Embed Size (px)
Citation preview

Case studyJanssen Pharmaceutical - Bedaquiline
Clinical Development On-campus

OpeningDeveloping a new treatment for tuberculosis for patients with limited current
treatment options
On Monday, November 24, 2004 Koen Andries, a senior discovery scientist at the
pharmaceutical company Janssen Pharmaceutica in Beerse, Belgium (a subsidiary of
the American multinational pharmaceutical company Johnson & Johnson) received
word from the editor of the scientific journal Science that his manuscript reporting
the discovery and development of the new antibiotic R20791001 for treating tuber-
culosis (TB) had been accepted for publication. This was exciting news and was in
stark contrast to a previous message regarding the very same manuscript a few weeks
earlier in which the editor stated that the manuscript had been rejected and would
not be sent for review (Exhibit 1). After a second, closer look, the editor reconsidered
their earlier decision and sent the manuscript for review after all. In their assessment,
both reviewers were highly positive and advised Science to publish the manuscript;
as one reviewer wrote, “given the healthcare crisis as a result of TB-HIV co-infec-
tion and rising resistance to existing TB drugs, this is an extraordinarily important
study and… of broad interest to the scientific and healthcare community” (Exhibit
2). The reviewer’s statement that TB is a current health crisis clearly fits the current
situation in developing countries. Each year, approximately 2 million people die of
TB, which corresponds to more than 5,000 patients each day! A full one-third of the
world's population is estimated to carry a latent M. tuberculosis infection, and 10% of
these individuals will eventually develop TB. Because it was such a landmark study
and was highly relevant to the field of TB, Science’s editor informed Andries that the
paper would be published online on December 9, 2004 and would appear in print on
January 14, 2005.2
Publication of their paper in the prestigious journal Science was a triumph for Andries
and his colleagues. The research that led to the discovery of these new anti-TB phar-
maceuticals began seven years previously and had not been easy. Along the way,
numerous challenges arose, many issues had to be resolved, and internal committees
had to be convinced of the potential of R207910.
1 Since the founding of Janssen Pharmaceutica in 1953, all compounds synthesized at the company were assigned a distinct R number. In 1955, R5 (ambucetamide) was the first Janssen Pharmaceutica drug approved by health authorities for the relief of menstrual pain. R5 was discovered in 1953 by the company’s founder, Dr. Paul Janssen.2 Andries K, Verhasselt P, Guillemont J, Göhlmann HWH, Neefs J-M, Winkler H, Van Gestel J, Timmerman P, Min Zhu, Lee E, Williams P, de Chaffoy D, Huitric E, Hoffner S, Cambau E, Truffot-Pernot C, Lounis N, Jarlier V. A diarylquinoline drug active on the ATP synthase of Mycobacterium tuberculosis. Science 2005 Jan 14; 307(5707): 223-7. Epub 2004 Dec 9.
Finally, in the middle of 2004, Andries and his colleagues (both within and outside the
company) were able to demonstrate that R207910 was a promising new antibiotic for
treating TB.
The results described in their 2005 Science paper were impressive. They reported
that R207910 binds a completely novel target, the first new target to emerge after
four decades of research in the field of TB. Andries’ team had also elucidated the
compound’s mechanism of action and found that the compound has potent in vitro
activity against both replicating and non-replicating bacilli. Andries’ team also showed
that R207910 was much more effective than reference compounds in a murine model
of TB infection, exerting significant bactericidal and sterilizing activity. In addition, the
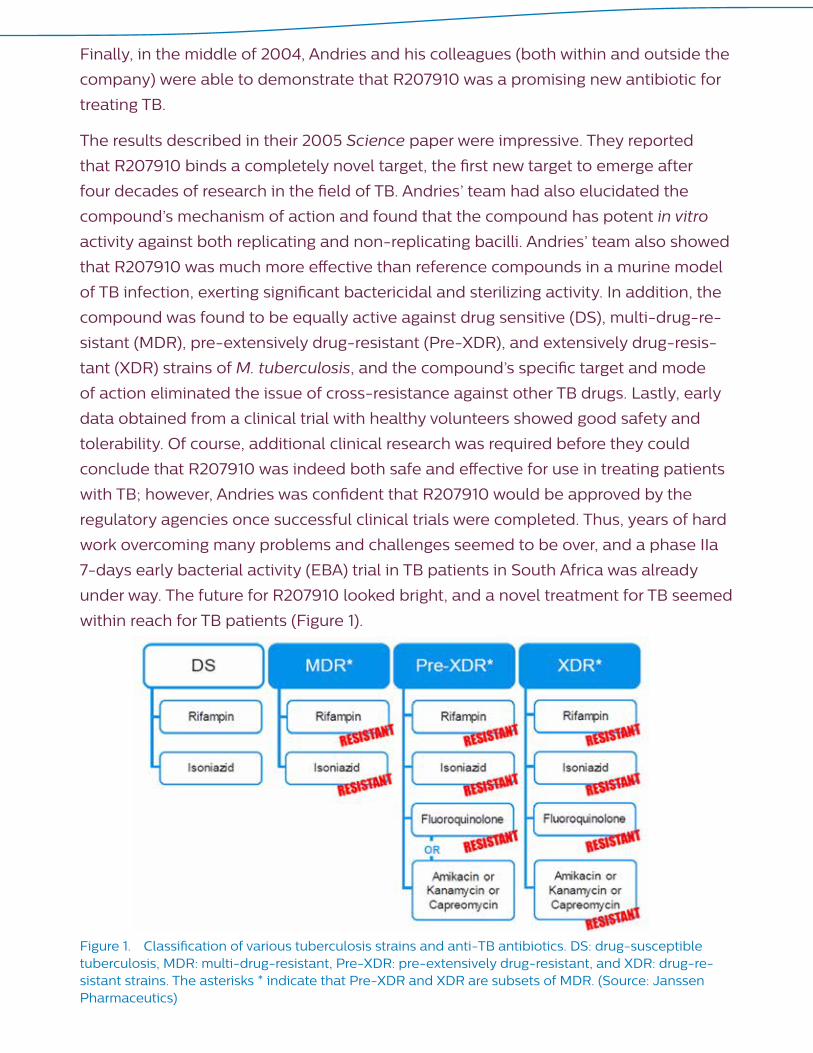
compound was found to be equally active against drug sensitive (DS), multi-drug-re-
sistant (MDR), pre-extensively drug-resistant (Pre-XDR), and extensively drug-resis-
tant (XDR) strains of M. tuberculosis, and the compound’s specific target and mode
of action eliminated the issue of cross-resistance against other TB drugs. Lastly, early
data obtained from a clinical trial with healthy volunteers showed good safety and
tolerability. Of course, additional clinical research was required before they could
conclude that R207910 was indeed both safe and effective for use in treating patients
with TB; however, Andries was confident that R207910 would be approved by the
regulatory agencies once successful clinical trials were completed. Thus, years of hard
work overcoming many problems and challenges seemed to be over, and a phase IIa
7-days early bacterial activity (EBA) trial in TB patients in South Africa was already
under way. The future for R207910 looked bright, and a novel treatment for TB seemed
within reach for TB patients (Figure 1).
Figure 1. Classification of various tuberculosis strains and anti-TB antibiotics. DS: drug-susceptible tuberculosis, MDR: multi-drug-resistant, Pre-XDR: pre-extensively drug-resistant, and XDR: drug-re-sistant strains. The asterisks * indicate that Pre-XDR and XDR are subsets of MDR. (Source: Janssen Pharmaceutics)

Despite its early promise, just a few months later a dark cloud settled over the TB
project. First, Andries received the initial data from the phase IIa clinical trial with TB
patients. The results showed that although R207910 (or TMC207, as the compound
was also known) had some therapeutic effect at the highest dose tested, unex-
pectedly—and in sharp contrast with the mouse studies—R207910 seemed to be
less effective than the reference compounds. The second, however, was far more
devastating to the project: the follow-up data from the phase I trial with healthy
volunteers revealed that R207910 had a terminal half-life of approximately 5 months.
Andries knew that this would be considered as an undesirable attribute for a drug that
was also a neglected disease medicine that would likely fail to produce a profit. The
disappointing phase IIa results, together with the long terminal half-life, were shared
and discussed by top management while checking in at an airport in December 2015.
Karel de Beule, the product development team leader at the time, was informed that
the company would no longer continue to develop R207910.
Andries immediately realized that fast action was needed if he was to rescue
R207910. After all, R207910 was not simply a “me-too” drug or a lifestyle drug. Here
was a compound that could potentially save the lives of the increasing numbers of
patients with MDR-TB and XDR-TB strains of TB. Although Andries had established
an impressive track record as a successful drug-discovery scientist for more than 22
years, he knew that his reputation with the company would not be sufficient; the team
would have to come up with solid, convincing data. De Beule’s team would need to
pore through all of the results obtained in the past seven years in an attempt to find
data that would convince top management the reverse their decision to terminate the
TB project. As Andries was thinking of the best way to tackle this new challenge, his
computer beeped with an incoming email. Immediately upon reading the email, his
mouth went dry and his eyes went moist. The message came from a medical doctor in
the Ukraine who apparently had read his Science paper on R207910.
“Dear Sir,
[….] I am 39 now and I am dead-sick: I suffer from polyresistant tubercu-
losis of the spinal cord and brain ………the disease comes treacherously
towards my eyes. I called the Ukrainian embassy in Brussels and our dip-
lomats are ready to assist in delivery your medicine. Maybe …… you can
treat me as a volunteer? […..]
Please help me!
DO NOT TURN ME DOWN!”

This heartbreaking message hit Andries hard. This was not the type of email he
usually received from fellow researchers who wanted to exchange scientific ideas
and data; this was a desperate cry for help from a distressed patient with TB, a
terminal patient with no treatment options. He realized that—of course—there was
no way his company would be able to provide the compound to this patient, as its
clinical development was still in the early stages and the project had recently been
terminated. Even if top management would decide to reconsider their decision and
he could manage to deliver R207910 to this patient, his company would be heavily
criticized for providing an experimental, potentially dangerous compound to a
desperate, vulnerable patient. Andries became even more determined to find sufficient
arguments to convince the internal review committees and top management that the
development of R207910 should continue. He discussed his thoughts with De Beule
and other colleagues who also believed in the compound, and as a starting point they
decided to re-evaluate the pre-clinical and clinical data, summarized in the Investiga-
tor’s Brochure. They realized that in order to present their findings at the next meeting
of the three internal review committees, there was no time to lose.
Background
The early years at the University of Ghent
When Koen Andries was 18 years old, he needed to choose between his two interests:
medicine and veterinary science. He decided to study veterinary science at the
University of Ghent in Belgium, primarily because the program would take only six
years compared to seven years for medical school. During his studies, he initially
considered becoming a practicing veterinarian; but towards the end of his final year,
he had developed an interest in research and wrote a scientific paper. His professor
in veterinary virology was impressed by the paper and offered Andries a job as his
assistant at the university. Andries accepted and began immediately after graduation
in the summer of 1975.
Andries worked as a virologist at the University of Ghent for seven years. During that
time, he studied veterinary vaccines as well as the pathogenesis of vomiting and
wasting disease, a viral disease in pigs caused by the porcine hemagglutinating en-
cephalomyelitis (PHE) virus. Andries used immunofluorescence to understand the
pathogenesis of PHE by sacrificing experimentally infected piglets at several time
points and studying their organs.3 Using this method, which was considered
cutting-edge at the time,
3 Andries K, Pensaert MB. Immunofluorescence studies on the pathogenesis of hemagglutinating en-cephalomyelitis virus (HEV) in pigs after oronasal inoculation. Am J Vet Res 1980; 41: 1372-1378.

Andries and his colleagues demonstrated that the PHE virus first replicates in the
gastrointestinal tract and then migrates along the vagus nerve to the brain stem, where
it replicates in the vomiting center, ultimately producing the disease’s characteristic
clinical signs, vomiting and wasting. This discovery was Andries’ first major scientific
achievement, and his results were published in several scientific papers. When he
presented his work on vomiting and wasting disease at a conference on coronaviruses
in Munich in 1979, he apparently caught the eye of Dr. D.A.J. Tyrrell, who published a
report of the conference in Nature.F4 That positive report would help Andries get a job
at the University of Antwerp a few years later.
Applying for a job at Janssen Pharmaceutica
In 1982, the University of Ghent announced a hiring freeze, and Andries had to leave
the faculty. He applied for a part-time professorship position at the University of
Antwerp. At about the same time, he applied for a research position at Janssen Phar-
maceutica, and he was interviewed by several staff members. At Janssen Pharma-
ceutica, two scientists wanted to hire Andries for two different research projects. One
scientist wanted him to assess the in-licensing of a vaccine against foot-and-mouth
disease, a job for which Andries was well-suited based on his prior experience with
veterinary vaccines. The other scientist was doing preliminary antiviral research and
had identified a compound that was active against herpes simplex virus in vitro. He
was looking for a researcher to study this compound in further detail. During his
interview, Andries met with three or four staff members throughout the company’s
hierarchy. Eventually—and before he realized it—he was introduced to Dr. Paul
Janssen (or “Dr. Paul”, as people used to call him), the company’s legendary founder
himself. Dr. Paul was interested in Andries’ previous achievements and was becoming
interested in antiviral compounds. At around that time, the pharmaceutical company
Burroughs Wellcome had published the first positive antiviral results using acyclovir, an
antiviral against the herpes simplex virus. That paper had caught Dr. Paul’s attention,
making him realize that medicines could be used to cure viral diseases. When Dr.
Paul asked Andries what he thought about developing drugs for viral diseases, the
reply was brutally honest: “I don’t really know much about it. I do know that viruses
are replicated by the host cells, and that it’s not easy to interfere with that replication
without disrupting the host cell’s metabolism. But some antivirals have selective
activity, so I think it can be done. I’d certainly like to try.” Dr. Paul apparently liked
this frank answer and hired Andries, even though he admitted knowing little about
antivirals.
4 Tyrrell DAJ. Viral pathogenesis and virulence. Nature1979; 280: 194.

During his interview at Janssen Pharmaceutica, Andries mentioned that he had also
applied for a part-time teaching position at the University of Antwerp. The company
had no objections, and when Antwerp offered him the part-time teaching job, Andries
successfully combined his research at Janssen Pharmaceutica with his teaching re-
sponsibilities.
Andries’ first research projects in the company
Andries first worked on the compound with in vitro activity against herpes simplex
virus. His task was to characterize the compound’s activity and establish in vivo models
that could be used to confirm its activity. Andries tested the compound both on mice
and guinea pigs, but was unable to replicate the in vitro activity in vivo. This was a
disappointing finding, particularly because he was unable to explain it. Andries then
decided to test the compound in other cell lines, as it had only been tested previous in
one cell line. The results were immediately clear: the compound was only active in that
one cell line, and not in any other cell lines tested. This striking result likely explained
why he saw no activity in vivo. Although the scientist in him wanted to investigate why
this drug was so cell type-specific, the drug developer in him realized that it would not
likely lead to a viable new drug, so he abandoned this line of research.
In the meantime, he had identified another promising compound that was effective
against human rhinoviruses (the family of viruses responsible for the common cold),
and this compound formed the basis of Andries’ first major research project, a project
that would last more than a decade. Initially, Andries and his colleagues identified
compounds that were active against only a few of the more than 100 rhinovirus
serotypes.5 Later, they discovered another group of compounds that was active against
other serotypes. By combining these two chemical scaffolds into hybrid structures,
they created broad-spectrum antiviral compounds.6 In addition, they deciphered the
mechanism of action: the compounds bind to the virus’ capsid, preventing uncoating
of the viral particles in the host cell. Interestingly, these broad-spectrum uncoating
inhibitors were also effective against polioviruses and other picornaviruses. It was a
very exciting time in the antiviral research world, and the team had several scientific
breakthroughs.
For example, by screening a panel of capsid-binding compounds against all known
rhinovirus serotypes, they were able to decipher the phylogeny of the rhinovirus
5 Andries K, Dewindt B, De Brabander M, Stokbroeckx R, Janssen PAJ. In vitro activity of R 61837, a new antirhinovirus compound. Arch Virol; 1988, 101: 155-167.6 Andries K, Dewindt B, Snoeks J, Willebrords R, Van Eemeren K, Stokbroekx R, Janssen, PAJ. In Vitro Activity of Pirodavir (R 77975), a Substituted Phenoxy-Pyridazinamine with Broad-Spectrum Antipicor-naviral Activity. Antimicrobl Agents and Chemother 1992; 36: 100-107.

group.7 Several compounds moved into phase I and phase IIa trials with human
subjects. The synthetic antiviral R61837 became the first compound with demon-
strated clinical effect in human volunteers infected with rhinoviruses.8 R77975 (i.e.,
pirodavir) became the first broad-spectrum compound effective against rhinoviruses.
Unfortunately, however, and as is often the case, the drug’s ADME profile9 was the fly
in the ointment. The team tried to develop orally bioavailable alternatives, but that
was problematic as well—because the compounds were esters, esterase activity in the
plasma rendered them inactive upon absorption. The results were disappointing, and
the project was terminated.
Exciting years in HIV research
In 1986, Andries began another large research project that focused on developing
antivirals against HIV. At the time, Dr. Paul had become highly interested in the
agent that causes AIDS. Science and Nature published several papers written by the
scientist Peter Duesberg, who was quite skeptical of the idea that AIDS was caused
by a virus. Andries and Dr. Paul had many lively discussions about the cause of AIDS
and whether drugs against HIV might be used to treat the disease. In the end, they
became convinced that HIV was indeed the cause of AIDS, and they decided to
initiate a project to develop antivirals that would be effective against HIV. However,
this was not a trivial undertaking. In those early days, only a few labs in the world—
including the group of Luc Montagnier and Françoise Barré-Sinoussi and the group
of Robert Gallo—had samples, and initially no one had been able to culture the virus.
So Dr. Paul was pushing Andries to find a solution: “What can we do? What can we
do?” But Andries was busy with his anti-rhinovirus research and did not know how
he could undertake another major research project at Janssen Pharmaceutica. In
addition, Dr. Paul had concerns about bringing HIV to the company. In those days,
nearly everybody was afraid of the virus, a situation comparable with today’s fears
surrounding the Ebola virus. Dr. Paul feared a negative response from labor unions
if they brought HIV to the company. Thus, they had to overcome this obstacle if they
were to develop antivirals for treating AIDS.
7 Andries K, Dewindt B, Snoeks J, Wouters L, Moereels H, Lewi PJ, Janssen PAJ. Two groups of rhi-noviruses revealed by a panel of antiviral compounds present sequence divergence and differential pathogenicity. J Virology 1990; 64: 117-1123.8 Al-Nakib W, Higgins PG, Barrow GI, Tyrrell DAJ, Andries K, Vanden Bussche G, Taylor N, Janssen PAJ. Suppression of colds in human volunteers challenged with rhinovirus by a new synthetic drug (R61837). Antimicrob Agents and Chemother 1989; 33(4): 522-525.9 ADME is a pharmacokinetics and pharmacology term meaning absorption, distribution, metabolism, and excretion. A compound’s ADME profile describes its disposition within an organism. These four factors influence the drug levels and the kinetics of drug exposure in the tissues and therefore influence the compound’s performance and pharmacological activity.
In 1986, Andries attended a meeting on antiviral research in Rotterdam, the
Netherlands, where he met Dr. Rudi Pauwels, a young researcher working in Professor
Eric de Clercq’s group at the University of Leuven, Belgium. Professor Eric de Clercq
had obtained an HIV sample from Japanese virologist Hiroaki Mitsuya and was able
to culture the virus in MT4 cells in vitro. Pauwels was using phenotypic screening to
identify antiviral compounds. In this method, the virus is produced by cells in culture,
and test compounds are added to the cells. The antiviral activity of the compounds
is then measured by quantifying the inhibition of virus production. Andries was quite
pleased to find a researcher who was culturing the virus and screening antivirals using
an approach that he felt was likely to succeed. Andries then discussed this promising
meeting with Dr. Paul, who immediately agreed to collaborate with Pauwels to
develop new drugs against HIV. In this collaboration, Janssen Pharmaceutica would
provide the compounds for screening, and the viral testing would be done at the
University of Leuven.
Once Janssen Pharmaceutica and the University of Leuven agreed on the specifics
of their collaboration, Dr. Paul and Andries selected a list of compounds for testing.
At that time, Janssen Pharmaceutica had nearly 100,000 compounds in its chemical
library, which was far too many to screen using Pauwels’ assay. Rather than choosing
compounds at random, Dr. Paul and Andries selected representative compounds from
a variety of chemical classes and scaffolds. The final “short” list contained approxi-
mately 600 compounds, which Pauwels then tested using his in vitro assay. Within six
months, he identified a compound—called R14458—that had in vitro anti-HIV activity
when applied at a concentration of 14 µg/ml. Importantly, R14458 had a selectivity
index of 10, meaning that the cytotoxic concentration was ten-fold higher than its
antiviral concentration, suggesting that the compound had high antiviral specificity.
R14458 was the first member of what would eventually become the tetrahydro-imid-
azobenzodiazepine (TIBO) class of compounds. After the discovery of R14458 in the
late 1980s, medical chemists were recruited to the project. Thus, Dr. Paul asked Mike
Kukla at Janssen Pharmaceutical’s Spring House, Pennsylvania division to synthesize
new analogs of R14458.
An interesting finding was that R14458 represented a subclass of compounds in their
extensive library. Once they learned that R14458 had anti-HIV activity, Andries and
his colleagues immediately looked at the other compounds in this subclass that
were structurally related to R14458 but were not included in the initial list. However,
although approximately 50 other compounds were chemically similar to R14458,
R14458 was the only member of the subclass with antiviral activity for HIV. Thus, their
initial choice of R14458 was extremely fortuitous.

Dr. Kukla synthesized several analogs of R14458 that were active against HIV, and he
increased the antiviral activity considerably by making various changes to the chemical
structure. Ultimately, the research team had several compounds with robust anti-HIV
activity in vitro. They had also elucidated the mechanism of action—compounds
appeared to act by inhibiting the virus’ reverse transcriptase via a mechanism that
differed from existing, nucleoside-based inhibitors of reverse transcriptase. Thus,
Janssen Pharmaceutica and their collaborators had developed the first non-nucle-
oside-based reverse transcriptase inhibitors (or NNRTIs). These exciting new results
were published in Nature.10
Unfortunately, once again the ADME profile was a fly in the ointment, as the
compounds were absorbed poorly when taken orally. In the UK, Prof. Brian Gazzard
tested the compounds in AIDS patients by administering the drugs intravenous-
ly. However, the results were disappointing, as they had no effect on the CD4
count, which was used as a readout of antiviral activity (in those days, researchers
were unable to measure viral loads). Ultimately, the TIBO group of compounds
was abandoned; in the meantime, the research team had discovered several other
chemical scaffolds with anti-HIV activity, some of which were bioavailable when taken
orally.
At about the same time, competitors had successfully developed their own NNRTIs.
For example, Boehringer Ingelheim and DuPont Pharmaceuticals developed
nevirapine and sustiva, respectively. So even though Andries, Dr. Paul and Pauwels
first discovered the NNRTI class of compounds, two rival companies had more success
in terms of developing orally bioavailable, clinically active NNRTIs.
In the early ninethies, the first NNRTI-resistant HIV strains were reported in patients
who had been treated with competitors’ NNRTIs. In 1993, Andries realized that
Janssen Pharmaceutica was too far behind its competitors to develop simply another
class of first-generation NNRTIs. Therefore, he suggested to aim for second-genera-
tion NNRTIs that would hopefully be effective against these new resistant strains of
HIV.
10 Pauwels R, Andries K, DeSmyter J, Schols D, Kukla MJ, Breslin HJ, Raeymaeckers A, Van Gelder J, Woestenborghs R, Heykants J, Schellekens K, Janssen MA, De Clercq E, Janssen PAJ. Potent and selective inhibition of HIV-1 replication in vitro by a novel series of TIBO derivatives. Nature 1990 (01 February 1990); 343: 470 – 474; doi:10.1038/343470a0

Also in 1993, it was discovered that HIV isolates carrying identical mutations in reverse
transcriptase did not have necessarily have the same IC50 values.11
This was a critical observation, as it suggested to Andries it would need a panel
of recombinant viruses, each with different point mutations in the same genetic
background if they were to develop drugs that would be effective against viruses with
first-line NNRTI mutations. A list of the most promising clinical mutants was quickly
prepared and discussed with Pauwels. To optimize the lead structures, Andries, Dr.
Paul and Pauwels decided to study the effects of individual chemical changes on
individual point mutations. In this respect, it was extremely important that the medical
chemist had a clear idea of what would happen if he modified the compound (in other
words, which changes to the compound would yield good activity on one HIV mutant
but not on another HIV mutant).
In 1995, Pauwels and colleagues—now at Tibotec—created the panel of NNRTI-resis-
tant HIV strains and began screening the chemical scaffolds again, this time against
both the original wild-type HIV virus and the new panel of resistant strains.
11 The half-maximal inhibitory concentration (IC50) is a measure of a compound’s ability to inhibit a specific biological and/or biochemical function. This quantitative measure indicates the concentration of a given drug is needed to inhibit 50% of a given biological process (or component in a process such as an enzyme, cell, cellular receptor, or microorganism). According to the FDA, the IC50 is defined as the concentration of a drug that provides 50% inhibition in vitro.
Pauwels did not remain at the University of Leuven. Although he was
a pharmacist by training, he was part of the medical faculty. And as a
trained pharmacist, his upward mobility in the medical faculty was rel-
atively limited. This was a source of frustration to Pauwels, an excellent
scientist who did solid research. He discussed his situation with Dr. Paul,
who offered to support him financially for five years so that he could con-
tinue his HIV research. This was certainly a generous offer, plus it saved
their promising HIV program. Then Dr. Pauwels made a clever move: he
took his agreement with Dr. Paul tofinancial investors. Because he had
secure income for the next five years, the banks were willing to lend him
additional capital. Pauwels now had the money he needed to create his
own biotech start-up company. Andries suggested the name “Tibotec”, a
reference to the TIBO compounds, and in 1994 Pauwels founded Tibotec.

Andries, Dr. Paul and Pauwels soon identified one scaffold that was not only active
against the wild-type strain as well as several—but unfortunately, not all—of the NN-
RTI-resistant strains. They realized that it might be possible to optimize this scaffold in
order to achieve broad-spectrum activity. However, their research was complicated by
the fact that their lead compound was metabolized rapidly by liver enzymes, again an
ADME-issue.
Therefore, Andries developed a bioassay by incubating all of the derivatives with
liver extracts, and Pauwels measured the anti-HIV activity of these derivatives both
before and after incubation, thereby measuring the extent to which the derivatives
were metabolized. Finally, fate smiled on the research team. Using their bioassay,
they were able to identify three separate metabolic “hot spots” in the lead compound,
and chemically modifying these hot spots yielded metabolically stable compounds.
At the same time, medical chemists Mike Kukla and Don Ludovici examined further
the activity against NNRTI-resistant mutants and eventually succeeded at making
chemical modifications that both increased the drug’s anti-HIV activity and increased
metabolic stability. This time-consuming process took nearly three years of intensive
research, but in April 1998, R147681 (which was later renamed TMC120, dapivirine) was
the first compound in the series to be selected by Janssen
Pharmaceutica for testing in humans. Shortly after that, new bioassay results provided
the key for a chemical modification that led to the discovery of R165335 (later renamed
TMC125), which was also known by its brand name, intelence.
In the summer of 1999, Andries recommended that R165335 undergo further
development based on its antiviral activity against NNRTI-resistant strains, its
metabolic stability, and its favorable plasma levels in animals. In December 1999,
Janssen Pharmaceutica’s internal Development Research Committee (DRC) agreed
to take R165335 to clinical development. In March 2000, a licensing agreement was
reached between Janssen Pharmaceutica and Tibotec (which was then a privately
held biotech company) for the development of intelence; in the agreement. Tibotec
did an excellent job developing intelence, which was not an easy task given that the
compound is highly insoluble. It was therefore quite an achievement to develop the
optimal formulation and bring the compound to the clinic. Their success paid off, and
intelence had robust activity against viral load in phase IIa studies. In 2001, Andries,
Dr. Paul and Pauwels had selected a second NNRTI, edurant, which had excellent
anti-HIV activity at extremely low doses, for further testing.
At about the same time, and independent from Janssen Pharmaceutica, Tibotec
acquired the rights to a protease inhibitor and performed additional chemical modifi-
cations, eventually developing the broad-spectrum protease inhibitor darunavir, inde-
pendently from Janssen Pharmaceutica. They applied the same strategy. A panel of
protease-resistant HIV strains was used to screen all three new compounds (intelence,
edurant, anddarunavir) for their activity against both wild-type and resistant strains of
HIV.
In 2002, Johnson & Johnson had the choice between leaving the HIV field altogether,
re-obtaining the licensing rights to intelence, or acquiring Tibotec, thereby obtaining
the rights to both intelence anddarunavir. They decided to acquire Tibotec, and
Tibotec became responsible for the clinical development ofdarunavir, intelence, and
edurant, which were approved by the FDA in June 2006, January 18 2008, and May
2011, respectively. Dapivirine is still being developed as a vaginal microbicide for use in
resource poor countries by International Partnership for Microbicides (IPM), an NGO.
The bedaquiline story
The search for non-azole-based antimycotics…
In the early 90’s, the famous mycologist Dr. Frank Odds joined Janssen Pharma-
ceutica to run the Mycology and Bacteriology department and to discover and
develop non-azole-based antimycotics. Janssen Pharmaceutica had been previously
successful at developing azole-based antimycotics such as ketoconazole and itracon-
azole, and they were now interested in developing non-azole-based antimycotics.
In addition to screening for new antimycotics, the company was also interested in
developing antibiotics against Helicobacter pylori. This was a strategic decision by the
company’s management. In the mid-1990s, Australian researchers discovered that
gastric ulcers were not caused by stress (as previously believed), but by the bacterium
Helicobacter pylori. Antacids, which were commonly used to control the symptoms
associated with gastric ulcers,12 drew large revenues, and this piqued the company’s
interest, as an antibiotic effective against H. pylori could potentially replace antacids
in the market. In his search for such an antibiotic, Odds decided to include Mycobac-
terium tuberculosis, the bacterium that causes TB, in his screen. This decision was
inspired by the World Health Organization’s statement in 1993 that TB had once again
risen to the level of a Global Health Emergency. This new TB pandemic was indirectly
due to the sharp increase in the number of HIV-infected patients: patients with AIDS
have a compromised immune system, which can activate tuberculosis in patients with
a latent M. tuberculosis infection.
12 Antacids are a type of medicine that can control the acid levels in your stomach.

Until that time, the research community had been generally complacent regarding TB,
as the disease was considered to be under control. As a result, very few researchers
were developing new antibiotics for treating TB. Spurred on the WHO statement,
Odds was keenly interested in developing compounds against this deadly bacterium.
However, a major obstacle stood in his way: his department did not have a biosafety
level 3 lab, which was required in order to work with Mycobacterium tuberculosis. He
solved this problem by using Mycobacterium smegmatis, a related—but nonpatho-
genic—mycobacterium.
Adopting this strategy was a bold decision and potentially a long shot, as compounds
that are effective against M. smegmatis are not necessarily effective against M. tuber-
culosis. The decision to initiate TB research at Janssen Pharmaceutica was not made
by upper management, nor was upper management even informed during the early
stages in the project. Indeed, the decision was made solely by Odds. This decision may
seem controversial in retrospect, but it is important to understand that researchers as
Janssen Pharmaceutica were generally allowed to perform small experiments without
consulting upper management, as long it did not involve excess costs or staff, and may
end up in a discovery. In the case of initiating TB research, the costs were relatively low
and only required adding some mycobacteria to a screen that was already planned.
The discovery of an antibiotic effective against H. pylori and
mycobacteria
Odds initially discovered a diarylquinoline compound which was synthesized by
medical chemist Jérôme Guillemont, with activity against H. pylori, and management
was informed. The level of activity was considered sufficient to initiate an optimization
project. Interestingly, the compounds that were found to be active against H. pylori
were also somewhat active against M. smegmatis (although the link had not been
established at that time). A lead optimization program was initiated, and R207910 was
one of the compounds included in the program. Despite his success, Odds’ primary
interest was finding new antimycotics that have a non-azole-based mechanism of
action. Unfortunately, he was not successful at that, and he left the company in 1999.
Taking over the TB project
Dr. Jef van Gestel was Odds’ successor. Van Gestel sent samples of R207910 to four TB
experts for testing against M. tuberculosis, but received somewhat conflicting results.
Two laboratories (one in vitro and one in vivo) reported that the compound was active,
whereas the other two laboratories (again, one in vitro and one in vivo) found no
activity.

In 2001, Janssen Pharmaceutica underwent a major reorganization. As a result, the
Mycology and Bacteriology department—where the TB research project had begun—
was closed, and Van Gestel retired, leaving R207910 sitting on the shelf. When Van
Gestel left the company, Andries took over the R207910 project. Although Andries
had been exclusively researching viruses for more than 25 years, he was very keen
on doing antibacterial research. His theoretical expertise by teaching Microbiology at
the University of Antwerp certainly helped him. He was passionate about developing
a drug for which there was such a high medical need. The challenges he faced were
clear. First, the results obtained from four external labs were conflicting. Moreover,
R207910 was extremely difficult to solubilize, given its apparent cLogP value of 7.2.13
In addition, R207910 was actually a mixture comprised two diastereoisomers with two
enantiomers each, and only one of these four chemical variants was active.
Developing a drug containing several chemical variants is generally not ideal, as
the inactive variants may have unwanted side effects. Moreover, obtaining the pure
enantiomer early in the development process is important from both a production
perspective and a financial perspective. Thus, medical chemists must find the best
strategy for producing the pure compound during a development process.
13 Solubility of a compound in both water and fat is one of the properties that determines its bio-availability, as an orally administered drug must first pass through the intestinal lining, be carried in aqueous blood, and finally penetrate the lipid-based cell membrane to reach the inside of the target cell. A model compound for the lipophilic cellular membrane is 1-octanol (a lipophilic hydrocarbon). The logarithm of the octanol/water partition coefficient (known as the LogP) is used to predict the solubility of an oral drug. If LogP is calculated (rather than measured experimentally), the term is called “cLogP”. A compound with a cLogP value of 7 means that the compound dissolves in organic solvents 107 times better than in aqueous solvents.
The discovery power of phenotypic screening
R207910 was discovered by phenotypic screening using cultured M.
smegmatis. Andries is a strong proponent of phenotypic screening, as it
is more efficient than using a target-based approach for screening new
anti-infection agents. “It is really quite easy to explain,” says Andries.
“With phenotypic screening with cultured mycobacteria, you’re actually
testing every compound against 614 targets at the same time, because
M. tuberculosis contain 614 genes that are essential for bacterial growth.
Thus, phenotypic screening is 614 times more efficient than single tar-
get-based assays. On the other hand, phenotypic screening can be a little
more labor-intensive. With some target-based screens, you can perform

high-throughput screening. With phenotypic screening, you can easily
test 100 compounds in a week or so, which I would call ‘medium-through-
put’ screening. Of course, you have to be smart in your approach. Rather
than randomly choosing compounds, you make strategic choices. This
approach has two key components: you need to select the best screen-
ing strategy, and you need to select the right compounds to screen. One
always talks about finding the needle in the haystack. I say you need to
find the right haystack first. Not every haystack contains a needle, and
some may contain several needles. At Janssen, our haystack—our chemi-
cal library—contains many needles. Why? Because Dr. Paul was an excel-
lent medical chemist, who motivated his medical chemists to synthesize
compounds with drug-like properties. In this respect, Janssen Pharma-
ceutica’s haystack is pure gold. But the sheer size of the library is not the
most important factor; quality, not quantity, is what matters most. You can
screen a million compounds and still not find a drug. I give Dr. Paul a lot
of credit for creating an excellent library of compounds. For example, we
discovered at least ten different scaffolds with activity against HIV. We also
found three or more scaffolds with nanomolar activity against respiratory
syncytial virus, and scaffolds with activity against rhinoviruses and the in-
fluenza virus. For nearly every virus we tested, we found reasonably selec-
tive compounds with moderate activity at µg/ml activity. If you then put a
medical chemist on the project, you can increase that activity by a factor
of 100 to 1000 in just a couple of years. In our hands, it worked every time.
People may say, ‘You were lucky.’ But if you are successful ten times in a
row, then there must be more to it than just luck.”
In 2001, the active enantiomer in R207910 was purified and tested in mice. The results
arrived in 2002 and were far from promising. At high doses, the drug killed the mice,
whereas at lower doses no response was measured. These findings—together with
the conflicting results from the four external labs—opened the project to skepticism at
Janssen Pharmaceutica, where other, commercially more attractive research programs
were competing for resources.

A setback, followed by amazing results
The disappointing initial data with mice notwithstanding, Andries and his colleagues
continued with their TB research, and in 2003 they found that R207910 had a unique
spectrum of antibacterial activity. In vitro tests with approximately 20 mycobacte-
ria, including M. tuberculosis and an MDR strain of TB, revealed that the minimum
inhibitory concentration (MIC)14 of ≤0.060 µg/ml, whereas the MIC for non-myco-
bacteria, including H. pylori, was significantly higher (≥32 µg/ml) (Exhibit 3). In the
meantime, scientists in the company’s formulation department solved the solubility
problem by using hydroxypropyl-beta-cyclodextrine, and Andries then tested the
new formulation in a mouse model of TB, with amazing results. When given as a
monotherapy, R207910 was as effective as—or in some cases, better than—rifampicin
monotherapy and the standard triple-cocktail containing the three frontline drugs
rifampicin, isoniazid, and pyrazinamide (Figure 2).
Figure 2. Efficacy of R207910 (bedaquiline; “B”) at reducing the number of bacterial colony forming units (CFU) in the lungs of an established mouse model of TB infection 4 and 8 weeks after infection. For comparison, mice treated with rifampicin alone (“R”) or with a combination of rifampicin, isoniazid (“H”), and pyrazinamide (“Z”) are also plotted. Data courtesy of K. Andries.
14 In microbiology, the minimum inhibitory concentration (MIC) is the lowest concentration of an antimicrobial that will inhibit the visible growth of a microorganism after overnight incubation. MIC is important in diagnostic laboratories to confirm resistance of microorganisms to an antimicrobial agent and to determine the potency of new antimicrobial agents.

Despite their high promise, these remarkable findings from the mouse studies did little
to silence the critics at Janssen Pharmaceutica. The most pressing questions were
related to the projected return on investment (ROI) for a drug that targets a neglected
disease and—perhaps more importantly—regarding the compound’s mechanism of
action (“If you don’t know the mechanism of action, how can you develop it into a
drug?”). Nevertheless, thanks in large part to support from his supervisor, Didier de
Chaffoy, Andries was able to continue working on the TB project. At the time, R207910
was one of the most promising drugs in De Chaffoy’s discovery pipeline. De Chaffoy
had the authority to approve testing through phase I clinical trials (pharmacokinet-
ics studies in human volunteers). He therefore approved preclinical toxicology testing
of R207910 in animals. Unfortunately, these preclinical toxicology studies gave the
Andries team an unexpected setback: at high doses, the drug caused over propor-
tional tissue accumulation, resulting in adverse effects in animals, and phospholip-
idosis15 due to its cationic amphiphilic properties. Although phospholipidosis can
be associated with myopathy and hepatic toxicity, this finding was not a complete
deal-breaker, as several other drugs on the market also cause phospholipidosis; nev-
ertheless, it was still a red flag. Thus, Andries and his team also attempted to create a
compound with better physicochemical properties; however, after considerable effort,
they found that eliminating the lipophilicity also eliminated the compound’s anti-TB
activity. Ultimately, they decided to continue developing the parent compound,
R207910.
Identifying the target and the mechanism of action
To convince his colleagues in the company, and to silence the skeptics, it became
extremely important to identify R207910’s target and its mechanism of action.
Therefore, Andries and his team isolated strains of M. tuberculosis and M. smegmatis
with in vitro resistance to R207910, and their colleagues in the company’s Functional
Genomics department sequenced the complete genomes of these strains for
comparison with their respective wild-type strains; it should be noted that in those
days, whole-genome sequencing was still quite a difficult process. However, their
efforts were rewarded with an interesting result: sequence analysis revealed that only
one bacterial gene—the atpE gene, which encodes the F0 subunit of ATP synthase—
contained mutations in all three mutant strains.
15 Phospholipidosis is a lysosomal storage disorder characterized by the excess accumulation of phos-pholipids in tissues. Many cationic amphiphilic drugs, including anti-depressants, antianginal, antima-larial, and cholesterol-lowering agents, are reported to cause drug-induced phospholipidosis (DIPL) in animals and humans. The mechanisms of DIPL involve trapping or selective uptake of DIPL drugs within the lysosomes and acidic vesicles of affected cells. (Source: Wikipedia)

The identification of these mutations provided compelling evidence that R207910
inhibits the proton pump function of ATP synthase in M. tuberculosis.
Despite this preliminary evidence, more data was needed in order to reach any firm
conclusions and—more importantly—to convince the research field. After all, during
more than four decades of research, no one had ever suggested that ATP synthase
may be a target for antibiotics. To confirm the novel but potentially controversial
finding that the atpE gene was responsible for developing resistance to R207910,
Andries performed complementation studies by transforming wild-type M. smegmatis
bacteria with a plasmid encoding the mutant F0 protein. The transformed cells were
resistant to R207910, and their MIC was identical to the source M. smegmatis strain.
The plasmid was then isolated back from the transformed bacteria, and the team
found that the mutation was retained. These results confirmed that ATP synthase was
the target for R207910. Identifying the compound’s target and its putative mechanism
of action were important achievements, as they increased the team’s likelihood of
securing internal support in order to continue developing the compound and to
publish the data in a top-tier scientific journal.
More—but manageable—complications
During the development process, Andries and his team discovered that R207910 was
subjected to oxidative metabolism primarily by the oxidizing enzyme CYP3A4, causing
the formation of the N-monodesmethyl (M2) metabolite. In mice, 80% of R207910
is converted to the M2 metabolite, which is both less active and more toxic than the
parent compound. The team then measured whether R207910 is metabolized in other
species, including rats, dogs, monkeys, and guinea pigs. In dogs, approximately 50%
of the drug was converted to the M2 metabolite, and was less toxic than in rodents. In
addition, the team found that virtually all (i.e., 99.9%) of the compound was bound to
proteins; thus, the free fraction was unmeasurable. Most PK/PD specialists consider
protein-bound compounds to be inactive, whereas only the free compound has the
desired activity. To get at this issue in further depth, Andries tested the effect of human
proteins on the MIC of R207910; to his surprise, including human proteins increased
the in vitro MIC only a factor of ten.
The metabolic conversion data and the finding that R207910 is almost exclusively
bound to proteins made it difficult to translate their in vitro and animal data to
the clinic. Moreover, it was difficult to establish doses for human volunteers and
patients in phase I and phase IIa studies, respectively. However, these difficulties
were manageable, and doses were determined for the first phase I study, which was
conducted in healthy male volunteers. In this double-blind, randomized,

placebo-controlled study, safety and tolerability were studied using six cohorts
containing nine subjects each. In each cohort, six subjects received the same single
dose of R207910 (10, 30, 100, 300, 450, or 700 mg), and three subjects received a
placebo. In a second trial with a similar design, three cohorts containing nine healthy
male volunteers received escalating doses (50, 150, and 400 mg) of R207910. In
this second study, each subject received either placebo (three subjects per cohort)
or R207910 (six subjects per cohort) for 14 days. Plasma analysis revealed that only
25-30% of R207910 is converted in humans to its main metabolite M2, and the
compound had an “effective half-life” of 24 hours. Importantly, the compound was
tolerated well in all cohorts and caused no consistent trends in the vital signs, electro-
cardiogram, or laboratory tests.
At this stage, Andries now had all the data he needed to write a paper for submission
to a top-tier scientific journal. Specifically, he had a compound from a new chemical
class, a new target with a novel mechanism of action, excellent results using a mouse
model of TB, and promising safety, tolerability, and pharmacokinetics data from two
independent phase I trials with healthy subjects. Thus, Andries and his colleagues
began writing a paper for submission to Science.
A big splash in the TB research community
Andries’ Science paper took everybody in the TB research community by surprise.
This was Andries’ first paper in the field of bacteriology and nobody in the TB
community had ever heard of him. Although he had published in the field of antivirals,
his research group was completely unknown in the TB field. Admittedly, the paper’s
last four authors—Vincent Jarier and Nacer Lounis from Paris, and Emma Huitric and
Sven Hoffner from Sweden—all of them were already established TB experts, but the
authors from Janssen Pharmaceutica, including the first author, were not. Thus, the TB
field was buzzing with excitement: here was the first new TB drug in four decades, with
a novel target and novel mechanism of action, robust activity, and much better than
the first-line TB drugs. Of course, not everyone in the field was convinced. Andries
later heard through other channels that his paper was discussed widely among the
TB research community, and quite a few researchers in the field were skeptical of the
data, even though it was published in Science.

The review by Science
Andries submitted their manuscript to Science in September 2004. Within
just a week, he received their reply. “To our utter surprise, our manuscript
was rejected. We had worked so hard to put together a complete picture.
We could have published a partial picture much earlier, but we wanted
the full story, and we wanted to include not only the drug’s discovery
and mechanism of action, but also some preliminary safety data and
even human pharmacokinetics. And after all that work, the manuscript
was rejected in a week. I asked a member of our company’s Public Rela-
tions department to contact Science and request a teleconference; not
to challenge their decision, of course, as their decision was made and we
respected that, but rather to understand the rationale behind their deci-
sion. Our plan was to submit an improved version to Nature, so it would
have been helpful to know how the paper could be improved. Shortly
after the PR department sent the email, Science replied. They had taken
a second look at our manuscript and said that if we still wanted to publish
in Science, they would send it out for review. Of course, we agreed imme-
diately. It turned out that the manuscript was originally screened by an
assistant editor because the editor was not available. When they received
our follow-up request, the editor evaluated the paper, realized her assis-
tant had been mistaken, and overruled her original decision.
Science sent the manuscript to two reviewers, and both were very posi-
tive. The paper was published, and we even got an image of the ATP syn-
thase on the front cover of the issue in which it was published. This was an
important lesson. If I would not have persist, and if we had not contacted
the journal, the paper would not have been published in Science.
Initially, despite our preliminary evidence, we were not 100% certain that
we had identified the correct target. Therefore, we opted for a cautious
title: ‘R207910 a diarylquinoline active on a potential new target of Myco-
bacterium tuberculosis’. To our surprise, Science changed the title to one

One of the paper’s co-authors was participating in a discussion with colleagues in the
US. The other participants in the discussion did not realize he was actually a co-author
of the paper, and many stated that they did not believe the results. They felt that the
high cLogP suggested that the compound might actually interact nonspecifically with
the bacterial cell wall. Andries had similar experiences when presenting the paper at
conferences; he often found that quite a few audience members did not believe that
ATP synthase was the target. After all, no one had ever heard of an antibiotic that
targets this protein, and ATP synthase is one of the most fundamental enzymes in
biology. Moreover, the F0 subunit—which was specifically implicated in the Science
paper as the target—is highly conserved across species. Skeptics simply did not
believe that it was possible to develop a drug that interacts specifically with ATP
synthase in mycobacteria without cross-reacting with the patient’s own mitochondrial
ATP synthase.
The Science paper included the relevant sequences of human and mycobacterial
ATP synthases as an explanation of R207910’s specificity. Resistant mutants contain
an alanine (A) to proline (P) substitution at amino acid 63 in the F0 subunit of myco-
bacterial ATP synthase. This single change in the protein increased the compound’s
MIC by a factor of a thousand. The importance of an amino acid substitution at this
position is supported by three mycobacterial species that are naturally resistant to
R207910, including M. xenopi (Figure 3). All three R207910-resistant species lack
an alanine residue at this position, and the MIC values are all 1000-fold higher than
R207910-sensitive (i.e., wild-type) M. tuberculosis. The human homolog also lacks an
alanine at this position, which explains why the patient’s ATP synthase is not affected
by R207910. Despite this evidence, and despite the complementation study, many
researchers in the field still refused to believe the bacterial ATP synthase was the
target. Andries explains his feelings at the time: “As scientists, we are trained to believe
the data. When someone sees a computer-generated 3D structure of a drug binding to
its target, they believe it, even though it may be completely inaccurate. We may like to
think we’re objective, but we’re really not.”
that was stronger: ‘A diarylquinoline drug active on the ATP synthase of
Mycobacterium tuberculosis’. Clearly, they found the data from comple-
mentation assay to be quite convincing.”

Figure 3. Amino acid alignment of ATP synthase F0 subunit from wild-type (R207910-sensitive) M. tuberculosis, R207910-resistant M. tuberculosis, M. xenopi, and H. sapiens. (Source: Janssen Pharma-ceutics with minor modifications).
In 2004, just after Andries discovered the drug’s target and mechanism of action,
Anil Koul joined his research group to examine whether R207910 was active against
dormant bacilli. Anil developed an assay in which the bacteria are inverted, with the
synthase target exposed to the outside. Anil was able to show clearly that R207910
binds to wild-type ATP synthase, but not to mutant F0 subunits. These results finally
convinced the skeptics in the TB community that the F0 subunit of mycobacterial ATP
synthase is the target of R207910.
Further discussion regarding the development of R207910
After completing the phase I studies, bedaquiline (the new name for R207910) went
to full development. At the time, two options were available for developing the drug.
The company had a development group based in the US with experience with the
antibiotic levofloxacin (a fluoroquinolone); however, they had no experience with TB.
Alternatively, they could hand the development over to Tibotec (which had already
been acquired by Johnson & Johnson by then), which was an attractive option, given
that they had been so successful at developing anti-HIV compounds. Because of
Andries’ close ties with Tibotec, he wanted bedaquiline to go with Tibotec, although
Tibotec had little experience outside of virology, and their development pipeline was
Mutations and polymorphism in
resistant mycobacteria

rather full with several promising antivirals, three for HIV and two for Hepatitis C (HCV).
Nevertheless, Andries was able to convince both Janssen Pharmaceutica’s upper
management, and clinical development of bedaquiline was transferred to Tibotec in
the summer of 2004 with De Beule appointed as the compound development team
leader. At Tibotec, scientists designed a one-week efficacy study in drug-susceptible
TB (DS-TB) patients to be performed in South Africa as a proof-of-principle study.
Because of his expertise in TB and microbiology in general, Andries stayed with the
compound’s development (which is rather unusual for a discovery scientist), and
became the development team’s Microbiology leader.
Disappointment from the first clinical trial with TB patients
A few months after the paper appeared in Science, the results from the Early Bacteri-
cidal Activity (EBA) phase IIa study became available. Although technically the study
was a success, the data were far from encouraging. In the trial, 75 treatment-naïve
patients with DS-TB were assigned randomly to receive once-daily monotherapy
with oral bedaquiline (25, 100, or 400 mg), 600 mg rifampin, or 300 mg isoniazid
for seven days. The results showed a statistically significant bactericidal effect (0.8
log10) in patients treated with the highest dose of bedaquiline, but only on the last
day of the experimental treatment (day 7). In contrast, the two reference compounds
rifampicin and isoniazid yielded much better results (Figure 4). This outcome was quite
unexpected, given that bedaquiline monotherapy outperformed all three first-line
TB drugs when tested in mice. Thus, the researchers questioned whether the mouse
data provided an accurate prediction of the compound’s therapeutic value in patients.
Also troubling was the finding that the patients who received bedaquiline had a small
increase in corrected QT interval (an increase of approximately 10 msec); which—
although not necessarily a deal-breaker—was certainly a concern.

Figure 4. Time course of bactericidal activity during 7 days of treatment with 25, 100, or 400 mg TMC207 (bedaquiline), 600 mg rifampin, or 300 mg isoniazid. The values are presented at the mean and 95% confidence interval. Log Fall indicates the change in log10 CFU/ml16 in the sputum from baseline (day 0). Note: at day 8 the log10 CFU counts are effected by standard TB treatment, which was initiated at day 8. (Source: Janssen Pharmaceutica).
The final nail in bedaquiline’s coffin
The final blow to the TB program came shortly after the clinical trial, when
management received the follow-up data from the phase I trial with healthy
volunteers. The data showed that bedaquiline had an effective half-life of approx-
imately 24 hours but also an extremely long terminal half-life, approximately five
months (Figure 6). In pharmacokinetics, the rule of thumb is that a compound remains
in the body for five times its terminal half-life, which translates to a retention time
of two years. To the company, this finding was a serious issue because low levels
of bedaquiline could still be measured in the patient’s plasma months after the last
drug intake and potential delayed toxicity could not completely be ruled out at this
point. The company was quite concerned, and upper management terminated the
development of bedaquiline in 2005.
16 In microbiology, colony-forming units (CFUs) are used to estimate the number of viable bacterial or fungal cells in a sample. In this context, viable is defined as the ability to multiply by binary fission under controlled conditions. Unlike most microscopic measures of cell viability, which count both live and dead cells, using CFUs requires culturing the microbes and therefore measures only viable cells.

Figure 5. Plasma levels of bedaquiline (TMC207) measured in healthy volunteers after the last dose. The black dotted horizontal line indicates the No Adverse Effect Level (NOAEL)17 determined in a 6-month study in dogs. At 6 months, the average concentration measured in the volunteers was 157 ng/ml. Effective half-life and terminal half-life are depicted by Eff.t½ and Term.t½ respectively. Data courtesy of K. Andries.
Andries discussed the situation with his colleagues. The decision had been made, and
it was “Game over” for bedaquiline. Nevertheless, some of his colleagues shared his
frustration. Andries explains the struggle he was facing: “Some experts focus so much
on their own specific expertise that they overlook to broader picture and don’t always
distinguish between development of a life-saving drug and development of a lifestyle
drug. TB is a life-threatening disease, and patients with extensive drug-resistant TB
have very limited treatment options and poor outcomes. Most of these patients simply
die. In such case, you must weigh the benefits for the patients against the potential
disadvantages. It’s a classic risk-benefit analysis.”
17 The No Observed Adverse Effect Level (NOAEL) denotes the level of exposure of an organism, found by experiment or observation, at which there is no biologically or statistically significant (e.g. alteration of morphology, functional capacity, growth, development or life span) increase in the frequency or severity of any adverse effects in the exposed population when compared to its appropriate control. In drug development, NOAEL of a new drug is assessed in toxicology experiments using laboratory animals. In pharmacology in addition to the NOAEL, often the Minimal Anticipated Biological Effect Level (MABEL) is determined to establish a safe clinical starting dose in human trials.

We cannot simply let it go!
After much consideration, Andries and colleagues concluded that they could not
simply let the project end. They wanted to resume development and bring this
compound to the clinic. They realized that they were facing huge challenges and
would need to overcome four major hurdles. They would have to convince (i) the
internal pre-clinical toxicology expert committee, (ii) the ‘First in Human’ committee
and (iii) the Clinical Advisory Board with external TB experts. Andries and colleagues
were well aware of the fact that they could not convince these internal committees
merely by making arguments, no matter how sound those arguments might be;
they needed convincing data. Even if they were able to convince the three internal
committees to re-start the development, subsequently they would be facing a though
meeting with the FDA to discuss the development path forward. The challenges were
enormous indeed.
Andries explains: “Looking back, the most important lesson I learned during my career
is that you need to be passionate about your drug; to convince others, you need to
serve as an advocate for the drug, be a ‘champion’ for your product. And in most cases,
people will be convinced only when presented with solid data. Of course, if you’re not
convinced yourself, you’ll never convince others; so you need to generate solid data
first. Once you’ve convinced yourself, you can attempt to convince your colleagues,
their colleagues in the internal committees, followed by upper management, and
finally the regulatory agencies in the countries where the patients are. Throughout the
entire process, you need to push; if you don’t push, you will lose.”

Readings

Before class, please read the following texts:
1. Tibotec - Investigator’s Brochure TMC207 (Bedaquiline), Edition 3, June 2006
and supplement data.
2. Andries K, et al., A Diarylquinoline Drug Active on the ATP Synthase of Myco-
bacterium tuberculosis Science 2005 Jan 14; 307(5707): 223-7. Epub 2004 Dec
9. http://science.sciencemag.org/content/307/5707/223.long
3. Cohen J. New TB drug promises shorter, simpler treatment. Science 10 Dec
2004; 306 (5703): 1872. DOI: 10.1126/science.306.5703.1872. http://science.
sciencemag.org/content/306/5703/1872
4. Cole ST, Alzari PM. TB - A new target, a new drug. Science 14 Jan 2005;
307(5707): 214-215, DOI: 10.1126/science.1108379. http://science.sciencemag.
org/content/307/5707/214
Additional information (Optional)
5. Ridley DB, et al., Developing drug for developing countries. Health Affairs,
2006; 25(2), 313-324. http://content.healthaffairs.org/content/25/2/313.full.
pdf+html
6. If you want to refresh your memory regarding basic pharmacology, you may
wish to look at the Pharmacology tutorials at http://handwrittentutorials.com/
videos.php. This site also contains other tutorials that you may find helpful.
7. In addition, you may wish to look at the Teaching Resource Centre Pharmacol-
ogy (TCR) database at http://coo.lumc.nl/TRC (you can create a free account at
http://www.medicaleducation.nl). You can download the TRC app for free from
the App Store and iTunes.

Exhibit 1. Rejection of the manuscript by Science
6 October 2004
Dr. K. Andries
Johnson & Johnson Pharmaceutical R & D Beerse
BELGIUM Ref: 1105869
Dear Dr. Andries:
Thank you for submitting your manuscript "R207910, a diarylquinoline active on
a potential new target of Mycobacterium tuberculosis" to Science. Because your
manuscript was not given a high priority rating during the initial screening process, we
will not be able to send it out for in-depth review. Although your analysis is interesting,
we feel that the scope and focus of your paper make it more appropriate for a more
specialized journal. We are therefore notifying you so that you can seek publication
elsewhere.
We now receive many more interesting papers than we can publish. We therefore
send for in-depth review only those papers most likely to be ultimately published in
Science. Papers are selected on the basis of discipline, novelty, and general signifi-
cance, in addition to the usual criteria for publication in specialized journals. Therefore,
our decision is not necessarily a reflection of the quality of your research but rather of
our stringent space limitations.
We wish you every success when you submit the paper elsewhere.
Sincerely,
Senior Editor
Science International Bateman House, 82-88 Hills Road, Cambridge CB2 1LQ, UK
Tel: +44 (0) 1223 326 500 Fax: +44 (0) 1223 326 501 Email: [email protected]
Science International is the business name of a U.K. branch of AAAS Science International, a U.S. company.
Corporate Registration No. FC17250 Branch Registration No. BR556 Vat No. 626138545

Ref. 1:
While this is an exciting and important article that merits early publication
in Science, there are certain additions to it that would be helpful. These
are: Some indication of how the molecule was discovered. Clearly, this
was a process that did not start with the mycobacterial genome.
Is there any information on the MIC of M. ulcerans, as the infections with
this organism are currently very difficult to treat?
While much attention is paid to issues of efficacy, less is available on po-
tential toxicity. One needs some reference to screening results for geno-
toxicity and for toxicity tests on the usual two animal species. These
would supplement the rather scanty information from the phase I human
studies. In the description of the results in an established murine infec-
tion (Fig 4b), it would be helpful to note the bacterial load at the time that
treatment was started. This is an indication of the severity of the infection
at that time.
Ref. 2:
This manuscript describes the properties of a diarylquinolone recent-
ly patented and termed R207910 or compound J. This compound has
exquisite selectivity and potency for mycobacterial species, including
M. tuberculosis and the M. avium complex, for which effective drugs are
lacking. Related actinomycetes are only poorly inhibited, while a number
of both Gram-negative and Gram-positive pathogens are essentially un-
affected. The in vitro potency against M. tuberculosis is as good or better
than isoniazid and rifampicin, and the in vivo potency is a log order better
in one mouse model. Perhaps most importantly, the compound retains
activity against M. tuberculosis strains that are singly or multiply resistant
to commonly used anti-tuberculars.
Exhibit 2. Reviewers’ comment Science manuscript

Replacement of either isoniazid, rifampicin or pyrazinamide, a combina-
tion used in all “short course” therapies, with J caused enhanced steril-
ization in an established infection mouse model, arguing that inclusion of
J with one or more of these compounds (the authors correctly argue that
monotherapy would be ill-advised) could potentially further shorten the
course of TB treatment, and be efficacious against strains that were singly
or doubly resistant to isoniazid or rifampicin.
The target for the compound is the proton-translocating F0 subunit of the
ATPase, a novel target that has not previously been the target for anti-
bacterial inhibitor discovery. Strains resistant to J have single amino acid
replacements in this gene, and expression of the gene in multi-copy leads
to resistance. Alignments of the sequence of the gene provide a reason-
able rationale for the selectivity of the compound, and its toxicity profile.
There are numerous other studies reported, including a pharmacokinetic
study and preliminary human tolerance studies, all of which suggest the
compound exhibits desirable properties as an addition to the dwindling
number of effective compounds available to treat TB. As such, and given
the health care crisis as a result of TB-HIV co-infection and rising resis-
tance to extant TB drugs, this is an extraordinarily important study and
series of results of broad interest to the scientific and health care commu-
nity. I personally would be interested in seeing a short paragraph related
to the discovery of the compound class, without the necessity of entering
the patent literature and perhaps structures of other compounds that are
stated as being effective (without a complete SAR1 description). Some of
the detailed pharmacokinetic studies could be included in the supple-
mentary material if space is an issue. Overall, the manuscript is concisely
written and understandable to those outside of the area.
1 The structure–activity relationship (SAR) is the relationship between the chemical or 3D structure of a molecule and its biological activity. The analysis of SAR enables the determination of the chemical groups responsible for evoking a target biological effect in the organism. This allows modification of the effect or the potency of a bioactive compound (typically a drug) by changing its chemical structure. Medical chemists use the techniques of chemical synthesis to insert new chemical groups into the biomedical compound and test the modifications for their biological effects.

Exhibit 3. In vitro activity of bedaquiline against M. tuberculosis, other mycobacteri-
al species, and non-mycobacteria isolates.
OrganismMTB Resistance Subtype N
Bedaquiline MIC (µg/ml)
Range MIC50 MIC90 MIC95
M. tuberculosis All 109 ≤0.008 - 0.12 0.03 0.06 0.06
DS-TB 65 ≤0.008 - 0.12 0.03 0.06 0.06
MDR-TB 44 ≤0.008 - 0.12 0.03 0.06 0.06N = number of isolates; MIC, minimum inhibitory concentration
Table 1. In vitro activity of bedaquiline against M. tuberculosis preclinical isolates. (Source: Janssen Pharmaceutica background document for the FDA’s Advisory Committee meeting)
Mycobacterial species N
Bedaquiline MIC (µg/ml)
Range Median
M. bovis 1 NA 0.003
M. kansasii 1 NA 0.003
M. marinum 1 NA 0.003
M. smegmatis 7 0.003 – 0.010 0.007
M. avium/M. intracellare (MAC) 7 0.003 – 0.010 0.010
M. fortuitum 5 0.007 – 0.010 0.010
M. absessus 1 NA 0.250
M. ulcerans 1 NA 0.500N = number of isolates; MIC, minimum inhibitory concentration; NA, not applicable
Table 2. In vitro activity of bedaquiline against other mycobacterial species. (Source: Janssen Pharma-ceutica background document for the FDA’s Advisory Committee meeting)
Non-mycobacterial organisms N
Bedaquiline MIC (µg/ml)
Range Median
Corynebacterium jeikeium 1 NA 4
Corynebacterium urealyticum 1 NA 4
Helicobacter pylori 20 2 - 4 4
Nocardia asteroids 1 NA >16
Nocardia farcinica 1 NA >16
Escherichia coli 1 NA >32
Haemophilus influenzae 1 NA >32
Streptococcus pneumoniae 10 16 - 32 >32
Staphylococcus aureus 1 NA >32N = number of isolates; MIC, minimum inhibitory concentration; NA, not applicable
Table 3. In vitro activity of bedaquiline against non-mycobacterial isolates. (Source: Janssen Pharma-ceutica background document for the FDA’s Advisory Committee meeting)

On-campusAssignment

You and your group members are co-workers in Andries’ research team. You are
attempting to obtain convincing data that you can present at the meeting with
the three company review committees describe above and upper management
in the hopes that they will reconsider their decision to terminate development of
bedaquiline. Therefore, you will re-evaluate all of the data in the Investigator’s
Brochure and will come up with a solid plan for the restart of the development.
Convincing the internal review committees and upper management will not be an
easy task, given their clear position. Specifically, they concluded that the problems
associated with bedaquiline were serious and further development of the product
for which the company will likely not receive a suitable return on investment would
require strong arguments.
To doYour group will prepare a brief PowerPoint presentation (5 slides
maximum), which will be presented during the meeting with the internal
committees.





























