Embed Size (px)
Citation preview

Case ReportSuccessful Management of Coronary Artery Rupture withStent-Graft A Case Report
Berkay Ekici Aycan Fahri Erkan Utku Kuumltuumlk and Hasan Fehmi Toumlre
Department of Cardiology Faculty of Medicine Ufuk University Mevlana Bulvarı (Konya Yolu) No 86-88 Balgat06520 Ankara Turkey
Correspondence should be addressed to Berkay Ekici berkayekicigmailcom
Received 6 March 2014 Revised 18 June 2014 Accepted 23 June 2014 Published 13 July 2014
Academic Editor Grigorios Korosoglou
Copyright copy 2014 Berkay Ekici et al This is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Perforation of coronary arteries is a relatively rare yet life-threatening complication of percutaneus coronary interventions andis encountered in approximately 05 of these procedures According to the type of coronary perforation various methods ofcorrection are employed ranging from conservative approach to emergency cardiac surgery Coronary stent-grafts are composedof two metal stents and a polytetrafluoroethylene layer between them Advent of such stents enabled efficient endovascular repairof coronary artery perforation We present a case of coronary artery perforation which had occurred during stent implantation forthe treatment of a bridged segment in the distal portion of the left anterior descending artery This perforation was successfullymanaged by implanting a stent-graft
1 Introduction
Coronary perforation (CP) is a rare percutaneous coronaryintervention (PCI) complication which may lead to pericar-dial effusion frequently accompanied by tamponade CP isoften mortal when it is undiagnosed or untreated Due tothe expanding volume of PCI procedures worldwide a rapidincrease in the number of CP cases has been observed in thelast decades Nevertheless definitive management of CP hasnot been established yet [1ndash3]
2 Case Presentation
A 74-year-old man was admitted to the cardiology depart-ment of our institution with a history of chest pain anddyspnea on exertion His functional capacity was class IIaccording to the New York Heart Association (NYHA)classification He had a history of stent implantation in theproximal left anterior descending coronary artery (LAD)two years ago in another facility Physical examination wasunremarkable except for the hypotension (9050mmHg) andbradycardia (57 beats per minute) A chest X-ray revealedmoderate cardiomegaly The patientrsquos complete blood countbiochemical analyses and the coagulation tests were normal
An electrocardiogram (ECG) showed sinus rhythm andnonspecific ST-T segment changes Transthoracic echocar-diography images revealed hyperdynamic left ventricularsystolic function grade I diastolic dysfunction left ventric-ular regional wall motion abnormality (mild anterior wallhypokinesia) and mild tricuspid and mitral regurgitationIn order to investigate the etiology of the chest pain dobu-tamine stress echocardiography was performed revealingworsening hypokinesia of the anterior wall Due to positivedobutamine stress echocardiography and recurring anginacoronary angiography was performed It revealed nonsignif-icant atherosclerotic plaques in the circumflex artery andthe right coronary artery a patent stent in the proximalLAD and myocardial bridges causing severe compressionand near complete occlusion of the middle and distal LADduring systole with pulsatile contrast hanging or a ldquomilkingeffectrdquo Despite medical therapy with acetylsalicylic acid a 120573-blocker and a calcium antagonist the patient continued toexperience dyspnea and chest pain during exercise thereforePCI for the treatment of the bridged segments in the LADwas planned After administration of a 600mg loading doseof clopidogrel and an intravenous bolus of 10000 unitsheparin left main coronary artery was cannulated with a7F JL4 guiding catheter and a 001410158401015840 floppy guide wire was
Hindawi Publishing CorporationCase Reports in MedicineVolume 2014 Article ID 391843 4 pageshttpdxdoiorg1011552014391843
2 Case Reports in Medicine
(a) (b) (c) (d)
(e) (f) (g) (h)
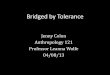
Figure 1 ((a)-(b)) Coronary angiography images of the patient in anterior-posterior cranial and lateral views which show myocardialbridges causing severe compression and near complete occlusion of the middle and distal segments of the LAD during systole markedby arrows ((c)-(d)) A drug eluting stent deployment at the middle segment of the LAD in lateral view ((e)-(f)) During stenting of thedistal segment of the LAD coronary artery perforation occurred and massive blood flow extravasating into the pericardial space ((g)-(h)) Apolytetrafluoroethylene-covered stent was deployed over the perforation site and this successfully sealed the perforation LAD left anteriordescending
advancedThemiddle segment of the LADwhich was almosttotally compressed by the myocardial bridge was stentedusing a 275 times 18mm drug eluting stent (DES) deployed at16 atmospheres There was no residual stenosis dissectionor evidence of compression by the myocardial bridge atthe end of this procedure During stenting of the bridgedsegment in the distal portion of the LAD with a 275 times14mmDES at 18 atmospheres CP occurred and angiographicimages showed massive and pulsatile extravasation from theLAD into the pericardial space (Figure 1) An immediatedrop in blood pressure and heart rate was noted and thepatient complained of severe chest pain Bigeminal ventric-ular premature complexes and slight ST segment depressionin the anterior precordial leads were noted on the ECG Astent-graft 19mm in length connected with a 3mm balloonwas implanted immediately in the site of the rupture with
subsequent complete restitution of blood flow in the LADandtermination of extravasation into the pericardial space Thechest pain abated and the ECG was normalized Protaminesulfate (50mg) was administered intravenously to reverse theeffect of heparin after intervention Ibuprofen (800mg 1 times2 po) was prescribed as an analgesic and anti-inflammatorymedication Transthoracic echocardiography in the catheterlaboratory and one day after the PCI procedure showed min-imal intrapericardial fluid but no progression was observedThe patient was followed up for 2 days in the coronary careunit and was discharged from the hospital 1 week later Atthe follow-up visits at 30 days and 2 months the patientrsquosNYHA class was improved and chest pain was alleviatedThepatient is currently on follow-up with medical treatment for4 months and long-term dual antiplatelet therapy for at least1 year has been planned
Case Reports in Medicine 3
3 Discussion
Coronary artery perforation is a rare but potentially fatalcomplication of PCI that can result in life-threatening cardiactamponade In the present era the incidence of CP rangesfrom 019 to 059 [4ndash6] CP occurs when a dissection orintimal tear completely penetrates the arterial wall leading toeither vessel puncture with minimal dye staining or vesselrupture with brisk extravasations of blood and dye into thepericardial space Several factors can be associated with theseconditions
(1) clinical variables advanced age female sex renal dys-function and non-ST-segment elevation myocardialinfarction
(2) angiographic factors chronic total occlusion coro-nary artery calcification tortuous vessels targetlesions in the circumflex and right coronary arterieslong target lesions (gt20mm) and eccentric lesions
(3) technique-associated factors use of hydrophilicextrastiff wires atherectomy devices increased balloonto artery ratio intravascular ultrasound guided PCIoptimization and high-pressure stent postdilatationpercutaneous excimer laser coronary angioplasty andcutting balloons [7ndash9]
Coronary perforation is encounteredmost frequently dueto distal migration of guide wire andor wire fracture oraccidental positioning of the guide wire outside the courseof the coronary artery Hydrophilic-coated guide wire mayincrease the risk of perforation because they more easilymigrate to the distal portion of the vessel [10] The CP classi-fication by Ellis et al [11] has received world-wide acceptanceType I extraluminal crater without extravasation Type IIpericardial or myocardial blushing Type III perforation ge1mm diameter with contrast streaming and cavity spilling
Traditional management of CP consists of prolongedballoon inflation (proximal to or at the site of perforationto prevent tamponade) and reversal of anticoagulation withprotamine It has been reported that the administration ofprotamine in patients with CP seems to be safe withoutan increase in the risk of vesselstent thrombosis Platelettransfusion is recommended in patients who had receivedabciximab If the renal function is normal eptifibatide andtirofiban infusions may be terminated with rapid reversalof effect owing to their short half-lives The development ofpericardial tamponade is not affected by the use of glyco-protein (GP) IIbIIIa antagonists Continuation of antiplatelettherapy is not associated with overt rebleeding [7] In a meta-analysis of three randomized trials no significant differencewas found in composite end points including complicatedCP between bivalirudin monotherapy and the use of unfrac-tionated heparin plus GP IIbIIIa inhibitors [12] Pericardio-centesis must be performed promptly if tamponade occursSurgical repair of CP comprises either ligation or suturingof the vessel and bypass grafting to the distal portion ofthe vessel In addition pericardial patchTeflon felt wrappingrepair of the CP with or without coronary bypass grafting isrecommended particularly whenmultiple stents with CP andsubepicardial hematoma are present [13]
The incidence of adverse outcomes emergency coronaryartery bypass grafting and death significantly decreased inthe present era [14] Stent-grafts for emergency implantationin case of CP must be an obligatory inventory of catheteriza-tion laboratories The polytetrafluoroethylene-coated stent isa safe and effective alternative which can be used for sealinga major CP and obviating cardiac surgery The utilization ofsynthetic stent-grafts is less invasive faster andmore effectivewhen compared to surgical interventions and is generallyconsidered to be the gold standard in the management of CP[15] The incidence of subacute thrombosis and restenosis inthe stent-grafts is relatively higher than in the conventionalcoronary stents (103 versus 34 resp) which may berelated to delayed endothelialization and increased suscep-tibility to thrombus formation in these stents Thereforelong-term dual antiplatelet therapy at least for 1 year isrecommended [16] In our case the rapidly forming massivepericardial effusion and hemodynamic instability led tothe decision of urgent intervention and a stent-graft wasimplanted immediately Angiographic images after the stent-graft procedure were satisfactory and the CP had been totallysealed The rupture in this case may have occurred dueto advanced age high-pressure balloon dilatation relativelysmall diameter of the vessel and the fragility of the vesselwall between the bridged segment and the normal segmentNevertheless the information about CP during stenting ofbridged segments is limited and the topic warrants furtherresearch
Stenting of a myocardial bridge is still controversial dueto high restenosis rates potential plaque prolapse and risk ofstent fracture Myocardial bridging is asymptomatic in mostof the cases but in rare instances it may be associated withserious complications such as acute coronary syndromeslethal arrhythmias and even sudden death Symptomaticpatients with objective evidence of ischemia on noninvasivestress tests and which are refractory to medical therapy PCIor surgical treatment should be preferred [17] Our casemay be interesting due to the nature of the target lesion (abridging segment) and to the best of our knowledge suchcases were not described constantly In our case the patientwas symptomatic despite therapy with acetylsalicylic acida 120573-blocker and a calcium antagonist therefore PCI formyocardial bridgingmiddle and distal part of the LAD arterywas performed
4 Conclusion
As a conclusion in cases of CP the importance of timelymanagement cannot be overemphasized Treatment of CPrequires rapid diagnosis and angiographic classification Toavoid this serious and potentially lethal complication cautionmust be exercised while advancing guide wires and duringdilatation of the coronary lesion either before stent duringor after stent implantation Immediate sealing of the rupturedcoronary vessel employing stent-grafts in addition to reversalof anticoagulation can defer a potentially lethal complicationUse of stent-grafts in large proximal perforations does notrequire any additional skill for an experienced interventional
4 Case Reports in Medicine
cardiologist Nevertheless distal coronary artery perforationsmay necessitate use of various embolic materials that aninterventional cardiologist should be familiar with
Conflict of Interests
No potential conflict of interests relevant to this paper wasreported
References
[1] M Fejka S R Dixon R D Safian et al ldquoDiagnosis manage-ment and clinical outcome of cardiac tamponade complicatingpercutaneous coronary interventionrdquo The American Journal ofCardiology vol 90 no 11 pp 1183ndash1186 2002
[2] R Von Sohsten C KopistanskyM Cohen andWG KussmaulIII ldquoCardiac tamponade in the ldquonew devicerdquo era evaluationof 6999 consecutive percutaneous coronary interventionsrdquoAmerican Heart Journal vol 140 no 2 pp 279ndash283 2000
[3] T Fukutomi S Takahiko J Popma Jeffrey et al ldquoEarly and lateclinical outcomes following coronary perforation in patientsundergoing percutaneous coronary interventionrdquo CirculationJournal vol 66 no 4 pp 349ndash356 2002
[4] P Fasseas J L Orford C J Panetta et al ldquoIncidence correlatesmanagement and clinical outcome of coronary perforationanalysis of 16298 proceduresrdquoTheAmerican Heart Journal vol147 no 1 pp 140ndash145 2004
[5] C F Witzke F Martin-Herrero S C Clarke E Pomerantzevand I F Palacios ldquoThe changing pattern of coronary perforationduring percutaneous coronary intervention in the new deviceerardquo The Journal of Invasive Cardiology vol 16 no 6 pp 257ndash301 2004
[6] R K Ramana D Arab D Joyal et al ldquoCoronary artery per-foration during percutaneous coronary intervention incidenceand outcomes in the new interventional erardquo Journal of InvasiveCardiology vol 17 no 11 pp 603ndash605 2005
[7] M Al-Mukhaini P Panduranga K Sulaiman A A Riyami MDeeb and M B Riyami ldquoCoronary perforation and coveredstents an update and reviewrdquoHeart Views vol 12 no 2 pp 63ndash70 2011
[8] F Litvack N Eigler J Margolis et al ldquoPercutaneous excimerlaser coronary angioplasty results in the first consecutive 3000patientsrdquo Journal of the American College of Cardiology vol 23no 2 pp 323ndash329 1994
[9] L Gruberg E Pinnow R Flood et al ldquoIncidencemanagementand outcome of coronary artery perforation during percuta-neous coronary interventionrdquo American Journal of Cardiologyvol 86 no 6 pp 680ndash682 A8 2000
[10] J H Rogers and J M Lasala ldquoCoronary artery dissection andperforation complicating percutaneous coronary interventionrdquoJournal of Invasive Cardiology vol 16 no 9 pp 493ndash499 2004
[11] S G Ellis S Ajluni A Z Arnold et al ldquoIncreased coronaryperforation in the new device era incidence classificationmanagement and outcomerdquo Circulation vol 90 no 6 pp2725ndash2730 1994
[12] J A Doll E Nikolsky G W Stone et al ldquoOutcomes ofpatients with coronary artery perforation complicating percu-taneous coronary intervention and correlations with the typeof adjunctive antithrombotic therapy pooled analysis fromREPLACE-2 ACUITY andHORIZONS-AMI trialsrdquo Journal ofInterventional Cardiology vol 22 no 5 pp 453ndash459 2009
[13] Y Inoue T Ueda S Taguchi I Kashima K Koizumi and SNoma ldquoTeflon felt wrapping repair for coronary perforationafter failed angioplastyrdquo Annals of Thoracic Surgery vol 82 no6 pp 2312ndash2314 2006
[14] G Stankovic D Orlic N Corvaja et al ldquoIncidence predictorsin-hospital and late outcomes of coronary artery perforationsrdquoThe American Journal of Cardiology vol 93 no 2 pp 213ndash2162004
[15] P Jamshidi K Mahmoody and P Erne ldquoCovered stents areviewrdquo International Journal of Cardiology vol 130 no 3 pp310ndash318 2008
[16] M Takano M Yamamoto S Inami et al ldquoDelayed endothe-lialization after polytetrafluoroethylene-covered stent implan-tation for coronary aneurysmrdquo Circulation Journal vol 73 no1 pp 190ndash193 2009
[17] T Y Shen C C Chen and Y Z Tseng ldquoStent graft usedto rescue coronary rupture during percutaneous coronaryintervention for myocardial bridgerdquo Internal Medicine vol 48no 12 pp 993ndash996 2009
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Case Reports in Medicine
(a) (b) (c) (d)
(e) (f) (g) (h)
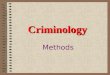
Figure 1 ((a)-(b)) Coronary angiography images of the patient in anterior-posterior cranial and lateral views which show myocardialbridges causing severe compression and near complete occlusion of the middle and distal segments of the LAD during systole markedby arrows ((c)-(d)) A drug eluting stent deployment at the middle segment of the LAD in lateral view ((e)-(f)) During stenting of thedistal segment of the LAD coronary artery perforation occurred and massive blood flow extravasating into the pericardial space ((g)-(h)) Apolytetrafluoroethylene-covered stent was deployed over the perforation site and this successfully sealed the perforation LAD left anteriordescending
advancedThemiddle segment of the LADwhich was almosttotally compressed by the myocardial bridge was stentedusing a 275 times 18mm drug eluting stent (DES) deployed at16 atmospheres There was no residual stenosis dissectionor evidence of compression by the myocardial bridge atthe end of this procedure During stenting of the bridgedsegment in the distal portion of the LAD with a 275 times14mmDES at 18 atmospheres CP occurred and angiographicimages showed massive and pulsatile extravasation from theLAD into the pericardial space (Figure 1) An immediatedrop in blood pressure and heart rate was noted and thepatient complained of severe chest pain Bigeminal ventric-ular premature complexes and slight ST segment depressionin the anterior precordial leads were noted on the ECG Astent-graft 19mm in length connected with a 3mm balloonwas implanted immediately in the site of the rupture with
subsequent complete restitution of blood flow in the LADandtermination of extravasation into the pericardial space Thechest pain abated and the ECG was normalized Protaminesulfate (50mg) was administered intravenously to reverse theeffect of heparin after intervention Ibuprofen (800mg 1 times2 po) was prescribed as an analgesic and anti-inflammatorymedication Transthoracic echocardiography in the catheterlaboratory and one day after the PCI procedure showed min-imal intrapericardial fluid but no progression was observedThe patient was followed up for 2 days in the coronary careunit and was discharged from the hospital 1 week later Atthe follow-up visits at 30 days and 2 months the patientrsquosNYHA class was improved and chest pain was alleviatedThepatient is currently on follow-up with medical treatment for4 months and long-term dual antiplatelet therapy for at least1 year has been planned
Case Reports in Medicine 3
3 Discussion
Coronary artery perforation is a rare but potentially fatalcomplication of PCI that can result in life-threatening cardiactamponade In the present era the incidence of CP rangesfrom 019 to 059 [4ndash6] CP occurs when a dissection orintimal tear completely penetrates the arterial wall leading toeither vessel puncture with minimal dye staining or vesselrupture with brisk extravasations of blood and dye into thepericardial space Several factors can be associated with theseconditions
(1) clinical variables advanced age female sex renal dys-function and non-ST-segment elevation myocardialinfarction
(2) angiographic factors chronic total occlusion coro-nary artery calcification tortuous vessels targetlesions in the circumflex and right coronary arterieslong target lesions (gt20mm) and eccentric lesions
(3) technique-associated factors use of hydrophilicextrastiff wires atherectomy devices increased balloonto artery ratio intravascular ultrasound guided PCIoptimization and high-pressure stent postdilatationpercutaneous excimer laser coronary angioplasty andcutting balloons [7ndash9]
Coronary perforation is encounteredmost frequently dueto distal migration of guide wire andor wire fracture oraccidental positioning of the guide wire outside the courseof the coronary artery Hydrophilic-coated guide wire mayincrease the risk of perforation because they more easilymigrate to the distal portion of the vessel [10] The CP classi-fication by Ellis et al [11] has received world-wide acceptanceType I extraluminal crater without extravasation Type IIpericardial or myocardial blushing Type III perforation ge1mm diameter with contrast streaming and cavity spilling
Traditional management of CP consists of prolongedballoon inflation (proximal to or at the site of perforationto prevent tamponade) and reversal of anticoagulation withprotamine It has been reported that the administration ofprotamine in patients with CP seems to be safe withoutan increase in the risk of vesselstent thrombosis Platelettransfusion is recommended in patients who had receivedabciximab If the renal function is normal eptifibatide andtirofiban infusions may be terminated with rapid reversalof effect owing to their short half-lives The development ofpericardial tamponade is not affected by the use of glyco-protein (GP) IIbIIIa antagonists Continuation of antiplatelettherapy is not associated with overt rebleeding [7] In a meta-analysis of three randomized trials no significant differencewas found in composite end points including complicatedCP between bivalirudin monotherapy and the use of unfrac-tionated heparin plus GP IIbIIIa inhibitors [12] Pericardio-centesis must be performed promptly if tamponade occursSurgical repair of CP comprises either ligation or suturingof the vessel and bypass grafting to the distal portion ofthe vessel In addition pericardial patchTeflon felt wrappingrepair of the CP with or without coronary bypass grafting isrecommended particularly whenmultiple stents with CP andsubepicardial hematoma are present [13]
The incidence of adverse outcomes emergency coronaryartery bypass grafting and death significantly decreased inthe present era [14] Stent-grafts for emergency implantationin case of CP must be an obligatory inventory of catheteriza-tion laboratories The polytetrafluoroethylene-coated stent isa safe and effective alternative which can be used for sealinga major CP and obviating cardiac surgery The utilization ofsynthetic stent-grafts is less invasive faster andmore effectivewhen compared to surgical interventions and is generallyconsidered to be the gold standard in the management of CP[15] The incidence of subacute thrombosis and restenosis inthe stent-grafts is relatively higher than in the conventionalcoronary stents (103 versus 34 resp) which may berelated to delayed endothelialization and increased suscep-tibility to thrombus formation in these stents Thereforelong-term dual antiplatelet therapy at least for 1 year isrecommended [16] In our case the rapidly forming massivepericardial effusion and hemodynamic instability led tothe decision of urgent intervention and a stent-graft wasimplanted immediately Angiographic images after the stent-graft procedure were satisfactory and the CP had been totallysealed The rupture in this case may have occurred dueto advanced age high-pressure balloon dilatation relativelysmall diameter of the vessel and the fragility of the vesselwall between the bridged segment and the normal segmentNevertheless the information about CP during stenting ofbridged segments is limited and the topic warrants furtherresearch
Stenting of a myocardial bridge is still controversial dueto high restenosis rates potential plaque prolapse and risk ofstent fracture Myocardial bridging is asymptomatic in mostof the cases but in rare instances it may be associated withserious complications such as acute coronary syndromeslethal arrhythmias and even sudden death Symptomaticpatients with objective evidence of ischemia on noninvasivestress tests and which are refractory to medical therapy PCIor surgical treatment should be preferred [17] Our casemay be interesting due to the nature of the target lesion (abridging segment) and to the best of our knowledge suchcases were not described constantly In our case the patientwas symptomatic despite therapy with acetylsalicylic acida 120573-blocker and a calcium antagonist therefore PCI formyocardial bridgingmiddle and distal part of the LAD arterywas performed
4 Conclusion
As a conclusion in cases of CP the importance of timelymanagement cannot be overemphasized Treatment of CPrequires rapid diagnosis and angiographic classification Toavoid this serious and potentially lethal complication cautionmust be exercised while advancing guide wires and duringdilatation of the coronary lesion either before stent duringor after stent implantation Immediate sealing of the rupturedcoronary vessel employing stent-grafts in addition to reversalof anticoagulation can defer a potentially lethal complicationUse of stent-grafts in large proximal perforations does notrequire any additional skill for an experienced interventional
4 Case Reports in Medicine
cardiologist Nevertheless distal coronary artery perforationsmay necessitate use of various embolic materials that aninterventional cardiologist should be familiar with
Conflict of Interests
No potential conflict of interests relevant to this paper wasreported
References
[1] M Fejka S R Dixon R D Safian et al ldquoDiagnosis manage-ment and clinical outcome of cardiac tamponade complicatingpercutaneous coronary interventionrdquo The American Journal ofCardiology vol 90 no 11 pp 1183ndash1186 2002
[2] R Von Sohsten C KopistanskyM Cohen andWG KussmaulIII ldquoCardiac tamponade in the ldquonew devicerdquo era evaluationof 6999 consecutive percutaneous coronary interventionsrdquoAmerican Heart Journal vol 140 no 2 pp 279ndash283 2000
[3] T Fukutomi S Takahiko J Popma Jeffrey et al ldquoEarly and lateclinical outcomes following coronary perforation in patientsundergoing percutaneous coronary interventionrdquo CirculationJournal vol 66 no 4 pp 349ndash356 2002
[4] P Fasseas J L Orford C J Panetta et al ldquoIncidence correlatesmanagement and clinical outcome of coronary perforationanalysis of 16298 proceduresrdquoTheAmerican Heart Journal vol147 no 1 pp 140ndash145 2004
[5] C F Witzke F Martin-Herrero S C Clarke E Pomerantzevand I F Palacios ldquoThe changing pattern of coronary perforationduring percutaneous coronary intervention in the new deviceerardquo The Journal of Invasive Cardiology vol 16 no 6 pp 257ndash301 2004
[6] R K Ramana D Arab D Joyal et al ldquoCoronary artery per-foration during percutaneous coronary intervention incidenceand outcomes in the new interventional erardquo Journal of InvasiveCardiology vol 17 no 11 pp 603ndash605 2005
[7] M Al-Mukhaini P Panduranga K Sulaiman A A Riyami MDeeb and M B Riyami ldquoCoronary perforation and coveredstents an update and reviewrdquoHeart Views vol 12 no 2 pp 63ndash70 2011
[8] F Litvack N Eigler J Margolis et al ldquoPercutaneous excimerlaser coronary angioplasty results in the first consecutive 3000patientsrdquo Journal of the American College of Cardiology vol 23no 2 pp 323ndash329 1994
[9] L Gruberg E Pinnow R Flood et al ldquoIncidencemanagementand outcome of coronary artery perforation during percuta-neous coronary interventionrdquo American Journal of Cardiologyvol 86 no 6 pp 680ndash682 A8 2000
[10] J H Rogers and J M Lasala ldquoCoronary artery dissection andperforation complicating percutaneous coronary interventionrdquoJournal of Invasive Cardiology vol 16 no 9 pp 493ndash499 2004
[11] S G Ellis S Ajluni A Z Arnold et al ldquoIncreased coronaryperforation in the new device era incidence classificationmanagement and outcomerdquo Circulation vol 90 no 6 pp2725ndash2730 1994
[12] J A Doll E Nikolsky G W Stone et al ldquoOutcomes ofpatients with coronary artery perforation complicating percu-taneous coronary intervention and correlations with the typeof adjunctive antithrombotic therapy pooled analysis fromREPLACE-2 ACUITY andHORIZONS-AMI trialsrdquo Journal ofInterventional Cardiology vol 22 no 5 pp 453ndash459 2009
[13] Y Inoue T Ueda S Taguchi I Kashima K Koizumi and SNoma ldquoTeflon felt wrapping repair for coronary perforationafter failed angioplastyrdquo Annals of Thoracic Surgery vol 82 no6 pp 2312ndash2314 2006
[14] G Stankovic D Orlic N Corvaja et al ldquoIncidence predictorsin-hospital and late outcomes of coronary artery perforationsrdquoThe American Journal of Cardiology vol 93 no 2 pp 213ndash2162004
[15] P Jamshidi K Mahmoody and P Erne ldquoCovered stents areviewrdquo International Journal of Cardiology vol 130 no 3 pp310ndash318 2008
[16] M Takano M Yamamoto S Inami et al ldquoDelayed endothe-lialization after polytetrafluoroethylene-covered stent implan-tation for coronary aneurysmrdquo Circulation Journal vol 73 no1 pp 190ndash193 2009
[17] T Y Shen C C Chen and Y Z Tseng ldquoStent graft usedto rescue coronary rupture during percutaneous coronaryintervention for myocardial bridgerdquo Internal Medicine vol 48no 12 pp 993ndash996 2009
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Case Reports in Medicine 3
3 Discussion
Coronary artery perforation is a rare but potentially fatalcomplication of PCI that can result in life-threatening cardiactamponade In the present era the incidence of CP rangesfrom 019 to 059 [4ndash6] CP occurs when a dissection orintimal tear completely penetrates the arterial wall leading toeither vessel puncture with minimal dye staining or vesselrupture with brisk extravasations of blood and dye into thepericardial space Several factors can be associated with theseconditions
(1) clinical variables advanced age female sex renal dys-function and non-ST-segment elevation myocardialinfarction
(2) angiographic factors chronic total occlusion coro-nary artery calcification tortuous vessels targetlesions in the circumflex and right coronary arterieslong target lesions (gt20mm) and eccentric lesions
(3) technique-associated factors use of hydrophilicextrastiff wires atherectomy devices increased balloonto artery ratio intravascular ultrasound guided PCIoptimization and high-pressure stent postdilatationpercutaneous excimer laser coronary angioplasty andcutting balloons [7ndash9]
Coronary perforation is encounteredmost frequently dueto distal migration of guide wire andor wire fracture oraccidental positioning of the guide wire outside the courseof the coronary artery Hydrophilic-coated guide wire mayincrease the risk of perforation because they more easilymigrate to the distal portion of the vessel [10] The CP classi-fication by Ellis et al [11] has received world-wide acceptanceType I extraluminal crater without extravasation Type IIpericardial or myocardial blushing Type III perforation ge1mm diameter with contrast streaming and cavity spilling
Traditional management of CP consists of prolongedballoon inflation (proximal to or at the site of perforationto prevent tamponade) and reversal of anticoagulation withprotamine It has been reported that the administration ofprotamine in patients with CP seems to be safe withoutan increase in the risk of vesselstent thrombosis Platelettransfusion is recommended in patients who had receivedabciximab If the renal function is normal eptifibatide andtirofiban infusions may be terminated with rapid reversalof effect owing to their short half-lives The development ofpericardial tamponade is not affected by the use of glyco-protein (GP) IIbIIIa antagonists Continuation of antiplatelettherapy is not associated with overt rebleeding [7] In a meta-analysis of three randomized trials no significant differencewas found in composite end points including complicatedCP between bivalirudin monotherapy and the use of unfrac-tionated heparin plus GP IIbIIIa inhibitors [12] Pericardio-centesis must be performed promptly if tamponade occursSurgical repair of CP comprises either ligation or suturingof the vessel and bypass grafting to the distal portion ofthe vessel In addition pericardial patchTeflon felt wrappingrepair of the CP with or without coronary bypass grafting isrecommended particularly whenmultiple stents with CP andsubepicardial hematoma are present [13]
The incidence of adverse outcomes emergency coronaryartery bypass grafting and death significantly decreased inthe present era [14] Stent-grafts for emergency implantationin case of CP must be an obligatory inventory of catheteriza-tion laboratories The polytetrafluoroethylene-coated stent isa safe and effective alternative which can be used for sealinga major CP and obviating cardiac surgery The utilization ofsynthetic stent-grafts is less invasive faster andmore effectivewhen compared to surgical interventions and is generallyconsidered to be the gold standard in the management of CP[15] The incidence of subacute thrombosis and restenosis inthe stent-grafts is relatively higher than in the conventionalcoronary stents (103 versus 34 resp) which may berelated to delayed endothelialization and increased suscep-tibility to thrombus formation in these stents Thereforelong-term dual antiplatelet therapy at least for 1 year isrecommended [16] In our case the rapidly forming massivepericardial effusion and hemodynamic instability led tothe decision of urgent intervention and a stent-graft wasimplanted immediately Angiographic images after the stent-graft procedure were satisfactory and the CP had been totallysealed The rupture in this case may have occurred dueto advanced age high-pressure balloon dilatation relativelysmall diameter of the vessel and the fragility of the vesselwall between the bridged segment and the normal segmentNevertheless the information about CP during stenting ofbridged segments is limited and the topic warrants furtherresearch
Stenting of a myocardial bridge is still controversial dueto high restenosis rates potential plaque prolapse and risk ofstent fracture Myocardial bridging is asymptomatic in mostof the cases but in rare instances it may be associated withserious complications such as acute coronary syndromeslethal arrhythmias and even sudden death Symptomaticpatients with objective evidence of ischemia on noninvasivestress tests and which are refractory to medical therapy PCIor surgical treatment should be preferred [17] Our casemay be interesting due to the nature of the target lesion (abridging segment) and to the best of our knowledge suchcases were not described constantly In our case the patientwas symptomatic despite therapy with acetylsalicylic acida 120573-blocker and a calcium antagonist therefore PCI formyocardial bridgingmiddle and distal part of the LAD arterywas performed
4 Conclusion
As a conclusion in cases of CP the importance of timelymanagement cannot be overemphasized Treatment of CPrequires rapid diagnosis and angiographic classification Toavoid this serious and potentially lethal complication cautionmust be exercised while advancing guide wires and duringdilatation of the coronary lesion either before stent duringor after stent implantation Immediate sealing of the rupturedcoronary vessel employing stent-grafts in addition to reversalof anticoagulation can defer a potentially lethal complicationUse of stent-grafts in large proximal perforations does notrequire any additional skill for an experienced interventional
4 Case Reports in Medicine
cardiologist Nevertheless distal coronary artery perforationsmay necessitate use of various embolic materials that aninterventional cardiologist should be familiar with
Conflict of Interests
No potential conflict of interests relevant to this paper wasreported
References
[1] M Fejka S R Dixon R D Safian et al ldquoDiagnosis manage-ment and clinical outcome of cardiac tamponade complicatingpercutaneous coronary interventionrdquo The American Journal ofCardiology vol 90 no 11 pp 1183ndash1186 2002
[2] R Von Sohsten C KopistanskyM Cohen andWG KussmaulIII ldquoCardiac tamponade in the ldquonew devicerdquo era evaluationof 6999 consecutive percutaneous coronary interventionsrdquoAmerican Heart Journal vol 140 no 2 pp 279ndash283 2000
[3] T Fukutomi S Takahiko J Popma Jeffrey et al ldquoEarly and lateclinical outcomes following coronary perforation in patientsundergoing percutaneous coronary interventionrdquo CirculationJournal vol 66 no 4 pp 349ndash356 2002
[4] P Fasseas J L Orford C J Panetta et al ldquoIncidence correlatesmanagement and clinical outcome of coronary perforationanalysis of 16298 proceduresrdquoTheAmerican Heart Journal vol147 no 1 pp 140ndash145 2004
[5] C F Witzke F Martin-Herrero S C Clarke E Pomerantzevand I F Palacios ldquoThe changing pattern of coronary perforationduring percutaneous coronary intervention in the new deviceerardquo The Journal of Invasive Cardiology vol 16 no 6 pp 257ndash301 2004
[6] R K Ramana D Arab D Joyal et al ldquoCoronary artery per-foration during percutaneous coronary intervention incidenceand outcomes in the new interventional erardquo Journal of InvasiveCardiology vol 17 no 11 pp 603ndash605 2005
[7] M Al-Mukhaini P Panduranga K Sulaiman A A Riyami MDeeb and M B Riyami ldquoCoronary perforation and coveredstents an update and reviewrdquoHeart Views vol 12 no 2 pp 63ndash70 2011
[8] F Litvack N Eigler J Margolis et al ldquoPercutaneous excimerlaser coronary angioplasty results in the first consecutive 3000patientsrdquo Journal of the American College of Cardiology vol 23no 2 pp 323ndash329 1994
[9] L Gruberg E Pinnow R Flood et al ldquoIncidencemanagementand outcome of coronary artery perforation during percuta-neous coronary interventionrdquo American Journal of Cardiologyvol 86 no 6 pp 680ndash682 A8 2000
[10] J H Rogers and J M Lasala ldquoCoronary artery dissection andperforation complicating percutaneous coronary interventionrdquoJournal of Invasive Cardiology vol 16 no 9 pp 493ndash499 2004
[11] S G Ellis S Ajluni A Z Arnold et al ldquoIncreased coronaryperforation in the new device era incidence classificationmanagement and outcomerdquo Circulation vol 90 no 6 pp2725ndash2730 1994
[12] J A Doll E Nikolsky G W Stone et al ldquoOutcomes ofpatients with coronary artery perforation complicating percu-taneous coronary intervention and correlations with the typeof adjunctive antithrombotic therapy pooled analysis fromREPLACE-2 ACUITY andHORIZONS-AMI trialsrdquo Journal ofInterventional Cardiology vol 22 no 5 pp 453ndash459 2009
[13] Y Inoue T Ueda S Taguchi I Kashima K Koizumi and SNoma ldquoTeflon felt wrapping repair for coronary perforationafter failed angioplastyrdquo Annals of Thoracic Surgery vol 82 no6 pp 2312ndash2314 2006
[14] G Stankovic D Orlic N Corvaja et al ldquoIncidence predictorsin-hospital and late outcomes of coronary artery perforationsrdquoThe American Journal of Cardiology vol 93 no 2 pp 213ndash2162004
[15] P Jamshidi K Mahmoody and P Erne ldquoCovered stents areviewrdquo International Journal of Cardiology vol 130 no 3 pp310ndash318 2008
[16] M Takano M Yamamoto S Inami et al ldquoDelayed endothe-lialization after polytetrafluoroethylene-covered stent implan-tation for coronary aneurysmrdquo Circulation Journal vol 73 no1 pp 190ndash193 2009
[17] T Y Shen C C Chen and Y Z Tseng ldquoStent graft usedto rescue coronary rupture during percutaneous coronaryintervention for myocardial bridgerdquo Internal Medicine vol 48no 12 pp 993ndash996 2009
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 Case Reports in Medicine
cardiologist Nevertheless distal coronary artery perforationsmay necessitate use of various embolic materials that aninterventional cardiologist should be familiar with
Conflict of Interests
No potential conflict of interests relevant to this paper wasreported
References
[1] M Fejka S R Dixon R D Safian et al ldquoDiagnosis manage-ment and clinical outcome of cardiac tamponade complicatingpercutaneous coronary interventionrdquo The American Journal ofCardiology vol 90 no 11 pp 1183ndash1186 2002
[2] R Von Sohsten C KopistanskyM Cohen andWG KussmaulIII ldquoCardiac tamponade in the ldquonew devicerdquo era evaluationof 6999 consecutive percutaneous coronary interventionsrdquoAmerican Heart Journal vol 140 no 2 pp 279ndash283 2000
[3] T Fukutomi S Takahiko J Popma Jeffrey et al ldquoEarly and lateclinical outcomes following coronary perforation in patientsundergoing percutaneous coronary interventionrdquo CirculationJournal vol 66 no 4 pp 349ndash356 2002
[4] P Fasseas J L Orford C J Panetta et al ldquoIncidence correlatesmanagement and clinical outcome of coronary perforationanalysis of 16298 proceduresrdquoTheAmerican Heart Journal vol147 no 1 pp 140ndash145 2004
[5] C F Witzke F Martin-Herrero S C Clarke E Pomerantzevand I F Palacios ldquoThe changing pattern of coronary perforationduring percutaneous coronary intervention in the new deviceerardquo The Journal of Invasive Cardiology vol 16 no 6 pp 257ndash301 2004
[6] R K Ramana D Arab D Joyal et al ldquoCoronary artery per-foration during percutaneous coronary intervention incidenceand outcomes in the new interventional erardquo Journal of InvasiveCardiology vol 17 no 11 pp 603ndash605 2005
[7] M Al-Mukhaini P Panduranga K Sulaiman A A Riyami MDeeb and M B Riyami ldquoCoronary perforation and coveredstents an update and reviewrdquoHeart Views vol 12 no 2 pp 63ndash70 2011
[8] F Litvack N Eigler J Margolis et al ldquoPercutaneous excimerlaser coronary angioplasty results in the first consecutive 3000patientsrdquo Journal of the American College of Cardiology vol 23no 2 pp 323ndash329 1994
[9] L Gruberg E Pinnow R Flood et al ldquoIncidencemanagementand outcome of coronary artery perforation during percuta-neous coronary interventionrdquo American Journal of Cardiologyvol 86 no 6 pp 680ndash682 A8 2000
[10] J H Rogers and J M Lasala ldquoCoronary artery dissection andperforation complicating percutaneous coronary interventionrdquoJournal of Invasive Cardiology vol 16 no 9 pp 493ndash499 2004
[11] S G Ellis S Ajluni A Z Arnold et al ldquoIncreased coronaryperforation in the new device era incidence classificationmanagement and outcomerdquo Circulation vol 90 no 6 pp2725ndash2730 1994
[12] J A Doll E Nikolsky G W Stone et al ldquoOutcomes ofpatients with coronary artery perforation complicating percu-taneous coronary intervention and correlations with the typeof adjunctive antithrombotic therapy pooled analysis fromREPLACE-2 ACUITY andHORIZONS-AMI trialsrdquo Journal ofInterventional Cardiology vol 22 no 5 pp 453ndash459 2009
[13] Y Inoue T Ueda S Taguchi I Kashima K Koizumi and SNoma ldquoTeflon felt wrapping repair for coronary perforationafter failed angioplastyrdquo Annals of Thoracic Surgery vol 82 no6 pp 2312ndash2314 2006
[14] G Stankovic D Orlic N Corvaja et al ldquoIncidence predictorsin-hospital and late outcomes of coronary artery perforationsrdquoThe American Journal of Cardiology vol 93 no 2 pp 213ndash2162004
[15] P Jamshidi K Mahmoody and P Erne ldquoCovered stents areviewrdquo International Journal of Cardiology vol 130 no 3 pp310ndash318 2008
[16] M Takano M Yamamoto S Inami et al ldquoDelayed endothe-lialization after polytetrafluoroethylene-covered stent implan-tation for coronary aneurysmrdquo Circulation Journal vol 73 no1 pp 190ndash193 2009
[17] T Y Shen C C Chen and Y Z Tseng ldquoStent graft usedto rescue coronary rupture during percutaneous coronaryintervention for myocardial bridgerdquo Internal Medicine vol 48no 12 pp 993ndash996 2009
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom