Embed Size (px)
Citation preview

Case Study #9West Nile Virus
Sara HalasziYoonhee ChoiDaniella Ross
November 15, 2007
(www.geocities.com/.../PagelsTom/02westnile.jpg)

The Case:
In late August 1999, an outbreak of mosquito-borne encephalitis occurs in NY state
August 23, 1999: infectious-disease doctor reports 2 cases of encephalitis in NYC (Queens)
Health Dept. then identifies 6 patients with encephalitis, 5 with extreme muscle weakness requiring respiratory support
First suspected to be St. Louis Encephalitis virus strain Outbreak confirmed as West Nile-like virus based on
identification of the virus in human, avian and mosquito samples.
Increased fatalities observed with NYC birds, especially crows, before and concurrent with this outbreak. . .

West Nile Virus
Family Flaviviridae, genus Flavivirus
First discovered in 1937 Uganda, West Nile region
40-60 nm in diameter Enveloped, icosahedral One molecule of + sense SS
RNA (10,000-11,000 bases) Member of the Japanese
encephalitis virus antigentic complex
Close antigentic relationship with other Flaviviruses (serologic cross-reactions)
www.lib.uiowa.edu/hardin/md/cdc/2290.html

Primary Mode of Transmission Main route of human infection through bites from
infected mosquitoes, mostly Culex species (vector)
Mosquitoes become infected when they feed on infected birds (reservoirs) and carry virus particles in their salivary glands
Corvidae birds (i.e. crows) are especially susceptible to WNV infection
Bird reservoirs sustain infectious viremia after exposure (1-4 days) and if they survive, develop life-long immunity

Primary Modes of Transmission People, horses, and most other mammals are
not known to develop infectious-level viremias very often, and thus are probably "dead-end" or incidental hosts.
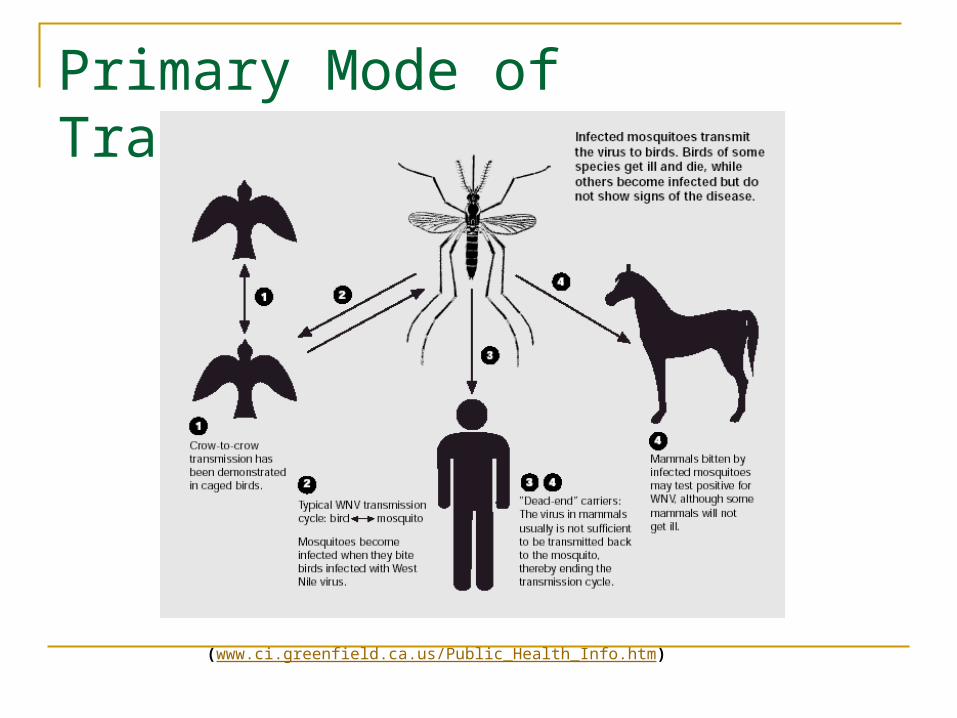
Primary Mode of Transmission
(www.ci.greenfield.ca.us/Public_Health_Info.htm)
Alternate Modes of Transmission WNV is not spread via casual contact, but
can be transmitted (less frequently) by: Organ transplantation Blood transfusion Breast milk and transplacental (mother-child) Occupational exposure (lab accidents)
WNV Infection 2-14 day incubation period ~80% of individuals infected with WNV are asymptomatic ~20% experience flu-like symptoms
(fever, fatigue, headache, muscle and joint pain) >1% experience severe symptoms
(encephalitis, meningitis, profound muscle weakness, high fever, seizures, paralysis)

WNV Infection
60-75% of people with neuroinvasive WNV infections have encephalitis or meningoencephalitis (with most fatalities from encephalitis)
The elderly and immuno-compromised are at a higher risk for developing encephalitis and other severe neuroinvasive infections
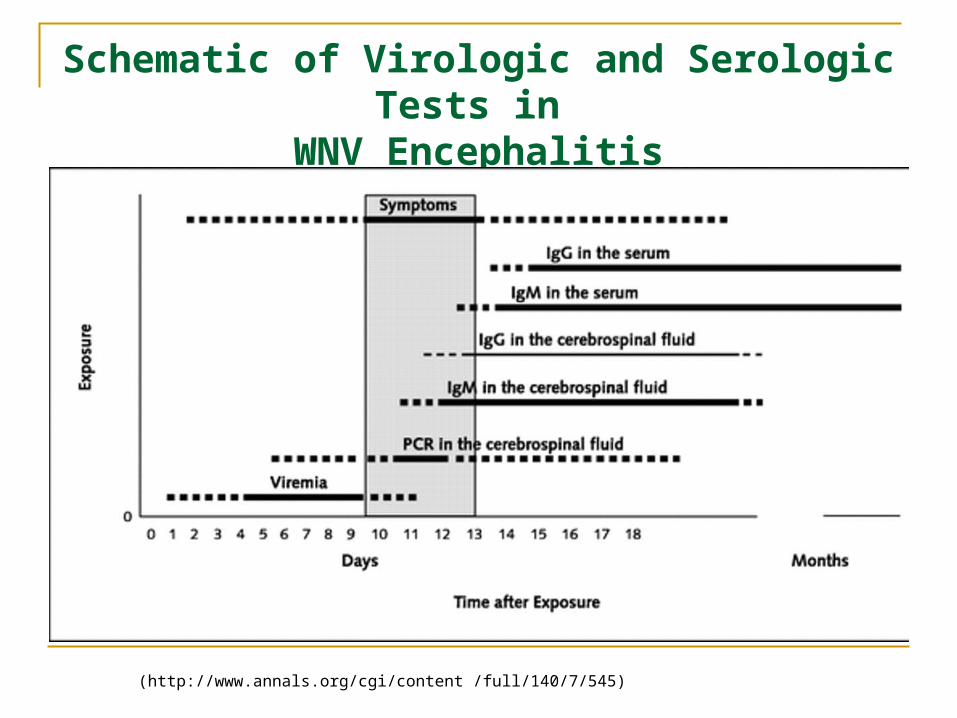
Schematic of Virologic and Serologic Tests in WNV Encephalitis
(http://www.annals.org/cgi/content /full/140/7/545)

Progression of WNVEncephalitis in deep gray nuclei
(http://www.annals.org/cgi/content /full/140/7/545)
WNV Epidemiology
The spread of WNV infection in the U.S. has been very well documented
Excellent case study of how a virus can enter a new territory and spread rapidly through a population. . .
Case figures reflect changes in methods of detection (rise in case number indicative of improved and widespread testing for infection)
WNV Infection Statistics
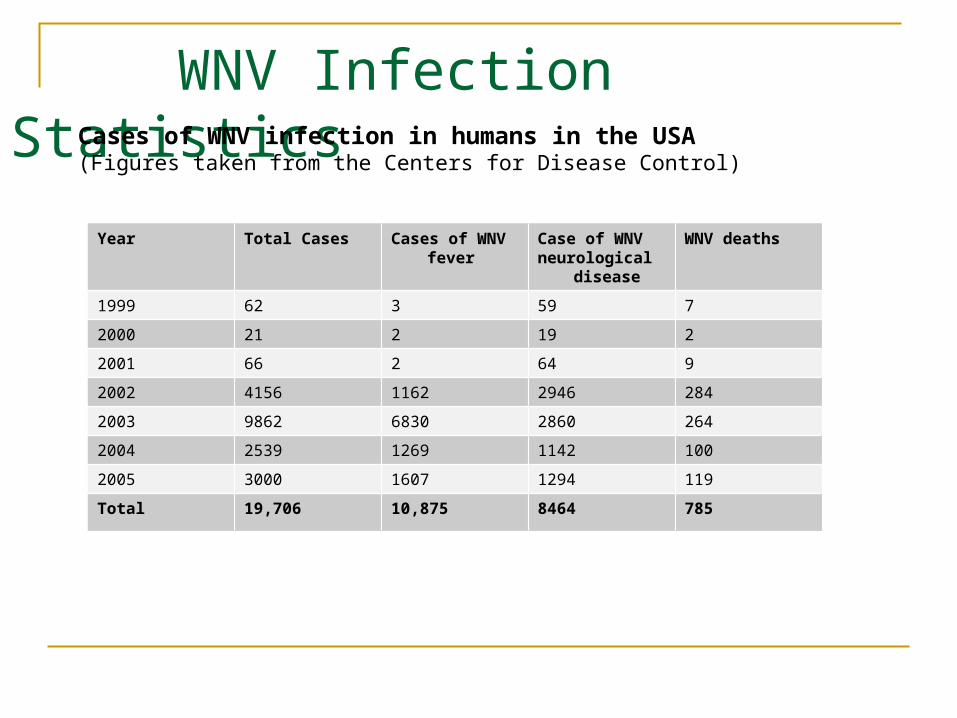
Year Total Cases Cases of WNV fever
Case of WNVneurological
disease
WNV deaths
1999 62 3 59 7
2000 21 2 19 2
2001 66 2 64 9
2002 4156 1162 2946 284
2003 9862 6830 2860 264
2004 2539 1269 1142 100
2005 3000 1607 1294 119
Total 19,706 10,875 8464 785
Cases of WNV infection in humans in the USA (Figures taken from the Centers for Disease Control)
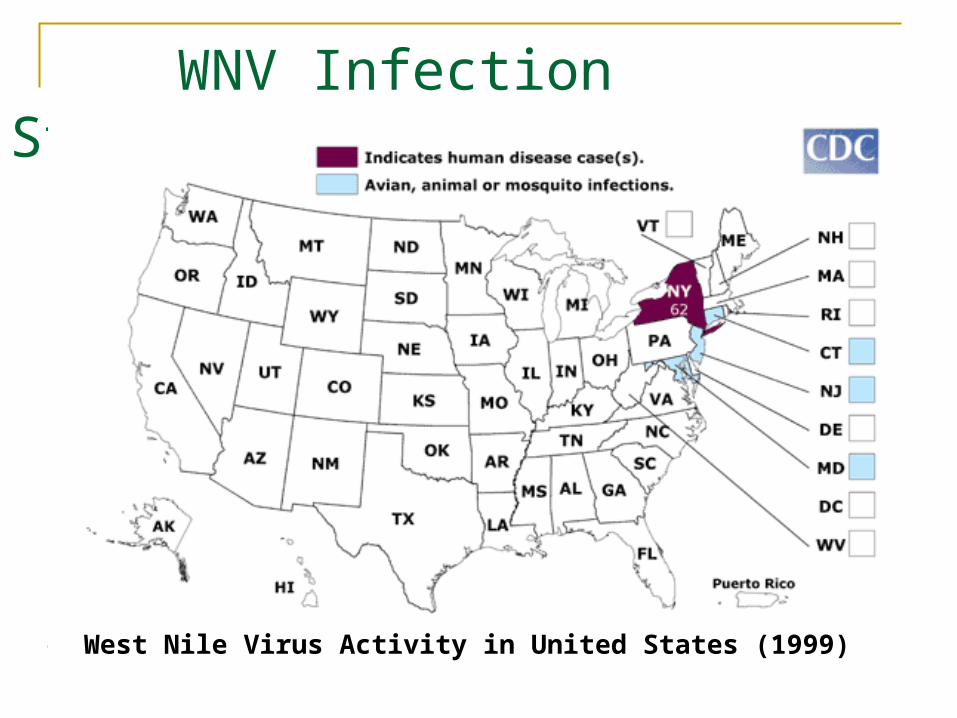
WNV Infection Statistics
West Nile Virus Activity in United States (1999)
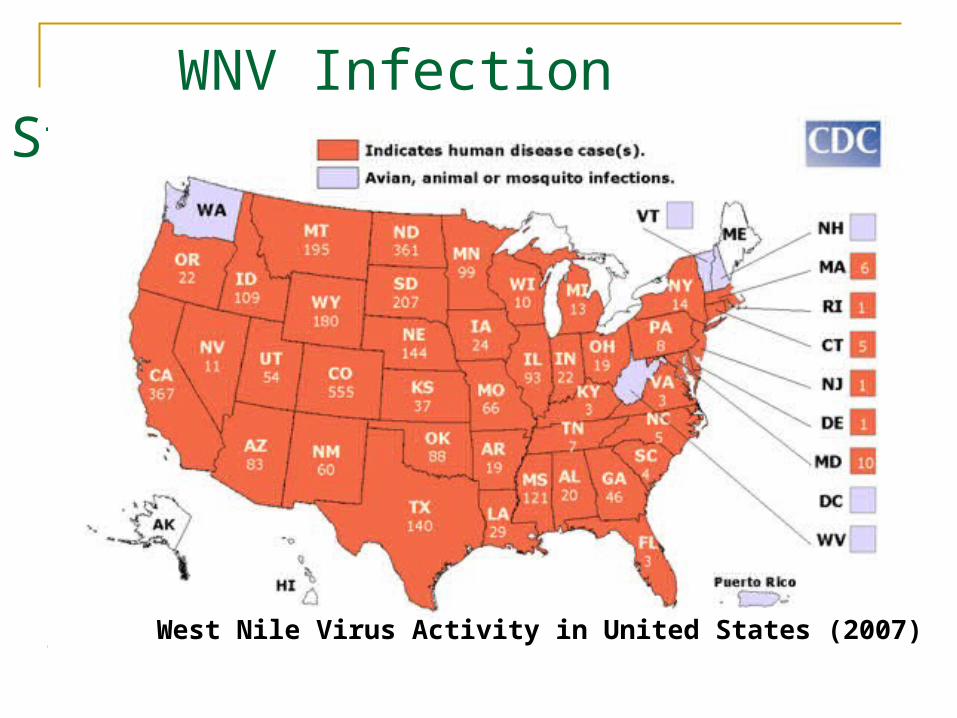
WNV Infection Statistics
West Nile Virus Activity in United States (2007)

Methods for Minimizing WNV Impact Prevention of mosquito bites is the best way to
avoid WNV infectionSome tips: Use insect repellent (i.e. DEET or other EPA
approved insect repellent) Elimination of mosquito breeding sites (standing
pools of water) Use extra caution when out during peak times of
mosquito activity: dawn and dusk, summer months Proper window screens Very careful handling of dead animals (if you must)
Prevention and Treatment of WNV No specific therapies for WNV infection
currently exist Supportive care is generally the only
treatment available (IV fluids, ventilator, prevention of secondary infection)

Prevention and Treatment (cont.) Recombinant vaccine and DNA vaccine
available for equine WNV infection
A horse being vaccinated against West Nile virus. Photo courtesy of CDC.
Vaccines and Antivirals
What about humans?? No antiviral agents or vaccines officially
approved, but research in the field is currently underway. . .
Chimeric vaccines (combination of genes from more than one virus in a single vaccine)
Naked DNA vaccines “cocktail” vaccines (individual WNV proteins)
Vaccines and Antivirals (in development) 1) Acambis vaccine:
(entered human clinical trials in 2006)
combines yellow fever genes and WNV surface proteins.
2) Attenuated dengue virus backbone to carry WNV protective antigens.
3) NIAID/Vical vaccine:
uses an existing codon-modified gene-based DNA plasmid vector to express WNV proteins
Antiviral Peptides Targeting WNV Envelop Protein P1 and P9 inhibited WNV infection in mice
cells Peptides inhibitory effects depend on their
capacity to bind to target E protein P9 binds to WNV E protein and interferes
with virus attachment (concentration dependent)
(Bai, Fengwei et al, “Antiviral Peptides Targeting the West Nile Virus Envelope Protein.” Journal of Virology, Feb. 2007, p. 2047-2055)
Vaccines and Antivirals (in development) Antiviral peptides targeting WNV envelope
proteins Antibodies from individuals who have
recovered from WNV infection Use of animal models to study how prior
infection with related viruses may confer partial or complete immunity will likewise be useful for vaccine research and treatment.