Embed Size (px)
Citation preview

Case ReportProfound Autonomic Instability Complicated by MultipleEpisodes of Cardiac Asystole and Refractory Bradycardia ina Patient with Anti-NMDA Encephalitis
Stephanie R. Mehr,1 Roy C. Neeley,2 Melissa Wiley,1 and Avinash B. Kumar2
1Department of Anesthesiology, Vanderbilt University, Nashville, TN 37212, USA2Department of Anesthesiology, Division of Critical Care, Vanderbilt University, Nashville, TN 37212, USA
Correspondence should be addressed to Avinash B. Kumar; [email protected]
Received 14 December 2015; Revised 1 March 2016; Accepted 28 March 2016
Academic Editor: Chin-Chang Huang
Copyright © 2016 Stephanie R. Mehr et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Anti-N-methyl-d-aspartate receptor encephalitis (anti-NMDARE) is autoimmune encephalitis primarily affecting young adultsand children. First described about a decade ago, it frequently manifests as a syndrome that includes progressive behavioralchanges, psychosis, central hypoventilation, seizures, and autonomic instability. Although cardiac arrhythmias often accompanyanti-NMDARE, the need for long-term electrophysiological support is rare. We describe the case of NMDARE whose ICU coursewas complicated by progressively worsening episodes of tachyarrhythmia-bradyarrhythmia and episodes of asystole from whichshe was successfully resuscitated. Her life-threatening episodes of autonomic instability were successfully controlled only after theplacement of a permanent pacemaker during her ICU stay. She made a clinical recovery and was discharged to a skilled nursingfacility after a protracted hospital course.
1. Introduction
Anti-N-methyl-d-aspartate receptor encephalitis (anti-NMDARE) is a severe form of autoimmune encephalitisresulting from autoantibodies directed against GluN1subunits of the NMDA receptor in the central nervoussystem. Dalmau and colleagues described this condition,which primarily affects young adults and children, for thefirst time as recently as 2007 [1, 2]. Patients frequentlypresent with variable neuropsychiatric symptoms rangingfrom psychosis to seizures to catatonia, adding to thecomplexity of an early diagnosis. We obtained writtenconsent from the patient’s family to present a complex caseof anti-NMDARE with catatonia, seizures, acute respiratoryfailure, and profound autonomic instability requiringaggressive interventions including multiple rounds of CPRand cardiac pacing in the ICU. We seek to focus on the ICUcourse of illness in this complex patient with a protractedhospital course.
2. Case Report
Our patient was a 31-year-old African American femalewith a 2-3-week history of acute behavioral changes, per-sonality breakdown, sexual inappropriateness, and religiousgrandiosity. Her past medical history was significant forasthma, genital HSV, and polycystic ovarian syndrome. Shewas admitted to the psychiatry service for evaluation ofher acute behavioral changes and cognitive decline. Dur-ing her admission, she developed new onset grand-malseizures and was transferred to the neurologic intensive careunit. She continued to have frequent seizures and beganto develop worsening catatonia. The neurological workupincluded multimodal imaging and CSF studies that werepositive for GluN1 antibodies, supporting a diagnosis of anti-NMDARE. Subsequent workup including CT scans of thechest, abdomen, and pelvis, ultrasound of the pelvis, and aPET scan was negative for a tumor etiology. Our patient didnot have a tumor etiology.
Hindawi Publishing CorporationCase Reports in Neurological MedicineVolume 2016, Article ID 7967526, 5 pageshttp://dx.doi.org/10.1155/2016/7967526
2 Case Reports in Neurological Medicine
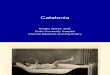
Figure 1: EKG strips with arrows outlining sudden progression ofsinus tachycardia to asystole for more than 15 seconds before anescape beat and return of sinus rhythm (spontaneously).
As the frequency of seizures increased, her mental statusdeteriorated and she was intubated for airway protection onhospital day 18. She had escalating episodes of autonomicinstability, manifested by episodes ranging from narrowcomplex tachycardia with heart rates in the 140–160 bpm tosevere bradycardia induced by vasovagal maneuvers such ascoughing, suctioning of the endotracheal tube, and defeca-tion. These episodes were initially self-limited but over sub-sequent days necessitated active pharmacologic interventionincluding combination of multiple rounds of glycopyrrolateand/or atropine and low doses of epinephrine during theepisodes.
The initial treatment of the bradycardic episodes wastargeted at reduction of vagal stimuli and triggers for brady-cardia. This included suppression of coughing episodes withintravenous fentanyl and premedication with inhaled lido-caine before endotracheal suctioning. Intermittent propofoland ketamine sedation were also attempted to decreasevasovagal triggers but no clinical efficacy was appreciated. Anearly tracheostomy (ICU day 5) was done to help alleviatethe airway irritation, decrease IV sedation, and facilitatemobilization.
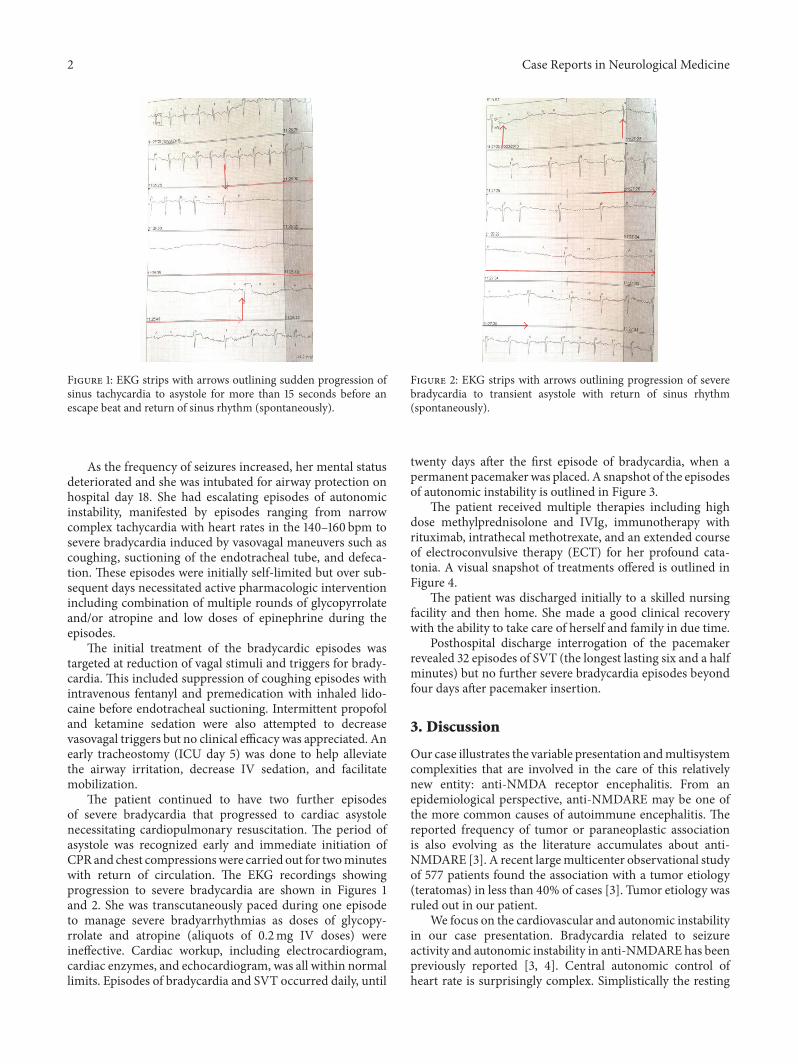
The patient continued to have two further episodesof severe bradycardia that progressed to cardiac asystolenecessitating cardiopulmonary resuscitation. The period ofasystole was recognized early and immediate initiation ofCPRand chest compressionswere carried out for twominuteswith return of circulation. The EKG recordings showingprogression to severe bradycardia are shown in Figures 1and 2. She was transcutaneously paced during one episodeto manage severe bradyarrhythmias as doses of glycopy-rrolate and atropine (aliquots of 0.2mg IV doses) wereineffective. Cardiac workup, including electrocardiogram,cardiac enzymes, and echocardiogram, was all within normallimits. Episodes of bradycardia and SVT occurred daily, until
Figure 2: EKG strips with arrows outlining progression of severebradycardia to transient asystole with return of sinus rhythm(spontaneously).
twenty days after the first episode of bradycardia, when apermanent pacemaker was placed. A snapshot of the episodesof autonomic instability is outlined in Figure 3.
The patient received multiple therapies including highdose methylprednisolone and IVIg, immunotherapy withrituximab, intrathecal methotrexate, and an extended courseof electroconvulsive therapy (ECT) for her profound cata-tonia. A visual snapshot of treatments offered is outlined inFigure 4.
The patient was discharged initially to a skilled nursingfacility and then home. She made a good clinical recoverywith the ability to take care of herself and family in due time.
Posthospital discharge interrogation of the pacemakerrevealed 32 episodes of SVT (the longest lasting six and a halfminutes) but no further severe bradycardia episodes beyondfour days after pacemaker insertion.
3. Discussion
Our case illustrates the variable presentation andmultisystemcomplexities that are involved in the care of this relativelynew entity: anti-NMDA receptor encephalitis. From anepidemiological perspective, anti-NMDARE may be one ofthe more common causes of autoimmune encephalitis. Thereported frequency of tumor or paraneoplastic associationis also evolving as the literature accumulates about anti-NMDARE [3]. A recent largemulticenter observational studyof 577 patients found the association with a tumor etiology(teratomas) in less than 40% of cases [3]. Tumor etiology wasruled out in our patient.
We focus on the cardiovascular and autonomic instabilityin our case presentation. Bradycardia related to seizureactivity and autonomic instability in anti-NMDARE has beenpreviously reported [3, 4]. Central autonomic control ofheart rate is surprisingly complex. Simplistically the resting

Case Reports in Neurological Medicine 3
10/7 10/8 10/11 10/19 10/19 10/22 10/24
Asystole at
1116
for 2m
inSe
vere b
radyca
rdia on
cough
ing
Sever
e brad
ycardia
Asystole at
2105
with co
ughing
Asystole w
ith sp
ontaneous
recover
y with
in 10 se
conds
at 22
00
Perman
ent p
acemake
r plac
ed
CPR
was
succ
essfu
l
Asystole at
2042hr
HR32
at1502
oxyg
en sa
tura
tions
dro
pped
to40
%. N
eede
d ag
gres
sive i
nter
vent
ion
Spon
tane
ous r
esol
utio
n
Reso
lved
spon
tane
ously
but
was
asso
ciat
ed w
ithdr
op in
blo
od p
ress
ure
Succ
essfu
lly ex
tern
ally
pac
ed
Pace
d fo
r HR
<50
at1015,1455
, and
1748
Addi
tiona
l epi
sode
s of b
rady
card
ia, a
t1905
hr,
2010
hr, a
nd2205
hr re
solv
ed sp
onta
neou
sly
Figure 3: Timeline of autonomic instability and interventions in the ICU.
heart rate is a function of the cardiogenic pacemaker anda balance between the bradycardiogenic parasympatheticsystem and the positive chronotropic sympathetic system.Mapping studies in animals have shown that several regionsof the telencephalon, including the insula, anterior cingulatecortices, and amygdala, are involved inmodulation of cardiacsympathetic and parasympathetic outflow. These connec-tions eventually influence the preganglionic sympathetic andparasympathetic neurons of the heart [1]. Seizure inducedactivation can result in a synchronization of cardiac auto-nomic discharges with epileptogenic activity called the “lock-step” phenomenon and induces a lethal bradyarrhythmia oreven asystole [4]. However in our case, not all bradycardiaepisodes were precipitated by vagal or epileptogenic stimuli.As the frequency of episodes escalated, several episodes ofbradycardia did not have a clear precipitating factor andmoreover these episodes were progressively more resistant topharmacological interventions.
Class I indications for temporary pacemakers in the ICUinclude asystole, symptomatic bradycardia with hypotensionand/or not responsive to atropine, and bifascicular blocks.Other common indications for temporary pacing includedrug toxicities (digoxin toxicity, beta-blocker) and hyper-kalemic bradycardia [5]. Frequently cardiologists will refrainfrom placing a pacemaker if the underlying mechanismof tachyarrhythmia-bradyarrhythmia is deemed episodicand/or related to the hyperacute phase of an illness. There
is variability in the practice of implanting permanent pace-makers in noncardiac diseases especially if the indicationis perceived to be reversible or time limited [6]. In case ofanti-NMDARE, the autonomic instability can last for severalweeks to months after the disease onset [1].
Anti-NMDARE patients frequently present to psychiatryservices as the first point of contact. The psychiatric symp-toms range from psychosis, auditory and visual hallucina-tions, aggression, anxiety, obsessive-compulsive behaviors,and depression to frank catatonia [7, 8]. The diagnosis isestablished by a positive serum or CSF sample screeningfor antibodies to the NMDA receptor subunit. Admissionbrain MRI scans have been reported as normal in as highas 70% of cases and EEG may show nonspecific slowing orslow continuous rhythmic activity during the later catatonicphase of illness [9].There are small case series that describe apattern of rhythmic delta activity (1–3Hz)with superimposedbursts of rhythmic (20–30Hz) beta activity that has beenlabeled “extreme delta brush” [10]. Multiple EEGs in ourpatient at the time of ICU admission were reviewed as deltawaves with intermixed beta activity suggestive of an extremedelta brush pattern. This pattern was noticeably absent priorto the patient’s transfer out of the ICU.
The key to an early diagnosis is often having a high indexof suspicion in this younger patient cohort with new onsetof neuropsychiatric symptoms combined with autonomicinstability with or without seizures [3]. Prognosis of patients

4 Case Reports in Neurological Medicine
Admission NeuroICU Sept 26
High dosemethylprednisolone andIVIg (5 doses)
2 doses of rituximab 2weeks apart. Last dose Oct 23
Intrathecalmethotrexate. Last doseOct 27
October to JanuaryElectroconvulsivetherapy for catatonia.Total of 31 treatmentsuntil Jan 13
Discharged to skilled nursing facility
September
October: discharged out of ICU
Figure 4: A brief snapshot of therapies and management strategies during hospitalization.
depends on early diagnosis, appropriate immunomodula-tory therapy, and, in paraneoplastic cases, complete tumorremoval. First-line immunotherapy is typically corticos-teroids, intravenous immunoglobulins, or plasma exchange.Second-line therapy in resistant cases may necessitate usingrituximab or cyclophosphamide and supportive care. Ourpatient underwent two courses of rituximab and intrathecalmethotrexate as well.
The debilitating outcomes of anti-NMDARE are primar-ily from the persistent long-term cognitive deficits. It is worthnoting that impairments in executive functions and memorycan persist for an extended period of time even after clinicalrecovery and hospital discharge. Role of theNMDA receptorsin the hippocampus is central to the postulatedmechanism ofcognitive and memory deficits. Connectivity to other areassuch as the frontal cortices may play a role in the cognitivedeficits as well [11].
Electroconvulsive therapy has been successfully tried inpatients with severe psychiatric symptoms such as catatonia.Our patient underwent immunotherapy, immunosuppres-sion, and long course of ECT prior to discharge. A schematicof the time course and treatments is outlined in Figure 3. Ourpatient had a recalcitrant course complicated by cardiores-piratory, psychiatric, and neurocognitive issues in spite of
multimodalmedical therapy until discharge from the hospitalto a skilled nursing facility.
4. Conclusion
Early recognition, aggressive cardiorespiratory support inthe ICU, and multistep pharmacological and supportive careby our multidisciplinary teams lead to a good outcome inour specific patient. Guidelines for early electrophysiologicalsupport in the setting of hemodynamic instability in anti-NMDARE are needed in the future.
Consent
Consent was obtained from patient family.
Competing Interests
The authors declare that they have no competing interests.
Acknowledgments
This study is supported by departmental funding only.

Case Reports in Neurological Medicine 5
References
[1] M. J. Titulaer, L.McCracken, I. Gabilondo et al., “Treatment andprognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study,”The Lancet Neurology, vol. 12, no. 2, pp. 157–165, 2013.
[2] J. Dalmau, A. J. Gleichman, E. G. Hughes et al., “Anti-NMDA-receptor encephalitis: case series and analysis of the effects ofantibodies,” The Lancet Neurology, vol. 7, no. 12, pp. 1091–1098,2008.
[3] L. H. Sansing, E. Tuzun, M. W. Ko, J. Baccon, D. R. Lynch, andJ. Dalmau, “A patient with encephalitis associated with NMDAreceptor antibodies,” Nature Clinical Practice Neurology, vol. 3,no. 5, pp. 291–296, 2007.
[4] J. W. Britton and E. Benarroch, “Seizures and syncope: ana-tomic basis and diagnostic considerations,” Clinical AutonomicResearch, vol. 16, no. 1, pp. 18–28, 2006.
[5] K. Jansen and L. Lagae, “Cardiac changes in epilepsy,” Seizure,vol. 19, no. 8, pp. 455–460, 2010.
[6] A. E. Epstein, J. P. Dimarco, K. A. Ellenbogen et al., “ACC/AHA/HRS 2008 guidelines for device-based therapy of cardiacrhythm abnormalities,” Heart Rhythm, vol. 5, pp. e1–e62, 2008.
[7] B. L. Sullivan, K. Bartels, and N. Hamilton, “Insertion andman-agement of temporary pacemakers,” Seminars in Cardiothoracicand Vascular Anesthesia, vol. 20, no. 1, pp. 52–62, 2016.
[8] B. Ziaeian and K. Shamsa, “Dazed, confused, and asystolic: pos-sible signs of anti–N-methyl-D-aspartate receptor encephalitis,”Texas Heart Institute Journal, vol. 42, no. 2, pp. 175–177, 2015.
[9] E. Lancaster, E. Martinez-Hernandez, and J. Dalmau, “Enceph-alitis and antibodies to synaptic and neuronal cell surfaceproteins,” Neurology, vol. 77, no. 2, pp. 179–189, 2011.
[10] S. E. Schmitt, K. Pargeon, E. S. Frechette, L. J. Hirsch, J. Dalmau,and D. Friedman, “Extreme delta brush; a unique EEG patternin adults with anti-NMDA receptor encephalitis,” Neurology,vol. 79, no. 11, pp. 1094–1100, 2012.
[11] C. Finke, U. A. Kopp, H. Pruss, J. Dalmau, K.-P.Wandinger, andC. J. Ploner, “Cognitive deficits following anti-NMDA receptorencephalitis,” Journal ofNeurology,Neurosurgery andPsychiatry,vol. 83, no. 2, pp. 195–198, 2012.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com





















![Catatonia Book[1]](https://img.pdfslide.us/doc/110x75/552321354a795934718b45b0/catatonia-book1.jpg)