Embed Size (px)
Citation preview

2/23/2017
1
CASE STUDIES IN ULTRASOUNDSarah Davis, DNP, ACNP-BC, FNP-BC & Jennifer Wilbeck, DNP, ACNP-BC, FNP-BC, ENP-C, FAANP
Objectives
►At the conclusion of this presentation, learners will be able to demonstrate the use of bedside ultrasound for the :— Assessment & management of shock
— Assessment & management of abscess
— Assessment & management of endocarditis
— Procedure of joint injections
— EXTRA: Assessment & management of abdominal, bony & extremity pain

2/23/2017
2
Bedside Ultrasound in Emergency Care
►Enhances diagnosis, resuscitation, monitoring, & treatment of acute conditions at bedside
►Guides procedural techniques
►Incredibly operator dependent
Commonly Used Transducers
https://upload.wikimedia.org/wikipedia/commons/b/b7/UsMachTxPhoto.jpg

2/23/2017
3
Ultrasound 101: Review
►Correct— Transducer
— Marker Positioning
— Depth
— Gain
— Positioning (the provider and the pt)
►Echogenicity
ASSESSMENT OF SHOCK
Insert Photo/Illustration credits here

2/23/2017
4
TYPES OF SHOCK
►Hypovolemic►Obstructive►Cardiogenic►Distributive
—Neurogenic —Anaphylactic—Septic
Inadequate tissue perfusion and cellular hypoxia are present in
every type of shock
Overall Goals of Shock Management
►Provide supportive therapy to affected body systems WHILE finding, managing, and treating the shock source
►IV access, central preferred

2/23/2017
5
Rapid Ultrasound in Shock Protocol (RUSH)
►Used in undifferentiated shock for rapid eval of reversible causes
►Improves accurate diagnosis in undifferentiated hypotension
►Utilizes 3-part bedside assessment— The pump
— The tank
— The pipes
►Always start with heart and IVC/IJ veins, then tailor clinically
Seif, D., Perea, P., Mailhot, T., Riley, D., & Mandavia, D. Bedside Ultrasound in Resuscitation & the Rapid Ultrasound in Shock Protocol (2012). Critical Care Research & Practice
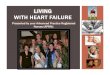
RUSH Protocol Summary
Taken directly from: Seif, D., Perea, P., Mailhot, T., Riley, D., & Mandavia, D. Bedside Ultrasound in Resuscitation & the Rapid Ultrasound in Shock Protocol (2012). Critical Care Research & Practice. Available at https://www.hindawi.com/journals/ccrp/2012/503254/abs/

2/23/2017
6
https://i1.wp.com/emcrit.org/wp-content/uploads/2011/03/RUSH-ED-sequencing-2017-01-30.jpg
HYPOVOLEMIC SHOCK

2/23/2017
7
Hypovolemic Shock
► Loss or redistribution of volume (blood, plasma, or other body fluids) which result in decreased intravascular volume
► Signs and symptoms noticeable when intravascular volume reduced by >15%
► Inadequate preload — Decreased diastolic filling
— Decreased cardiac output

2/23/2017
8
Hypovolemic Shock Causes
►Acute blood loss or ongoing hemorrhage
►Fluid depletion (Non-hemorrhagic)
►Gastrointestinal (Vomiting/diarrhea)
►Burns
►Polyuria
►Aggressive pharmaceutical diuresis
►Insensible losses

2/23/2017
9
Classes of Hemorrhagic Shock
Assessment: Inferior Vena Cava (IVC) Evaluation
►Vena cava is a collapsible vein— Not affected by vasoconstriction— Changes in size based on intravascular volume
►Evaluated by ECHO— Size (<1.2 cm)— Respiratory variation (>50% collapse with inspiration)
►More accurate indicator of potential volume responsiveness than CVP

2/23/2017
10

2/23/2017
11
Hypovolemic Shock Treatment
►Appropriate/meaningful volume resuscitation— Crystalloid boluses with ongoing infusion— Blood product administration
►CAUTIOUS use of vasopressors— Fill before you squeeze!
►Optimized oxygen delivery
►Treatment of underlying hypovolemic cause

2/23/2017
12
OBSTRUCTIVE SHOCK
Obstructive Shock
►Mechanical obstruction impacting the cardiovascular system that decreases ventricular filling and/or emptying
►End result is decreased cardiac output, decreased tissue perfusion, and oxygen delivery

2/23/2017
13
Obstructive Shock Causes
► Decreased ventricular filling— Cardiac tamponade
— Tension pneumothorax
— Vena cava compression or thrombus
— Atrial mass or thrombus
►Decreased ventricular emptying— Pulmonary embolism
https://upload.wikimedia.org/wikipedia/commons/2/2f/Pneumothorax_CXR.jpg

2/23/2017
14
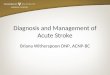
Pneumothorax
►Free air in the pleural space
►Can be Primary or Secondary— Spontaneous: No evidence of lung dz.— Secondary: Lung disease comorbidity
►Tension PTX must be ruled out!— Decreased in venous return to R heart— Decreased CO— Mediastinal shift
Pneumothorax

2/23/2017
15
Lung sliding or no lung sliding?

2/23/2017
16
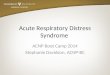
Simple Pneumothorax
CXR should be Upright,
end-expiration
Tension Pneumothorax
►Hypotension
►Tachycardia
►Diaphoresis
►Cardiovascular Collapse
►Tracheal Deviation

2/23/2017
17
Management: Needle Thoracostomy
https://65.media.tumblr.com/tumblr_lv49d27nwn1qafl51o1_500.jpg
►Use with unstable patient with Tension PTX
►14-18G angio, 2nd ICS MCL OR 4th-5th ICS, Anterior axillary line
►Need long enough catheter
Hemothorax
►Blood in intrapleural space
►Lung can hold up to 2L blood
►No sxs with small amount— 200 mL to be seen on CXR
►Large HTX (> 1L) = Shocky

2/23/2017
18
Obstructive Shock Management
►Rapid treatment of the cause
►Gentle volume and vasopressor use— Temporizing measure only
►Airway stabilization
https://upload.wikimedia.org/wikipedia/commons/9/9f/Blausen_0164_CardiacTamponade_02.png
CARDIOGENIC SHOCK
Insert Photo/Illustration credits here

2/23/2017
19
Cardiogenic Shock
► Occurs when the heart fails as a pump
► Decreased contractility leads to decreased stroke volume
► Leads to decreased cardiac output and blood pressure, resulting in decreased tissue perfusion
Cardiogenic Shock Causes
►Myocardial infarction
►HFrEF exacerbation
— Ischemic
— Non‐ischemic
►Dysrhythmias
►Left ventricular outflow tract obstruction
— Hypertrophic obstructive cardiomyopathy

2/23/2017
20
Cardiogenic Shock Treatment
►Myocardial infarction— Restoration of coronary artery perfusion
— Anticoagulation, angioplasty, stent, and/or CABG
►HFrEF— Address underlying cause
— Inotropic support, afterload reduction, diuresis
►Dysrhythmias— Antiarrhythmic drugs, DCCV, and/or defibrillation

2/23/2017
21
DISTRIBUTIVE SHOCK
Sepsis and Septic Shock►Sepsis: Infection + ≥ 2 SIRS criteria
►Severe Sepsis: Sepsis plus at least one sign of hypoperfusion or organ dysfunction that is new and not explained and/or a serum lactate level >4.0 mmol/L
►Septic Shock: Severe sepsis associated with refractory hypotension (BP<90/60) despite adequate fluid resuscitation and/or a serum lactate level >4.0 mmol/L

2/23/2017
22
Photo credit: http://www.traumayellow.com/uploads/2/0/9/5/20955098/4670173_orig.png; for more information, see http://www.qsofa.org/index.php#whatis
Goal Directed: Septic Shock Treatment (Part 1)Within 3 hours of presentation:►Measure lactate level
►Obtain cultures before antibiotics: — Two sets of blood cultures— +/- urine culture
►Administer broad spectrum antibiotics
►Administer 30ml/kg crystalloid for hypotension or lactate ≥4mmol/L

2/23/2017
23
Sub Xiphoid View

2/23/2017
24
Goal Directed: Septic Shock Treatment (Part 2)
Within 6 hours of presentation:
►Apply vasopressors (for hypotension that does not respond to initial fluid resuscitation) to maintain a mean arterial pressure (MAP) ≥65mmHg
►In the event of persistent hypotension after initial fluid administration (MAP < 65 mm Hg) or if initial lactate was ≥4 mmol/L, re-assess volume status and tissue perfusion
►Re-measure lactate if initial lactate elevated
Serial Ultrasound in Fluid Management

2/23/2017
25
2 hours later….
Same Patient

2/23/2017
26
Septic Shock: Treatment Updates
►Fluids (Crystalloids; albumin if needed)
►Vasopressors— Norepinephrine, epinephrine, vasopressin
►Inotropes if cardiac dysfunction— Dobutamine
►Corticosteroids— ONLY if unable to meet hemodynamic goals
Concluding Points about Shock…
►Shock states are dynamic— Stay vigilant
►Managing shock is a collaborative effort— Utilize your team

2/23/2017
27
ASSESSMENT OF ABSCESSES
Insert Photo/Illustration credits here
Bedside US for Evaluation of Abscesses (soft-tissues)
►Used when physical exam unclear— Assists with identifying location, size & composition
— Differentiate cellulitis vs. abscess
— Especially useful in highly vascular areas—Doppler color settings can identify arteries

2/23/2017
28
Key Assessments in Abscesses (soft-tissues)
►High-frequency linear array or convex array transducer— Convex for deeper fluid collections
— High-frequency linear in peds for smaller footprint
►Use 2 planes to evaluate shape & depth of fluid collections
►Increase gain to visualize subtle details of water content in subcuttissues
Key Assessments in Abscesses (soft-tissues)
Cellulitis Subcutaneous Abscess
Increased distance between the skin & underlying fascia or bone
Organized collection of pus & debris in sharply demarcated area
Increased echogenicity of subcut tissue w/ hypoechoic bands causing cobblestone appearance
Most commonly, hypoechoic roughly spherical mass
+/- Postereior acoustic enhancement and/ormotion of fluid-filled area with palpation
Campo & Lafferty. Essential Procedures for Emergency, Urgent, & Primary Care settings (2nd edition), 228-9.

2/23/2017
29
MANAGEMENT OF ABSCESSES
Insert Photo/Illustration credits here
Overall Management of Abscess
►http://sonoguide.com/abscess.html
►http://emedicine.medscape.com/article/1379916-overview
►http://lbstack.com/US%20Handouts/Soft%20tissue%20handout.pdf

2/23/2017
30
Peritonsillar Abscesses Management
https://upload.wikimedia.org/wikipedia/commons/3/39/PeritonsilarAbsess.jpg
►Airway, pain management, antibiotics— Augmentin or Clinda
►+/- steroids
►Drainage of fluid collection— I&D
— Needle drainage
Ludwig’s Angina
►AIRWAY, vascular access, & broad spectrum antibiotics
►Ultrasound may detect:— Gas in tissues, abscesses & LAD
— Locate airway among edematous anterior neck tissue
— Guide fluid aspirations

2/23/2017
31
ASSESSMENT OF ENDOCARDITIS
Insert Photo/Illustration credits here
Endocarditis must be considered in patients presenting with fever and
stroke-like symptoms

2/23/2017
32
MANAGEMENT OF ENDOCARDITIS
Insert Photo/Illustration credits here
Endocarditis Management
►Ultrasound is an additional tool to assess if there is an effusion in the setting of pericarditis
►Antibiotic therapy— Native vs. prosthetic valves
— Also consider IVDA or congenital anomaly
— Multi-drug therapies
►Surgical intervention may be required

2/23/2017
33
JOINT INJECTIONS
Insert Photo/Illustration credits here

2/23/2017
34
Indications for Joint injections
►Arthrocentesis— Diagnostic— Therapeutic
►Therapeutic Joint injections
►US guidance shown to improve intra-articular needle position, improving outcomes
https://stemcelldoc.files.wordpress.com/2011/11/ultrasound-guided-injection.jpg
EXTRA CASES…
Insert Photo/Illustration credits here

2/23/2017
35
ABDOMINAL PAIN
Insert Photo/Illustration credits here
Pleural Effusions

2/23/2017
36
BONY PAIN
Insert Photo/Illustration credits here
Conclusion
►Ultrasound gaining increased utility in the ED/urgent care settings
►Utility for assessment, management & monitoring of patients
►Highly user-dependent — Practice
— Certification opportunities