Embed Size (px)
Citation preview

Original Articles
Casemix - what is it and what does it mean to ophthalmology? Michael Goggin, FRCSI, FCOphth Robin Michael, BSc(Hons), GradDipCompSc, M P H
Abstract The Australian government is committed to the establishment of a prospective payment system based on casemix information for acute hospital care in the near future, because these systems are demonstrably socially equitable and more efficient than present ‘historical’ systems. Since ophthalmology is an outpatient-based speciality, the establishment of a good ambulatory casemix system is essential to this speciality. Considerable input from clinicians will be required to establish a satis- factory system, and to maintain it in years to come.
Key words: Casemix, eye.
Resources for health care are limited. Any equitable system of distribution of these resources must reflect need and current use. This can only be achieved by ascertaining current patterns of use and deciding where funds and other resources should be allocated. This process of data acquisition and its subsequent classification, in the broadest appli- cation, is casemix.
Casemix, traditionally, has addressed the problems of acute inpatient care quite comprehen- sively. Systems based on diagnosis-related groups (DRG) apply to inpatients exclusively. However, the Australian Federal Government is addressing the application of the principles of casemix to the non-inpatient setting as part of the process of readying the Australian health care system for a prospective payment system based on resource use. This is not unreasonable, since as much as 30% of
a typical acute hospital budget is spent in the provi- sion of non-inpatient services.‘
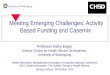
Ophthalmology is becoming more and more an outpatient-based speciality. Fewer patients are admitted to hospital, even for surgical procedures. Since 1988, when the then new ophthalmic day surgery facility at Flinders Medical Centre became fully operative, the numbers of ophthalmology patients treated in the general operating theatre has steadily decreased while the number of day cases has steadily increased (Figure 1). The overall number of inpatients, surgical or medical, has also fallen over this time, despite increased outpatient activity. Currently, the Department of Ophthal- mology at Flinders expends only 40% of its resources on inpatient services, 35% on same-day services and 25% on outpatient services. As ophthalmologists, therefore, it is important to us to ensure that any proposed non-inpatient casemix system is adequate.
Existing non-inpatient systems Several systems for classifying so-called ‘ambulatory encounters’ have been developed, mostly by the Health Care Financing Administration (HCFA) in the USA.
Ambulatory visit groups Ambulatory visit groups (AVGs) were developed at Yale University for HCFA. This system classifies individual patientlhealth-care professional encounters in the ambulatory setting. It is based on diagnosis (similar to DRGs) and classification depends on whether or not a procedure is carried
-
From the Flinders Medical Centre, Bedford Park, South Australia 5042. Reprints: Dr Michael Goggin.
Casemix 111

$ 700
& 600
& 400 a 300
100
81 82 83 84 85 88 87 88 89 90 91
Year =General theatre EZ Day surgery
Figure 1 Ophthalmic surgical procedures, 1981 to 1991.
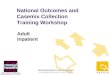
out and whether the patient is presenting for their first or a subsequent visit. A total of 571 types of encounter are identified. For historical reasons, encounters with radiologists, anaesthetists or pathol- ogists are excluded. The development of this system involved considerable clinical input, so the classifi- cation has quite good clinical relevance. The ‘logic’ (or grouping process) used is shown in Figure 2.
Ambulatory patient groups This is a second-generation classification system, and as such deals with some of the deficiencies of the AVGs. It also is based on patient visits and the initial classification variable is whether or not a procedure is carried out. Unlike most other ambula- tory systems, this system includes day surgery cases and accident and emergency cases as well as out- patient clinics.
Radiological encounters and the use of pathology and anaesthesia services are also addressed by this
Principal diagnosis related to body system?
I I
Yes + 22 MADC
I
t N O
23 MADC
t Preventive and
carried out? administrative AVGs
+ Significant procedure
A Yes No * t
Procedure AVGs Medical Medical
‘New patient’ repeat visit AVGs AVGs
Figure 2 Ambulatory visit groups (AVG) logic MADC= medical ambulatory diagnostic categories.
system. However, there is no differentiation between general and local anaesthesia. In addition, a number of ancillary tests and procedures, including chemotherapy administration, are dealt with in a quite detailed fashion. For those cases not undergoing a procedure, there are a number of medical APGs. If a case has a significant sign, symptom or finding but no diagnosis at a specific encounter, this can also be coded.
Figure 3 shows the logic for APG grouping. Figures 4 and 5 illustrate the logic for ophthalmology visits, both medical and involving significant procedures. Surgical groupings are made on the basis of the type of procedure, its site and degree of complexity. Medical grouping is on the basis of the primary reason for the visit. The lack of detail, from the clinical point of view, in the latter is due to the cost homogeneity of most visits that are not to do with cataract, refraction or conjunctivitis.
Products of ambulatory care and of ambulatory surgery The New York State Department of Health deve- loped these two systems (PAC and PAS). The PAC system classifies medical patients into 24 groups and has reference to four levels of service: diagnostic, therapeutic, problem management and ‘well care’. These four groupings are then subdivided, largely on the basis of speciality services. The PAS system was designed to categorise operating theatre time and is based on 42 categories of procedures subclas- sified by body system and type of procedure (diagnostic, therapeutic etc.). Its relatively small number of groups calls into question the clinical homogeneity of the groups.
Ambulatory casemix projects in Australia Flinders Medical Centre, Adelaide, and the Royal Children’s Hospital, Melbourne, were selected as
Significant procedure carried out? - Yes No + + + +
+ +
7 major medical 17 major procedure groups groups
Procedure, method, site etc.
Procedure APGs
Diagnosis, age, sex
Medical APGs
Figure 3 Ambulatory patient groups (APG) logic (general).
112 Australian and New Zealand Journal of Ophthalmology 1993; 21(2)

Non-invasive test Contact lens Laser - r Simple
Eye procedures 1
1 Site
Complex
- Lens
Anterior segment
Posterior segment
- Muscle
- Plastic
Glaucoma
Simple
Moderate Complex
Not glaucoma Simple
i I Complex
Simple
Complex
demonstration sites for the Ambulatory Encounters Project supported by the National Casemix Unit. This study spanned two years and is now drawing to a close. It involved, at Flinders, the computerised gathering of clinical and demographic data on nearly all ambulatory encounters within the hospital to allow evaluation of non-inpatient classification systems and to cost non-inpatient services at this hospital.
The system was first applied in the ophthalmology clinic, but now almost all points of patient contact are equipped with computer. terminals, code books with bar codes, and bar code readers. These are connected to a Mainframe VAX computer and encounters are coded by International Classification of Diseases-9 (ICD-9-CM) by the health-care worker who conducts the encounter. Flinders Medical Centre had previously carried out a cost estimating study on non-inpatient episodes and so was uniquely poised to undertake this project.’ Approximately 17 300 encounters in the eye clinic were encoded in the 18 months from January 1991 to 30 June 1992 when the data collection for this project took place.
Cataract
Refraction
Conjunctivitis t Other eye disorder
Figure 5 Ambulatory patient groups (APG) logic (ophthal-
‘Medical’ Visit
mology medical visits).
Figure 4 Ambulatory patient groups (APG) logic (ophthalmology pro-
cedures).
The New South Wales Health Department also undertook a non-inpatient casemix study called the National Ambulatory Casemix Project. This was to design a casemix classification system for Australian hospitals that could be easily and quickly implemented using data currently available in most Australian outpatient departments (i.e., without relying on complex computerised data gathering systems). This group has produced a draft summary report of their findings proposing a classification system or ‘grouper’ based on their study in 15 typical Australian hospitals nati~nwide.~ This work was presented at the recent Fourth National Casemix Conference. In the outpatient setting, the grouper relies for cost prediction on the collection of only three items of information: the medical speciality of the clinic attended; whether a doctor was present at the encounter; and whether the patient was a new or repeat patient.
Most hospitals could collect this kind of data with minimal extra effort. However, the clinical applica- tions of the information available from this form of grouping (because of its lack of homogeneity with regard even to diagnosis within the groups) will be limited. The report of this group on same day services is awaited.
The future in ambulatory care casemix To establish a useable system both for clinicians and management, several decisions must be made in consultation between these two interested parties. A successful casemix system in Australia will depend on cooperation between these groups. Both must gain tangible benefits from the tedious task of data collection in a routine setting. The occasional effort required to gather this kind of information for short-
Casemix 113

term studies is relatively easy. The constant effort to provide even a few extra seconds per encounter in a busy clinic to ‘code’ a patient can prove very irksome to a clinician pressed for time who regards his primary role as applying his clinical skills, not assisting in what he regards as a ‘management’ task. The alternative of employing professional coders is very expensive because of the large numbers of encounters to be encoded. Those best suited to carry out the task of coding are those with the greatest insight into the patient’s condition, presumably the clinician managing the patient. For this reason the maintenance of a high degree of clinical relevance is essential. The only way to ensure a successful system is to ensure clinician cooperation.
On a different level, decisions have yet to be made regarding the coding variables. The criteria used to choose these must rest on economic and clinical grounds. From the economic viewpoint, some vari- ables shown to affect cost in a predictable way are physician time (though this is not a reliable predictor of total cost when taken in isolation) in conjunction with some dichotomous variables, such as presence
or absence of drug prescription, and whether or not pathology or radiology services are used.2 From a clinical point of view, such variables as diagnosis, procedures carried out, demographics, and the dichotomous variables mentioned above are the minimum. If further data are required by local clini- cians, they could be collected as needed in any adequately constructed system. By and large, the amount of data required by clinicians is usually far in excess of that required by management.
The final product of such a system should be useable clinical information for the clinician, useable financial information for management, and value for money for the taxpayer.
References 1. Hindle D, Laffey J. Classification of ambulatory encounters
in hospitals: a preliminary investigation of needs and methods. Canberra: Australian Institute of Health, 1990.
2. Michael R, Piper K. Non-inpatient costing study. Aust Health Rev 1991; 14: 127-36.
3. Lagaida R, Hindle D. Design of an Australian ambulatory casemix classification: a summary report. Sydney: New South Wales Health Department, 1992.
114 Australian and New Zealand Journal of Ophthalmology 1993; 21(2)