Embed Size (px)
Citation preview

271
ciated with inflammation and did not have any trauma history. The lesion was not tender and was not fixed underlying struc-ture. The mass had a clear margin and other lesion was not ob-served in her body. We excised the tumor and around normal scalp (3 mm from the tumor margin).
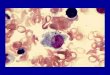
In histopathologic findings the epidermis and cutaneous ap-pendages were spared and numerous eosinophils and multinu-cleated giant cells including Touton giant cells were seen in the specimen (Fig. 2A, B). Immunohistochemical study showed CD68 positivity in most areas (Fig. 2C) and S-100 protein was negative. We confirmed juvenile xanthogranuloma. There was no recurrence for 12 months after resection.
DISCUSSION
Juvenile xanthogranuloma is an uncommon histiocytic cuta-neous lesion. It is a type of non-Langerhan’s cell histiocytosis (WHO Class IIb). It has been previously called as naevoxantho-endothelioma.
JXG is a disease of the young child. Infant and children are predominantly affected2). Median age of onset is 2 years4), how-ever lesions may be present at birth. Most JXG presents with solitary lesion which vary in size. Most are under 5 mm in diam-eter, but giant nodules may grow over 2 cm in size. Children less than 6 months of age tend to present with multiple lesions and the male preponderance is much higher (12 : 1) in young infants with multiple skin lesions4,6). The lesions are most fre-quently locate in the face or on the scalp and tends to show self-limited course over the course of several months to years. JXG involving just the skin usually follows a benign course without
INTRODUCTION
Juvenile xanthogranuloma (JXG) is an uncommon histiocytic cutaneous lesion. It is a type of non-Langerhan’s cell histiocyto-sis (WHO Class IIb). Average age of onset is 2-year-old4). The color of lesion is reddish to yellow-brown. The most common affected area is face or scalp and most lesions are under 5 mm size. It has not been clearly described on the growing rate or doubling time of this tumor. Previous reports, however, men-tioned that the tumor was rapidly enlarged to 21 mm for 5 months after curettage of the small papule5,10). This lesion tends to show self-limited course over several months to years. How-ever, large size or recurrent JXG on skin can make atypical course or cosmetic problems. Therefore, the excision is consid-ered in such lesion. We report a rapid growing JXG on the scalp of 18-month-old girl who underwent extended excision.
CASE REPORT
An 18-month-old girl visited due to rapid growing scalp le-sion. Her lesion occurred spontaneously and it was yellow spot as like acne at first. It showed a rapid growth from 1mm to 12 mm-size during 8 weeks and its color had changed from yellow to orange-yellow (Fig. 1). She did not show any symptoms asso-
J Korean Neurosurg Soc 50 : 271-273, 2011
http://dx.doi.org/10.3340/jkns.2011.50.3.271
Copyright © 2011 The Korean Neurosurgical Society
Print ISSN 2005-3711 On-line ISSN 1598-7876
Rapid-Growing Juvenile Xanthogranuloma on the Scalp in 18-Month-Old Girl
Young Woo Park, M.D., Eun Jeong Koh, M.D., Ph.D., Ha Young Choi, M.D., Ph.D.
Department of Neurosurgery, Clinical Research Institute, Chonbuk National University Medical School Hospital, Jeonju, Korea
Juvenile xanthogranuloma (JXG) is an uncommon histiocytic cutaneous lesion. An 18-month-old girl visited our clinic due to rapid growing orange-yellowish lesion on scalp. Enlarging time from 1 mm to 12 mm was just 8 weeks. We excised the tumor and adjacent normal tissue. Histopathologi-cal study showed numerous eosinophils and Touton giant cells within the lesion. Immunohistochemical study revealed positive immunoreactivity for CD68 in most areas. No recurrence was seen during 12 months after resection. We report a case with rapidly growing JXG on scalp with peculiar histopathologic findings.
Key Words : Juvenile xanthogranuloma · Scalp.
www.jkns.or.kr
Case Report
• Received : March 16, 2011 • Revised : May 15, 2011• Accepted : August 30, 2011• Address for reprints : Eun Jeong Koh, M.D., Ph.D. Department of Neurosurgery, Chonbuk National University Medical School/ Hospital, 664-14 Deokjin-dong 1-ga, Deokjin-gu, Jeonju 561-756, Korea Tel : +82-63-250-1870, Fax : +82-63-277-3273 E-mail : [email protected]
online © ML Comm

272
J Korean Neurosurg Soc 50 | September 2011
did not recur after resection. In the JXG cases in which sponta-neous regression will not occur or in multiple systemic JXG, chemotherapy to treat Langerhans cell histiocytosis should be considered11).
In histopathology a mixture of histiocytes, Touton giant cells and inflammatory cells represent JXG. The precursor of the his-tiocytes and giant cells are monocyte or macrophage in origin7). In general, immunoreactivity for CD68 and factor XIIIa is posi-tive, and S-100 protein is negative in JXG12). Our patient also showed numerous eosinophils and Touton giant cells in H&E stain and CD68 positive and S-100 negative in immunohisto-chemistry.
CONCLUSION
Neurosurgeon rarely experience patients with JXG and have the possibility of overlooking this disease entity. We report our experience of rapidly growing JXG on scalp with review of char-acteristics and treatment of JXG.
References 1. Behne K, Casey T : Ulcerated juvenile xanthogranuloma of the scalp.
Australas J Dermatol 44 : 74-75, 20032. Caputo R : Cutaneous nonhistiocytoses X in Freedberg IM, Eisen AZ,
Wolff K, Austien KF, Goldsmith LA, Kats SI, Fitspatrick TB (eds) : Fits-patrick’s Dermatology in General Medicine, ed 5. New York : McGraw Hill, 1999, Vol 2, pp1892-1902
3. Cornips EM, Cox KE, Creytens DH, Granzen B, Weber JW, Ter Laak-Poort MP : Solitary juvenile xanthogranuloma of the temporal muscle and bone penetrating the dura mater in a 2-month-old boy. J Neuro-surg Pediatrics 4 : 588-591, 2009
4. Dehner LP : Juvenile xanthogranulomas in the first two decades of life : a clinicopathologic study of 174 cases with cutaneous andextracutane-ous manifestations. Am J Surg Pathol 27 : 579-593, 2003
5. Dong H, Wang X, Liu X, Yang L, Campbell TM, Cerroni L, et al. : Rap-id-growing juvenile xanthogranuloma : The reality of a second opinion teleconsultation. Letters to the editor. Australas J Dermatol 51 : 216-217, 2010
6. Freyer DR, Kennedy R, Bostrom BC, Kohut G, Dehner LP : Juvenile xanthogranuloma : forms of systemic disease and their clinical implica-tions. J Pediatr 129 : 227-237, 1996
7. Hayashi N, Komatsu T, Komatsu T, Hiroi M, Ueno H : Juvenile xantho-
treatment. Other sites of involvement can be eye, muscle, brain or spinal cord, lung, liver, and spleen. Multiple lesions of viscer-al organ can be interfering of normal function and brain lesion can be a cause of seizure or other problem. Nakasu et al.9) re-ported intracranial solitary JXG in 2-year-old boy. Cornips et al.3) reported a 2-month-old boy with temporal muscle and bone penetrating the dura mater. In cases of systemic JXG, de-fined as the involvement of two or more visceral organs, fatal cases have been reported due to hepatic failure and thrombocy-topenia7). In our patient the lesion appeared around 16-month-old age and it was continuously growing for 8 weeks.
Observation or simple tumor excision is the treatment of choice8). Our 18-month-old girl had a solitary lesion on the scalp, but the lesion showed rapidly growing nature. Enlarging time from 1 mm to 12 mm was just 8 weeks. Therefore, it was hard to expect spontaneous regression. We chose surgical treatment. Behne and Casey1) reported that 7-month-old girl showed 1.4 cm sized ulcerated JXG with 6 weeks growing period. Numajiri et al.10) reported recurrent 21 mm-sized JXG of 9-month girl with 5 months growing duration. In case of rapid growing JXG, waiting can make cosmetic and functional problems. We per-formed extended excision to prevent recurrence and the tumor
A B CFig. 2. Photomicroscopic findings of biopsy specimen. A : Dermal infiltration of foamy and spindle-shaped histiocytes with numerous giant cells in-cluding Touton cells (H&E, original magnification ×40). B : Numerous Touton giant cells, cytoplasm within the wreath of macrophages is slightly more eosinophilic than that at the periphery (H&E, ×200). C : Immunohistochemistric study showing cytoplasmic expression of CD68 on Touton giant cells (×200).
Fig. 1. Photograph showing orange-yellow colored lesion on scalp.

273
Rapid-Growing Juvenile Xanthogranuloma | YW Park, et al.
10. Numajiri T, Nishino K, Fujiwara T, Takeda K, Sowa Y : Juvenile xantho-granuloma presenting rapid progression after curettage : a case report with clinicopathological findings. J Plast Reconstr Aesthet Surg 60 : 1248-1251, 2007
11. Stover DG, Alapati S, Regueria O, Turner C, Whitlock JA : Treatment of juvenile xanthogranuloma. Pediatr Blood Cancer 51 : 130-133, 2008
12. Zelger BW, Sidoroff A, Orchard G, Cerio R : Non-Langerhans cell his-tiocytoses. A new unifying concept. Am J Dermatopathol 18 : 490-504, 1996
granuloma presenting with unilateral prominent nodule of the eyelid : report of a case and clinicopathological findings. Jpn J Ophthalmol 48 : 435-439, 2004
8. Janssen D, Harms D : Juvenile xanthogranuloma in childhood and ado-lescence : a clinicopathologic study of 129 patients from the kiel pediat-ric tumor registry. Am J Surg Pathol 29 : 21-28, 2005
9. Nakasu S, Tsuji A, Fuse I, Hirai H : Intracranial solitary juvenile xantho-granuloma successfully treated with stereotactic radiosurgery. J Neu-rooncol 84 : 99-102, 2007

















![CD68 [KP1] - Biocare MedicalCD68 [KP1] 1. Petrovichev NN, Christyakova OV, Smirnov AV, Poltoranina VS, Rudinskaya TD. Antimacrophage monoclonal antibody D11 in the diagnosis of tumors](https://img.pdfslide.us/doc/110x75/5f0ccab67e708231d43726eb/cd68-kp1-biocare-medical-cd68-kp1-1-petrovichev-nn-christyakova-ov-smirnov.jpg)






![1 [Poster] Xanthogranuloma in the su- prasellar region: a](https://img.pdfslide.us/doc/110x75/62cdee8c07244125e8260f9d/1-poster-xanthogranuloma-in-the-su-prasellar-region-a-.jpg)



