Embed Size (px)
Citation preview
Int J Clin Exp Pathol 2015;8(2):2165-2170www.ijcep.com /ISSN:1936-2625/IJCEP0004730
Case Report Multfocal micronodular pneumocyte hyperplasia in a Chinese man masquerading as miliary tuberculosis
Qi Sun1, Hou-Rong Cai2, Eugene J Mark3, Li-Yun Miao2, Hong-Yan Wu1, Qiang Zhou1, Jun Chen1, Wei Zhang4, Fan-Qing Meng1
Departments of 1Pathology, 2Respiratory Medicine, Nanjing Drum Tower Hospital, The Affiliated Hospital of Nanjing University Medical School, Nanjing, Jiangsu Province, China; 3Department of Pathology, Massachusetts General Hospital and Harvard Medical School, Boston, MA, USA; 4Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, Nanjing, Jiangsu Province, China
Received December 11, 2014; Accepted February 6, 2015; Epub February 1, 2015; Published February 15, 2015
Abstract: Multifocal Micronodular Pneumocyte Hyperplasia (MMPH) is a rare and histologically, distinctive pulmo-nary manifestation of tuberous sclerosis complex (TSC) characterized by numerous and extensive proliferative le-sions of type II pneumocytes similar to atypical adenomatous hyperplasia (AAH) or non-mucinous adenocarcinoma in situ (AIS). We reported MMPH in a 38-year-old Chinese man with TSC masquerading for 16 months as miliary tuberculosis and discussed the differential diagnosis.
Keywords: Tuberous sclerosis complex, multifocal micronodular pneumocyte hyperplasia
Introduction
Tuberous sclerosis complex (TSC) is a genetic disease characterized by hamartomatous lesion in various organs [1]. Pulmonary mani-festations of TSC include lymphangioleiomyo-matosis (LAM) and multifocal micronodular pneumocyte hyperplasia (MMPH). MMPH, as described by Popper in 1991 [2], has multifocal well-demarcated nodular lesions consisting of proliferation of type II pneumocytes with mild fibrous thickening of the alveolar septa particu-larly when extensive. Active proliferating pneu-mocytes with atypia can lead to diagnostic problem. We describe MMPH in a Chinese man with TSC, and discuss the clinical, histological and molecular features of MMPH with empha-sis on the differential diagnosis.
Case report
Clinical history
A 38-year-old man was admitted to local hospi-tal because of a constant dull chest pain in the sternum for one year. Computed tomography (CT) of the chest revealed multiple bilateral
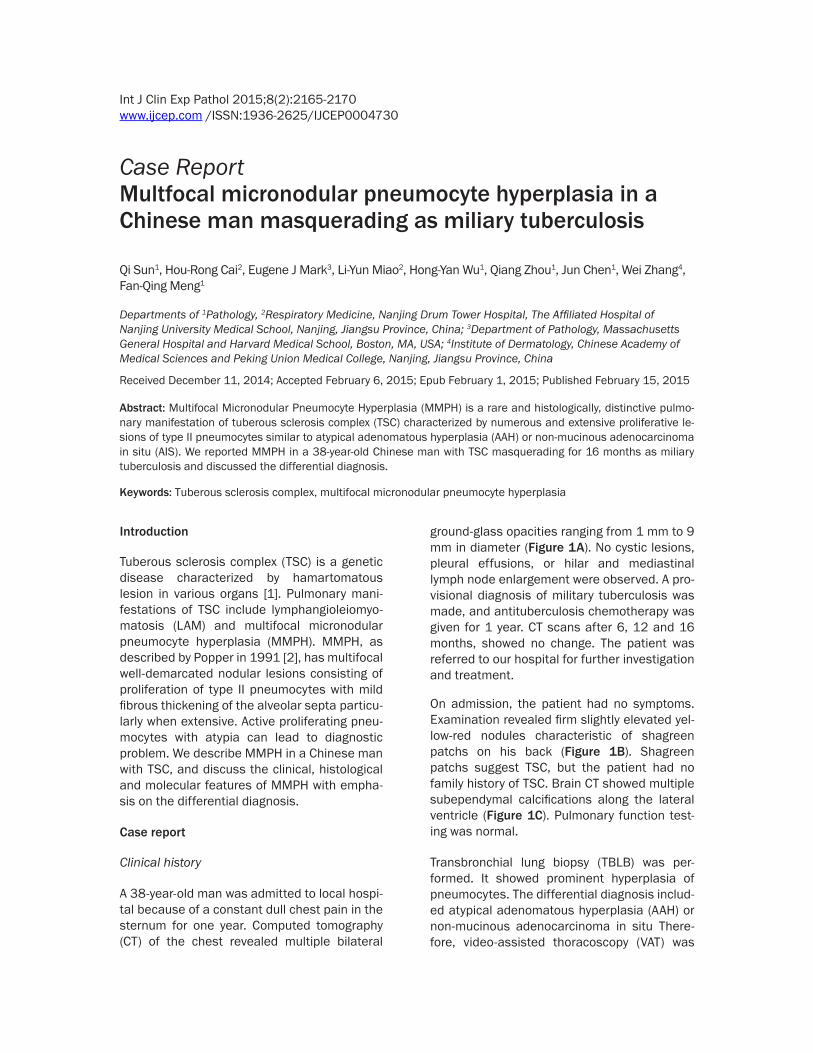
ground-glass opacities ranging from 1 mm to 9 mm in diameter (Figure 1A). No cystic lesions, pleural effusions, or hilar and mediastinal lymph node enlargement were observed. A pro-visional diagnosis of military tuberculosis was made, and antituberculosis chemotherapy was given for 1 year. CT scans after 6, 12 and 16 months, showed no change. The patient was referred to our hospital for further investigation and treatment.
On admission, the patient had no symptoms. Examination revealed firm slightly elevated yel-low-red nodules characteristic of shagreen patchs on his back (Figure 1B). Shagreen patchs suggest TSC, but the patient had no family history of TSC. Brain CT showed multiple subependymal calcifications along the lateral ventricle (Figure 1C). Pulmonary function test-ing was normal.
Transbronchial lung biopsy (TBLB) was per-formed. It showed prominent hyperplasia of pneumocytes. The differential diagnosis includ-ed atypical adenomatous hyperplasia (AAH) or non-mucinous adenocarcinoma in situ There- fore, video-assisted thoracoscopy (VAT) was
Multifocal micronodular pneumocyte hyperplasia in tuberous sclerosis complex
2166 Int J Clin Exp Pathol 2015;8(2):2165-2170
performed during the operation, the surgeon noted white nodules beneath the pleura.
Pathologic findings
Three wedge lung tissues from the upper, mid-dle and lower lobe of right lung were obtained. Lots of white firm tiny and small nodules, rang-ing from 1 mm to 5 mm in diameter, were found on cut surface.
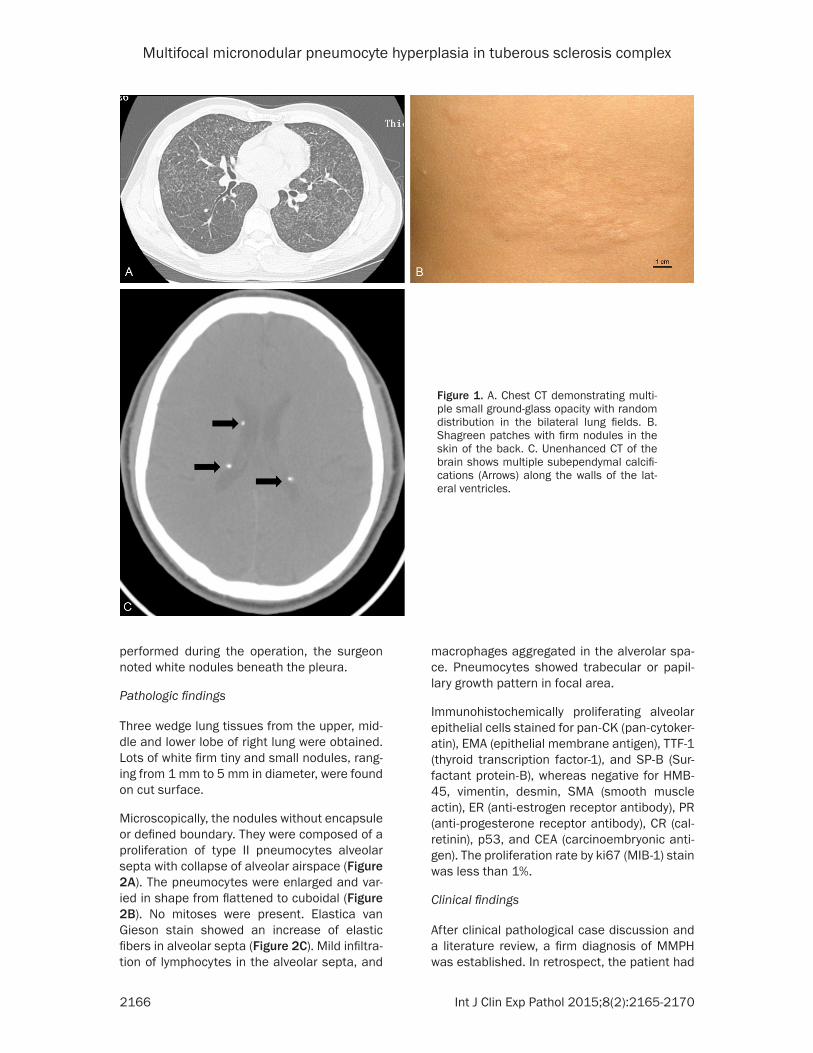
Microscopically, the nodules without encapsule or defined boundary. They were composed of a proliferation of type II pneumocytes alveolar septa with collapse of alveolar airspace (Figure 2A). The pneumocytes were enlarged and var-ied in shape from flattened to cuboidal (Figure 2B). No mitoses were present. Elastica van Gieson stain showed an increase of elastic fibers in alveolar septa (Figure 2C). Mild infiltra-tion of lymphocytes in the alveolar septa, and
macrophages aggregated in the alverolar spa- ce. Pneumocytes showed trabecular or papil-lary growth pattern in focal area.
Immunohistochemically proliferating alveolar epithelial cells stained for pan-CK (pan-cytoker-atin), EMA (epithelial membrane antigen), TTF-1 (thyroid transcription factor-1), and SP-B (Sur- factant protein-B), whereas negative for HMB-45, vimentin, desmin, SMA (smooth muscle actin), ER (anti-estrogen receptor antibody), PR (anti-progesterone receptor antibody), CR (cal-retinin), p53, and CEA (carcinoembryonic anti-gen). The proliferation rate by ki67 (MIB-1) stain was less than 1%.
Clinical findings
After clinical pathological case discussion and a literature review, a firm diagnosis of MMPH was established. In retrospect, the patient had
Figure 1. A. Chest CT demonstrating multi-ple small ground-glass opacity with random distribution in the bilateral lung fields. B. Shagreen patches with firm nodules in the skin of the back. C. Unenhanced CT of the brain shows multiple subependymal calcifi-cations (Arrows) along the walls of the lat-eral ventricles.
Multifocal micronodular pneumocyte hyperplasia in tuberous sclerosis complex
2167 Int J Clin Exp Pathol 2015;8(2):2165-2170
two of the major diagnostic criteria for TSC, namely subependymal nodules and shagreen patches [1]. The patient did not have the third part of the triad, namely seizures or mental retardation. Unfortunately, the patient refused to take genetic test for confirming TSC gene mutation.
Discussion
Pulmonary manifestation appears in 1%-2% of patients with TSC and usually associated with LAM [3, 4]. MMPH is an additional and rarer manifestation in TSC patients. It occurs in patients with TSC or with LAM, alone but has been reported in men without TSC or LAM [5, 6]. The negative staining for HMB45, estrogen and progesterone receptors in our cases rule one against LAM and also indicate a pathoge-netic difference between MMPH and LAM [7].
Less than 50 cases of MMPH are reported in the pathologic literature. The age range has been 13-64 years old [8, 9]. Only a few cases occurred in men [4, 7, 10]. Clinically, MMPH usually have no respiratory symptoms. Some
patients with MMPH present with dyspnea, cough, and mild hypoxemia [10] but most patients have no respiratory symptoms. MMPH presents on x-ray as multiple tiny nodules 1-20 mm in diameter [7, 11], as in this case that are randomly scattered throughout the lung [10].
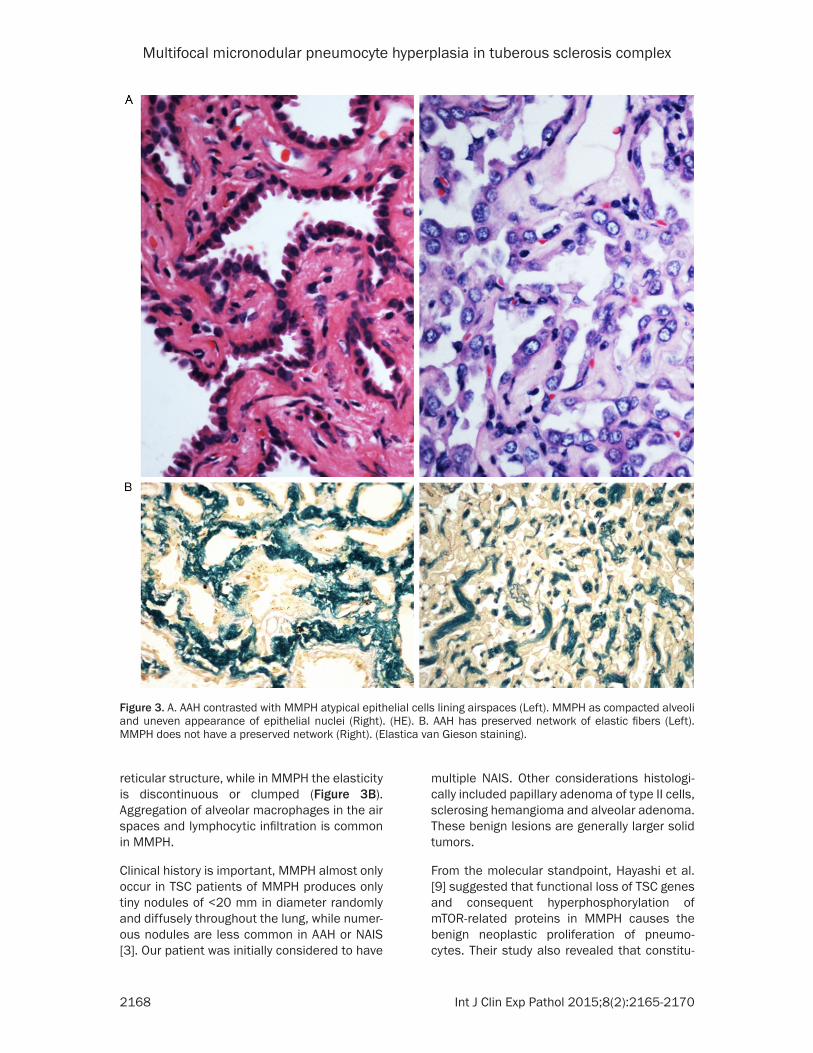
In our case, VAT played an important role in establishing the diagnosis. MMPH must be his-tologically distinguished from AAH or NAIS [3-7, 12]. MMPH has been in fact described as alve-olar epithelial atypical adenomatous hyperpla-sia [13]. However, AAH foci are usually less than 5 mm in diameter and often appear in association to lung carcinomas. Although nuclear features play a part in the differential diagnosis of AAH and MMPH [3-7], nuclear atypia can appear in both diseases. However, the cells in AAH comprise a more homogeneous population compared to that seen in MMPH (Figure 3A). The epithelial cells in AAH show immunoreactivity for p53 and CEA while the cases of MMPH do not. Both AAH and MMPH can have thickened alveolar septa with an increase in elastic fibers, but the proliferation of elastic fibers in AAH is often assembled in a
Figure 2. A. Relatively circumscribed nodules composed of a proliferation of type II pneumo-cytes in the lung. (HE, ×20). B. Pneumocytes (Thick arrows) admixed with lymphocytes, and macrophages (Thin arrows) aggregated in al-veoli. (HE, ×200). C. Increase in elastic fibers in alveolar septa. (Elastica van Gieson staining, ×40).
Multifocal micronodular pneumocyte hyperplasia in tuberous sclerosis complex
2168 Int J Clin Exp Pathol 2015;8(2):2165-2170
reticular structure, while in MMPH the elasticity is discontinuous or clumped (Figure 3B). Aggregation of alveolar macrophages in the air spaces and lymphocytic infiltration is common in MMPH.
Clinical history is important, MMPH almost only occur in TSC patients of MMPH produces only tiny nodules of <20 mm in diameter randomly and diffusely throughout the lung, while numer-ous nodules are less common in AAH or NAIS [3]. Our patient was initially considered to have
multiple NAIS. Other considerations histologi-cally included papillary adenoma of type II cells, sclerosing hemangioma and alveolar adenoma. These benign lesions are generally larger solid tumors.
From the molecular standpoint, Hayashi et al. [9] suggested that functional loss of TSC genes and consequent hyperphosphorylation of mTOR-related proteins in MMPH causes the benign neoplastic proliferation of pneumo-cytes. Their study also revealed that constitu-
Figure 3. A. AAH contrasted with MMPH atypical epithelial cells lining airspaces (Left). MMPH as compacted alveoli and uneven appearance of epithelial nuclei (Right). (HE). B. AAH has preserved network of elastic fibers (Left). MMPH does not have a preserved network (Right). (Elastica van Gieson staining).
Multifocal micronodular pneumocyte hyperplasia in tuberous sclerosis complex
2169 Int J Clin Exp Pathol 2015;8(2):2165-2170
tive activation of phospho-Akt (an upstream regulatory protein of mTOR) in both AAH and NAIS was more frequently detected than TSC LOH, suggesting different molecular mecha-nisms between MMPH and preinvasive lesions of pneumocytes. Although TSC is an autosomal dominant disease associated with gene muta-tions of TSC1 or TSC2, two-thirds of cases have sporadic mutations [14], which leads to under-diagnosis in TSC patients without the classical clinical triad. Our case, evaluation of the TSC gene mutations was not taken. However, our patient had no family history of TSC, suggesting that this case was sporadic.
The prognosis of MMPH is good. In the litera-ture, 2 patients died of respiratory and heart failure due to bilateral pulmonary nodules of MMPH [5] or progressive cystic changes in other organs [7]. Without any treatment, the lesions in our patient remained unchanged after diagnosis of MMPH for 2 years.
As to our knowledge, MMPH has not been previ-ously reported in the mainland of China. Therefore, it is important to be aware of its exis-tence in TSC patient in order to prevent more aggressive surgery and avoiding other diagno-ses including tuberculosis.
Disclosure of conflict of interest
None.
Address correspondence to: Dr. Fan-Qing Meng, Department of Pathology, Nanjing Drum Tower Hospital, The Affiliated Hospital of Nanjing University Medical School, 321 Zhongshan Road, Nanjing, Jiangsu Province, China. Tel: (0086)2583304616-10166; E-mail: [email protected]
References
[1] Roach ES, Gomez MR, Northrup H. Tuberous sclerosis complex consensus conference: re-vised clinical diagnostic criteria. J Child Neurol 1998; 13: 624-8.
[2] Popper HH, Juettner-Smolle FM, Pongratz MG. Micronodular hyperplasia of type II pneumo-cytes: a new lung lesion associated with tuber-ous sclerosis. Histopathology 1991; 18: 347-54.
[3] Kobashi Y, Sugiu T, Mouri K, Irei T, Nakata M, Oka M. Multifocal micronodular pneumocyte hyperplasia associated with tuberous sclero-
sis: differentiation from multiple atypical ade-nomatous hyperplasia. Jpn J Clin Oncol 2008; 38: 451-4.
[4] Miravet Sorribes L, Mancheño Franch N, Batal-la Bautista L. Multifocal micronodular pneu-mocyte hyperplasia in a patient with tuberous sclerosis. Arch Bronconeumol 2013; 49: 36-7.
[5] Cancellieri A, Poletti V, Corrin B. Respiratory failure due to micronodular type II pneumocyte hyperplasia. Histopathology 2002; 41: 263-5.
[6] Shintani Y, Ohta M, Iwasaki T, Ikeda N, Tomita E, Nagano T, Kawahara K. A case of micronod-ular pneumocyte hyperplasia diagnosed through surgical resection. Ann Thorac Cardio-vasc Surg 2010; 16: 45-7.
[7] Kobashi Y, Sugiu T, Mouri K, Irei T, Nakata M, Oka M. Clinicopathological analysis of multifo-cal micronodular pneumocyte hyperplasia as-sociated with tuberous sclerosis in Japan. Res-pirology 2008; 13: 1076-81.
[8] Behnes CL, Schütze G, Engelke C, Bremmer F, Gunawan B, Radzun HJ, Schweyer S. 13-year-old tuberous sclerosis patient with renal cell carcinoma associated with multiple renal an-giomyolipomas developing multifocal mi-cronodular pneumocyte hyperplasia. BMC Clin Pathol 2013; 13: 4.
[9] Hayashi T, Kumasaka T, Mitani K, Yao T, Suda K, Seyama K. Loss of heterozygosity on tuber-ous sclerosis complex genes in multifocal mi-cronodular pneumocyte hyperplasia. Mod Pathol 2010; 23: 1251-60.
[10] Ristagno RL, Biddinger PW, Pina EM, Meyer CA. Multifocal micronodular pneumocyte hy-perplasia in tuberous sclerosis. AJR Am J Roentgenol 2005; 184 Suppl 3: S37-9.
[11] Suzuki K, Seyama K, Hayashi T, Yamashiro Y, Shiraishi A, Kuwatsuru R. Reversed halo sign in tuberous sclerosis complex. Case Rep Radi-ol 2013; 2013: 428501.
[12] Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger KR, Yatabe Y, Beer DG, Powell CA, Riely GJ, Van Schil PE, Garg K, Austin JH, Asamura H,Rusch VW, Hirsch FR, Scagliotti G, Mitsudomi T, Huber RM, Ishikawa Y, Jett J, San-chez-Cespedes M, Sculier JP, Takahashi T, Tsuboi M, Vansteenkiste J, Wistuba I, Yang PC, Aberle D, Brambilla C, Flieder D, Franklin W, Gazdar A, Gould M, Hasleton P, Henderson D, Johnson B, Johnson D, Kerr K, Kuriyama K, Lee JS, Miller VA, Petersen I, Roggli V, Rosell R, Saijo N, Thunnissen E, Tsao M, Yankelewitz D. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisci-plinary classification of lung adenocarcinoma. J Thorac Oncol 2011; 6: 244-85.
[13] Okamura H, Yamauchi H. Pulmonary manifes-tations of tuberous sclerosis: its relationship to

Multifocal micronodular pneumocyte hyperplasia in tuberous sclerosis complex
2170 Int J Clin Exp Pathol 2015;8(2):2165-2170
pulmonary lymphangioleiomatosis. Jpn J Chest Dis 1988; 37: 216-22.
[14] Rose VM, Au KS, Pollom G, Roach ES, Prashner HR, Northrup H. Germ-line mosaicism in tuber-
ous sclerosis: how common? Am J Hum Genet 1999; 64: 986-92.









![Endometrium presentation - Dr Wright[1] · Endometrial Hyperplasia Simple hyperplasia Complex hyperplasia (adenomatous) Simple atypical hyperplasia ... Progression of Hyperplasia](https://img.pdfslide.us/doc/110x75/5b8a421e7f8b9a50388bc13d/endometrium-presentation-dr-wright1-endometrial-hyperplasia-simple-hyperplasia.jpg)