Embed Size (px)
Citation preview

Hindawi Publishing CorporationCase Reports in MedicineVolume 2013, Article ID 296874, 3 pageshttp://dx.doi.org/10.1155/2013/296874
Case ReportKernohan’s Notch: A Forgotten Cause of Hemiplegia—CT ScansAre Useful in This Diagnosis
Ragesh Panikkath, Deepa Panikkath, Sian Yik Lim, and Kenneth Nugent
Department of Internal Medicine, Texas Tech University Health Sciences Center, Lubbock, TX 79430, USA
Correspondence should be addressed to Ragesh Panikkath; [email protected]
Received 19 April 2013; Revised 2 July 2013; Accepted 8 October 2013
Academic Editor: John Kortbeek
Copyright © 2013 Ragesh Panikkath et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Hemiparesis ipsilateral to a cerebral lesion can be a false localizing sign. This is due to midline shift of the midbrain resulting incompression of the contralateral pyramidal fibers on the tough dural reflection tentorium cerebelli. This may result in partial orcomplete damage to these fibers. Since these fibers are destined to cross in the medulla and innervate the opposite side of thebody, this causes hemiparesis ipsilateral to the site of cerebral lesion. Computed tomography (CT) scans have not been used tosupport the diagnosis of this entity until now.We report a 68-year-old woman with a subdural hematoma who developed ipsilateralhemiparesis without any other explanation (Kernohan’s notch).TheCTof the head showed evidence of compression of themidbraincontralateral to the hematoma and was useful in the diagnosis. The purpose of this report is to increase the awareness of thispresentation and to emphasize the utility of CT scans to support the diagnosis.
1. Introduction
Hemiparesis ipsilateral to the site of a cerebral lesion has beencalled Kernohan’s notch. This sign (originally described atautopsy) has been reported with cerebral tumors, subduralhematomas (SDH), and extradural hematomas with midlineshift. Recently magnetic resonance imaging (MRI) has beenused for this diagnosis in appropriate clinical situations;indirect supportive evidence for this sign has not beendescribed utilizing the more commonly available computedtomography (CT) imaging.
2. A Case Report
We report a 69-year-old womanwith Alzheimer’s disease andrecurrent falls who presented in a comatose state. A CT scanof the head showed a large right subdural hematoma with amidline shift of 18mm. She underwent urgent neurosurgicalevacuation of the subdural hematoma. Her consciousnessgradually recovered, but she had right hemiplegia. An MRIdid not show any left-sided infarcts which would explainthis. Since her hemiplegia was ipsilateral to the side of thesubdural hematoma, the possibility of Kernohan’s notch was
considered. Gross deviation of the crura of the midbrain tothe left side was noted on detailed review of the CT scanof the head done prior to the evacuation of the hematoma(Figure 1). A CT of head after craniotomy and evacuationof subdural hematoma showed persistent deformity of themidbrain (Figure 2). The MRI images also showed evidenceof a shift of the midbrain to the left with hyperintensity in themidbrain in the region of compression.The clinical picture ofipsilateral weakness in a patient with a subdural hematoma,evidence of compression of the midbrain in the CT andMRI of the brain, and the absence of any infarcts on thecontralateral side in diffusion weighted T1 and T2 sequencesof MRI confirmed our suspicion of Kernohan’s notch.
3. Discussion
The corticospinal tracts originate in the motor cortex in thefrontal lobes and descend through the internal capsules andsubsequently through the midbrain and pons, before themajority of the fibers (80%) decussate in the medulla. Due tothis decussation, the left cerebral motor cortex controls themovements of the right-side of the body and vice versa. Inthe midbrain, the pyramidal tract courses anteriorly in the

2 Case Reports in Medicine
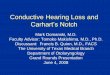
Figure 1: CT of the head showing gross posterior and lateral dis-placement of midbrain with deformity of the crus cerebri (pointedby the arrow) to the left side.Themidline ismarkedwith a black line.The subdural hematoma is visible on the right-side.
Figure 2: CT of the head after craniotomy and evacuation of subdu-ral hematoma showing persistent midline shift of the midbrain withdeformity of crus cerebri (marked by arrow).
crus cerebri. Due to the crossing of pyramidal tract fibersdownstream in the medulla, damage of the fibers in themidbrain results in paralysis of the opposite side of the body.The pyramidal tract controls discrete voluntary movements,like skilled and precise movements.
The explanation for ipsilateral hemiparesis to the side of aspace occupying lesion predates the invention ofMRI andCTimaging techniques. Kernohan and Woltman in an autopsystudy reported the presence of a notch in the midbrain
Subdural hematoma
Uncal herniation
Kernohan’s notch
Tentorium cerebelli
Figure 3: Schematic representation of Kernohan’s notch. Demon-strated here are a subdural hematoma and uncal herniation on thesame side. Notching of the midbrain is seen on the opposite side(Kernohan’s notch). This damages the contralateral pyramidal tractfibers in themidbrain and causes hemiparesis on the side of subduralhematoma.
contralateral to the side of the space occupying lesion due tocompression of the midbrain against tough dural reflectiontentorium cerebelli [1, 2] as shown in the schematic repre-sentation in Figure 3. This can damage the crus cerebri of themidbrain (carrying pyramidal fibers) resulting in complete,partial, or no disruption of the pyramidal fibers located init. Since the pyramidal fibers in the midbrain innervate theopposite side of the body, it results in paralysis ipsilateral tothe site of the lesion. The recovery after hemiplegia may becomplete, partial, or none depending on the extent of damageto pyramidal fibers. This phenomenon has been describedwith cerebral tumors, extradural hematoma, and subduralhematomas.
The recognition of this syndrome is critically important;if unrecognized, it may lead to surgery on the wrong sideof the brain. For example, 80 years after the description ofthis phenomenon by Kernohan, Wolf reported an unfortu-nate incident in which a patient presented with a subduralhematoma after getting hit by a golf stick [3]. The patient hadleft-sided weakness, and the CT of the head demonstrateda left-sided SDH. The surgeons thought that the left-rightmarkers of theCT scan imageweremisplaced. Two burr holesfollowed by a craniotomy on the right-side did not reveal anySDH. A CT of the head performed the next day showed thepresence of a right-sided craniotomy and a left-sided SDH.
Kernohan’s notch phenomenon has been previouslydemonstrated by MRI. An abnormal signal in T2-weightedimages on MRI in the contralateral midbrain may be amarker for poor neurological recovery [4]. CT scans havenot been thought to be helpful in diagnosing this condition.This is the first report of a CT scan being used to supportthe diagnosis of this syndrome. The CT scan obtained forthe diagnosis of an intracranial space occupying lesion canidentify contralateral midbrain compression as well. Thisalong with clinical features suggestive of ipsilateral pyramidaltract involvement can support a diagnosis of Kernohan’s

Case Reports in Medicine 3
notch. Use of a CT of the head for this purpose does notrequire additional imaging and is helpful in centers which donot have access toMRI. Above all, awareness of this syndromeand a high index of clinical suspicion are crucial for thediagnosis of Kernohan’s notch.
The concept of functional deterioration of a focus distantto the site of injury and its role in functional recovery aftera stroke was proposed more than a decade before Kernohanpublished his series of patients. Constantin von Monakovcoined the term diaschisis (Greek for shocked throughout) in1914; this term is used for sudden loss of function of a portionof the brain connected to a distant damaged area. The site ofdiaschisis and the originally damaged area are connected toeach other by neurons, or the damage could arise because ofdisturbances in regional blood flow [5]. Therefore, damageto a structure can affect the function of remaining intactsystems. Monakov proposed that there is a delicate balancebetween different components of the brain and an injury toa component could affect other parts of the brain even if it isnot anatomically damaged or close to the site of injury.
4. Conclusion
In summary, paralysis ipsilateral to the site of a lesion inthe brain could be due to compression of the contralat-eral cerebral peduncles against the tough dural reflectionscausing damage to the pyramidal tract fibers in the brainstem. This false localizing sign needs to be recognized toprevent inappropriate surgery andmedical management.Thepurpose of this case report is to increase the awareness of thissign and to promote the usefulness of CT scans to supportthis diagnosis. If this phenomenon is suspected, additionalcuts obtained at the midbrain level with 3D reconstruc-tion might be helpful for the diagnosis. More studies areneeded to determine if procedures like early surgery (evac-uation of hematoma/surgeries aimed at intracranial pressurereduction) in patients with clinical findings consistent withKernohan’s notch will help reduce the compression of themidbrain and its consequences.
Conflict of Interests
The authors declare that they have no conflict of interests.
Authors’ Contribution
All authors had access to the data, helpedwrite this paper, andapproved the final version of the paper.
References
[1] J.W. Kernohan andH.W.Woltman, “Incisura of the crus due tocontralateral brain tumor,” Mayo Clinic Proceedings, vol. 3, pp.69–72, 1928.
[2] J.W. Kernohan andH.W.Woltman, “Incisura of the crus due tocontralateral brain tumor,”Archives of Neurology and Psychiatry,vol. 21, no. 2, pp. 274–287, 1929.
[3] R. F. E. Wolf, C. A. Ter Weeme, and A. P. Krikke, “Kernohan’snotch andmisdiagnosis,”TheLancet, vol. 345, no. 8944, pp. 259–260, 1995.
[4] K. S. Moon, J. K. Lee, S. P. Joo et al., “Kernohan’s notchphenomenon in chronic subdural hematoma: MRI findings,”Journal of Clinical Neuroscience, vol. 14, no. 10, pp. 989–992,2007.
[5] E. Gonzalez-Aguado, J. Martı-Fabregas, and J. L. Martı-Vilalta,“The phenomenon of diaschisis in cerebral vascular disease,”Revue neurologique, vol. 30, no. 10, pp. 941–945, 2000.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com