.0 0 2.0
Nurses 5 6.1 7.7 8.2 We do not have a medical program 1 3.0 0 2.0 personal support worker 1 3.0 3.8 2.0 Paramedical care 1 3.0 3.8 2.0 The professors 1 0 0 2.0 The medical school uses our pelvic models for teaching catheterization to physicians from out of country
1 0 3.8 2.0
Dental students 1 0 3.8 0 Note: High N=33, Intermediate N=26, and Low N=49.
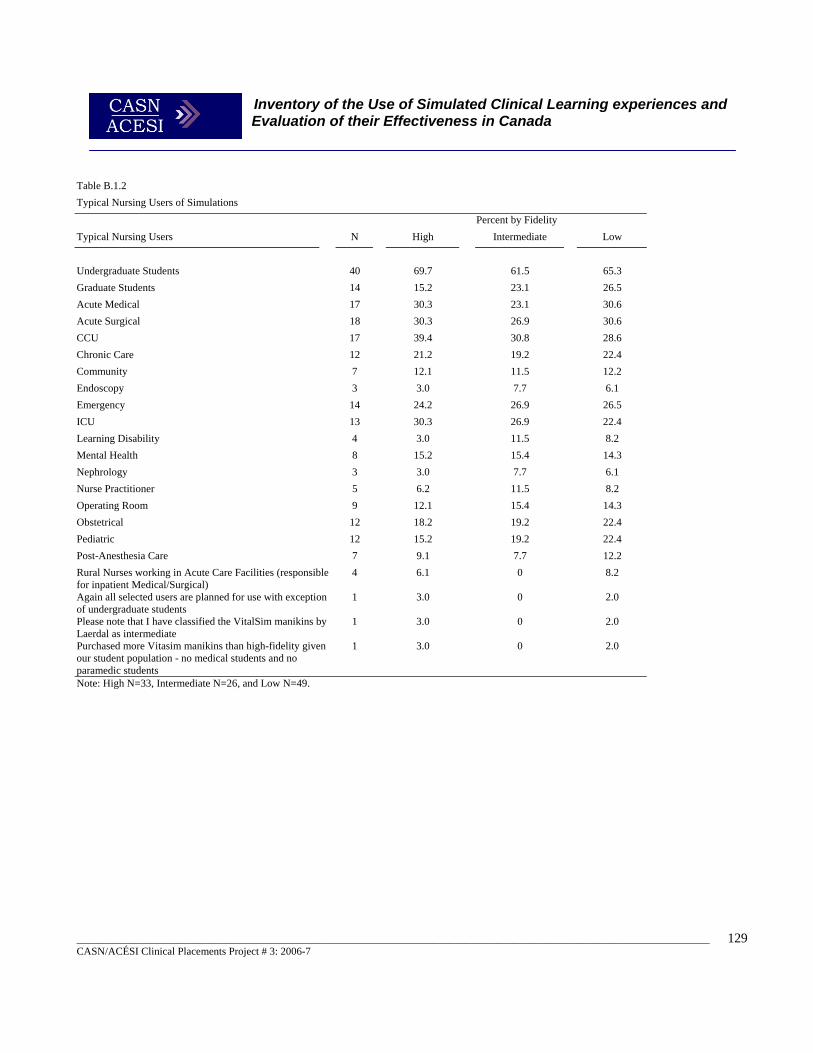
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
129
Table B.1.2 Typical Nursing Users of Simulations
Percent by Fidelity Typical Nursing Users N High Intermediate Low
Undergraduate Students 40 69.7 61.5 65.3 Graduate Students 14 15.2 23.1 26.5 Acute Medical 17 30.3 23.1 30.6 Acute Surgical 18 30.3 26.9 30.6 CCU 17 39.4 30.8 28.6 Chronic Care 12 21.2 19.2 22.4 Community 7 12.1 11.5 12.2 Endoscopy 3 3.0 7.7 6.1 Emergency 14 24.2 26.9 26.5 ICU 13 30.3 26.9 22.4 Learning Disability 4 3.0 11.5 8.2 Mental Health 8 15.2 15.4 14.3 Nephrology 3 3.0 7.7 6.1 Nurse Practitioner 5 6.2 11.5 8.2 Operating Room 9 12.1 15.4 14.3 Obstetrical 12 18.2 19.2 22.4 Pediatric 12 15.2 19.2 22.4 Post-Anesthesia Care 7 9.1 7.7 12.2 Rural Nurses working in Acute Care Facilities (responsible for inpatient Medical/Surgical)
4 6.1 0 8.2
Again all selected users are planned for use with exception of undergraduate students
1 3.0 0 2.0
Please note that I have classified the VitalSim manikins by Laerdal as intermediate
1 3.0 0 2.0
Purchased more Vitasim manikins than high-fidelity given our student population - no medical students and no paramedic students
1 3.0 0 2.0
Note: High N=33, Intermediate N=26, and Low N=49.
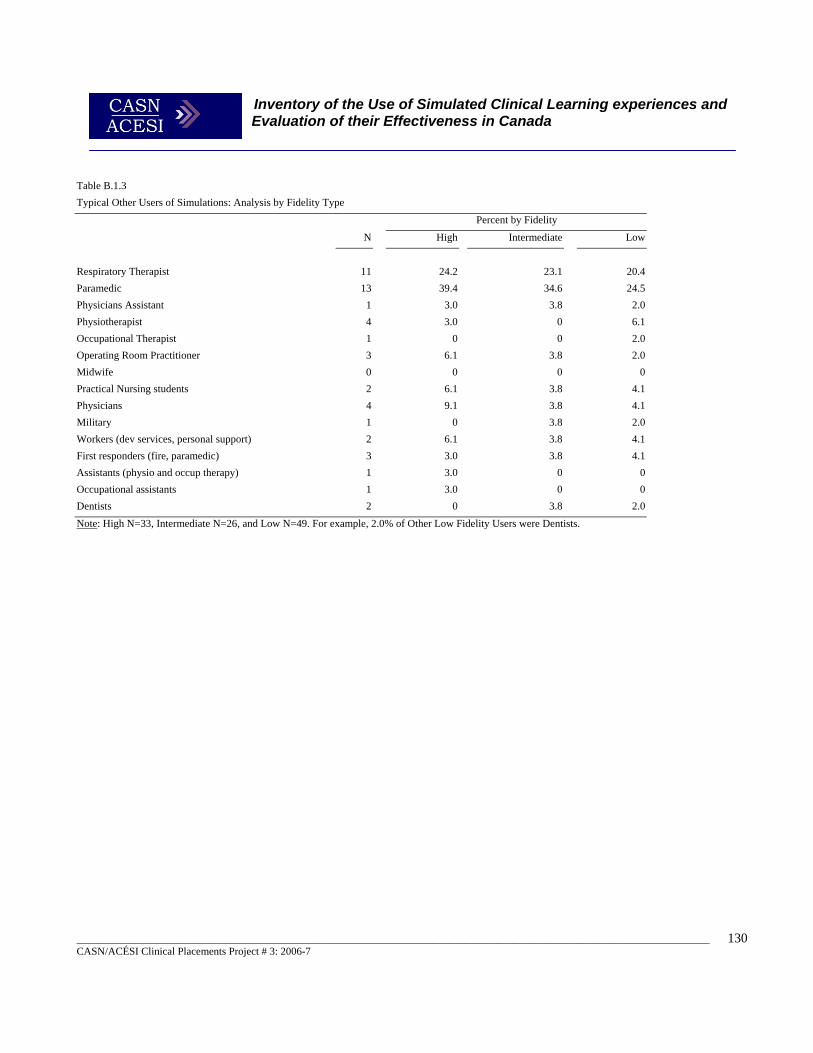
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
130
Table B.1.3 Typical Other Users of Simulations: Analysis by Fidelity Type
Percent by Fidelity
N High Intermediate Low
Respiratory Therapist 11 24.2 23.1 20.4 Paramedic 13 39.4 34.6 24.5 Physicians Assistant 1 3.0 3.8 2.0 Physiotherapist 4 3.0 0 6.1 Occupational Therapist 1 0 0 2.0 Operating Room Practitioner 3 6.1 3.8 2.0 Midwife 0 0 0 0 Practical Nursing students 2 6.1 3.8 4.1 Physicians 4 9.1 3.8 4.1 Military 1 0 3.8 2.0 Workers (dev services, personal support) 2 6.1 3.8 4.1 First responders (fire, paramedic) 3 3.0 3.8 4.1 Assistants (physio and occup therapy) 1 3.0 0 0 Occupational assistants 1 3.0 0 0 Dentists 2 0 3.8 2.0 Note: High N=33, Intermediate N=26, and Low N=49. For example, 2.0% of Other Low Fidelity Users were Dentists.
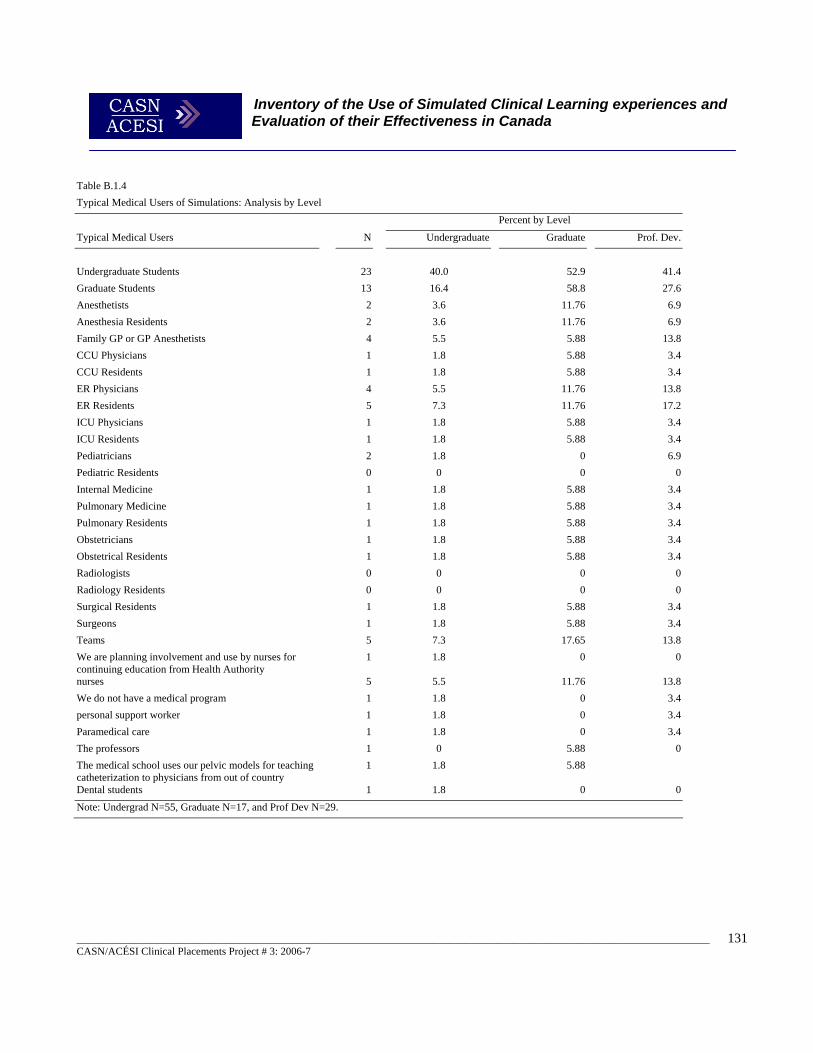
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
131
Table B.1.4 Typical Medical Users of Simulations: Analysis by Level
Percent by Level
Typical Medical Users N Undergraduate Graduate Prof. Dev.
Undergraduate Students 23 40.0 52.9 41.4Graduate Students 13 16.4 58.8 27.6Anesthetists 2 3.6 11.76 6.9Anesthesia Residents 2 3.6 11.76 6.9Family GP or GP Anesthetists 4 5.5 5.88 13.8CCU Physicians 1 1.8 5.88 3.4CCU Residents 1 1.8 5.88 3.4ER Physicians 4 5.5 11.76 13.8ER Residents 5 7.3 11.76 17.2ICU Physicians 1 1.8 5.88 3.4ICU Residents 1 1.8 5.88 3.4Pediatricians 2 1.8 0 6.9Pediatric Residents 0 0 0 0Internal Medicine 1 1.8 5.88 3.4Pulmonary Medicine 1 1.8 5.88 3.4Pulmonary Residents 1 1.8 5.88 3.4Obstetricians 1 1.8 5.88 3.4Obstetrical Residents 1 1.8 5.88 3.4Radiologists 0 0 0 0Radiology Residents 0 0 0 0Surgical Residents 1 1.8 5.88 3.4Surgeons 1 1.8 5.88 3.4Teams 5 7.3 17.65 13.8We are planning involvement and use by nurses for continuing education from Health Authority
1 1.8 0 0
nurses 5 5.5 11.76 13.8We do not have a medical program 1 1.8 0 3.4personal support worker 1 1.8 0 3.4Paramedical care 1 1.8 0 3.4The professors 1 0 5.88 0The medical school uses our pelvic models for teaching catheterization to physicians from out of country
1 1.8 5.88
Dental students 1 1.8 0 0Note: Undergrad N=55, Graduate N=17, and Prof Dev N=29.
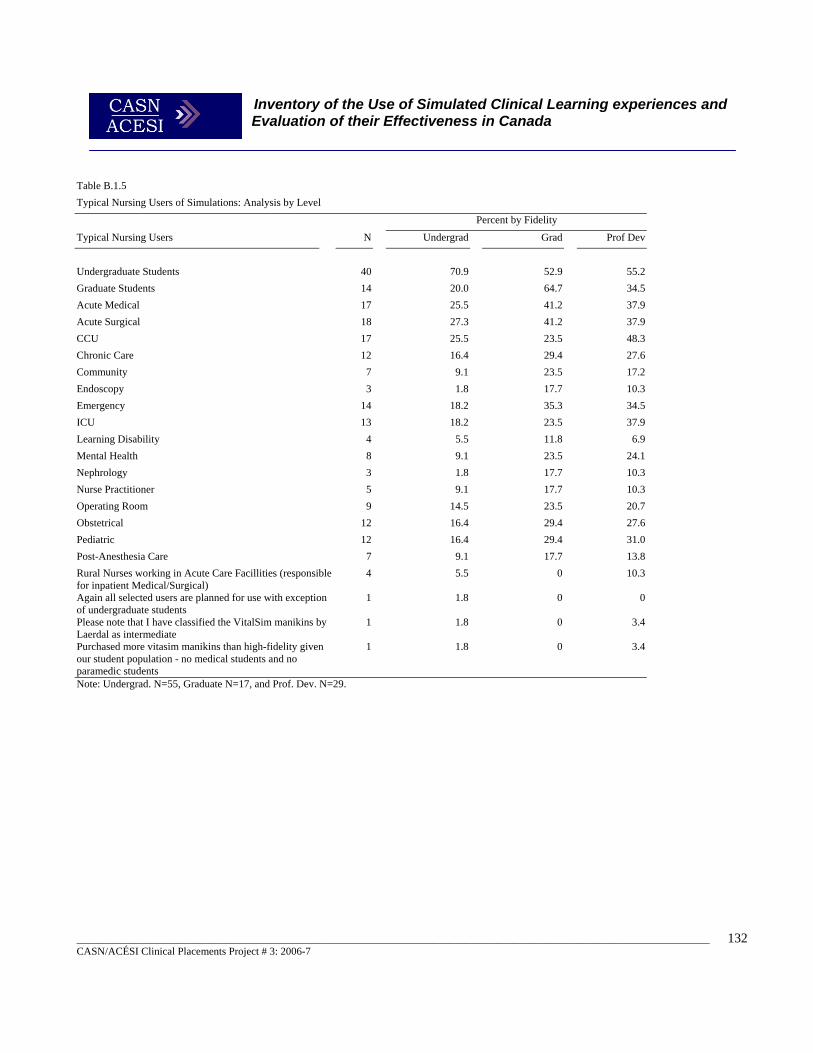
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
132
Table B.1.5 Typical Nursing Users of Simulations: Analysis by Level
Percent by Fidelity
Typical Nursing Users N Undergrad Grad Prof Dev
Undergraduate Students 40 70.9 52.9 55.2 Graduate Students 14 20.0 64.7 34.5 Acute Medical 17 25.5 41.2 37.9 Acute Surgical 18 27.3 41.2 37.9 CCU 17 25.5 23.5 48.3 Chronic Care 12 16.4 29.4 27.6 Community 7 9.1 23.5 17.2 Endoscopy 3 1.8 17.7 10.3 Emergency 14 18.2 35.3 34.5 ICU 13 18.2 23.5 37.9 Learning Disability 4 5.5 11.8 6.9 Mental Health 8 9.1 23.5 24.1 Nephrology 3 1.8 17.7 10.3 Nurse Practitioner 5 9.1 17.7 10.3 Operating Room 9 14.5 23.5 20.7 Obstetrical 12 16.4 29.4 27.6 Pediatric 12 16.4 29.4 31.0 Post-Anesthesia Care 7 9.1 17.7 13.8 Rural Nurses working in Acute Care Facillities (responsible for inpatient Medical/Surgical)
4 5.5 0 10.3
Again all selected users are planned for use with exception of undergraduate students
1 1.8 0 0
Please note that I have classified the VitalSim manikins by Laerdal as intermediate
1 1.8 0 3.4
Purchased more vitasim manikins than high-fidelity given our student population - no medical students and no paramedic students
1 1.8 0 3.4
Note: Undergrad. N=55, Graduate N=17, and Prof. Dev. N=29.
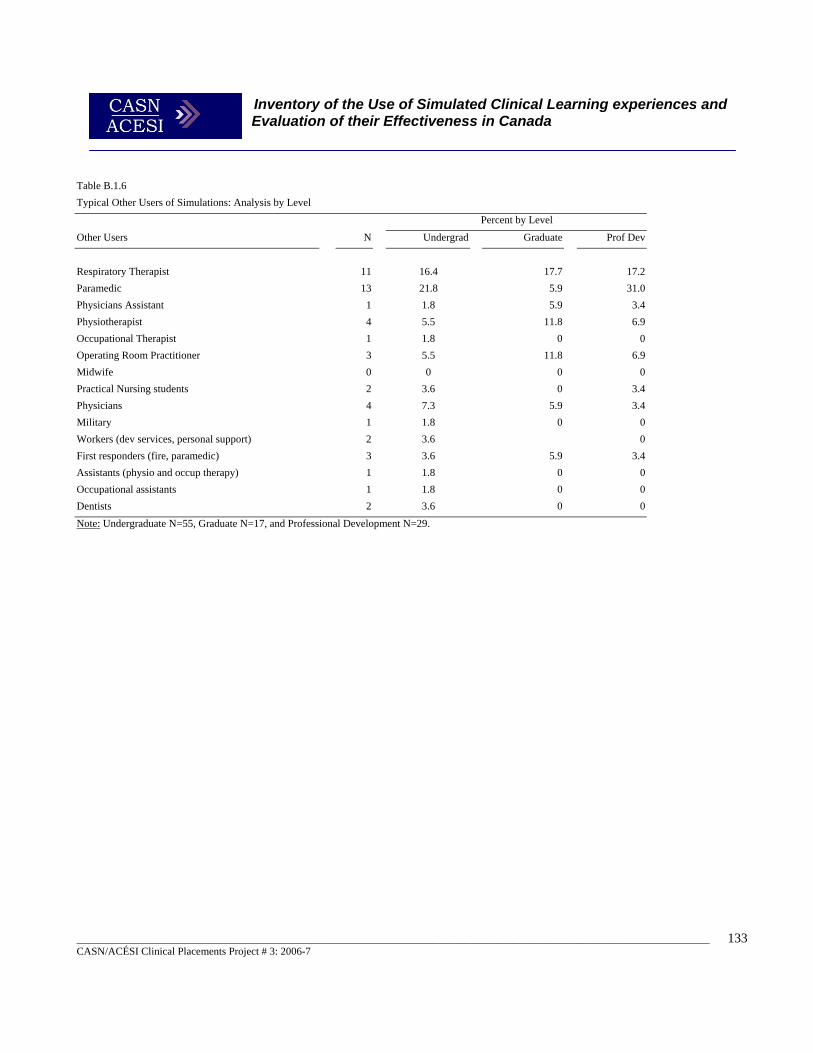
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
133
Table B.1.6 Typical Other Users of Simulations: Analysis by Level Percent by Level
Other Users N Undergrad Graduate Prof Dev
Respiratory Therapist 11 16.4 17.7 17.2 Paramedic 13 21.8 5.9 31.0 Physicians Assistant 1 1.8 5.9 3.4 Physiotherapist 4 5.5 11.8 6.9 Occupational Therapist 1 1.8 0 0 Operating Room Practitioner 3 5.5 11.8 6.9 Midwife 0 0 0 0 Practical Nursing students 2 3.6 0 3.4 Physicians 4 7.3 5.9 3.4 Military 1 1.8 0 0 Workers (dev services, personal support) 2 3.6 0 First responders (fire, paramedic) 3 3.6 5.9 3.4 Assistants (physio and occup therapy) 1 1.8 0 0 Occupational assistants 1 1.8 0 0 Dentists 2 3.6 0 0 Note: Undergraduate N=55, Graduate N=17, and Professional Development N=29.
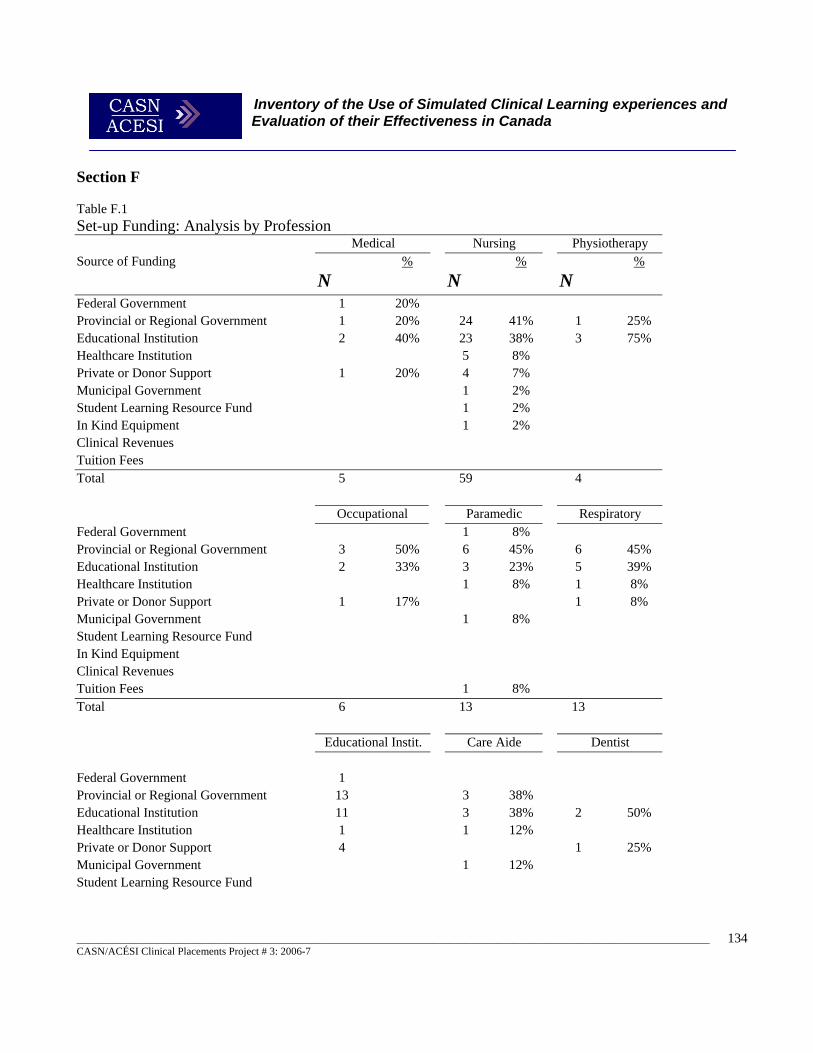
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
134
Section F Table F.1
Set-up Funding: Analysis by Profession Medical Nursing Physiotherapy Source of Funding
N %
N %
N %
Federal Government 1 20% Provincial or Regional Government 1 20% 24 41% 1 25% Educational Institution 2 40% 23 38% 3 75% Healthcare Institution 5 8% Private or Donor Support 1 20% 4 7% Municipal Government 1 2% Student Learning Resource Fund 1 2% In Kind Equipment 1 2% Clinical Revenues Tuition Fees Total 5 59 4
Occupational Paramedic Respiratory
Federal Government 1 8% Provincial or Regional Government 3 50% 6 45% 6 45% Educational Institution 2 33% 3 23% 5 39% Healthcare Institution 1 8% 1 8% Private or Donor Support 1 17% 1 8% Municipal Government 1 8% Student Learning Resource Fund In Kind Equipment Clinical Revenues Tuition Fees 1 8% Total 6 13 13 Educational Instit. Care Aide Dentist Federal Government 1 Provincial or Regional Government 13 3 38% Educational Institution 11 3 38% 2 50% Healthcare Institution 1 1 12% Private or Donor Support 4 1 25% Municipal Government 1 12% Student Learning Resource Fund
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
135
In Kind Equipment Clinical Revenues 1 25% Tuition Fees Total 30 8 4 Note. N = 64.
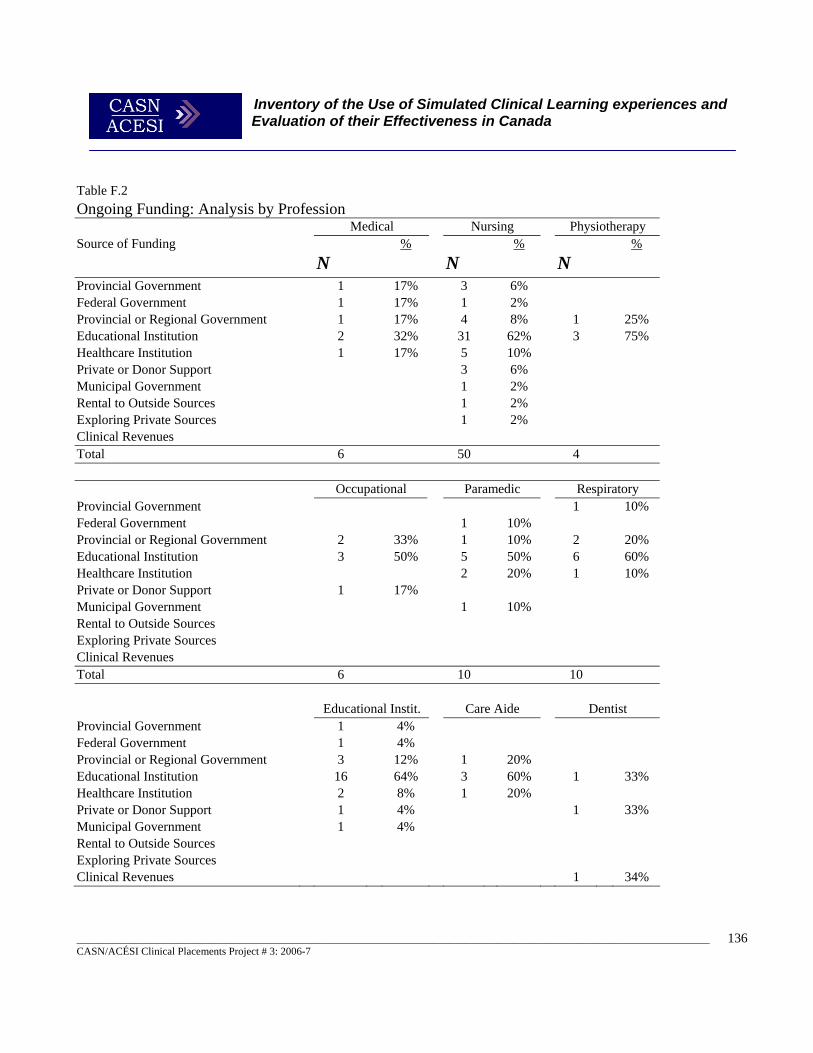
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
136
Table F.2 Ongoing Funding: Analysis by Profession Medical Nursing Physiotherapy Source of Funding
N %
N %
N %
Provincial Government 1 17% 3 6% Federal Government 1 17% 1 2% Provincial or Regional Government 1 17% 4 8% 1 25% Educational Institution 2 32% 31 62% 3 75% Healthcare Institution 1 17% 5 10% Private or Donor Support 3 6% Municipal Government 1 2% Rental to Outside Sources 1 2% Exploring Private Sources 1 2% Clinical Revenues Total 6 50 4
Occupational Paramedic Respiratory
Provincial Government 1 10% Federal Government 1 10% Provincial or Regional Government 2 33% 1 10% 2 20% Educational Institution 3 50% 5 50% 6 60% Healthcare Institution 2 20% 1 10% Private or Donor Support 1 17% Municipal Government 1 10% Rental to Outside Sources Exploring Private Sources Clinical Revenues Total 6 10 10 Educational Instit. Care Aide Dentist Provincial Government 1 4% Federal Government 1 4% Provincial or Regional Government 3 12% 1 20% Educational Institution 16 64% 3 60% 1 33% Healthcare Institution 2 8% 1 20% Private or Donor Support 1 4% 1 33% Municipal Government 1 4% Rental to Outside Sources Exploring Private Sources Clinical Revenues 1 34%
Inventory of the Use of Simulated Clinical Learning experiences and Evaluation of their Effectiveness in Canada
_______________________________________________________________________________________________________________________ CASN/ACÉSI Clinical Placements Project # 3: 2006-7
137
Total 25 5 3 Note. N = 64.





























