Embed Size (px)
Citation preview
Case Report
Metastases to Pineal Gland
PATRICIA WEBER, MD," KIRK V. SHEPARD, MD, t AND SRlNlVASAN VIJAYAKUMAR, MD*
Metastases to the pineal gland is an uncommon event. Bronchogenic carcinomas are the most frequent source of the primary lesion. A case of small cell carcinoma of the lung with solitary metastases to the pineal gland is reported; the literature is reviewed.
Cancer 63:164-165, 1989.
ETASTASES to the pineal gland is an uncommon M manifestation of malignancy. Less than 35 cases of metastases to the pineal gland have been reported and are most commonly associated with lung and breast car- cinomas. Many cases of pineal metastases include in- volvement of other organs, but we report a rare case of small cell lung carcinoma with a solitary metastasis to the pineal gland. Symptoms seen in regard to pineal gland metastases are discussed.
Case Report
A 62-year-old man presented to the Cleveland Clinic Foun- dation, Cleveland, Ohio, in December 1985 with complaints of dyspnea, cough, and weakness. A chest x-ray revealed a right lower lobe infiltrate and a questionable right hilar fullness. Fur- ther workup showed the patient to have limited-stage small cell carcinoma of the lung. A bone marrow biopsy, bone scan, com- puterized tomography (CT) scan of the head, and a CT scan of the abdomen and pelvis were negative for metastases.
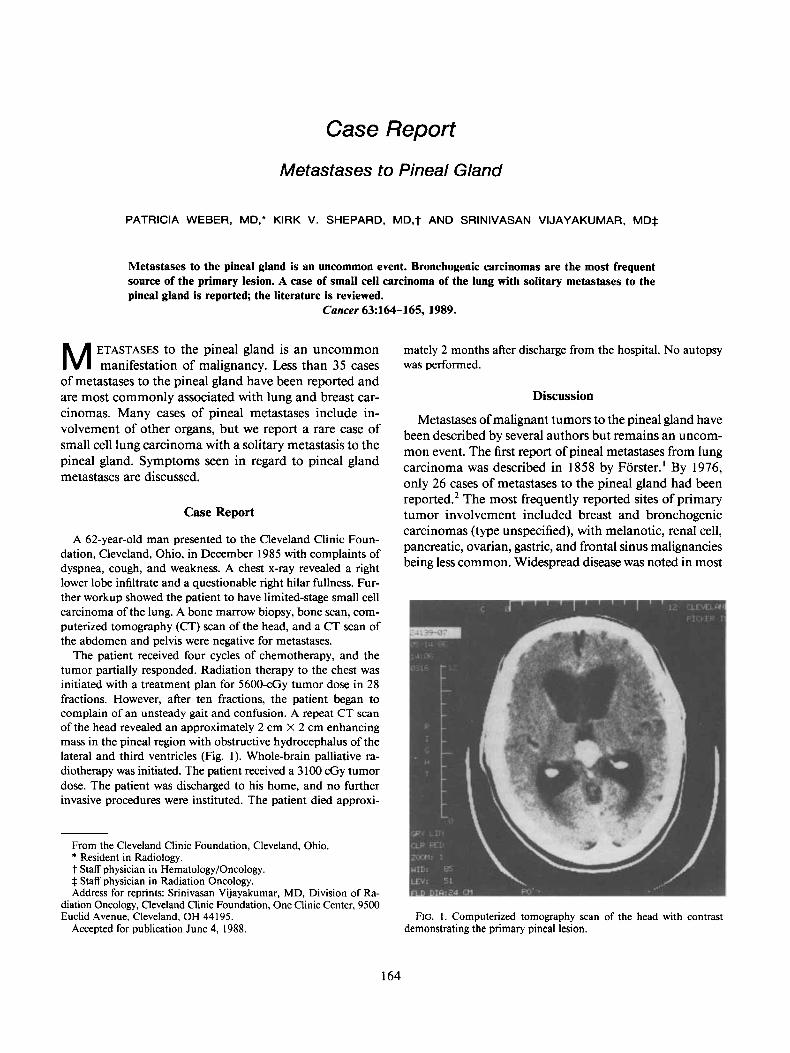
The patient received four cycles of chemotherapy, and the tumor partially responded. Radiation therapy to the chest was initiated with a treatment plan for 5600-cGy tumor dose in 28 fractions. However, after ten fractions, the patient began to complain of an unsteady gait and confusion. A repeat CT scan of the head revealed an approximately 2 cm X 2 cm enhancing mass in the pineal region with obstructive hydrocephalus of the lateral and third ventricles (Fig. 1). Whole-brain palliative ra- diotherapy was initiated. The patient received a 3 100 cGy tumor dose. The patient was discharged to his home, and no further invasive procedures were instituted. The patient died approxi-
mately 2 months after discharge from the hospital. No autopsy was performed.
Discussion
Metastases of malignant tumors to the pineal gland have been described by several authors but remains an uncom- mon event. The first report of pineal metastases from lung carcinoma was described in 1858 by Forster.' By 1976, only 26 cases of metastases to the pineal gland had been reported.* The most frequently reported sites of primary tumor involvement included breast and bronchogenic carcinomas (type unspecified), with melanotic, renal cell, pancreatic, ovarian, gastric, and frontal sinus malignancies being less common. Widespread disease was noted in most
From the Cleveland Clinic Foundation, Cleveland, Ohio. * Resident in Radiology. t Staff physician in Hematology/Oncology. 4 Staff physician in Radiation Oncology. Address for reprints: Srinivasan Vijayakumar, MD, Division of Ra-
diation Oncology, Cleveland Clinic Foundation, One Clinic Center, 9500 Euclid Avenue, Cleveland, OH 44 195.
Accepted for publication June 4, 1988. FIG. 1. Computerized tomography scan of the head with contrast
demonstrating the primary pineal lesion.
164

No. I METASTASES TO PINEAL GLAND - Weber et al. 165
of these cases; however, nine of the 26 patients had the pineal gland as the solitary site of intracranial involve- mmt.2 Our case report also demonstrates that the pineal gland is the only site of metastases.
In another study by Halpert et al. various sites of brain metastases from 338 lung carcinomas were rev ie~ed .~ One hundred twenty-nine cases of brain metastases were noted with three of these cases involving the pineal gland. Of the three pineal metastases from primary lung carcinomas (piithologic findings not specified), only one was a solitary ceintral lesion. Ouyang and Rozdilsky have described a small cell carcinoma of the lung with metastases to the pineal gland.4
Ortega et al. performed autopsies on 130 patients with widespread neoplastic disease, finding five cases of pineal meta~tases.~ Three of these cases had isolated pineal le- sions, all of which grossly replaced pineal tissue. The re- maining two cases revealed other sites of intracranial in- volvement with only minimal pineal gland replacement.
In the cases described above, the time from diagnosis of the primary tumor to the onset of central nervous sys- tem (CNS) symptoms and CNS involvement was not al- waiys specified. One episode of primary renal cell carci- na'ma with pineal metastases describes a patient with complaints of vertigo and episodes of confusion five years after becoming symptomatic from her primary tumor.4 Another patient with pineal metastases secondary to a small cell bronchogenic carcinoma was asymptomatic during his entire i l lne~s .~ The study of Ortega el al. con- cluded that their patients were never symptomatic from pineal involvement, but from distortion of surrounding structures5
Most cases of pineal metastases have been diagnosed by autopsy. The proximity of these tumors to vital brain
structures limits one's ability to perform biopsies on these lesions. The most important factor in differentiating met- astatic intracranial disease from a primary lesion is a his- tory of malignancy.6 In patients with a known history of malignant neoplasm, approximately 90% of supratentorial lesions represent metastases.' Young adults and children usually are those affected by primary pineal tumors. Our patient had a primary small cell lung carcinoma and was elderly, both of which are consistent with metastases to the pineal gland. The pineal lesion developed soon after a negative CT scan of the head, which was performed at the time of diagnosis of small cell lung carcinoma. All of these factors led us to a diagnosis of metastatic disease rather than a primary pineal tumor. No biopsy was per- formed because of the risks involved.
Metastases of small cell lung carcinoma to the pineal gland is rare, and metastases to the pineal gland without other brain metastases is even rarer. The presenting symptoms of CNS involvement are variable and may oc- cur before or after the primary focus of tumor has been discovered.
REFERENCES I . Forster. Ein Fall von Markschwamm mutungewohnlich vielfacher
Metastatischer Verbreitung. Virchows Arch [A] 1858; 13:27 1-274. 2. Holness RO, Sangalang VE. Myelomatous metastases to the pineal
body. Surg Neurol 1976; 5:97-100. 3. Halpert B, Erickson EE, Fields WS. Intracranial involvement from
carcinoma of the lung. Arch Pathol 1960; 69:93-103. 4. Ouyang R, Rozdilsky B. Metastases of carcinoma to the pineal
body. Arch Neurol 1966; 19399-403. 5 . Ortega P, Malamud N, Shimkin M. Metastases to the pineal body.
Arch Pathol 1951; 52518-528. 6. Tomita T, Wetzel N. Metastases to the midbrain. J Neuro-Oncol
1984; 2:73-77. 7. Voorhies R, Sundaresan N, Thaler H. The single supratentorial
lesion: An evaluation of preoperative diagnostic tests. J Neurosurg 1980; 53:364-368.



![Light and electron microscopic examination of pineal gland in ......histological structure of the pineal gland [8–18]. So, in our study it was aimed to examine the pineal gland of](https://img.pdfslide.us/doc/110x75/60c0abd73475835fb9682a43/light-and-electron-microscopic-examination-of-pineal-gland-in-histological.jpg)



![Fluoride and Pineal Gland · 2. Pineal Gland—Anatomy and Physiology In humans, the pineal gland is a neuroendocrine gland weighing about 150 mg [57]. The organ, part of the epithalamus,](https://img.pdfslide.us/doc/110x75/5fb399b0033ed705fe72d5fd/fluoride-and-pineal-gland-2-pineal-glandaanatomy-and-physiology-in-humans-the.jpg)




















