Embed Size (px)
Citation preview

Case Review Course
5th session – July 31, 2013
In the name of God
By Mohammad Reza Emami

Review the List of GI disorders
Evaluation of a case
Approach to the patient
with dysphagia
Discussing differential diagnoses
Review some mini-
cases
1 2 3 4 6Symptoms
of Gastrointestinal Diseases
Agenda
5

Esophageal disorders :
I. Gastroesophageal Reflux Disease (GERD)
II. Barrett’s Esophagus
III. Hiatal hernia
IV. Rings and Webs
V. Esophageal diverticulum
VI. Achalasia
VII. Diffuse Esophageal Spasm (DES)
VIII. Esophagitis
• Infectious esophagitis
• Non-infectious esophagitis
1- Review the list of GI disorders

Stomach disorders :
I. Peptic Ulcer Disease (PUD)
II. Zollinger-Ellison Syndrome (ZES)
III. Gastritis
IV. Ménétrier's disease
1- Review the list of GI disorders (continue)

Nutritional and malabsorption disorders :
I. Celiac disease
II. Tropical sprue
III. Short Bowel Syndrome
IV. Bacterial Overgrowth Syndrome (BOS)
V. Food allergies
VI. Lactose intolerance
VII. Irritable Bowel Syndrome (IBS)
VIII. Whipple’s disease
IX. Protein-Losing Enteropathy
1- Review the list of GI disorders (continue)

Gastroenteritis :
I. Bacterial gastroenteritis
II. Viral gastroenteritis
III. Parasitic gastroenteritis
1- Review the list of GI disorders (continue)

Inflammatory intestinal disorders :
I. Inflammatory Bowel Disease (IBD)
• Ulcerative Colitis
• Crohn’s Disease
II. Microscopic colitis
1- Review the list of GI disorders (continue)

Anorectal disorders :
I. Diverticular disease
• Diverticulosis
• Diverticulitis
II. Procidentia
III. Fecal incontinence
IV. Hemorrhoidal disease
V. Anorectal abcess
VI. Anal fistule
VII. Anal fissure
1- Review the list of GI disorders (continue)

GI Neoplasms :
I. Esophageal cancer
II. Gastric cancer
III. Small intestine tumors
IV. Colorectal cancer
V. Anal cancer
1- Review the list of GI disorders (continue)

The most common GI symptoms are:
abdominal pain, heartburn, nausea and
vomiting, altered bowel habits, GI bleeding,
and jaundice.
Others are:
dysphagia, anorexia, weight loss, fatigue,
and extraintestinal symptoms.
2- Symptoms of Gastrointestinal Diseases
See Table 1

A 43-year old man has persistent dysphagia following cancer of the right buccal space. To treat the cancer, he had radiation therapy and neck dissection. He currently exhibits pharyngeal dysphagia, aspiration, hoarse vocal quality, and right lower facial weakness. He currently receives nutrition through a NG-tube.
3- Approach to the patient with dysphagia
What would be your next measure ?

3- Approach to the patient with dysphagia (continue)

A 64-year-old white woman with a history of breast cancer
treated with lumpectomy and radiation, hypertension, high
cholesterol, and ovarian polyps presents to her primary care
physician complaining of difficulty and pain with swallowing,
as well as occasional chest pain. She indicates that her
problem started with liquids, but has progressed to solids, and
that the food “just gets stuck in my throat.” The chest pain
was once so bad that she took one of her husband’s
nitroglycerin pills and the pain subsided, but it has since
occurred many times. The physician orders an x-ray of the
chest, but it is not diagnostic. Manometry is conducted, and it
shows uncoordinated contractions.
What is the most likely diagnosis?
4- Evaluation of a case

5- Discussing differential diagnoses
A. Breast cancer relapse
B. Diffuse esophageal spasm
C. Esophageal cancer
D. Myocardial infarction
E. Nutcracker esophagus

Answer A is incorrect. Although this patient
has had cancer in the past, she does not seem
to be suffering from it again. Her symptoms
do not indicate any such etiology.
5- Discussing differential diagnoses (continue)
A. Breast cancer relapse×

The correct answer is B. Spasms of the esophagus are characterized by problems with both solids and liquids, causing odynophagia and dysphagia, as well as noncardiac angina. Globus pharyngeus, or the feeling of food stuck in one’s throat, is also very common. Nitroglycerin may actually confuse the diagnosis because it acts to relax the smooth muscle, thereby relieving the pain. X-rays may be helpful in diagnosis by showing what is known as a corkscrew formation of the esophagus. The anatomy of the esophagus may be divided into three parts, and when these three do not contract in a uniform manner as with spasms, then a food bolus may become trapped and cause pain. Manometry establishes the diagnosis by showing these uncoordinated contractions.
B. Diffuse esophageal spasm
5- Discussing differential diagnoses (continue)

Answer C is incorrect. Usually, cancer will cause
dysphagia only for solids and may not cause the
pain this patient is experiencing unless it has
spread beyond the walls of the esophagus.
5- Discussing differential diagnoses (continue)
C. Esophageal cancer×

Answer D is incorrect. A myocardial infarction will
not present with the given history of
progressive dysphagia. Remember that chest pain
does not always translate into a cardiac etiology.
5- Discussing differential diagnoses (continue)
D. Myocardial infarction×

Answer E is incorrect. Very similar to spasms, nutcracker
esophagus differs in the fact that it is characterized by
continuous, coordinated contractions on
manometry. This difference is important with treatment
because spasms may ultimately be treated with a
myotomy, while nutcracker cannot.
5- Discussing differential diagnoses (continue)
E. Nutcracker esophagus×
See more information about “Nutcracker esophagus”

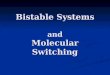
1- Diffuse Esophageal Spasm (DES)
4- Achalasia
2- Esophageal stricture
3- Esophageal cancer
Figure 1,2,3,4 – Esophageal disorders

6- Review some mini-cases
1 2
3 4

6- Review some mini-cases (continue)
1Presentation DDx Workup
34 yo F presents with retrosternal stabbing chest pain that improves when she leans forward and worsens with deep inspiration. She had a URI one week ago.
• Pericarditis• Aortic dissection• MI• Costochondritis• GERD• Esophageal
rupture
• ECG• CPK-MB, troponin• CXR• Echocardiography• CBC• Upper endoscopy

6- Review some mini-cases (continue)
2Presentation DDx Workup
30 yo F presents with alternating constipation and diarrhea and abdominal pain that is relieved by defecation. She has no nausea, vomiting, weight loss, or blood in her stool.
• IBS• IBD• Celiac disease• Chronic
pancreatitis• GI parasitic
infection• Lactose
intolerance
• Rectal exam, stool for occult blood
• CBC• Electrolytes• Stool for ova and
parasitology• AXR• CT –
abdomen/pelvis

6- Review some mini-cases (continue)
3Presentation DDx Workup
58 yo M presents with pleuritic chest pain, fever, chills, and cough with purulent yellow sputum. He is a heavy smoker with COPD.
• Pneumonia• Bronchitis• Lung abcess• Lung cancer• TB• Pericarditis
• CBC• Sputum Gram
stain and culture• CXR• CT – chest • ECG• PPD

6- Review some mini-cases (continue)
4Presentation DDx Workup
45 yo diabetic F presents with dysuria, urinary frequency, fever, chills, and nausea over the past three days. There is left CVA tenderness on exam.
• Acute pyelonephritis
• Nephrolithiasis• Renal Cell
Carcinoma (RCC)• Lower UTI
• UA• Urine culture and
sensitivity• CBC, BUN/Cr• U/S – renal • CT – abdomen

Esophageal chest pain
Cardiac chest painvs.
• non-exertional
• prolonged
• interrupts sleep.
• is meal-related.
• is relieved with antacids.
• is accompanied by heartburn,
dysphagia, or regurgitation.
• is not influenced by changes in
body position.
• lasts for only an hour or less.
• may sometimes radiate down the
left arm, across the left shoulder
and upper back, or up to the neck
and to the lower jaw.
• is accompanied by anxiety,
profuse sweating, nausea and
vomiting, shortness of breath,
and fainting.
• is not exacerbated by respiration.

Thank you
“That which does not kill us makes us stronger.”Friedrich Nietzsche