Embed Size (px)
Citation preview

Case Study 56Kenneth Clark, MD

Question 1
• This is a 59-year-old Caucasian woman with a history of granulomatous nephritis (diagnosed 7 years prior), myelodysplastic syndrome, and common variable immunodeficiency with progressively worsening dizziness, blurry vision and headache. Workup at an outside hospital revealed a “sellar mass” along with panhypopituitarism, adrenal insufficiency and hypothyroidism.
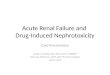
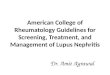
• Describe the MRI findings.

Axial T1 Axial T1 + Contrast
Axial T2 Axial T2 FLAIR

Answer
• Symmetric enlargement of pituitary gland and infundibulum with mild homogeneous enhancement. No areas of T2 or T2 FLAIR signal abnormality are evident.

Question 2
• What is the differential diagnosis of a sellar lesion?

Answer
• Pituitary Adenoma• Craniopharyngioma• Meningioma• Pituitary Carcinoma• Pituicytoma• Oncocytoma• Granular Cell Tumor• Lymphocytic Hypophysitis• Granulomatous Hypophysitis• Metastatic Disease (rare)

Question 3
• What are the common signs and symptoms of sellar lesions (tumors or inflammatory)?

Answer
• Headaches (non-specific)• Double Vision (non-specific)• Loss of Peripheral Vision – Bitemporal
Hemianopsia (non-specific)• Facial Pain and Numbness (non-specific)• Symptoms related to hormonal abnormalities
– lack of energy– weight loss, nausea, vomiting, constipation– amenorrhea and infertility– dry skin, increased pigmentation of the skin– cold intolerance– mental status changes: sleepiness, psychosis

Question 4
• The lesion was resected. Describe the findings.
• Click here to view the slide

Answer
• The tissue shows near complete effacement of pituitary architecture by a rich lymphohistiocytic infiltrate. The histiocytes have large irregularly shaped nuclear with prominent nucleoli and finely distributed pale blue chromatin. The cytoplasmic borders are completely indistinct, resulting in a syncytial appearance of groups of histiocytes. Small numbers of small monomorphic lymphocytes are positioned around the periphery of the histiocyte collections. Small randomly isolated nests of polytypic pituitary cells are seen randomly distributed throughout the specimen.

Question 5
• What is your diagnostic impression?

Answer
• The lesion appears to be inflammatory in nature rich in histiocytes – either infectious or idiopathic in etiology. It does not appear to be neoplastic, although lymphoma cannot be entirely ruled out at this point.

Question 6
• What immunohistochemical and/or special stains would be helpful in confirming your initial impression of this lesion?

Answer• Inflammatory Cell Markers
– CD3 (T-cells)– CD20 (B-cells)– CD68 (macrophages, histiocytes)
• GFAP, IDH1 (to rule out an unusual glial process)• Synaptophysin (to ascertain the pituitary element)• Reticulin (to evaluate residual pituitary
structure/architecture)
• Click to view CD3, CD68, Reticulin

Question 7
• Based on the results of the stains (see below) and H&E slides, what is the general diagnostic category?
• CD3 - highlights numerous small mature lymphocytes• CD20 - very rare positive b-lymphocytes• CD68 - strong staining in numerous histiocytes; highlights ill-defined
granuloma formation• Synaptophysin - positive in sparse scattered small nests of pituitary
cells; highlights architectural distortion by histiocytes• GFAP - rare positive glial cells near periphery of lesion• IDH1 - negative• Reticulin – highlights total effacement of nested pituitary architecture

Answer
• Inflammatory/histiocytic process

Question 8
• What is the differential diagnosis of a non-necrotizing histiocytic / granulomatous process?

Answer
• Neurosarcoidosis
• Infectious (fungal or mycobacterial)
• Langerhans cell histiocytosis
• Erdheim Chester disease
• Rosai-Dorfman disease

Question 9
• What additional stains would you order to better characterize the lesion?

Answer
• Acid Fast, Grocott (rule out infectious process)• CD1A & S100
– Langerhans cell histiocytosis: histiocytes are CD1a and S100 positive
– Erdheim Chester disease: histiocytes are S100 negative (usually) and CD1a negative
– Rosai Dorfman disease: histiocytes are S100 positive and CD1a negative
– Sarcoidosis has similar staining profile of ECD

Question 10
• The results of the additional stains are as follows:– S100: shows sparsely scattered background
folliculo-stellate cells; negative in histiocytes– CD1a: negative– Grocott: negative– Acid Fast: negative
• What is your diagnosis?

Answer
• Non-necrotizing granulomatous hypophysitis, favor neurosarcoidosis

Question 11
• Why favor sarcoidosis when Erdheim Chester disease has a similar histologic appearance and immunohistochemical profile? Explain.

Answer• ECD, which is far more rare than sarcoidosis (300-400
reported cases worldwide), is also called polyostotic sclerosing histiocytosis because it most often involves long bones. Because this patient had a history of non-necrotizing renal granulomas and no bone lesions it is much more likely that this represents sarcoidosis involving the pituitary than ECD. Furthermore, ECD has a progressive and usually fatal course in cases with extra-osseous involvement and is not responsive to steroid therapy; if this patient had ECD at the time of her renal biopsies her clinical course would likely have been much more aggressive and probably fatal. Histologically, ECD lesions often show Touton-like giant cells and are rich in eosinophils – neither of which are seen in this lesion. Considering the clinical AND histopathologic elements of this case, it seems that sarcoidosis is more likely than ECD.

References
• Veyssier-Belot C, Cacoub P, Caparros-Lefebvre D, Wechsler J, Brun B, Remy M, Wallaert B, Petit H, Grimaldi A, Wechsler B, Godeau P (1996) Erdheim–Chester disease. Clinical and Radiologic Characteristics of 59 Cases. Medicine (Baltimore). 75:157–169.
• Louis D, Ohgaki H, Wiestler O, Cavanee W. WHO Classification of Tumours of the Central Nervous System. IARC: Lyon 2007.
• Burns T. Neurosarcoidosis (2003). Arch Neurol. 60:1166-1168.• Rosai J. Rosai and Ackerman’s Surgical Pathology. Elsevier 2004.