Embed Size (px)
Citation preview

Case RoundsLaura Miles
Teams Case RoundsFebruary 10 2012

Case 1Case 1

ObjectivesObjectives Develop a differential diagnosis for chest
pain
Review the common causes of chest pain in children and adolescents
Recognize ‘red flags’ needing further investigation
Go through cardiac causes of chest pain

16 yo old male
Admitted to emerg with crushing chest pain

HistoryHistory Several months of intermittent CP
CP occurs for 5-10 minutes at a time
No relieving factors
No obvious aggravating factors
Occasionally feels lightheaded with chest pain
Several ?syncopal episodes

More HistoryMore History Chest pain is worse in left anterior chest but
does radiate across both sides
Usually 8-10/10 pain
No respiratory symptoms
No association with eating
No history of trauma

Past Medical HistoryPast Medical History No major medical illnesses
Immunizations probably up to date (he thinks)
No known allergies
No regular medications

Social HxSocial Hx Smoker – ½ ppd
Hx of drug use – cocaine, ecstasy, marijuana etc. Denies recent use
Currently living with Aunt – mom unable to care for him

Ddx?Ddx? MSK
Respiratory
GI
Cardiac

Red FlagsRed Flags Syncope
Family Hx Need to ask specifically about sudden deaths Include unexplained drownings, single vehicle
collisions
Exercise induced

MSKMSK Chest wall pain accounts for over 30% of
pediatric chest pain
Can be muscular, bony or involving connective tissue
Can be traumatic or atraumatic
Costochondritis – usually related to traumatic strain
Precordial catch – short duration, unclear etiology

RespiratoryRespiratory Significant proportion of
children/adolescents presenting with chest pain actually have uncontrolled asthma Dyspnea Cough Pneumothorax
Pneumonia
PE

GIGI Hx of chest pain worsening after meals can
be very suspicious for reflux
Peptic ulcer disease

PsychogenicPsychogenic History can be key

CardiacCardiac Arrhythmias
SVT VT
Coronary Arteries Kawasaki disease Anomalous origin of coronary artery
compression between aortic and pulmonary roots
Myocardial Myocarditis Cardiomyopathy

Cardiac continuedCardiac continued Aortic
Dissection associated with connective tissue disease
Pericardial Acute pericarditis
Valvular Severe aortic or subaortic obstruction
Limited cardiac output during exercise Severe mitral regurgitation
Volume overload of the left ventricle and increased myocardial work

Back to our patient…Back to our patient… Any further history you want?

Physical ExamPhysical Exam

Ix?Ix? Normal CBC and extended electrolytes
Troponins normal x 3
Urine tox screen positive only for cannabis

ECGECG

Ok, so for those of you who know the case, that wasn’t his actual ECG…

The conclusions…The conclusions… Despite some abnormal findings on his
actual ECG his chest pain was thought to be psychosomatic
Chest pain in retrospect could be brought on by stress
Chest pain would improve as he was able to calm himself down

Case 2Case 2

ObjectivesObjectives To recognize some of the more common
arrhythmias and their ECG pattern and symptoms
To develop an approach and differential diagnosis to an uncommon arrhythmogenic presentation

16 year old male
Seen in peripheral hospital for palpitations, chest pain and feeling generally unwell
You are called by the emerg doc at the peripheral site who is looking for advice

What do you want to What do you want to know?know?
Had been playing hockey
Initially felt unwell and had to leave the ice and sit down
Developed chest pain, some shortness of breath and noticed his heart was ‘beating funny’
Chest pain was predominantly on the left side
Stabbing pain 8/10

Hx continuedHx continued Feeling lightheaded, worse with standing

HR 200
RR 30
BP 85/40
O2 sats 95% on room air

Looks very pale and overall unwell
Well hydrated
Pulses slightly weak
CRT 3-4 seconds peripherally
Cardiac exam: normal S1,split S2 no murmur
Quiet precordium
Respiratory exam clear
Normal abdominal exam

What should I do??What should I do??

IV access and started fluid bolus
ECG – ‘looks like SVT’
Drawing up medication – but chest pain and increased HR spontaneously stop

What’s going on?What’s going on?

SVTSVT Paroxysmal supraventricular tachycardia
Narrow complex tachycardia originating above the ventricular tissue
Accessory pathway
Sudden onset and usually sudden cessation

Diagnosing SVTDiagnosing SVT ECG during event
Palpitation diary – teach parents or patient how to count a HR and record HR during events
Event Recorder

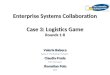
SVT ECGSVT ECG

SVT ManagementSVT Management Initially – vagal maneuvers
Beta blockers
Ablation

SVT in infants…SVT in infants… Need to be especially careful in this
population
Because infants can’t tell you about a racing heart, they can go into heart failure if not discovered early
Teach parents how to count HR

Repeat ECGRepeat ECG

Wolff Parkinson WhiteWolff Parkinson White ‘Preexcitation’ a portion of the ventricle is
being activated ahead of schedule
Can present with AV Reentry tachycardia
At risk for antegrade conduction Can consider ablation in certain cases

Your patient finally Your patient finally arrives…arrives…
HR 100
RR 20
BP 100/60
Sats 100 % on room air
CRT improved – 2 seconds peripherally
Looks much better than previously advertised

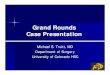
ECGECG

Ventricular Ventricular TachycardiaTachycardia
Incidence of ventricular ectopy 0.5% in infants up to 18-50% in adolescents
Differential diagnosis includes SVT with aberrancy, antidromic reciprocating tachycardia (AV reentry with atrial to ventricular conduction)
Classified as VT once you have at least 3 ventricular ectopic beats in a row

Ventricular Ventricular TachycardiaTachycardia
Most commonly seen after repair or palliation of congenital cardiac lesions
Cardiomyopathy
Channelopathies Long QT Brugada syndrome
Abnormal coronary artery placement

Ventricular Ventricular TachycardiaTachycardia
Idiopathic – often has absent symptoms
Arrhythmogenic right ventricular dysplasia RV dilatation Myocardial thinning Fatty replacement of the myocardium Familial inheritance Increased risk of sudden death
Cardiac tumours

Ventricular Ventricular TachycardiaTachycardia
Catecholamine related polymorphic VT Occurs with emotion or stress Often results in syncope Can degenerate into V fib Tx with beta blockers to prevent recurrent
episodes ICD in refractory cases

Management of VTManagement of VT Unstable: synchronised cardioversion
Antiarrhythmic medication for asymptomatic/stable patients Amiodarone
Torsade de pointes – magnesium
Cardiology referral
Further testing – echo, MRI, stress testing

Thanks!Thanks!
Any questions?