Embed Size (px)
Citation preview
Int J Clin Exp Med 2018;11(4):4193-4202www.ijcem.com /ISSN:1940-5901/IJCEM0062085
Case ReportPediatric atypical neuroblastoma: three cases report and a literature review
Ling Liu1, Yang Li2,3, Xi-Lin Xiong2,3, Ri-Ling Chen1, Hai-Xia Guo2,3, Hong-Gui Xu2,3, Jian-Pei Fang2,3, Hong-Man Xue2,3
1Department of Pediatric, Affiliated Hospital of Guangdong Medical University, people’s Avenue South 57 of Zhan Jiang 524000, Guangdong, China; 2Guangdong Provincial Key Laboratory of Malignant Tumor Epigenetics and Gene Regulation, 3Department of Pediatric Hematology/Oncology, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Along The West Road 107 of Guangzhou 510120, Guangdong, China
Received February 5, 2016; Accepted January 25, 2018; Epub April 15, 2018; Published April 30, 2018
Abstract: Atypical neuroblastoma (NB) refers to the primary onset of NB without a detectable mass in common sites, but in bone marrow or/and other metastasis parts. For a better elucidation and defining atypical NB, our experiences in three unusual cases of Chinese atypical NB are reported on this paper. Clinically, the first case had no other parts of the tumor infiltration in addition to bone marrow, but the second and third case was presented with the metastasis sites of NB including both bone marrow and bone. Usually in China, treatments of radiotherapy, surgery and hematopoietic stem cell transplantation (HSCT) may not suitable for patients with atypical NB, likely due to the absent of visible solid mass and sometimes without the drug approval of the conditioning regimen like mel-phalan, so, aggressive chemotherapy seems to be the effective first-line choice. Our experiences show that atypical NB might be associated with a worse outcome than typical NB despite extremely aggressive treatments. Several important aspects of diagnosis and management of atypical NB are highlighted in the following three case reports.
Keywords: Atypical, neuroblastoma, child
Introduction
Neuroblastoma (NB) deriving from neural crest cells that destined for anywhere in the body associated with sympathetic nerve system [1, 2], is the most common extracranial tumor diagnosed as young children, and account for 8-10% of all childhood cancers [3]. A general consensus about management of NB includes multimodal combination therapy such as che-motherapy, radiotherapy, surgery and hemato-poietic stem cell transplantation (HSCT). Mo- st, some NB eventually develops progressive disease and confers overall poor prognosis, more than 50% of NB patients still die of this disease [4].
Atypical NB is a rare tumor followed by an aty- pical course and variable presentation, to the best of our knowledge, this is the first three cases report of atypical NB on a single center. Till now, there is no literature describing the significant differences including the clinical pro-
files, laboratory findings, biologic prognostic factors, treatment and outcome between NB and atypical NB, therefore the purpose of th- is study is to contribute to a better delineation of the heterogeneous characteristics of this rare entity and figures prominently in distingui- shing between the diagnoses of NB and atypical NB.
Case report
Case 1
The first case, a 4-year-old male presented with a primary complaint about pain in left knee joint and pale over a 7-month period and low fever for two days (Table 1). A physical examination showed moderate anemia appearance, the bean-size cervical lymph nodes, mild hepato-splenomegaly. There was mild tenderness of left knee on palpation. The abdomen was so- ft and no additional mass was palpable. The rest of the physical examination was not spe-cial. Laboratory tested results of case 1 was
Pediatric atypical neuroblastoma: three cases report
4194 Int J Clin Exp Med 2018;11(4):4193-4202
Table 1. Summary of the clinical filesCase 1 Case 2 Case 3
Gender Male Male MaleAge (years) 4 3 3Metastasis Bone marrow Bone marrow and bone Bone marrow and boneClinical Pain in left knee joint and pale Recurrent bilateral knee pain with fever Pain in left hip joint, fever and paleNeuroblastoma cell % in bone marrow 67 41 56.5MYCN - - -Disease status of primary at end of induction chemotherapy Complete remission Partial remission Partial remission
Pediatric atypical neuroblastoma: three cases report
4195 Int J Clin Exp Med 2018;11(4):4193-4202
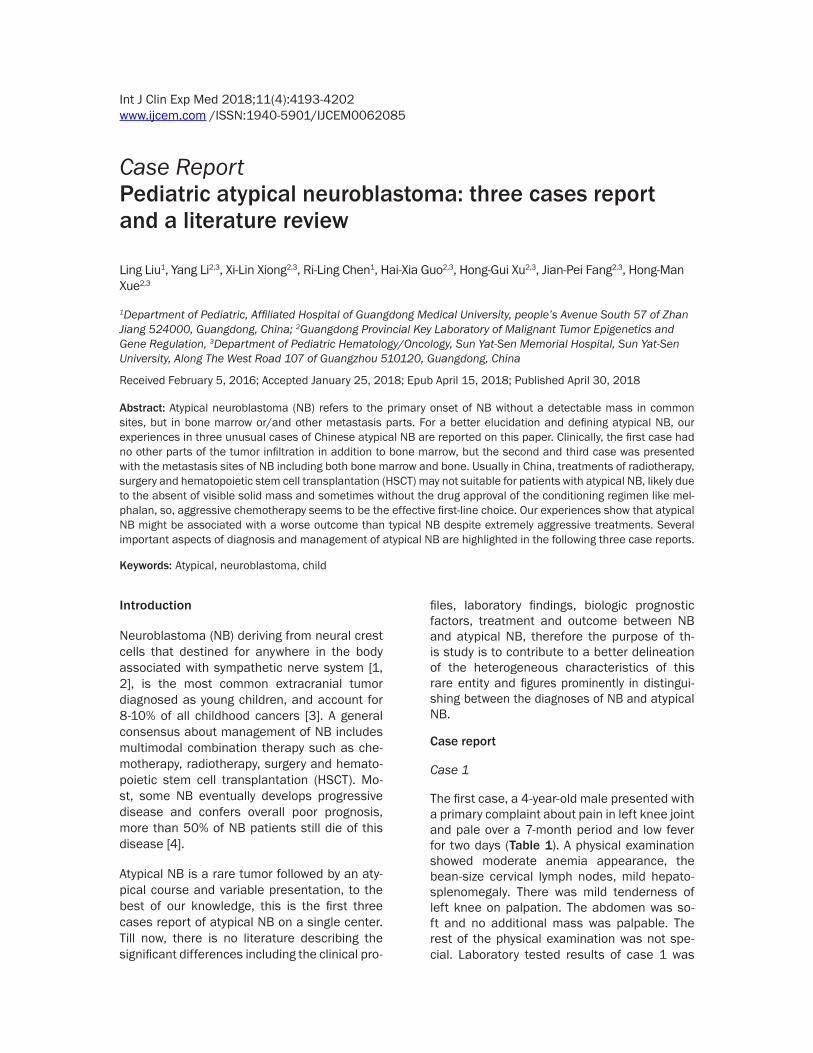
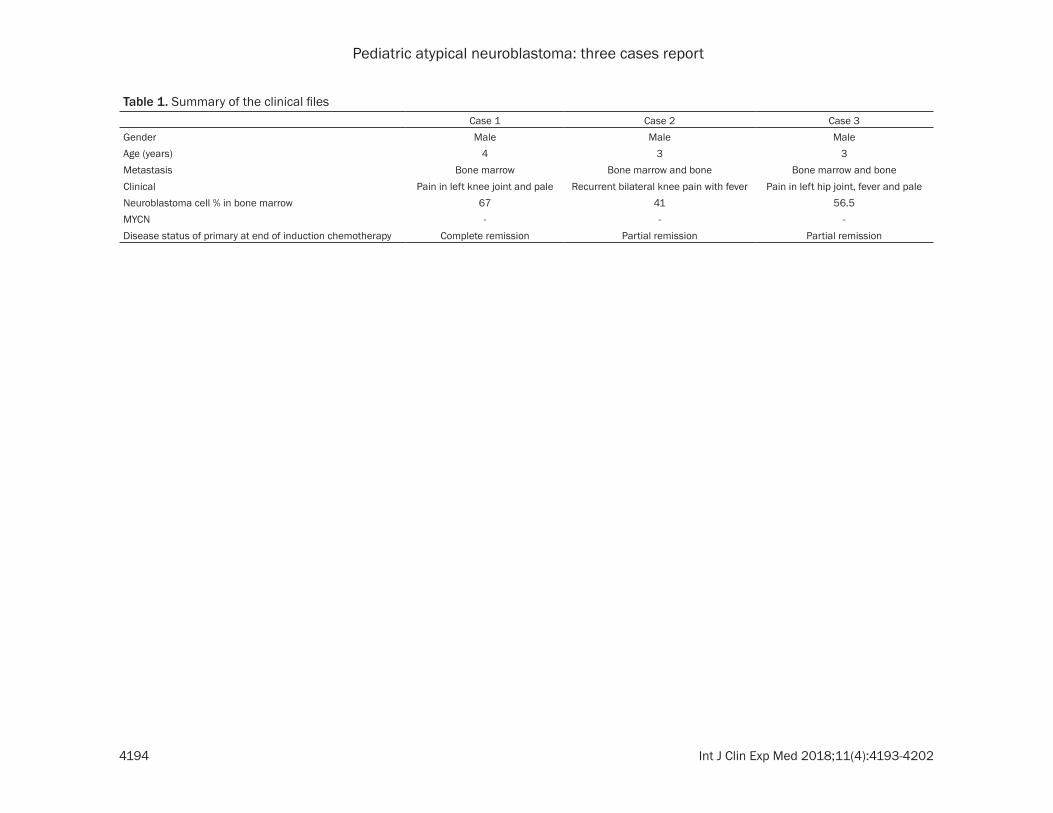
≤ 10). Furthermore, blood chemistry tests, which included aspartate aminotransferase (AST), alanine aminotransferase (ALT), lactate dehydrogenase (LDH), creatinine, alpha feto-protein (AFP) and carcinoembryonic antigen (CEA), were all normal. Meanwhile, bone mar-row smears (Figure 1A, 1B) presented that the ratio of characteristic NB cells was 67%, the- se cells typically forming Homer-Wright rosett- es. Genetic testing using fluorescence in situ hybridization presented that absence of MY- CN amplification in the metastatic tumor cells in bone marrow. Chest and abdomen comput- ed tomography (CT) scan (Figure 2A) reveal- ed splenomegaly and multiple small lymph no- des enlargement in the armpits and retroperi- toneum, no infiltration of the lungs, mediasti-num and bilateral adrenalectomy. Total body
Figure 1. Bone marrow morphology in case 1. A: Before the start of the treatment, the ratio of characteristic NB cells was 67% (wright’s stain × 100). B: Before chemotherapy begins, the neoplastic cells with cell bodies varied in size, scant cytoplasm stained with blue and enlarged nuclei, typically formed Homer-Wright rosettes (wright’s stain × 1000). C and D: From the fourth course, the bone marrow smear revealed complete alleviation.
Figure 2. Image results in case 1. A: The chest and abdomen CT in case 1 initially showed splenomegaly and meta-static lymph node enlargement in the armpits and retroperitoneum, but no pathology in the lungs, mediastinum and bilateral adrenalectomy. B: In case 1, PET/CT obtained in the fourth course documented tumor activity was inhibited apparently and no additional bone involvement.
Table 2. The course of induction chemo-therapyCourse 1 2 3 4 5 6 7 8 9Protocol C C P C P C P C C
A A V A V A V T TV V P V P V P
CAV: Cyclophosphamide + Pirarubicin + Vincristine, PVP: Cisplatin + Etoposide, CT: Cyclophosphamide + Topotecan.
as follows: white blood cell count, 5.42 × 109/L (normal range, 5-11 × 109/L), decreased hemoglobin, 97 g/L (normal range, 110-130 g/L), platelet count, 389 × 109/L (normal ran- ge, 100-300 × 109/L), increased serum NSE, 274.2 ng/ml (normal range ≤ 16.3 ng/ml), increased Urine VMA/Cr, 150 (normal range
Pediatric atypical neuroblastoma: three cases report
4196 Int J Clin Exp Med 2018;11(4):4193-4202
skeletal scintigraphy and abdominal ultrasou- nd both showed no pathologic findings. X-ray film of the chest showed bronchopneumonia and no mediastinum mass.
Treatment was limited to nine courses of che-motherapy with high-risk NB induction proto- col (SMHPO-N2011) described (Tables 2 and 3). Peripheral blood minimal residual disease (MRD) analyzed by flow cytometry detecting CD45-/CD56+/GD2+ tumor cells starting from the seventh course. If MRD > 1 × 10-4 it may be regarded as positive.
After two courses of chemotherapy, pain in left knee was in remission successfully, and super-ficial lymph nodes, the liver and the spleen were not palpable. From the fourth course, urine VMA (Table 4) continuously to be within normal limits, and the bone marrow smear (Figure 1C, 1D) revealed complete alleviation. In the fifth course, serum NSE (Table 4) returned to normality, but from the sixth course, serum NSE back to positive. In the fourth course, a reevaluation positron emission computed tomo- graphy (PET/CT) scan (Figure 2B) showed a complete remission that tumor activity was inhibited without increased metabolism areas, and normal imaging in other parts of the body. In the seventh course, MRD of NB (Table 4) in peripheral blood was found to be positive (3.32 × 10-4), and from the eighth course the MRD continued to be negative (0.51 × 10-4). Ultima- tely, the patient completed the whole induction chemotherapy and achieved a complete remis-sion, but he had relapsed after 6-months fol-low-up due to lack of consolidation chemother-apy for economic reason. This patient achieved a complete remission again after re-adminis-tered chemotherapy.
and swelling, however, left knee joint tender-ness was noted. His laboratory test results were as follows: white blood cell count of 5.04 × 109/L, decreased hemoglobin of 90 g/L, decreased platelet count of 46 × 109/L, increased serum NSE of 234.4 ng/ml, incre- ased urine VMA/Cr of 28.5. The bone marrow aspirate (Figure 3A, 3B) revealed 41% typical NB cells with arranged in Homer-Wright rosettes. The MYCN amplification was nega-tive. The chest and abdomen CT scans (Figure 4A) revealed augmented liver and multiple small lymph nodes enlargement in the armpits, no infiltration of the lungs, mediastinum and re- troperitoneal. The infiltration in the left distal femur and the left proximal tibia, joint effusion in left knee were noted with magnetic reso-nance imaging (MRI) of the bilateral knee. PET /CT (Figure 4B) dated-September 2011 was obtained and it showed the diffusely increas- ed metabolism of the bone marrow and bilat-eral femurs, enlargement of spleen and lymph nodes in bilateral neck, armpit, mesentery and pelvic cavity, compatible with tumor in- filtration.
Nine courses of chemotherapy with protocol SMHPO-N2011 were performed. Peripheral bl- ood MRD of NB was analyzed starting from the sixth course.
After one course of chemotherapy, ostealgia was complete in remission, from the fourth course, the bone marrow smear (Figure 3C, 3D) revealed complete alleviation, from the sixth course urine VMA (Table 4) got normal. Serum NSE (Table 4) drastically decreased to normal in the fourth course, while followed by a strong, continuous elevation from the seventh course. In the fifth course, PET/CT (Figure 4C) dis-closed multiple residual tumor lesions th-
Table 3. The composition and usage of protocolProtocol name Dosage and usage DaysCAV Cyclophosphamide (CTX) 1.2 g/m2.d, iv drip d1-d2 Pirarubicin (THP) 25 mg/m2.d, iv drip d1-d3 Vincristine (VCR) 0.022 mg/kg.d (or 0.67 mg/m2.d), iv drip d1-d3PVP Cisplatinum (DDP) 50 mg/m2.d, iv drip d1-d4 Etoposide (VP16) 200 mg/m2.d, iv drip d1-d3CT CTX 1.2 g/m2.d, iv drip d1-d2 Topotecan 2 mg/m2.d, iv drip d1-d3
Case 2
The second case, a 3-year-old male was referred to our clinic for a workup, his chief complaint was, “recurrent bi- lateral knee pain with fever for one month.” On exami-nation, the patient suffered from moderate anemia, and the neck examination was positive for bean-size lym- ph nodes. His abdomen was soft, no mass was palpab- le. Joints were no redness
Pediatric atypical neuroblastoma: three cases report
4197 Int J Clin Exp Med 2018;11(4):4193-4202
Table 4. The values of serum NSE, urine VMA and MRD in peripheral blood
CourseNSE (ng/ml) VMA/Cr VMA (mg/24 H) MRD (× 10-4)
Case 1 Case 2 Case 3 Case 1 Case 2 Case 3 Case 1 Case 2 Case 3 Case 1 Case 21 274.2 234.4 724.4 150 28.5 148 - - 100 - -2 32.5 22.7 20.9 187 - 5.5 - 28.9 - - -3 17.5 22.7 21.1 - - 15.3 - 23.8 - - -4 - 12.5 16.3 - - 15 12.1 18 - - -5 11.2 14 53 - - 9.3 - 21 - - -6 27.8 8.2 17.6 - - 10.8 15.3 12.6 - - 0.737 15 19.8 43.1 - - 10.3 - 13.8 - 3.32 0.318 - 20.6 16.6 - 10.6 9.1 2.5 - - 0.72 -9 75.4 20.7 16.9 - - 25.3 8.7 10.1 - 0.51 8.36Note: NSE (normal range ≤ 16.3 ng/ml); VMA/Cr (normal range ≤ 10); VMA (normal range: 5~15 mg); MRD (normal range < 1 × 10-4).
at characterized by multiple osteolytic bo- ny destruction and increased metabolism of the bilateral humerus, the sternum, the spine vertebral and accessories, the pelvis and the femurs. The last PET/CT scan (Figure 4D), per-formed after the entire induction chemothera-py, also showed bone invasion without remis-sion in accord with the former (Figure 4C). In the sixth course, NB peripheral blood negative MRD value (Table 4) was 0.73 × 10-4, unfortu-nately MRD became positive (8.36 × 10-4) in the ninth course. Eventually, the second case achieved partial remission, and then he ab- andoned subsequent treatment also for eco-nomic reason.
Case 3
The third case, a 3-year-old male with pain in left hip joint for two months history, repeated fever and pale for one month was referred to our hospital for a workup (Table 1). On exa- mination, moderate anemia was observed. On palpation, there was no superficial lymphade-nopathy, the abdomen was flat and no mass
was palpable. The rest of the physical exami- nation revealed no abnormalities. Laboratory findings of case 3 showed that white blood ce- ll count was 6.97 × 109/L, decreased hemog- lobin of 79 g/L, platelet count of 244 × 109/L, increased serum NSE of 724.4 ng/ml, increas- ed urine VMA/Cr of 148. Simultaneously, bo- ne marrow smears (Figure 5A, 5B) showed the ratio of characteristic NB cells was 56.5%. The MYCN amplification was negative. MRI of lu- mbar and pelvis revealed the significant infil- tration in lumbar vertebral body, sacrum, bilat-eral iliac, ischium, pubis and bilateral femo- ral head. Abdominal ultrasound found multiple gallstones without other solid mass. PET/CT (Figure 6A) showed the diffusely increased metabolism of multiple bones with osteolytic lesion, increased metabolism of spleen and lymph nodes in left pelvic wall, all consistent with bone marrow involvement.
The nine courses of intensive chemotherapy with protocol SMHPO-N2011 were perform- ed, after one course of chemotherapy, osteal-gia was complete in remission, from the fifth
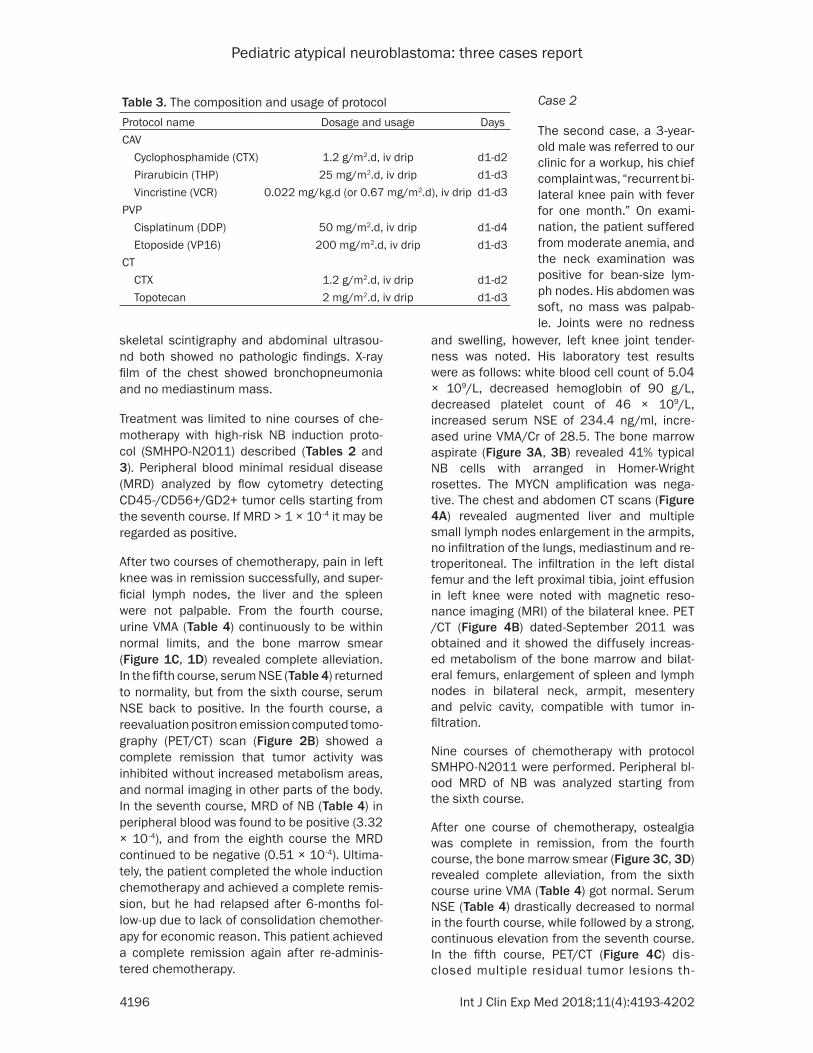
Figure 3. Bone marrow morphology in case 2. A: Before chemotherapy begins the ratio of characteristic NB cells was 41% (wright’s stain × 100). B: Before chemotherapy begins, the neoplastic cells with cell bodies varied in size, scant cytoplasm stained with blue and enlarged nuclei, typically formed Homer-Wright rosettes (wright’s stain × 1000). C and D: From the fourth course, the bone marrow smear revealed complete alleviation.
Pediatric atypical neuroblastoma: three cases report
4198 Int J Clin Exp Med 2018;11(4):4193-4202
course, the bone marrow smear (Figure 5C, 5D) revealed complete remission. In the fourth course, serum NSE (Table 4) dropped to nor-mality, but rapidly rising from the fifth course, in the second course, urine VMA (Table 4) got normal, but from the third course, urine VMA turned to be positive. In the third and the la- st course, PET/CT (Figure 6B, 6C) showed a complete response in the multiple bone invasion lesions and lymph nodes, enlarged spleen but with normal metabolism. Finally, the
third case achieved partial remission after the entire induction chemotherapy, and he experi-ences consolidation chemotherapy at present.
Discussion
Previously reported cases of atypical NB were rare. On the basis of our retrospective literatu- re review showing that there are only 12 case reports about the atypical NB [5-9]. Darren Salmi and colleagues described a 20-month-old female with unknown primary site detect-
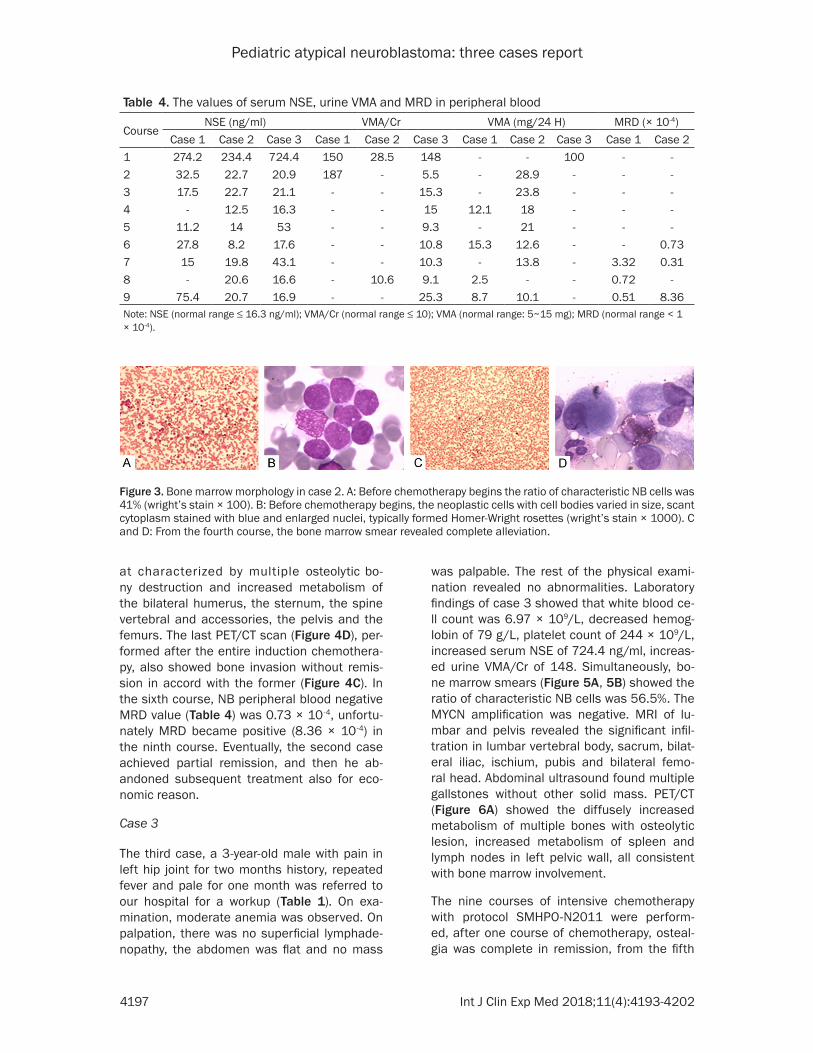
Figure 4. Image results in case 2. (A) The chest and abdomen CT in case 2 initially showed augmented liver and multiple small lymph nodes enlargement in the armpits, no infiltration of the lungs, mediastinum and retroperito-neal. (B) PET/CT in case 2 initially it showed the diffusely increased metabolism in the bone marrow and bilateral femurs, enlargement of spleen and lymph nodes in bilateral neck, armpit, mesentery and pelvic cavity, compatible with tumor infiltration. (C) In case 2, PET/CT in the fifth course disclosed that the residual bone metastases with the increased density and metabolism of bilateral femur, sternum, pelvis, spinal vertebral body and accessories. (D) In case 2, the review of PET/CT in the ninth course was similar to the former (C), and bone involvement no remission.
Pediatric atypical neuroblastoma: three cases report
4199 Int J Clin Exp Med 2018;11(4):4193-4202
ed based on imaging studies included CT and I123 MIBG scan [6]. Similarly, Ki Woong Sung reported that in 143 NB two patients originat- ed from unknown primary sites in 1.4% of cas- es [8]. In these cases it remains unclear where neoplasms originated after patients had been diagnosed as NB. Consequently, the primary occult tumor may not large enough for detec-tion based on imaging studies. Furthermore,
literature review has revealed that the stand- ard diagnostic criterion and clear definition are still enigmatic. According to the special char- acteristics of these cases of pediatric NB de- scribed here, we try to define the atypical NB as the primary onset of NB without a detect-able mass in common sites based on imag- ing studies, but in bone marrow or/and other metastasis parts.
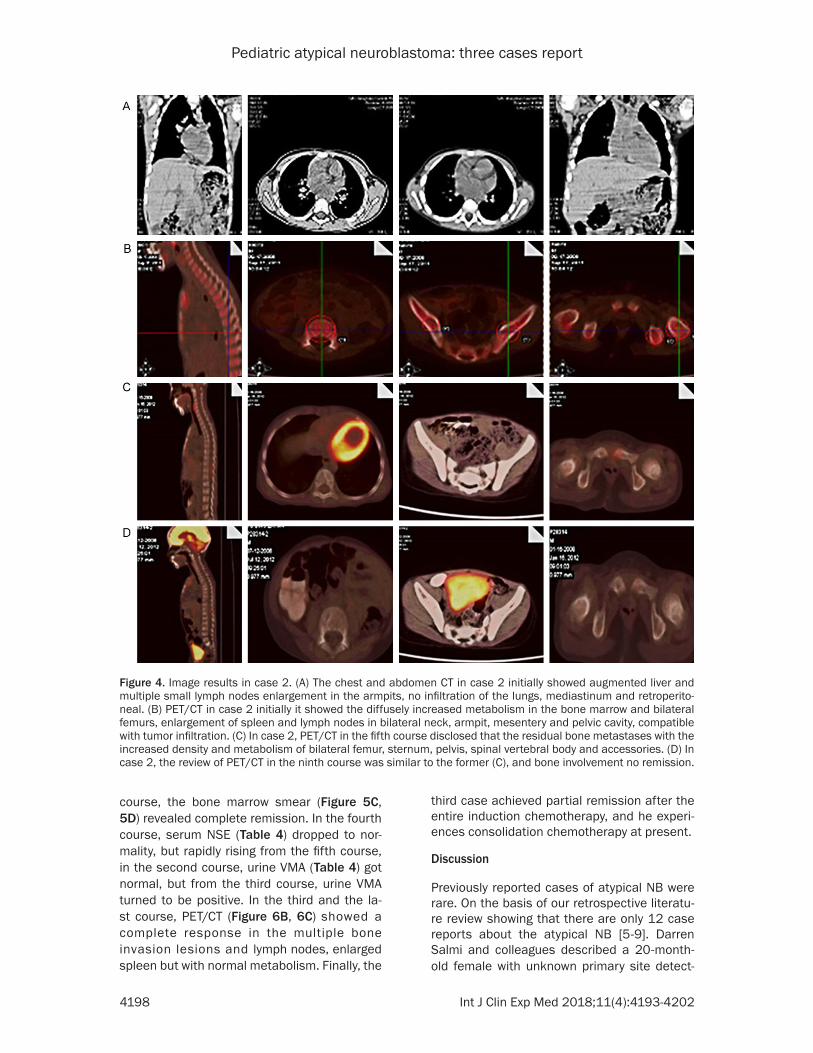
Figure 5. Bone marrow morphology in case 3. A: Before chemotherapy begins the ratio of characteristic NB cells was 56.5% (wright’s stain × 100). B: Before chemotherapy begins, the neoplastic cells with cell bodies varied in size, scant cytoplasm stained with blue and enlarged nuclei, typically formed Homer-Wright rosettes (wright’s stain × 1000). C and D: From the fifth course, the bone marrow smear revealed complete alleviation.
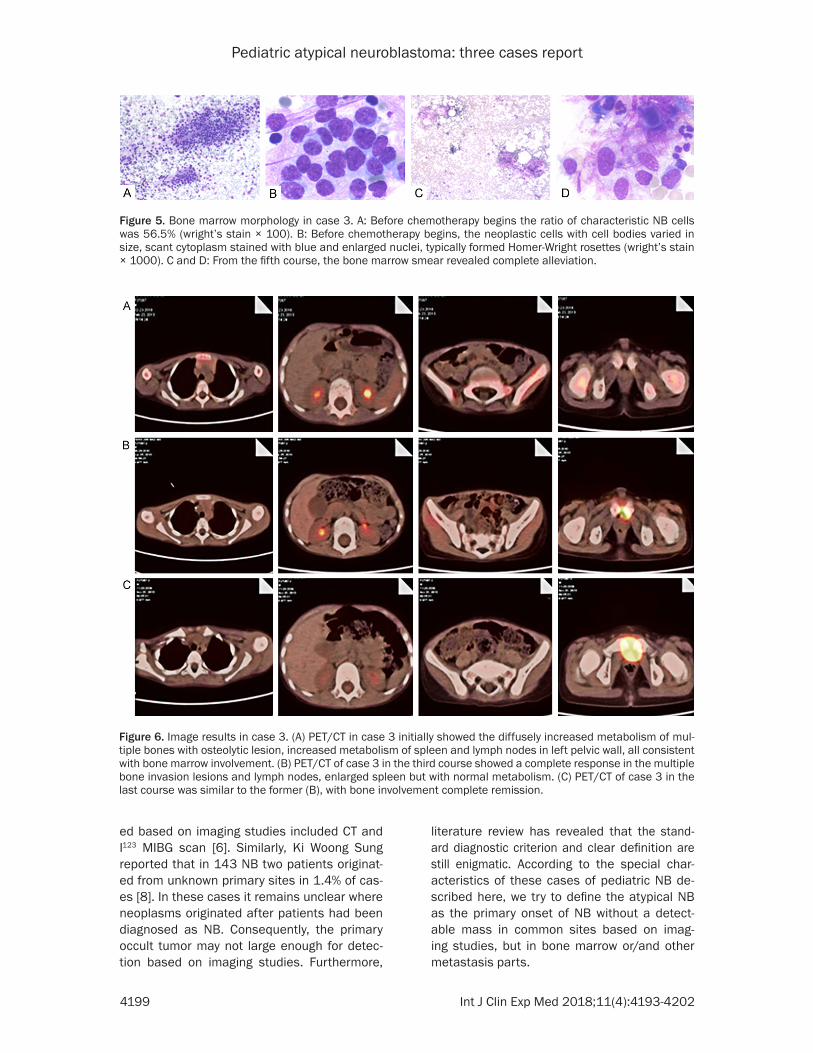
Figure 6. Image results in case 3. (A) PET/CT in case 3 initially showed the diffusely increased metabolism of mul-tiple bones with osteolytic lesion, increased metabolism of spleen and lymph nodes in left pelvic wall, all consistent with bone marrow involvement. (B) PET/CT of case 3 in the third course showed a complete response in the multiple bone invasion lesions and lymph nodes, enlarged spleen but with normal metabolism. (C) PET/CT of case 3 in the last course was similar to the former (B), with bone involvement complete remission.

Pediatric atypical neuroblastoma: three cases report
4200 Int J Clin Exp Med 2018;11(4):4193-4202
Bone and bone marrow metastases from un- known primary tumor commonly appear as pain in joint or pale. Unlike atypical NB, NB us- ually has definite primary sites. Hence, the di- agnosis of atypical NB depends on exclusion of definite primary sites NB. The diagnosis is faci- litated by significantly clinical features such as no detectable primary tumor via conventional imaging methods at diagnosis, but typical NB cells were found in the metastasis or infiltra- tion areas, and the specific NB tumor markers (such as NSE and urine VMA, etc) were positive [10]. However, equivocal features may be en- countered, and the main differential diagnosis encompasses hematological disease, rheuma- tic diseases and infectious diseases. Among them, pale may be readily misdiagnosed as leu-kemia while overlooking atypical or discordant clinical features. It is important to identify tho- se patients from hematological disease and morphology of medullary cells may be the ef- fective tool for this purpose. Strikingly, empha-sis of the atypical NB diagnosis should be placed on no substantial mass in common sites as the classical primary NB as the key and it should avoid becoming a major obstacle to make a definitive diagnosis.
Serum NSE and urine VMA are relatively valu-able and specific tumor markers of NB [11, 12]. The serum NSE > 200 ng/ml is strongly associated with a worse outcome only in pa- tients with stage IV and MYCN amplification negative NB, and that serum NSE is a limited prognostic marker in the typical NB risk stratifi-cation [13]. In our study, all the atypical NB patients showed the serum NSE increased sig-nificantly during the first visit and the trend of it was positively correlated with the disease severity and activity. Generally, the urine VMA as catecholamine metabolites is often helpful and has been proved as a valuable marker for predicting clinical behavior of NB [14]. There is no difference in the clinical value between 24 hours for testing urine VMA and single urine testing urine VMA/Cr [15]. Although urine VMA is widely used and valuable in the diagnosis of NB, the trend of urine VMA or urine VMA/Cr were not in accordance with the undesired prognosis in our patients. Compare with urine VMA or urine VMA/Cr, serum NSE was compar-atively favorable prognostic indicator in atypi-cal NB although it was less specific in general NB. A large-scale study will be necessary to
determine if urine VMA is in a limited sense in atypical NB.
Peripheral blood MRD of NB figures prominently in finding occult tumor, significantly improving the sensitivity and accuracy, and further sug-gesting tumor recurrence or metastasis [16, 17], and has been reported as a significant prognostic factor for patients with NB [18]. Another provocative finding is that that MRD was constantly monitored for four months and widely available to evaluate prognosis [19, 20]. Virtually all NB tumor cells express CD56 and GD2 [21, 22], though phenotype of CD56+/CD45- is not unique to NB, the GD2 is highly expressed on NB cells and don’t express on cells of human bone marrow and peripheral blood make it as a specific marker for NB MRD detection. In our study, peripheral blood MRD analyzed by flow cytometry detecting CD45-/CD56+/GD2+ tumor cells as previous report [23, 24], especially, the various trend of MRD values post-chemotherapy of case 1 and 2 con-sistent with worse prognosis of case 2. So, peripheral blood MRD could be considered a useful marker for evaluating prognosis and monitoring treatment response of atypical NB.
Amplification of the MYCN occurs in 20% of NB, is the most unfavorable prognostic factors and highly correlated with tumor aggressive-ness [25], in this report, all three cases the am- plification of the MYCN was negative, it seems that the MYCN status is quite limited correlat- ing with clinical behavior of atypical NB.
Atypical NB is a rare subtype of NB. Although our study was limited to only three cases, they showed that PET/CT as a non-invasive tech-nique can provide better visualization of the anatomic extent and will most likely become an option for monitoring treating response of at- ypical NB. Treatment of atypical NB in China par-ticularly presents a great challenge, due to lack of solid mass and transplant related drugs like melphalan, while conventional intensive che-motherapy seems the only way for controlling the atypical NB. Although intensive chemoth- erapy was used, the majority of our patients showed a temporary and poor response. Since there is no subsequent consolidation therapy (for financial reasons) the case 1 relapsed, and the other two patients (case 2 and case 3) merely achieved partial remission after induc-tion chemotherapy.

Pediatric atypical neuroblastoma: three cases report
4201 Int J Clin Exp Med 2018;11(4):4193-4202
Conclusion
In our limited experience, we found that des- pite intensive chemotherapy the patient with atypical NB usually represented a worse clini- cal course and poor prognosis especially in those with bone metastases. This manuscript emphasizes that the importance of distinguish-ing atypical NB from typical NB lies in the fact that the atypical NB may have a much worse clinical behavior, on the other hand, the com-bined application of serum NSE, urine VMA, MRD and PET/CT are best regarded as an as- sistive technique for the diagnosis and moni- toring of the atypical NB. In addition, as the data are limited, a large-scale study is required to investigate whether MYCN status and urine VMA are quite limited in correlating with clinical behavior of atypical NB.
Acknowledgements
This work was supported by Grant 2014A0- 30313024 from the Guangdong Natural Sci- ence Foundation; Grant from the Guangdong Science and Technology Department (2015- B050501004).
Disclosure of conflict of interest
None.
Address correspondence to: Dr. Yang Li, Guang- dong Provincial Key Laboratory of Malignant Tumor Epigenetics and Gene Regulation, Department of Pediatric Hematology/Oncology, Sun Yat-Sen Me- morial Hospital, Sun Yat-Sen University, Along The West Road 107 of Guangzhou 510120, Guangdong, China. Tel: 13570209818; E-mail: [email protected]
References
[1] Okura H, Yatomi K, Saito Y, Kasuga C, Ishii H, Karagiozov K, Miyajima M and Arai H. Unex-pected intraparenchymal hematoma caused by brain metastasis in a patient with neuro-blastoma: case report. Neurol Med Chir (To-kyo) 2011; 51: 784-788.
[2] Papaioannou G and McHugh K. Neuroblasto-ma in childhood: review and radiological find-ings. Cancer Imaging 2005; 5: 116-127.
[3] Muthu M, Cheriyan VT, Munie S, Levi E, Frank J, Ashour AE, Singh M and Rishi AK. Mecha-nisms of neuroblastoma cell growth inhibition by CARP-1 functional mimetics. PLoS One 2014; 9: e102567.
[4] Keshelava N, Davicioni E, Wan Z, Ji L, Sposto R, Triche TJ and Reynolds CP. Histone deacety-lase 1 gene expression and sensitization of multidrug-resistant neuroblastoma cell lines to cytotoxic agents by depsipeptide. J Natl Cancer Inst 2007; 99: 1107-1119.
[5] Marcus KJ, Shamberger R, Litman H, von All-men D, Grupp SA, Nancarrow CM, Goldwein J, Grier HE and Diller L. Primary tumor control in patients with stage 3/4 unfavorable neuro-blastoma treated with tandem double autolo-gous stem cell transplants. J Pediatr Hematol Oncol 2003; 25: 934-940.
[6] Salmi D, Patel C, Imashuku S, Shimada H and Satake N. Neuroblastoma of unknown primary site with periorbital bone metastasis in a child. Pediatr Blood Cancer 2010; 55: 361-363.
[7] al-Mulhim I. Neuroblastoma in children: a 10-year experience in Saudi Arabia. J Trop Pediatr 1998; 44: 77-80.
[8] Sung KW, Yoo KH, Koo HH, Kim JY, Cho EJ, Seo YL, Kim J and Lee SK. Neuroblastoma originat-ing from extra-abdominal sites: association with favorable clinical and biological features. J Korean Med Sci 2009; 24: 461-467.
[9] Kusumakumary P, Ajithkumar TV, Ratheesan K, Chellam VG and Nair MK. Pattern and out-come of neuroblastoma. A 10 year study. Indi-an Pediatr 1998; 35: 223-229.
[10] Csathy L, Kappelmayer J, Szegedi I, Kajtar B, Kiss C and Hevessy Z. Classical and atypical neuroblastoma--case reports. Cytometry B Clin Cytom 2011; 80: 134-136.
[11] Hervas Benito I, Rivas Sanchez A, Bello Arques P, Canete A, Fernandez JM, Saura Quiles A, Gonzalez Cabezas P, Ruiz Rodriguez JC, Castell V, Perez Pastor JL, Monfort JA and Mateo Na-varro A. [Value of 123I-MIBG scanning, neuron-specific enolase and serum ferritin in the di- agnosis and follow-up of patients with neuro-blastoma]. Rev Esp Med Nucl 2001; 20: 369-376.
[12] Smith SJ, Diehl NN, Smith BD and Mohney BG. Urine catecholamine levels as diagnostic markers for neuroblastoma in a defined popu-lation: implications for ophthalmic practice. Eye (Lond) 2010; 24: 1792-1796.
[13] Cangemi G, Reggiardo G, Barco S, Barbagallo L, Conte M, D’Angelo P, Bianchi M, Favre C, Galleni B, Melioli G, Haupt R, Garaventa A and Corrias MV. Prognostic value of ferritin, neu-ron-specific enolase, lactate dehydrogenase, and urinary and plasmatic catecholamine me-tabolites in children with neuroblastoma. Onco Targets Ther 2012; 5: 417-423.
[14] Scapolla C, Cangemi G, Barco S, Barbagallo L, Bugnone D, Maffia A, Melioli G, Profumo A, Benatti U and Damonte G. Identification and structural characterization by LC-ESI-IONTRAP
Pediatric atypical neuroblastoma: three cases report
4202 Int J Clin Exp Med 2018;11(4):4193-4202
and LC-ESI-TOF of some metabolic conjugation products of homovanillic acid in urine of neuro-blastoma patients. J Mass Spectrom 2012; 47: 816-824.
[15] Kawaguchi S, Hirachi N and Fukamachi M. New analyser for the determination of urinary vanillylmandelic acid, homovanillic acid and creatinine. J Chromatogr 1991; 567: 11-19.
[16] Hartomo TB, Kozaki A, Hasegawa D, Van Huy-en Pham T, Yamamoto N, Saitoh A, Ishida T, Kawasaki K, Kosaka Y, Ohashi H, Yamamoto T, Morikawa S, Hirase S, Kubokawa I, Mori T, Ya-nai T, Hayakawa A, Takeshima Y, Iijima K, Mat-suo M, Nishio H and Nishimura N. Minimal re-sidual disease monitoring in neuroblastoma patients based on the expression of a set of real-time RT-PCR markers in tumor-initiating cells. Oncol Rep 2013; 29: 1629-1636.
[17] Stutterheim J, Gerritsen A, Zappeij-Kannegiet-er L, Yalcin B, Dee R, van Noesel MM, Berthold F, Versteeg R, Caron HN, van der Schoot CE and Tytgat GA. Detecting minimal residual dis-ease in neuroblastoma: the superiority of a panel of real-time quantitative PCR markers. Clin Chem 2009; 55: 1316-1326.
[18] Burchill SA, Bradbury FM, Selby P and Lewis IJ. Early clinical evaluation of neuroblastoma cell detection by reverse transcriptase-polymerase chain reaction (RT-PCR) for tyrosine hydroxy-lase mRNA. Eur J Cancer 1995; 31a: 553-556.
[19] Fukuda M, Miyajima Y, Miyashita Y and Horibe K. Disease outcome may be predicted by mo-lecular detection of minimal residual disease in bone marrow in advanced neuroblastoma: a pilot study. J Pediatr Hematol Oncol 2001; 23: 10-13.
[20] Tchirkov A, Paillard C, Halle P, Bernard F, Bordi-goni P, Vago P, Demeocq F and Kanold J. Sig-nificance of molecular quantification of mi- nimal residual disease in metastatic neuro-blastoma. J Hematother Stem Cell Res 2003; 12: 435-442.
[21] Patel K, Moore SE, Dickson G, Rossell RJ, Bev-erley PC, Kemshead JT and Walsh FS. Neural cell adhesion molecule (NCAM) is the antigen recognized by monoclonal antibodies of simi-lar specificity in small-cell lung carcinoma and neuroblastoma. Int J Cancer 1989; 44: 573-578.
[22] Schulz G, Cheresh DA, Varki NM, Yu A, Staffile-no LK and Reisfeld RA. Detection of ganglio-side GD2 in tumor tissues and sera of neuro-blastoma patients. Cancer Res 1984; 44: 5914-5920.
[23] Beiske K, Ambros PF, Burchill SA, Cheung IY and Swerts K. Detecting minimal residual dis-ease in neuroblastoma patients-the present state of the art. Cancer Lett 2005; 228: 229-240.
[24] Valentijn LJ, Koster J, Haneveld F, Aissa RA, van Sluis P, Broekmans ME, Molenaar JJ, van Nes J and Versteeg R. Functional MYCN signa-ture predicts outcome of neuroblastoma irre-spective of MYCN amplification. Proc Natl Acad Sci U S A 2012; 109: 19190-19195.
[25] Di Cataldo A, Dau D, Conte M, Parodi S, De Ber-nardi B, Giuliano M, Pession A, Viscardi E, Luksch R, Castellano A, Bertuna G and Haupt R. Diagnostic and prognostic markers in in-fants with disseminated neuroblastoma: a ret-rospective analysis from the Italian coopera-tive group for neuroblastoma. Med Sci Monit 2009; 15: Mt11-18.