Embed Size (px)
Citation preview

Case report
Page 1 of 3
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
For citation purposes: Jyothsna P, Nayak SB, Mohandas Rao KG, Kumar N, Abhinitha P. High level branching and very superficial course of radial artery in the anatomical snuffbox: its clinical and surgical implications. OA Case Reports 2013 Aug 08;2(7):66. Co
mpe
ting
inte
rest
s: n
one
decl
ared
. Con
flict
of i
nter
ests
: non
e de
clar
ed.
All a
utho
rs c
ontr
ibut
ed to
the
conc
eptio
n, d
esig
n, a
nd p
repa
ratio
n of
the
man
uscr
ipt,
as w
ell a
s rea
d an
d ap
prov
ed th
e fin
al m
anus
crip
t.Al
l aut
hors
abi
de b
y th
e As
soci
ation
for M
edic
al E
thic
s (AM
E) e
thic
al ru
les o
f disc
losu
re.
High level branching and very superficial course of radial artery in the anatomical snuffbox: its clinical
and surgical implications P Jyothsna, SB Nayak*, KG Mohandas Rao, N Kumar, P Abhinitha
It begins 1 cm distal to the elbow joint, at the level of neck of radius. It runs medial to the brachiora-dialis throughout its course in the forearm. Just above the wrist, it is palpable between the flexor carpi radialis medially and anterior bor-der of radius laterally. It then turns posterolaterally round the wrist superficial to the lateral ligament of the wrist and deep to the abductor pollicis longus and extensor pollicis brevis muscles. It crosses the scaph-oid and trapezium bones and just before it passes between the heads of the first dorsal interosseous it is crossed by the tendon of the extensor pollicis longus muscle. Between the extensor muscles of the thumb, it is crossed by the cephalic vein and digi-tal branches of the radial nerve which supply the thumb and index finger. It passes between the two heads of the first dorsal interosseous muscle and enters the palm1. The common mode of termination of the RA is by form-ing the deep palmar arch. Although variations in the origin of the RA are common, with an incidence of 15%2, variations in the course are rare, with an incidence of only 0.52%3. For radi-ological, surgical and routine patient care purpose, precise knowledge of the course of the RA and its relation to adjacent structures in the distal part of the forearm and wrist is of great importance. We present a rare case of ‘very superficial course’ of the RA and discuss its clinical and surgical importance.
Case reportDuring routine dissection classes for medical undergraduates, we found the following variations of the RA in
the right upper limb of an adult male cadaver aged approximately 65 years old. The RA had its origin from the brachial artery in the cubital fossa. The proximal part of its course in the forearm was normal. It gave its super-ficial palmar branch, 8 cm above the proximal border of the flexor reti-naculum (Figure 1). The superficial palmar branch passed through the thenar eminence muscles before completing the superficial palmar arch. After giving the superficial palmar arch, the RA turned laterally and passed superficial to the abduc-tor pollicis longus, extensor pollicis brevis and extensor pollicis longus tendons (Figure 2). After crossing these tendons, it passed between the two heads of the first dorsal interosseous muscle and entered the palm. Its course and distribution in the palm were normal.
DiscussionThe variations in the origin and proximal course of the RA are more common than its distal course and termination. RA may originate from the axillary artery4,5, thoracoac-romial trunk6 or brachial artery7,8. Manners-Smith9 classified the varia-tions in the course of the RA into two classes according to its relation to the tendons forming the anatomical snuff box. In the first class, the RA is sin-gle and is entirely superficial to the tendons of the anatomical snuff box, also known as the superficial dorsal artery of the forearm. In the second class, the RA divides into superficial and deep branches, documented as duplication of the RA9. The cur-rent case belongs to the first class of Manners-Smith classification. In one
AbstractIntroductionVariation in the origin of radial artery is one of the common anomalies in the upper limb. However, distal part of its course shows a constant pattern. The knowledge of variations of the radial artery is of importance in vascular and reconstructive sur-geries. Here, we report the unusual superficial course and branching of the radial artery in the forearm and the dorsum of the hand. Case reportThe radial artery gave its superficial palmar branch 8 cm above the proximal border of the flexor retinaculum. After giving the superficial branch, it passed on to the dorsal aspect of the hand, by winding round the lateral aspect of the wrist superficial to the tendons form-ing the boundaries of anatomical snuff box and reached the first interosse-ous space. It passed between the two heads of the first dorsal interosseous muscle to enter the palm.ConclusionThe knowledge of this variation of the radial artery is important while per-forming intravenous cannulations and plastic surgeries. It is also impor-tant to cardiothoracic surgeons as the radial artery is increasingly being used for the coronary bypass graft in place of the great saphenous vein.
IntroductionThe radial artery (RA) is the smaller terminal branch of the brachial artery.
*Corresponding authorEmail: [email protected]
Melaka Manipal Medical College (Manipal Campus), Manipal University, Karnataka, India
Ana
tom
y

Case report
Page 2 of 3
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
For citation purposes: Jyothsna P, Nayak SB, Mohandas Rao KG, Kumar N, Abhinitha P. High level branching and very superficial course of radial artery in the anatomical snuffbox: its clinical and surgical implications. OA Case Reports 2013 Aug 08;2(7):66.
elevation of the forearm flaps13–16 or misinterpreted in contrast radiographs17. Harvesting of the RA is one of the common surgical proce-dures. Patients with anatomical vari-ations of the RA have a significantly lower puncture and success rate in such procedures18. The RA is being used for coronary artery bypass grafting19 and it has been shown to have a superior perioperative and post-operative course than the saphe-nous vein grafts20. In the current case, the superficial palmar branch of the RA took its origin 8 cm above the proximal border of the flexor retinac-ulum and ran just undercover of the skin in the distal third of the forearm. Awareness of this variation is very important as the artery is liable to get injured in skin incisions in the distal third of the forearm. The very super-ficial course of the RA in the anatomi-cal snuff box and its close relation to the cephalic vein is also a predispos-ing factor for its inadvertent injuries. It might get punctured instead of the cephalic vein while setting an intra-venous line. Superficial cuts in the anatomical snuffbox might result in significant bleeding when the artery is very superficial as the one being reported here.
ConclusionThe knowledge of this variation of the radial artery is important during intravenous cannulations and plastic surgeries. It is also important to cardi-othoracic surgeons as the radial artery is increasingly being used for the coronary bypass graft in place of the great saphenous vein. The knowledge of high origin of superficial palmar branch and very superficial course of the RA in the anatomical snuffbox may be important for the plastic surgeons, cardiologists and radiologists.
References1. Standering S. Gray’s anatomy. The ana-tomical basis of clinical practice. 39th ed. London: Elsevier Churchill Livingstone; 2005.p883–28.
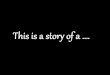
Figure 2: Dissection of the lateral side of the right hand showing the anatomi-cal snuff box. Note the superficial relationship of the radial artery (RA) to the extensor pollicis brevis (EPB) and extensor pollicis longus (EPL) tendons. First dorsal interosseous (FDI), dorsal venous arch (DVA), branches of the radial nerve (RN) and cephalic vein (CV) can also be seen.
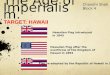
Figure 1: Dissection of the distal part of the front of the right forearm showing the variation of the radial artery (RA). Note its course superficial to the tendon of abductor pollicis longus (APL) and the high origin of its superficial palmar branch (SBRA). Branches of the radial nerve (RN) along with cephalic vein and flexor carpi radialis tendon (FCR) can also be seen.
of the recent studies, the RA passed superficial to the anatomical snuff-box and crossed superficial to the tendon of the extensor pollicis longus muscle in one out of 75 specimens studied10.
The superficial arteries of the upper extremity may be mistaken for veins, which may become a basis for intraarterial injections instead of intended intravenous injections11,12. They may also be encountered during

Case report
Page 3 of 3
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
For citation purposes: Jyothsna P, Nayak SB, Mohandas Rao KG, Kumar N, Abhinitha P. High level branching and very superficial course of radial artery in the anatomical snuffbox: its clinical and surgical implications. OA Case Reports 2013 Aug 08;2(7):66.
2. McCormack LJ, Cauldwell EW, Anson BJ. Brachial and antebrachial arterial pat-terns; a study of 750 extremities. Surg Gynecol Obstet. 1953 Jan;96(1):43–54.3. Rodriguez-Niedenfuhr M, Vazquez T, Nearn L, Ferreira B, Parkin I, Sanudo JR. Variations of the arterial pattern in the upper limb revisited: a morphological and statistical study, with a review of the literature. J Anat. 2001 Nov;199(Pt 5): 547–66.4. Celik HH, Sargon MF, Konan A, Kural E. High brachial artery bifurcation: a report of 2 cases. Bull Assoc Anat (Nancy). 1996 Sep;80(250):13–4.5. Konarik M, Knize J, Baca V, Kachlik D. Superficial brachioradial artery (radial artery originating from the axillary artery): a case report and its embryologi-cal background. Folia Morphol (Warsz). 2009 Aug;68(3):174–8.6. Loukas M, Louis RG Jr, Almond J, Armstrong T. A case of an anomalous radial artery arising from the thoracoac-romial trunk. Surg Radiol Anat. 2005 Dec;27(5):463–6.7. Shen S, Hong MK. A rare case of bilat-eral variations of upper limb arteries: brief review of nomenclature, embryol-ogy and clinical applications. Surg Radiol Anat. 2008 Oct;30(7):601–3.
8. Vollala VR, Nagabhooshana S, Bhat SM. Trifurcation of brachial artery with variant course of radial artery: rare observation. Anat Sci Int. 2008 Dec;83(4):307–9.9. Manners-Smith T. The limb arteries of primates. J Anat Physiol. 1912 Jan;46(Pt 2): 95–172.10. Chandni G, Vikram P, Murlimanju BV, Vaishali RS. A morphological study of variations in the origin and course of radial artery. Res J Pharm Biol Chem Sci. 2012;3(2):333–40.11. Deligonul U, Gabliani G, Kern MJ, Vandormael M. Percutaneous bra-chial catheterization: the hidden haz-ard of high brachial artery bifurcation. Cathet Cardiovasc Diagn. 1988;14(1): 44–5.12. Thomas R, Newell R. Anomalous arteries in the upper limb. Clin Anat. 1995;7:57.13. Devansh MS. Superficial ulnar artery flap. Plast Reconstr Surg. 1996 Feb;97(2): 420–6. 14. Funk GF, Valentino J, McCulloch TM, Graham SM, Hoffman HT. Anomalies of forearm vascular anatomy encoun-tered during elevation of the radial forearm flap. Head Neck. 1995 Jul–Aug; 17(4):284–92.
15. Heden P, Gylbert L. Anomaly of the radial artery encountered during elevation of the radial forearm flap. J Reconstr Microsurg. 1990 Apr;6(2):139–41.16. Thoma A, Young JEM. The super-ficial ulnar artery “trap” and the free forearm flap. Ann Plast Surg. 1992 Apr;28(4):370–2.17. Rodriguez-Niedenfuhr M, Burton GJ, Deu J, Sanudo JR. Development of the arterial pattern in the upper limb of staged human embryos: normal devel-opment and anatomic variations. J Anat. 2001 Oct;199(Pt 4):407–17.18. Valsecchi O, Vassileva A, Musumeci G, Rossini R, Tespili M, Guagliumi G, et al. Failure of transradial approach during coronary interventions: anatomic consid-erations. Cathet Cardiovasc Interv. 2006 Jun;67(6):870–8.19. Sajja LR, Mannam G, Pantula NR, Sompalli S. Role of radial artery graft in coronary artery bypass grafting. Ann Thorac Surg. 2005 Jun;79(6): 2180–8.20. Cohen G, Tamariz MG, Sever JY, Liaghati N, Guru V, Christakis GT, et al. The radial artery versus the saphenous vein graft in contemporary CABG: a case-matched study. Ann Thorac Surg. 2001 Jan;71(1):180–5.