Embed Size (px)
Citation preview

Clinical Radiology (1990) 42, 57-59
Case Report: Percutaneous Supra-aortic Angioplasty in High Risk Coronary Patient S. S H A R M A , U. K A U L * , N. M I S R A a n d M. R A J A N I
Departments o f Radiodiagnosis and * Cardiology, Cardiothoracic and Neurosciences Centre, All India Institute o f Medical Sciences, New Delhi, India
a
We have performed percutaneous angioplasty of the in- nominate and carotid arterial stenoses in a high risk patient with proximal disease involving the vessels arising from the aortic arch and seriously limiting blood flow to all four cerebral vessels. The patient also had severe left main and triple vessel coronary artery disease. The role of supra- aortic angioplasty in this clinical setting is discussed.
Rapid technica l a d v a n c e s a n d the ava i l ab i l i ty o f m a n y favourable shor t a n d l o n g t e rm resul ts have m a d e pe rcu taneous t r a n s l u m i n a l a n g i o p l a s t y a v iable al ternat ive to r econs t ruc t ive vascu la r surgery in the m a n a g e m e n t o f pa t i en t s wi th i leo- femora l , popl i tea l , subclavian, rena l a n d c o r o n a r y ar te r ia l s tenoses (Tegt- meyer et al., 1984; K r e p e l et al., 1985; R o u b i n et al., 1986; Kachel et al., 1987; B r o w n et al., 1988; V a n A n d e l et al., 1988). Recent ly , a n g i o p l a s t y has also b e e n ex tended to the m a n a g e m e n t o f i so la ted , discrete, ca ro t id a r te r ia l ste-
n o s e s wi th e n c o u r a g i n g resul ts ( B r o c k e n h e i m e r a n d Mathias , 1983; Wiggl i a n d Gra tz l , 1983; F re i t ag et al., 1986; Tsai et al., 1986; K a c h e l et al., 1987).
We have recent ly e n c o u n t e r e d a pa t i en t wi th wide- spread, severe, p r o x i m a l disease c o m p r o m i s i n g b l o o d flow to all f ou r cerebra l vessels. The pa t i en t also had symptomat ic severe left m a i n a n d t r ip le vessel c o r o n a r y artery disease. W e r epo r t ou r exper ience wi th sup ra - aortic a ng iop l a s ty in this cl inical set t ing.
CASE R E P O R T
A 48-year-old male patient with a history of longstanding stable angina pectoris was admitted with accelerating angina. Upon present- ation, there was class III (New York Heart Association) exertional angina. In addition to his cardiac symptoms, he was also found to have had recurrent syncope suggesting vertebro-basilar insufficiency of 6 months duration and multiple episodes of reversible ischaemic neuro- logical defects of 2 years duration. These ischaemic neurological episodes were in the form of transient loss of power in the left half of the body accompanied by unsteadiness of gait. Twenty-four hour Holter monitoring during which the patient had episodic giddiness did not reveal any cardiac arrhythmia. Risk factors for premature atherosclero- sis included a past history of smoking 15-20 cigarettes per day for the last 20 years and non-familial hyperlipidaemia (total cholesterol--340 rag/%; LDL cholesterol--260 mg/%, HDL cholesterol--30 mg/%; serum triglycerides--270 mg/%).
Physical examination revealed feeble pulses in the right arm and absent pulses in the left arm; a blood pressure of 70 mmHg (systolic) in right arm, unrecordable in left arm; and 130/80 mmHg in the lower limbs. There were bilateral carotid bruits. The patient had no ischaemic symptoms in the arms. The remainder of the examination, including cardiopulmonary and neurological system, was unremarkable.
Coronary angiography using the standard Judkin's technique from the right femoral artery, revealed a 60% proximal left main stenosis, occlusion of the left anterior descending artery after the origin of first
Correspondence to: Dr Sanjiv Sharma, Department of Radio- diagnosis, Cath Laboratory, Cardiothoracic Centre, All India Institute of Medical Sciences, Ansari Nagar, New Dellii-110029, India.
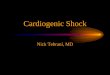
diagonal branch with retrograde filling by collaterals from the circum- flex and right coronary arteries, a long 30% proximal circumflex stenosis, and diffuse disease of the proximal right coronary artery. Digital subtraction angiography of the aortic arch and neck vessels revealed a 90% stenosis at the origin of the innominate artery with post- stenotic dilatation, a 70% left carotid artery stenosis at its origin, and complete occlusion of the proximal left subclavian artery (Fig. I). In addition, there was 30 % narrowing of the right internal carotid artery at its origin. The intracranial branches of the carotid arteries were normal. The distal left subclavian artery was filling via the left vertebral artery in the late frames of the angiogram (subclavian-steal phenomenon).
Percutaneous balloon dilatation of the innominate, left carotid, and left subclavian arteries was attempted prior to coronary bypass surgery in order to obviate the problems of compromised cerebrovascular status during and after the coronary bypass surgery. Since angioplasty in such patients carries a high risk due to the fragile cardiac status, we were prepared for emergency coronary bypass surgery during the angioplasty procedure.
THE P R O C E D U R E
Af te r c ross ing the left c a ro t id o b s t r u c t i o n wi th a 5 F r e n c h femora l -ce rebra l ca the te r (Cord i s Corp . , M i a m i , F lor ida) , a t r ans - s t enof i c p ressure g r a d i e n t o f 40 m m H g
Fig. 1 - Intra-arterial digital subtraction angiogram of the aortic root in the left anterior oblique view showing tight stenoses at the origin of innominate and left carotid arteries, and complete occlusion of subclavian artery soon ~fter its origin.
5 8 CLINICAL RADIOLOGY
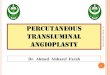
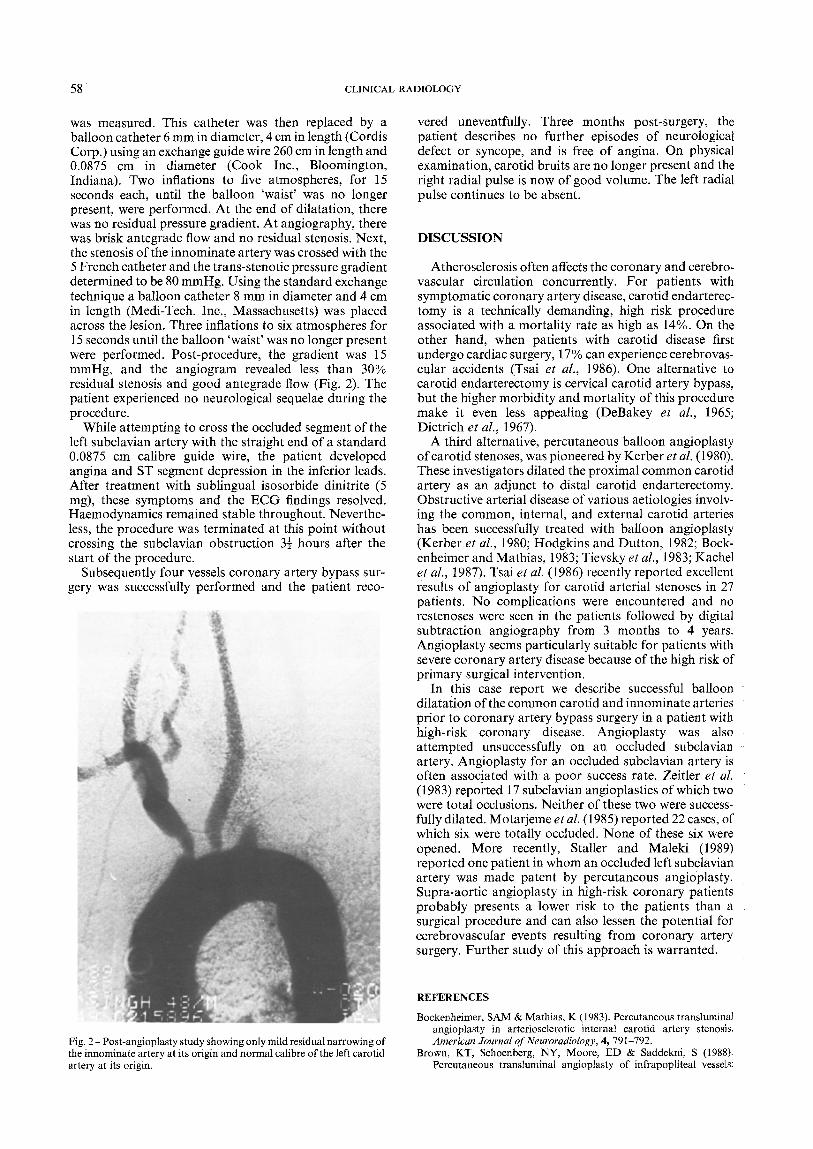
was measured. This catheter was then replaced by a balloon catheter 6 mm in diameter, 4 cm in length (Cordis Corp.) using an exchange guide wire 260 cm in length and 0.0875 cm in diameter (Cook Inc., Bloomington, Indiana). Two inflations to five atmospheres, for 15 seconds each, until the balloon 'waist' was no longer present, were performed. At the end of dilatation, there was no residual pressure gradient. At angiography, there was brisk antegrade flow and no residual stenosis. Next, the stenosis of the innominate artery was crossed with the 5 French catheter and the trans-stenotic pressure gradient determined to be 80 mmHg. Using the standard exchange technique a balloon catheter 8 mm in diameter and 4 cm in length (Medi-Tech. Inc., Massachusetts) was placed across the lesion. Three inflations to six atmospheres for 15 seconds until the balloon 'waist' was no longer present were performed. Post-procedure, the gradient was 15 mmHg, and the angiogram revealed less than 30% residual stenosis and good antegrade flow (Fig. 2). The patient experienced no neurological sequelae during the procedure.
While attempting to cross the occluded segment of the left subclavian artery with the straight end of a standard 0.0875 cm calibre guide wire, the patient developed angina and ST segment depression in the inferior leads. After treatment with sublingual isosorbide dinitrite (5 mg), these symptoms and the ECG findings resolved. Haemodynamics remained stable throughout. Neverthe- less, the procedure was terminated at this point without crossing the subclavian obstruction 3½ hours after the start of the procedure.
Subsequently four vessels coronary artery bypass sur- gery was successfully performed and the patient reco-
Fig. 2 - Post-angioplasty study showing only mild residual narrowing of the innominate artery at its origin and normal calibre of the left carotid artery at its origin.
vered uneventfully. Three months post-surgery, the patient describes no further episodes of neurological defect or syncope, and is free of angina. On physical examination, carotid bruits are no longer present and the right radial pulse is now of good volume. The left radial pulse continues to be absent.
DISCUSSION
Atherosclerosis often affects the coronary and cerebro- vascular circulation concurrently. For patients with symptomatic coronary artery disease, carotid endarterec- tomy is a technically demanding, high risk procedure associated with a mortality rate as high as 14%. On the other hand, when patients with carotid disease first undergo cardiac surgery, l 7% can experience cerebrovas- cular accidents (Tsai et al., 1986). One alternative to carotid endarterectomy is cervical carotid artery bypass, but the higher morbidity and mortality of this procedure make it even less appealing (DeBakey et al., 1965; Dietrich et al., 1967).
A third alternative, percutaneous balloon angioplasty of carotid stenoses, was pioneered by Kerber et al. (1980). These investigators dilated the proximal common carotid artery as an adjunct to distal carotid endarterectomy. Obstructive arterial disease of various aetiologies involv- ing the common, internal, and external carotid arteries has been successfully treated with balloon angioplasty (Kerber et al., 1980; Hodgkins and Dutton, 1982; Bock- enheimer and Mathias, 1983; Tievsky et al., 1983; Kachel et al., 1987). Tsai et al. (1986) recently reported excellent results of angioplasty for carotid arterial stenoses in 27 patients. No complications were encountered and no restenoses were seen in the patients followed by digital subtraction angiography from 3 months to 4 years. Angioplasty seems particularly suitable for patients vCith severe coronary artery disease because of the high risk of primary surgical intervention.
In this case report we describe successful balloon dilatation of the common carotid and innominate arteries prior to coronary artery bypass surgery in a patient with high-risk coronary disease. Angioplasty was also attempted unsuccessfully on an occluded subclavian artery. Angioplasty for an occluded subclavian artery is often associated with a poor success rate. Zeitler et al. (1983) reported 17 subclavian angioplasties of which two were total occlusions. Neither of these two were success- fully dilated. Motarjeme et al. (1985) reported 22 cases, of which six were totally occluded. None of these six were opened. More recently, Staller and Maleki (1989) reported one patient in whom an occluded left subclavian artery was made patent by percutaneous angioplasty. Supra-aortic angioplasty in high-risk coronary patients probably presents a lower risk to the patients than a surgical procedure and can also lessen the potential for cerebrovascular events resulting from coronary artery surgery. Further study of this approach is warranted.
REFERENCES
Bockenheimer, SAM & Mathias, K (1983). Percutaneous transluminal angioplasty in arteriosclerotic internal carotid artery stenosis. American Journal of Neuroradiology, 4, 791-792.
Brown, KT, Schoenberg, NY, Moore, ED & Saddekni, S (1988). Percutaneous transluminal angioplasty of infrapopliteal vessels:

SUPRA-AORTIC ANGIOPLASTY IN PRESENCE OF CORONARY DISEASE 59
preliminary results and technical considerations. Radiology, 169, 75- 78.
DeBakey, ME, Crawford, ES, Cooley, DA, Morris, GC, Garrett, E & Fields, WS (1965). Cerebral arterial insufficiency--one to 11 years result following cerebral reconstructive operation. American Journal of Surgery, 161, 921 925.
Dietrich, EB, Garrett, HE, Ameriso, J, Crawford, ES, El-Bayer, M & DeBakey, ME (1967). Occlusive disease of the common carotid and subclavian arteries treated by carotid subclavian bypass. American Journal of Surgery, 114, 800-808.
Freitag, G, Freitag, J, Koch, RD & Wagemann, W (1986). Percutaneous transluminal angioplasty of carotid artery stenosis. Neuroradiology, 28, i26-127.
Hodgkins, GN & Dutton, JW (1982). Subclavian and carotid angio- plasties for Takayasu's arteritis. Journal of the Canadian Association of Radiology, 33, 205-207.
Kachel, R, Endert, G, Basche, S, Grossmann, K & Glaser, FH (1987). Percutaneous transluminal angioplasty (dilatation) of carotid, ver- tebral and innominate artery stenosis. Cardiovascular and Interven- tional Radiology, 10, 142-146.
Kerber0 CS, Cromwell, LD & Lehden, DL (1980). Catheter dilatation of proximal carotid stenosis during distal bifurcation endarterectomy. American Journal of Neuroradiology, 1, 348-349.
Krepel, VM, VanAndel, GJ, VanErp, WFM & Breslau, PJ (1985). Percutaneous transluminal angioplasty of the femopopliteal artery: Initial and long term results. Radiology, 156, 325-328.
Motarjeme, A, Keifer, J, Zuska, A & Nabawi, P (1985). Percutaneous
transluminal angioplasty for treatment of subclavian steal. Radio- logy, 155, 611-613.
Roubin, GS, Gruntzig, AR & Casarella, WJ (1986). Percutaneous coronary angioplasty: technique, indications, and results. Cardio- vascular and Interventional Radiology, 9, 261-272.
Staller, BJ & Maleki, M (1989). Percutaneous transluminal angioplasty for innominate artery stenosis and total occlusion of subclavian artery in Takayasu's type arteritis. Catheterization and Cardiovascu- lar Diagnosis, 16, 91-94.
Tegtmeyer, CJ, Kofler, TJ & Ayers, CA (1984). Renal angioplasty: current status. American Journal of Radiology, 142, 17-21.
Tievsky, AL, Druy, EM & Mardiat, JG (1983). Transluminal angio- plasty in post surgical stenosis of the extracranial carotid artery. American Journal of Neuroradiology, 4, 800-802.
Tsai, F, Matovich, V, Heishima, G, Shah, DC, Mehringer, CM & Tiu G et al. (1986). Percutaneous transluminal angioplasty of the carotid artery. American Journal of Neuroradiology, 7, 349-358.
VanAndel, GJ, VanErp, WFM, Krepel, VM & Breslau, PJ (1988). Percutaneous transluminal dilatation of the iliac artery: long term results. Radiology, 156, 321-323.
Wiggli, U & Gratzl D (1983). Transluminal angioplasty of stenotic carotid arteries. Case reports and protocol. American Journal of Neuroradiology, 4, 793-795.
Zeitler, E, Berger, G & Schmitt-Ruth, R (1983). Percutaneous translu- minal angioplasty of the supra aortic arteries In: Dotter, CT, Gruntzig, W, Schoop, W & Zeitler E. (eds) Percutaneous Translumi- nal Angioplasty. Springer-Verlag, Berlin, pp. 245-262.