-
Case ReportPerforated Closed-Loop Obstruction Secondary to
GallstoneIleus of the Transverse Colon: A Rare Entity
S. P. Carr,1 F. T. MacNamara,1,2 K. M. Muhammed,2 E.
Boyle,1,2
S. M. McHugh,1,2 P. Naughton,1,2 and A. Leahy1,2
1Royal College of Surgeons in Ireland, Dublin 2,
Ireland2Department of Surgery, Beaumont Hospital, Dublin 17,
Ireland
Correspondence should be addressed to S. P. Carr;
[email protected]
Received 7 November 2014; Accepted 11 January 2015
Academic Editor: Fernando Turégano
Copyright © 2015 S. P. Carr et al.This is an open access article
distributed under the Creative Commons Attribution License,
whichpermits unrestricted use, distribution, and reproduction in
any medium, provided the original work is properly cited.
Introduction. Gallstone ileus (GSI) of the colon is an extremely
rare entity with potentially serious complications
includingperforation. Case Presentation. An 88-year-old man
presented to the emergency department with abdominal pain and
distension.Clinical exam revealed signs of peritonism. Computed
tomography (CT) revealed GSI of the transverse colon with a
closed-looplarge bowel obstruction (LBO) and caecal perforation.
The patient underwent emergency laparotomy. A right hemicolectomy
wasperformed, the gallstone was removed, and a primary bowel
anastomosis was undertaken. A Foley catheter was sutured into
theresidual gallbladder bed to create a controlled biliary fistula.
The patient recovered well postoperatively with no complications.He
was discharged home with the Foley catheter in situ. Discussion.
Gallstone ileus is a difficult diagnosis both clinically
andradiologically with only 50% of cases being diagnosed
preoperatively. Most commonly it is associated with impaction at
theileocaecal valve and small bowel obstruction. Gallstone ileus
should also be considered as a rare but potential cause of LBO.This
isthe first reported case of caecal perforation secondary to
gallstone ileus of the transverse colon. Successful operative
managementconsisted of a one-stage procedure with right
hemicolectomy and formation of a controlled biliary fistula.
1. Introduction
Most common mechanical bowel obstruction due to agallstone
occurs at the ileocaecal valve due to the reduceddiameter and
reduced active peristalsis [1]. This has beenreported as being
associated with jejunal perforation [2, 3].
Colonic obstruction due to a gallstone occurs rarely [4, 5].The
obstructing stone needs tomeasure at least 5 cm in diam-eter or
larger than 2.5 cm with concurrent bowel pathology[6–8]. Colonic
perforation in this setting is rare with onlythree previous
reported cases of sigmoid perforation. This isthe first reported
case of perforation secondary to gallstoneileus (GSI) of the
transverse colon resulting in close-looplarge bowel obstruction
(LBO).
2. Case Report
An88-year-oldman presented to the EmergencyDepartmentin a
tertiary Irish hospital with abdominal pain anddistension
having being referred by his general practitioner. His symp-toms
had occurred three days prior to presentation. Therewas no
associated nausea or vomiting. The patient had noprevious medical
or surgical history and was on no regularmedications. He had no
previous known history of gallstones.
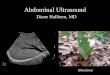
An abdominal X-ray and erect chest X-ray wererequested. His
abdominal X-ray revealed a distended largebowel with a collapsed
small bowel (Figure 1). His chestX-ray revealed free
intraperitoneal air visible under thediaphragm (Figure 2). Computed
tomography (CT) scanof the abdomen and pelvis was performed. This
revealeda close-loop LBO at the level of the transverse colon,
withcaecal distention to 10 centimetres, pneumatosis of the
caecalwall, and free intraperitoneal air and fluid consistent
withenteral perforation. The patient was subsequently scheduledfor
emergency laparotomy.
The patient underwent a vertical midline laparotomy.Theright
colon was noted to be grossly distended with caecalischemia and
perforation. A seven-centimetre gallstone was
Hindawi Publishing CorporationCase Reports in SurgeryVolume
2015, Article ID 691713, 4
pageshttp://dx.doi.org/10.1155/2015/691713
-
2 Case Reports in Surgery
Figure 1: Abdominal X-ray revealing distended large bowel with
acollapsed small bowel.
Figure 2: Chest X-ray revealing free intraperitoneal air under
thediaphragm.
noted to be causing obstruction at the proximal third of
thetransverse colon, where a cholecystocolic fistula communi-cating
between the transverse colon and the gallbladder wasidentified
(Figures 3, 4, and 5). The decision was taken toperform a right
hemicolectomy that was performed from theterminal ileum to healthy
transverse colon. A primary side-to-side stapled anastomosiswas
performed.Due to the degreeof inflammation around the gallbladder
and duodenum acomplete cholecystectomy was not performed. A
controlledfistula from the gallbladder bed to the skin was
createdvia the insertion of a Foley catheter through a
separateupper abdominal incision. Five millilitres of sterile water
wasinflated into the Foley catheter balloon, and a
purse-stringsuture was used on the gallbladder wall around the
catheterto hold the balloon in the gallbladder bed. A
completeabdominal washout was performed and two Robinson drainswere
placed via separate incisions in the abdominal cavity.
Postoperatively the patient recovered well. The
patientrecommenced oral intake day three postoperatively
andcompleted a ten-day course of intravenous
antibiotics.Hewasdischarged home with the Foley catheter in situ,
where it wassubsequently removed in surgical outpatients.
Figure 3: Photograph of the large 7 cm gallstone removed from
thetransverse colon.
Figure 4: Intraoperative picture showing 7 cm gallstone
causingobstruction at the proximal third of the transverse colon,
with acholecystocolic fistula communicating between the transverse
colonand the gallbladder.
Figure 5: Intraoperative picture showing 7 cm gallstone
beingremoved from the transverse colon.
-
Case Reports in Surgery 3
3. Discussion
It is acknowledged that GSI is a difficult diagnosis
bothclinically and radiologically with only 50% of cases
beingdiagnosed preoperatively [9]. Only 50% of patients pre-senting
with GSI have a history of gallstones or biliarypathology [10].
Considering the high mortality rate (15–18%)[1] associated with
GSI, prompt diagnosis and appropriatesurgical management are
essential for a favorable outcome.
With regard to imaging techniques, CT is recognized ashaving the
greatest diagnostic accuracy with a sensitivity of93% and
specificity of 100% [11]. In an emergency setting CTprovides a more
rapid and accurate diagnosis [12] and alsoallows for a better
determination of the degree of obstruction,its location and
visualisation of bilioenteric fistulae, and thecondition of the
adjacent bowel mucosa. Despite the numberof modern radiological
diagnostic modalities GSI involvingthe colon is such a rarity
diagnosis is still most oftenmade onlaparotomy [13].
Debate exists regarding surgical options for GSI caus-ing
uncomplicated small bowel obstruction. Enterotomyalone with removal
of the obstructing gallstone alone withexpectant management is
regarded as the most appropriatesurgical management in an emergency
setting [1, 9]. Single-stage surgery comprises a combination of
enterolithotomy,cholecystectomy, and fistulotomy. Enterotomy alone
is asso-ciated with a lower mortality rate (11.7%) when compared
tosingle-stage surgery (16.9%). With regard to
intraoperativefistula management, there is a low rate of further
compli-cations reported as a result of not performing a
fistulotomyat primary surgery with only 5% recurrence rate of
GSI.Furthermore, only 10% of patients require further surgeryfor
persistent biliary symptoms [1]. In this case, however,in order to
treat the caecal perforation a right colectomywas performed
necessitating the operative treatment of thecholecystocolic
fistula.
There is a paucity of reported cases involving
colonicperforation. In 2009, van Kerschaver et al. reported onGSI
causing necrosis and perforation of the rectosigmoidjunction. A
Hartmann’s procedure was performed to treatthe perforation and the
obstruction. A subsequent chole-cystectomy and closure of the
cholecystocolonic fistula wereplanned to be performed at the time
of restoration ofthe intestinal continuity [14]. D’Hondt and
Schoofs alsoreported on the surgical management of sigmoid
perforationsecondary to GSI in 2011 and 2010, respectively [15,
16].All of these previous cases report on GSI causing
pressure-related perforation at the site of obstruction. Our case
isunique in that we report the surgical management of aremote
perforation of the caecum as a result of GSI causingLBO.
Furthermore, octogenarians may have an incompetentileocecal valve
which would negate the evolution of a closed-loop obstruction. This
was not the case in our reportedpatient. Successful patient outcome
was achieved throughprompt preoperative diagnosis and successful
single-stagesurgery involving right hemicolectomy and controlled
biliaryfistula formation.
4. Conclusion
Gallstone ileus causing a LBO is a rare entity, and
casesinvolving colonic perforation are rarer still. Previous
reportedcases have demonstrated colonic perforation at the site
ofmechanical obstruction. We report on a closed-loop LBOleading to
remote perforation secondary to GSI at the trans-verse colon.
Successful management included right hemi-colectomy and controlled
biliary fistula formation. Gallstoneileus should be considered in
patients as a potential cause ofbowel obstruction, even without
previously known history ofgallstones.
Conflict of Interests
The authors declare that there is no conflict of
interestsregarding the publication of this paper.
References
[1] R. M. Reisner and J. R. Cohen, “Gallstone ileus: a review of
1001reported cases,” The American Surgeon, vol. 60, no. 6, pp.
441–446, 1994.
[2] L. E. Browning, J. D. Taylor, S. K. Clark, and N. D.
Karanjia,“Jejunal perforation in gallstone ileus—a case series,”
Journal ofMedical Case Reports, vol. 1, article 157, 2007.
[3] M. Gupta, S. Goyal, R. Singal, R. Goyal, S. Goyal, and A.
Mittal,“Gallstone ileus and jejunal perforation along with
gangrenousbowel in a young patient: a case report,”North American
Journalof Medical Sciences, vol. 2, no. 9, pp. 442–443, 2010.
[4] H. Fjermeros, “Gall-stone ileus. Case reports and review
of178 cases from Scandinavia and Finland,” Acta
ChirurgicaScandinavica, vol. 128, pp. 186–192, 1964.
[5] H. L. Foss and J. Summers, “Intestinal obstruction from
gall-stones,”Annals of Surgery, vol. 115, no. 5, pp. 721.b2–735.b2,
1942.
[6] G. W. Buetow and R. S. Crampton, “Gallstone ileus. A report
of23 cases,” Archives of surgery, vol. 86, pp. 504–511, 1963.
[7] P. Holm-Nielsen and P. Linnet-Jepsen, “Colon
obstructioncaused by gallstones,”Acta Chirurgica Scandinavica, vol.
107, no.1, pp. 31–40, 1954.
[8] W. V. Young Jr., “Gallstone ileus of the colon. Report of
anunusual type of colon obstruction,” Archives of Surgery, vol.
82,pp. 333–336, 1961.
[9] A. A. Ayantunde and A. Agrawal, “Gallstone ileus:
diagnosisand management,” World Journal of Surgery, vol. 31, no. 6,
pp.1294–1299, 2007.
[10] W. Kirchmayr, G. Mühlmann, M. Zitt, J. Bodner, H. Weiss,
andA. Klaus, “Gallstone ileus: rare and still controversial,”
ANZJournal of Surgery, vol. 75, no. 4, pp. 234–238, 2005.
[11] C. Y. Yu, C. C. Lin, R. Y. Shyu et al., “Value of CT in
thediagnosis and management of gallstone ileus,”World Journal
ofGastroenterology, vol. 11, no. 14, pp. 2142–2147, 2005.
[12] J.-W. Chou, C.-H. Hsu, K.-F. Liao et al., “Gallstone ileus:
reportof two cases and review of the literature,” World Journal
ofGastroenterology, vol. 13, no. 8, pp. 1295–1298, 2007.
[13] D. N. Lobo, J. C. Jobling, and T. W. Balfour, “Gallstone
ileus:diagnotic pitfalls and therapeutic successes,” Journal of
ClinicalGastroenterology, vol. 30, no. 1, pp. 72–76, 2000.
[14] O. van Kerschaver, V. van Maele, L. Vereecken, and M.
Kint,“Gallstone impacted in the rectosigmoid junction causing a
-
4 Case Reports in Surgery
biliary ileus and a sigmoid perforation,” International
Surgery,vol. 94, no. 1, pp. 63–66, 2009.
[15] M. D’Hondt, A. D’Haeninck, and F. Penninckx,
“Gallstoneileus causing perforation of the sigmoid colon,” Journal
ofGastrointestinal Surgery, vol. 15, no. 4, pp. 701–702, 2011.
[16] C. Schoofs, R. Vanheste, L. Bladt, and F. Claus,
“Cholecysto-colonic fistula complicated by gallstone impaction and
perfo-ration of the sigmoid,” JBR-BTR, vol. 93, no. 1, p. 32,
2010.
-
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation
http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing
Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume
2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing
Corporationhttp://www.hindawi.com
![Choledocholithiasis, Ascending Cholangitis, and Gallstone ... · bilirubinate to form biliary sludge, which can aggregate eventually into a gallbladder stone [10]. Black pigment stones](https://img.pdfslide.us/doc/110x75/5e04b56d64882534e3400732/choledocholithiasis-ascending-cholangitis-and-gallstone-bilirubinate-to-form.jpg)