Embed Size (px)
Citation preview

CASE REVIEW
Clinical diagnosis and management strategiesof amelogenesis imperfecta variants
W. Kim Seow BDS, MDSc, DDSc, PhD, FRACDS
AbstractAmelogenesis imperfecta (AI) is a group of inherited disorders primarily affecting dental enamel. Variants of AI generally
are classified as hypoplastic, hypocalcified, or hypomaturation types based on the primary enamel defect. The aim of this studywas to analyze the clinical presentations, diagnostic features, and clinical complications of different variants of AI. Thirty-twopatients from 17families with several subtypes of AI were studied. The results showed that distinctive clinical features may beobserved in each variant. However, all AI patients suffered common clinical problems of poor esthetics, teeth sensitivity, andloss of occlusal vertical dimension. The mildest problems were found in the pitted hypoplastic type whereas the most severeproblems were encountered in the hypocalcified type of AI. Management strategies include composite resin veneers and jacketcrowns for anterior teeth as well as steel crowns for posterior teeth. Knowledge of the clinical features and dental complicationsof each variant of AI helps in the diagnosis of the condition and allows institution of early preventive measures. (Pediatr Dent15:384-93, 1993)
IntroductionThe term "amelogenesis imperfecta" (AI) now
reserved for those developmental enamel defects in-herited primarily as defects of the enamel only. 1 Theprevalence of this condition has been estimated to rangefrom I in 7182t0 1 in 14,000,3 depending on the popula-tion studied. The etiology of AI is thought to be alter-ation of the genes involved in complex processes ofenamel formation and maturation.
A few classifications of AI, based on clinical appear-ance of the defects as well as the inheritance patternshave been proposed in the past,1,4,5 the most recent andcomprehensive being suggested by Witkop1 (Table 1).In general, the defects in AI may be classified as hypo- Type I
plastic, hypocalcified, or hypomaturation types, de- IAIB
pending on the stage of enamel formation that is pri- ICmarily affected.1 The hypoplastic types are characterized IDby a deficiency in the quantity of enamel, which may be IEexpressed clinically as thin enamel or pits or grooves IFon the enamel surface.1,4,s By contrast, the hypocalcified IGvarieties are characterized by enamel that is insuffi-ciently mineralized, and appear clinically as soft, dis- Type I!
colored enamel that is easily removed.~, 4. s The IIA
hypomaturation types of AI are associated with abnor-IIB
malities of the maturation stages of enamel formation, IICresulting in the enamel being opaque and chalky inappearance2,4,~ As shown in Table 1, autosomal domi- Type IIInant, autosomal recessive, and X-linked modes of in- IliA
heritance have been reported. IIIB
Although recent research has made significant ad- Type IVvances into the diagnosis of a few types of AI by mo-lecular~and biochemicalgmethods, these sophisticated IVAtechniques are not yet routinely available. Currently,diagnosis of the different AI variants rests mainly on IVBthe dental clinical presentations and their modes of
inheritance as determined from family pedigrees. Ac-curate diagnosis is clinically important for several rea-sons. First, it is important to exclude the presence ofcertain systemic diseases that may show generalizedenamel hypoplasia as accompanying signs.1°-14 Second,accurate diagnosis enables genetic counselling,~5 whichis often sought by affected families. Third, accuratediagnosis leads to the recognition of clinical problemsthat are associated with the condition, so preventivemeasures may be instituted early. Fourth, diagnostic
Table 1. Classification of amelogenesis imperfecta accordingto Witkop (1989)
Hypoplastichypoplastic, pitted autosomal dominanthypoplastic, local autosomal dominanthypoplastic, local autosomal recessivehypoplastic, smooth autosomal dominanthypoplastic, smooth Xqinked dominanthypoplastic, rough autosomal dominantenamel agenesis, autosomal recessive
Hypomaturationhypomaturation, pigmented autosomalrecessivehypomaturation, X-linked recessivesnow-capped teeth, autosomal dominant?
Hypocalcifiedautosomal dominantautosomal recessive
Hypomaturation-hypoplastic withtaurodontismhypomaturation-hypoplastic withtaurodontism, autosomal dominanthypoplastic-hypomaturation withtaurodontism, autosomal dominant
384 Pediatric Dentistry: November/December 1993 - Volume 15, Number 6

differentiation of the many variants of AI may help todetermine the type of restorations 16-19 that are mostsuccessful.
Although the genetic defects in the X-linked form ofAI now have been linked to amelogenin genes on the X-chromosome,6~ the molecular defects associated withthe other types of AI are still unclear. Hence, the diag-nosis of AI currently rests largely on clinical criteria.
With the exception of a few epidemiological investi-gations,3, 20, 2~ previous studies of AI have been mainlycase reports of individuals or small numbers of fami-lies.22-3s
The aim of the present study was to analyze theclinical presentations and dental complications in agroup of affected patients to determine the distinctclinical features of each variant.
Patients and methods
The study subjects were all referred to the authorover the past few years for dental management ofenamel hypoplasia, and diagnosed as having AI by theauthor. A total of 32 subjects (16 males and 16 females)from 17 different, unrelated families were available forstudy. At the time of initial dental examination, theirmean age was 12.8 + 5.6 years (range 7.2-34.5 years).
All the patients were examined at the University ofQueensland Dental School. The teeth were dried, and amirror and probe used for the dental examination.Erythrosin disclosing dyes were painted on the enamelof some patients to demonstrate the surface defects.Bite-wing and panorex radiographs were exposed aspart of their routine dental management. The results ofthe dental examinations were recorded in comprehen-sive charts.
Table 2. Characteristics of families with the hypoplastic variants of amelogenesis imperfectaFamily Hypoplastic Likely Clinical Problems
Variant Mode of Clinical Features Poor Sensitivity Loss ofInheritance Esthetics of teeth OVD
1 Pitted AD Small discrete pits on all surfaces. + 0 0Normal contact between teeth. Normalradiographic contrast of enamel and dentin.
As above. +
As above. Extensive loss of enamel on +occlusal of primary molars.
Thin, smooth, hard, glossy enamel. ++White to yellow-brown in color. No contactbetween teeth. Radiographs show thin enamel.
As above. No contact between teeth. ++Radiographs show thin layer of enamel.
Females show vertical bands of alternating +++normal thick, and abnormal thin enamel inboth primary and permanent dentitions.
Females show above. Males shows uniformly +++thin, smooth enamel.
All females show above. +++
In addition to above, one male shows ++anterior open bite.
10 Rough AD Thin, hard enamel with rough surfaces. ++ 0Minimal contact between teeth. Radiographsshow thin enamel.
As above. Primary dentition shows thin, ++less rough enamel.
Horizontal pits and grooves of missing enamel ++in the middle third of the crowns of allpermanent teeth. The enamel present showshypomaturation defects.
2 Pitted AD 0 0
3 Pitted AD + +
4 Smooth AD ++ +
5 Smooth AD + +
6 Smooth XL 0 0
7 Smooth XL
8 Smooth XL
9 Smooth XL
11 Rough AD
12 Local AR
++ ++(Males) (Males)
0 0
+ +
0 0
+ 0
AD = autosomal dominant; AR = autosomal recessive; XL = X-linked; OVD = occlusal vertical dimension; + = mildly affected;++ = moderately affected; +++ = severely affected.
Pediatric Dentistry: November/December 1993 - Volume 15, Number 6 385

Table 3. Characteristics of families with the hypocalcified and hypomaturation variants of amelogenesis imperfecta
Likely _____Clinical ProblemsFamily Mode of
InheritanceClinical Features Esthetics
AffectedSensitivity
of TeethLoss ofOVD
Hypocalcification
14
15
16
Hypomaturation
17
AR/XL Enamel appears soft, opaque white-yellowupon eruption. Early loss of enamel. Minimalcontact between teeth. Radiographs showenamel loss and lack of contrast betweenenamel and dentin.
AD As above.
AR/XL As above.
XL/AR Thin enamel with mottled opaque-whitediscoloration. Enamel may chip away.Normal contact between teeth. Radiographsshow thin enamel and less contrast betweenenamel and dentin. Mild anterior open bitepresent.
AD = autosomal dominant; AR = autosomal recessive; XL = X-linked; OVD = occlusal vertical dimension; + = mildly affected;++ = moderately affected; +++ = severely affected.
For every proband, a family pedigree chart was con-structed. In an affected family, examination of as manyfamily members as possible was performed. Dentalmanagement outcomes are not part of the study de-sign.
Diagnosis of amelogenesis imperfectaA diagnosis of Al was based on the following crite-
ria: 1) generalized enamel hypoplasia of both the pri-mary and permanent dentition; 2) family history of thecondition, although in the recessive forms, or newmutations, there may be no previous history; 3) ab-sence of systemic diseases that may cause generalizedenamel hypoplasia resembling Al (e.g. systemic disor-ders involving calcium metabolism such as renal andliver disorders).10-11
In addition, the trichodentoosseous (TOO) syndrome(kinky hair, dysplastic nails, sclerotic bones, enamelhypoplasia, severe taurodontism),39"41 which showshypocalcification enamel defects, was excluded.13 Vari-ants of ectodermal dysplasia, which may also showgeneralized enamel hypoplasia,12-42 as well as fluorosis43
also were excluded.
ResultsTables 2 and 3 show the 17 families in the study, and
the type of variant diagnosed in each case. Twelvefamilies showed the hypoplastic variety. Three of thesewere classified further as having the pitted hypoplastictype, another seven, the smooth hypoplastic type, andtwo, the rough hypoplastic type. In addition, one fam-ily showed the local hypoplastic variety.
There were three families with the hypocalcificationtype of Al, and another one that showed thehypomaturation variety.
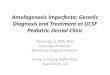
Pitted hypoplastic Al (autosomal dominant)Clinical features. Five affected children from the
three families with the pitted type of Al (Table 2) allshowed classical features of small, discrete, pinpoint-to-pinhead sized pits, which were arranged in horizon-tal or vertical rows (Fig la). In areas of the teeth sub-jected to occlusal stresses, there were localized areas ofenamel loss. Contacts between the teeth were normal.
Defects in the primary dentition in this form of Almay be demonstrated in an affected female child fromfamily #3 (Fig lb). The defects in the thinner enamel of
Fig 1 a. Permanent teeth of a male patient from family #1 withthe pitted type of Al.
386 Pediatric Dentistry: November/December 1993 - Volume 15, Number 6

Fig 1 b. Anterior teeth of patient from family #2 stained witherythrosin dye. The surface pits may occur in vertical rows asshown on the labial surfaces of the primary lateral incisors.
Fig 2a. Dentition of a male patient (family #12) affected withthe local hypoplastic type of Al. Restorations had been placedpreviously on the labial surfaces of the maxillary centralincisors.
Fig 2b. Bite-wing radiographs of the patient depicted in Fig 5a,showing bulbous appearance of the crowns and constrictedcervical areas due to lack of enamel at these areas of thecrowns. There is also complete coronal pulp calcification.
primary teeth may be less conspicuous compared withthe permanent dentition. In this patient, staining theteeth with erythrosin-disclosing dye clearly demon-strated the pitted hypoplastic defects.
Radiographs of affected teeth in the pitted type of Alshowed normal enamel thickness and normal contrastbetween enamel and dentin.
In all the families, autosomal dominant modes ofinheritance were demonstrated.
Clinical problems. Minor esthetic problems wereencountered in two patients who showed mild stain-ing of the enamel pits. Except for one patient who hadextensive loss of enamel of her primary teeth, nonecomplained of sensitivity. There was also little poten-tial for loss of occlusal height. Mild gingivitis was notedin many patients.
Local hypoplastic Al (autosomal recessive)
Clinical features. One male patient presented withthe local hypoplastic type of Al (Family #12, Table 2).All his permanent teeth showed hypoplastic defectsthat occurred as horizontal bands of pitted or missingenamel (Fig 2a). In the entire dentition, the enamelappeared opaque. Radiographs revealed normal enamelthickness (Fig 2b). Of interest is the complete calcifica-tion of the coronal parts of the pulp chambers, as wellas the bulbous appearance and constricted cervices ofthe crowns, which may be related to the lack of enamelat the cervical areas (Fig 2b).
As there was no history of the condition in othermembers of the family, it was postulated that the modeof transmission was autosomal recessive or X-linkedrecessive. Alternatively, it may represent a new geneticmutation in the family.
Clinical problems. The patient complained of pooresthetics and some sensitivity to hot and cold. Therewas little potential for loss of occlusal vertical height,and minimal gingivitis.
Fig 3a. Dentition of patient from family #4 affected with thesmooth thin hypoplastic type of Al.
Fig 3b. Bite-wing radiographs of patient in Fig 2a, showing thinenamel and spacing between the teeth.
Pediatric Dentistry: November/December 1993 - Volume 15, Number 6 387

Fig 4a. Mixed dentition of a female patient(family #6) affected by the smoothhypoplastic (X-linked) type of Al showingthe classical vertical striping effect ofalternating bands of normal and affectedenamel.
Fig 4b. Permanent dentition of an affectedfemale patient from family #8 (X-linkedsmooth hypoplastic Al) clearly depicting thevertical striping effect on the facial surfacesof the entire dentition.
Fig 4c. Dentition of mother of proband infamily #7 affected by the X-linked smoothhypoplastic type of Al. Note the mild verticalridging of the enamel surface.
Smooth, thin hypoplastic Al (autosomal dominant)
Clinical features. Seven patients from three fami-lies with the autosomal dominant type of smooth hy-poplastic type of Al were available for examination(Table 2). All the patients showed thin, hard, smooth,and glossy enamel, which varied in color from white tocream-brown (Fig 3a). The teeth appeared narrow in alldimensions and there were no contacts between theteeth. Radiographs of the affected patients showed athin layer of enamel outlining the crowns (Fig 3b).
In the three families studied, autosomal dominantpatterns of inheritance were observed. This variant maybe distinguished from the smooth, hypoplastic X-linkeddominant type by the fact that in the autosomal domi-nant variant, both sexes are affected equally to thesame extent, whereas in the X-linked type, males areaffected more severely.
Clinical problems. All affected patients with thesmooth hypoplastic Al complained of poor esthetics aswell as moderate dental sensitivity. Enamel loss onocclusal surfaces in the older, untreated patients wassevere, leading to potential problems of loss of verticaldimension. Gingival health in this group of patientsappeared better compared with the rough hypoplastictypes, most probably due to the enamel surfaces beingrelatively smooth.
Smooth hypoplastic Al(X-linked)
Clinical features. A total ofseven affected females and twomales from four separate fami-lies were diagnosed as havingthe X-linked type of hypoplas-tic Al (Table 2). In this variant,the affected females classicallyshowed alternating verticalbands of normal and hypoplas-tic enamel (Fig 4a), an effectknown as Lyonization,15-16 whichmay be seen in X-linked condi-tions. The expression of theenamel defect in vertical ridgesand grooves was seen also in theprimary dentition although theeffects may not be as pro-nounced. Radiographs of the af-fected females revealed theenamel to be thin. Contacts be-tween the teeth may vary, de-pending on severity of the de-fect. In two of the families (#6and #8), the expression in thefemales was severe (Figs 4a, 4b).However, in the other two fami-lies (#7 and #9), only faint verti-cal ridging of enamel was notedin the mother (Fig 4c) and ma-ternal grandmother of the male
proband, indicating that in this family, the femaleswere affected only to a mild degree. The teeth hadnormal contacts and the radiographs showed only mildthinning of the enamel.
By contrast, the enamel defects in affected males infamilies #7 and #9 were severe, and manifested asuniformly thin and smooth enamel (Fig 4d). Further-more, the teeth appeared small and no contacts existedbetween the teeth. In addition, radiographic appear-ance of the teeth in affected males usually showed theenamel to be extremely thin or nonexistent.
The classical differences in clinical manifestationsbetween the sexes, as well as the family pedigrees,indicated that in these families the most likely mode ofinheritance was X-linked. For example, in family #6, anaffected father has transmitted the condition to all ofhis daughters and none of his sons. By contrast, anaffected mother may transmit the condition to half herdaughters and half her sons.
Clinical problems. Poor dental esthetics was suf-fered by all male and female patients who showedextensive vertical grooving of the enamel. However,females tended to complain less of dental sensitivityand suffered less dental destruction and loss of occlusalvertical dimension. Most affected patients showed se-vere gingival inflammation.
Fig 4d. Early mixed dentition of maleproband in family #9 showing uniformlythin enamel surface, in direct contrast to thevertically ridged enamel seen in his mother(Fig 4c).
388 Pediatric Dentistry: November/December 1993 - Volume 15, Number 6

Fig 5. Dentition of an affected female from family #11 withhypoplastic type of Al showing thin, rough enamel.
Rough hypoplastic Al (autosomal dominant)
Clinical features. Two families (#10 and #11, Table2) presented with the autosomal dominant, rough hy-poplastic type of Al. In this variant, both sexes areaffected to the same degree and presented with similarfeatures of thin, hard, rough-appearing enamel (Fig 5).There were minimal contacts between the teeth, andradiographs revealed thin enamel that had normal ra-diographic contrast with dentin.
In the primary dentitions of the study patients, thedefects were not as obvious as in the permanent denti-tion, particularly in the anterior teeth. However, in theposterior primary teeth, moderate loss of tooth struc-ture and dental caries were noted on the occlusal sur-faces. In all the three families showing this type of Al,the most likely mode of inheritance was autosomaldominant.
Clinical problems. Poor dental esthetics resultingfrom stained and rough teeth was the chief complaintof most patients. Sensitivity of the teeth, as well as lossof occlusal vertical dimension, were not as great as thehypocalcified types. Severe gingivitis was noted in mostpatients.
Hvpomaturation Al (autosomal recessive/X-lmkecl recessive)
Clinical features. A male patient (family #17, Table3) presented with the hypomaturation-type Al. Heshowed typical features of opaque white enamel withareas of hypoplasia in the entire permanent dentition(Fig 6). There were normal contacts between the teeth.A mild anterior open bite was present. Radiographsrevealed lack of contrast between enamel and dentin,although the enamel thickness appeared normal. Sincethe appearance of the enamel defects was similar todental fluorosis, this possibility was excluded fromhistory, as well as the radiographic appearance ofenamel.
The patient appeared to be the only affected mem-ber of his family. Thus the mode of inheritance may bepostulated to be either autosomal recessive or X-linkedrecessive or a new genetic mutation in the family.
Clinical problems. Dental esthetics of the patientwas only mildly affected. There was no sensitivity ofthe teeth, and little potential for loss of occlusal verticaldimension through loss of tooth structure.
Fig 6. Dentition of a male patient (family #17) affected by thehypomaturation type of Al. Note similar appearance of teethto dental fluorosis.
Fig 7. Primary dentition of patient with the hypocalcified Al(autosomal dominant) showing total loss of enamel on maxillaryanterior teeth and opaque discoloration of remaining enamelon other teeth.
Hypocalcified Al (autosomal recessive/autosomal dominant)
Clinical features. Three families (#14-#16, Table 3)presented with the hypocalcification-hypoplastic typeof Al. In all affected members of families snowing thisvariant of Al, the enamel typically appeared soft,opaque, and yellow-white upon eruption (Fig 7). Ittended to chip away easily, particularly on the facialsurfaces, exposing large areas of dentin. There wereadequate contacts between the teeth. The primary den-tition appeared as severely affected as the permanentdentition with large areas of enamel missing from mostof the primary teeth.
Radiographically, in all cases, there was minimalcontrast between enamel and dentin, and the enamelthickness ranged from normal to thin.
Pediatric Dentistry: November/December 1993 - Volume 15, Number 6 389

In one of the families (#15, Table 3)with this type of Al, an autosomal domi-nant mode of inheritance was evident.However, in the two remaining families(#14 and #16, Table 1), the proband ineach case was male and there were noprevious histories of the condition in thefamilies. It may be postulated that in eachof these cases, an autosomal recessive, oran X-linked recessive mode of inheritanceor a new genetic mutation is possible.
Clinical problems. All affected pa-
Fig 8a, 8b. Anterior teeth of patient presenting with the rough, hypoplasticAl(left) successfully restored with composite resin facings (right).
tients complained of extremely poor dental estheticsand moderate levels of sensitivity to hot and cold. Inthe older, untreated patients, there was excessive lossof occlusal vertical height. Also, it was noted thatmargins around previous amalgam restorations weredefective due to the fracture of supporting tooth struc-ture.
Discussion
Diagnostic difficultiesSince the current classifications of Al variants are
based mainly on clinical presentations and patterns ofinheritance of relatively few patients, revision may benecessary as new knowledge becomes available. Thecurrent classification systems dividing the enamel de-fects into hypoplastic, hypocalcified, andhypomaturation types may cause difficulties in identi-fying some variants that simultaneously show clinicalfeatures of two or more groups (e.g., hypoplasia isoften noted in the hypocalcified groups). Overlappingfeatures also have been identified bothmicromorphologically18~20-22 and microradiologically.44-45 Some Al variants such as the pitted hypoplastic typeare clinically distinctive and easily diagnosed. Otherssuch as the X-linked variants may be more difficult todiagnose due to their presentations in a few pheno-types, as well as the existence of striking differences inexpression between males and females.
In addition, the unavailability of dental data fromcertain family members, as well as incompleteness ofpedigrees, may compromise accurate diagnosis in manyAl patients. Furthermore, the modes of inheritance inmany small families may be difficult to determine, par-ticularly in the recessive types. Also, in many variantsof Al, such as the X-linked varieties, the modes of in-heritance are still not clearly established.46-47
Management of oral complications
The families in this study represented the hypoplas-tic subtypes IA, IC-IF, hypomaturation subtype IIB,and hypocalcification subtypes IIIA and HIB in Witkop'sclassification1 (Table 1). The relative prevalence of eachtype is comparable to those found in previous reports.2-4 In addition to delineating further the distinctive phe-notypic features of Al variants, this study compared
the different complications that may be encountered ineach type. This may have value in planning effectivepreventive and restorative strategies for managing eachvariant.
In this study, it was found that the main clinicalproblems of Al in general were esthetics, dental sensi-tivity, and loss of occlusal vertical dimensions throughloss of dental structure. The severity of dental prob-lems experienced by the patients, however, varied witheach type of AL The hypoplastic variants tended to beassociated with less severe clinical problems, with themildest problems encountered in the pitted hypoplas-tic type of Al. By contrast, the patients with thehypocalcified type of Al usually presented with themost severe clinical problems.
Poor dental esthetics. Poor dental esthetics in Alwas usually the result of surface roughness, staining,and abnormal crown shapes from enamel loss. Severalstrategies may be used to overcome the compromisedesthetics. In the patients with hypoplastic types of Al,there is usually sufficient enamel available for bondingso that composite resins veneers may be used to maskthe staining and improve the crown morphology (Fig8a, 8b). However, in patients affected by thehypocalcified varieties of Al, enamel is usually insuffi-cient for direct bonding, and dentin bonding resins23 orglass ionomer cements34 are first required to bond tothe underlying dentin before applying the veneer ofcomposite resins. Other anterior veneers using porce-lain are also likely to be useful, particularly if sufficientenamel is available for bonding; however, their use inAl teeth has not been evaluated.
Porcelain jacket crowns, which provide esthetic per-manent restorations, are probably the restoration ofchoice for Al and have been reported to be successful inaffected adults,19 but their use in young patients usu-ally is contraindicated due to the presence of largepulps.
In the primary dentition, anterior primary teeth maybe restored with strip crowns, using glass ionomercements as an intermediary material underneath thecomposite resin veneers. Alternatively, anterior stain-less steel crowns with composite resin facings havebeen tried successfully.48
Dental sensitivity. Sensitivity of the teeth to hot
390 Pediatric Dentistry: November/December 1993 - Volume 15, Number 6

Fig 9a, 9b. Hypoplastic primary molars of a patient with the pitted variant of Al(left), successfully restored with stainless steel crowns (right).
and cold is a common complaint of patients with Al.The severest problems are encountered in the variantspresenting with the least amount of enamel, such as thehypocalcified and the smooth and thin hypoplastictypes. In the young permanent dentition, as well as theprimary dentition, the most effective method to man-age dental sensitivity is full coronal coverage usingstainless steel crowns in the posterior teeth (Fig 9).
In constructing steel crowns, a conservative tech-nique of tooth separation using separating elastics priorto the insertion of the crowns is recommended.49'50 Thistechnique, which obviates the need for proximal re-duction of tooth structure, allows the stainless steelcrowns to be inserted with minimal tooth reduction.
Furthermore, glass ionomer cements are likely to bebetter luting agents for the crowns compared with zincphosphate if there are large areas of exposed dentin.
Dental caries and intracoronal restorations. Al-though a few studies have suggested that patients withAl have less dental caries20 due to a lack of proximalcontacts and elimination of fissures through enamelloss, it is equally likely that in many forms of Al, therough enamel surfaces predispose to increased plaqueretention and greater caries susceptibility. Furthermore,the loss of enamel and the presence of large areas ofexposed dentin also may increase caries. Therefore,caries-preventive measures such as frequent topicalapplications and dietary control are strongly recom-mended for all Al patients.
Except for mildly affected teeth, intracoronal resto-rations with amalgam are usually unsuccessful due tofracture of the weak enamel margins. In this study, itwas found that for small restorations, adherent materi-als such as glass ionomer cements and composite res-ins17 are better retained compared to amalgam restora-tions. However, in most cases, full coverage is requiredfor posterior teeth due to extensive enamel loss, as wellas for the prevention of further loss of tooth structure.In the primary and early mixed dentition, stainlesssteel crowns are effective restorations.
Anterior open bite. Alteration of the occlusal verti-cal dimensions may occur in Al. Anterior open bite hasbeen associated in Al, particularly in the hypocalcifiedtypes,20'21/ 51~53 although its etiology remains unclear.Theories include the suggestion that it has resulted
from abnormal tongue positioningcaused by teeth sensitivity as well as thepossibility that the anterior open bite is afeature of the Al syndrome.52-53 What-ever its cause, the open bite often is diffi-cult to treat. Types of corrective treat-ment that have been suggested rangefrom routine orthodontic banding47 toorthognathic surgery,46 all with varyingdegrees of success.
In contrast to anterior open bite, col-lapse of the posterior occlusal segments,
leading to deep anterior overbite also has been reportedin some types of AL2-20-3a 35 In this study, the patientsmost predisposed to this problem belonged to thehypocalcified Al group (Table 3). In addition, affectedmale patients of the X-linked type of Al, as well as allpatients with the smooth hypoplastic type of Al alsodemonstrated this propensity. Loss of occlusal verticaldimension is best prevented as early as possible, pref-erably in the primary dentition by fabricating posteriorsteel crowns.50 In the case of patients who have lostextensive interocclusal height, rehabilitation may beachieved by posterior full crowns and/or by overlaydentures.30'35
Gingival inflammation. All Al patients are predis-posed to poor gingival health. There is enhanced plaqueretention and calculus formation resulting from therough enamel surfaces, which may extendsubgingivally. Increased preventive oral health prac-tices as well as frequent professional prophylaxis forman important component of management strategies forthese patients.
Other clinical problems that have been reported pre-viously in Al include delayed eruption and/or toothimpaction.23 This problem was noted in only one malepatient in this study who had the hypocalcified type ofAL Resorption of unerupted teeth also has been re-ported previously,33 but was not noted in this patientseries.
Future studiesFuture research into several aspects of Al are re-
quired to improve the understanding of this condition.Molecular studies of the genetic aspects of the diseasewould provide important insight into its pathogenesis.Comparative biochemical, clinical, and electron micro-scopic studies of affected teeth from different variantsof Al would lead to better understanding of the differ-ences in defects found in each type. Furthermore, whileprevious prevalence studies have provided useful in-formation, further epidemiological studies of otherpopulations/racial groups are necessary. In these stud-ies, improved diagnostic criteria based on current un-derstanding of the phenotypic expressions of the dif-ferent variants may provide more accurate figures ofprevalence.
Pediatric Dentistry: November/December 1993 - Volume 15, Number 6 391

In conclusion, this clinical study has provided fur-
ther insight into the diagnostic features and clinicalcomplications of the different AI variants. Accurate
diagnosis and appreciation of associated clinical prob-lems in each case enable the institution of early preven-
tive measures and management techniques using amultidisciplinary approach.
Dr. Seow is associate professor in Pediatric Dentistry, Dental School,University of Queensland, Australia, and visiting professor, HarvardSchool of Dental Medicine and Children’s Hospital, Boston, Mass.
1. Witkop CJ Jr: Amelogenesis imperfecta, dentinogenesisimperfecta and dentin dysplasia revisited: problems in classifi-cation. J Oral Pathol 17:547-53, 1988.
2. B~ckman B, Holm AK: Amelogenesis imperfecta: prevalenceand incidence in a northern Swedish county. Community DentOral Epidemiol 14:43-47, 1986.
3. Witkop CJ Jr, Sauk JJ Jr: Heritable defects of enamel. In OralFacial Genetics, Stewart RE, Prescott GH (eds), St Louis: Mosby Co., 1976, pp 151-226.
4. Sundell S, Valentin J: Hereditary aspects and classification ofhereditary amelogenesis imperfecta. Community Dent OralEpidemiol 14:211-16, 1986.
5. Shields ED: A new classification of heritable human enameldefects and a discussion of dentin defects. Birth Defects 19:107-27, 1983.
6. Lagerstrom M, Dahl N, Nakahori Y, Nakagome Y, Backman B,Landegren U, Pettersson U: A deletion in the amelogenin gene(AMG) causes X-linked amelogenesis imperfecta (AIH1).Genomics 10:971-75, 199l.
7. Lau EC, Slavkin HC, Snead ML: Analysis of human enamelgenes: Insights into genetic disorders of enamel. Cleft Palate J27:121-30, 1990.
8. Salido EC, Yen PH, Koprivnikar K, Yu LC, Shapiro LJ: Thehuman enamel protein gene amelogenin is expressed fromboth the X and Y chromosomes. Am J Hum Genet 50:303-316,1992.
9. Wright JT, Butler WT: Alteration of enamel proteins inhypomaturation amelogenesis imperfecta. J Dent Res 68:1328-30, 1989.
10. Seow WK: Enamel hypoplasia in the primary dentition: a re-view. ASDC ] Dent Child 58:441-52, 1991.
11. Lubinsky M, Angle C, Marsh, PW, Witkop CJ Jr: Syndrome ofamelogenesis imperfecta, nephrocalcinosis, impaired renal con-centration, and possible abnormality of calcium metabolism.Am J Med Genet 20:233-43, 1985.
12. Witkop CJ Jr, Brearley LJ, Gentry WC Jr: Hypoplastic enamel,onycholysis, and hypohidrosis inherited as an autosomal domi-nant trait. Oral Surg Oral Med Oral Pathol 39:71-86, 1975.
13. Seow WK: Taurodontism of the mandibular first permanentmolar distinguishes between the tricho-dento-osseous (TDO)syndrome and amelogenesis imperfecta. Clin Genet 43: 240-46, 1993.
14. Crawford JL: Concomitant taurodontism and amelogenesisimperfecta in the American Caucasian. ASDC J Dent Child37:171-75, 1970.
15. Witkop CJ Jr: Partial expression for sex-linked amelogenesisimperfecta in females compatible with the Lyon hypothesis.Oral Surg Oral Med Oral Patho123:174-82, 1967.
16. Berkman MD, Singer A: Demonstration of the Lyon hypothesisin X-linked dominant hypoplastic amelogenesis imperfecta.Birth Defects 7:204-9, 1971.
17. Simonsen RJ, Kanca J: Surface hardness of posterior compositeresins using supplemental polymerization after simulatedocclusal adjustment. Quintessence Int 17:631-33, 1986.
18. Hals E: Dentin and enamel anomalies: histologic observations.In Genetics and Dental Health. Witkop CJ, ED. New York:
McGraw-Hill 19:246-60, 1962.19. Patel PR, Hovijitra S, Kafrawy AH, Bixler D: X-linked (reces-
sive) hypomaturation amelogenesis imperfecta: prosthodontic, genetic and histopathologic report. J ProsthetDent 66:398-402, 1991.
20. Sundell S, Koch G: Hereditary amelogenesis imperfecta. I.Epidemiology and clinical classification in a Swedish childpopulation. Swed Dent J 9:157-69, 1985.
21. Backman B: Amelogenesis imperfecta--clinical manifestationsin 51 families in a northern Swedish county. Scand J Dent Res96:505-16, 1988.
22. Wright JT: Analysis of a kindred with amelogenesis imperfecta.J Oral Pathol 14:366-74, 1985.
23. Alexander SA: The treatment of hypocalcified amelogenesisimperfecta in a young adolescent. J Pedod 9:95-100, 1984.
24. Crawford PJM, Evans RD, Aldred MJ: Amelogenesis imperfecta:autosomal dominant hypomaturation-hypoplasia type withtaurodontism. Br Dent J 164:71-73, 1988.
25. DeSort KD: Amelogenesis imperfecta, the genetics, classifica-tion and treatment. J Prosthet Dent 49:786-92, 1983.
26. Escobar VH, Goldblatt LI, Bixler D: A clinical, genetic, andultrastructural study of snow-capped teeth: amelogenesisimperfecta, hypomaturation type. Oral Surg Oral Med OralPatho152:607-14, 1981.
27. Fritz GW: Amelogenesis imperfecta and multiple impactions.Oral Surg Oral Med Oral Pathol 51:460, 1981.
28. Gertzman GB, Gaston G, Quinn I: Amelogenesis Imperfecta:Local hypoplastic type with pulpal calcification. J Am DentAssoc 99:637-9, 1979.
29. Haug RH, Ferguson FS: X-linked recessive hypomaturationamelogenesis imperfecta: report of case. J Am Dent Assoc102:865-67, 1981.
30. Johnson A, Winstanley RB: Use of simple overdentures in thetreatment of young patients with developmental anomalies.Quintessence Dent-Technol 11:27-33, 1987.
31. Joho JP, Marechaux SC: Amelogenesis imperfecta: treatmentof a case. ASDC J Dent Child 47:266-68, 1980.
32. Malone W, Bazola FN: Early treatment of amelogenesisimperfecta: J Prosthet Dent 16:504-44, 1966.
33. McLarty EL, Giansanti JS, Hibbard ED: X-linkedhypomaturation type of amelogenesis imperfecta exhibitinglyonization in affected females. Oral Surg Oral Med Oral Pathol36:678-85, 1973.
34. Rada RE, Hasiakos PS: Current treatment modalities in theconservative restoration of amelogenesis imperfecta: a casereport. Quintessence Int 21:937-42, 1990.
35. Renner RP, Ferguson FS: Overdenture management ofamelogenesis imperfecta. Quintessence Int 14:1009-22, 1983.
36. Winter GB, Lee KW, Johnson NW: Hereditary AmelogenesisImperfecta. A rare Autosomal Dominant type. Br Dent J127:157-64, 1969.
37. Witkop CJ Jr, Kuhlman W, Sauk J Jr: Autosomal recessive pig-mented hypomaturation, Amelogenesis Imperfecta. Oral SurgOral Med Oral Patho136:367-82, 1973.
38. Crawford PJ, Aldred MJ: X-linked amelogenesis imperfecta.Presentation of two kindreds and a review of the literature.Oral Surg Oral Med Oral Pathol 73:449-55, 1992.
39. Seow WK: The trichodentoosseous syndrome: review of theliterature and case report. Pediatr Dent 15:355-61, 1993.
40. Shapiro SD, Quattromani FL, Jorgenson RJ, Young RS: Tricho-dento-osseous syndrome: heterogeneity or clinical variability.Am J Med Genet 16:225-36, 1983.
41. Lichtenstein J, Warson R, Jorgenson R, Dorst JP, McKusick VA:The tricho-dento-osseous (TDO) syndrome. Am J Hum Genet24:569-82, 1972.
42. Koshiba H, Kimura O, Nakata M, Witkop CJ: Clinical geneticand histologic features of the trichoonychodental (TOD) syn-drome. Oral Surg Oral Med Oral Pathol 46:376-85, 1978.
43. Cutress TW, Suckling GW: Differential diagnosis of dental
392 Pediatric Dentistry: November/December 1993 - Volume 15, Number 6

fluorosis. J Dent Res 69 (Spec Iss):714-20,1990.44. Backmann B, Anneroth G, Horstedt P: Amelogenesis
imperfecta—a scanning electron microscopic andmicroradiographic study. J Oral Pathol Med 18:140-45,1989.
45. Backmann B, Anneroth G: Microradiographic study ofamelogenesis imperfecta. Scand J Dent Res 97:316-29,1989.
46. Nakahori Y, Takenaka O, Nakagome Y: A human X-Y homolo-gous region encodes "amelogenin." Genomics 9:264-69,1991.
47. Aldred MJ, Crawford PJ, Roberts E, Gillespie CM, ThomasNST, Fenton I, Sandkuijl LA, Harper PS: Genetic heterogeneityin X-linked amelogenesis imperfecta. Genomics:14:567-73,1992.
48. Gibbard PD: The management of children and adolescentssuffering from amelogenesis imperfecta and dentinogenesisimperfecta. Int J Orthod 12:15-25, 1974.
49. Seow WK: The application of tooth separation in pedodontics.ASDC J Dent Child 51:428-30,1984.
50. Seow WK, Latham SC: The spectrum of dental manifestationsin vitamin D-resistant rickets. Pediatr Dent 8:245-50,1986.
51. Wright JT, Waite P, Mueninghoff L, Sarver DM: Themultidisciplinary approach managing enamel defects. J AmDent Assoc 122:62-65,1991.
52. Persson M, Sundell S: Facial morphology and open bite defor-mity in amelogenesis imperfecta. A roentgenocephalometricstudy. Acta Odontol Scand 40:135-44,1982.
53. Rowley R, Hill FJ, Winter GB: An investigation of the associa-tion between anterior openbite and amelogenesis imperfecta.Am J Orthod Dentofacial Orthop 81:229-35,1982.
New chairman of the board and board directorof the American Board of Pediatric Dentistry
Thomas J. WickliffeDuring the Annual Meeting of the American
Board of Pediatric Dentistry at Richmond, Vir-ginia, Dr. Thomas J. Wickliffe, a pediatric dentistin Billings, Montana, was installed as chairmanof the board. Dr. Wickliffe received a DDS and anMSD in pediatric dentistry from Indiana Univer-sity. He is a past president of the Ninth DistrictDental Society and the Montana Academy of Pe-diatric Dentistry, and is a fellow of the AmericanAcademy of Pediatric Dentistry. Dr. Wickliffehas served on the Membership Committee of theAcademy.
Michael W. RobertsDr. Roberts received his DDS from the Univer-
sity of Texas—Houston. He completed a generalpractice residency at the U.S. Public Health Ser-vice Hospital in Boston and received a MScD inpediatric dentistry from the Boston UniversitySchool of Graduate Dentistry. In 1989, Dr. Rob-erts joined the University of North Carolina Schoolof Dentistry and School of Medicine faculties asgraduate program director, pediatric dentistry,following a career in the U.S. Public Health Ser-vice. He is a fellow of the American Academy ofPediatric Dentistry, American Society of Dentistryfor Children, and American College of Dentists.Dr. Roberts has served on numerous committeesof the American Academy of Pediatric Dentistryand is currently chairman, membership.
Pediatric Dentistry: November/December 1993 - Volume 15, Number 6 393