Embed Size (px)
Citation preview

Int J Anat Res 2017, 5(2.3):3923-26. ISSN 2321-4287 3923
Case Report
FUSION OF TYPICAL THORACIC VERTEBRAENivedha Viswanathan*1, Ayesha Parveen 2, Yuvaraj Maria Francis 3, PriyaDharshini gowthaman. A 4.
ABSTRACT
Address for Correspondence: Ms. Nivedha Viswanathan, No.39, Ashok Brindavan Nagar, 1stmain road, Iyyappanthangal, Chennai-600056, Tamilnadu, India. E-Mail: [email protected]
Any abnormal fusion of vertebrae results in a clinical condition called block vertebrae or vertebral synostosis.Among all the known vertebral fusion, the fusion of thoracic vertebrae is less common and comparatively rare.During the formation of vertebral column in the 4th week of intrauterine life the sclerotome part of the somitesmigrate around the notochord and the neural tube and undergoes a process called resegmentation. Any defect insuch a process can lead to vertebral anomalies causing neurological signs and symptoms. The possible causefor the fusion of thoracic vertebra can be congential, vertebral malformations DISH (diffuse idiopathic skeletalhyperostosis) and other rheumatological degenerative diseases or infections like tuberculosis. This can lead towide complications affecting different systems of the body. The fusion of thoracic vertebra can present manyclinical signs including formation of abnormal curvatures of the spine like scolosis, kyphosisetc .the objectiveof the study is to present a case on the fusion of typical thoracic vertebra.KEY WORDS: Vertebral Malformations, Block Vertebrae, Scoliosis, Kyphosis, Sclerotome.
INTRODUCTION
International Journal of Anatomy and Research,Int J Anat Res 2017, Vol 5(2.3):3923-26. ISSN 2321-4287
DOI: https://dx.doi.org/10.16965/ijar.2017.219
Access this Article online
Quick Response code Web site: International Journal of Anatomy and ResearchISSN 2321-4287
www.ijmhr.org/ijar.htm
DOI: 10.16965/ijar.2017.219
*1,2 BPT Student, Saveetha College of Physiotherapy, Saveetha Univeristy, Chennai, Tamilnadu,India.3,4 Tutor, Department of Anatomy, Saveetha Medical College, Saveetha Univeristy, Chennai,Tamilnadu, India.
Received: 12 Apr 2017Peer Review: 12 Apr 2017Revised: None
Accepted: 23 May 2017Published (O): 30 Jun 2017Published (P): 30 Jun 2017
A typical vertebra consists of a vertebral archand foramen, a body, transverse processes andusually a spinous process. Thoracic vertebracompose the middle segment of the vertebralcolumn, between the cervical and lumbar verte-brae. In humans there are 12 thoracic vertebraewith the expections of T1, T9, T10, T11 and T12are called typical thoracic vertebrae. The Verte-brae develops from the sclerotome portions ofthe somites, which are derived from paraxialmesoderm.As development proceeds the sclero-tome portions of each somite undergoes aprocess called resegmentation. Resegmentation
occurs when the caudal half of each sclerotomegrows and fuses with cephalic half of each subadjavent sclerotome. Thus each vertebrae isformed fromthe combination of the caudal halfof one somite and the cranial half of itsneighbour. Mesenchymal cells between cepha-lic and caudal parts of the original sclerotomesegment do not proliferate but fill the spacebetween two precartilagenous vertebral bodies.In this way they contribute to the formation ofinvertebral discs.Congenital anamolies are common in the verte-bral column, awareness of vertebral anomaliesare useful to anastomosis and to clinicians as

Int J Anat Res 2017, 5(2.3):3923-26. ISSN 2321-4287 3924
Nivedha Viswanathan, Ayesha Parveen et al. FUSION OF TYPICAL THORACIC VERTEBRAE: A CASE REPORT.
these anomalies may be result in pain,decreased mobility, muscular weakness of limbsand sensory deficits [1,2]. It has got value forphysiciancs, surgeons, radiologists, orthopae-diciancs, anesthetics, rheumatologists, patholo-gists, paediatricians and for forensic medicinealso. Various vertebral anomalies of anatomicinterest have been reported viz, occipitalisation,sacralisation; lumbarisation absence of poste-rior elements of vertebral arch and vertebralsynostosis. fusion of vertebra at single or mul-tiple levels is reffered to as block veretebra orvertebral synostosis or spinal fusion [3]. The fu-sion of 2 or more vertebrae can be congenital oracquired. the fusion may be congential due tofailure of segmentation of sclerotomes atcertain levels at the time of organogenesis,leading to klippelfeil syndrome or other associ-ated spinal deformities such as scolosis [3]. Theacquired fusion of vertebrae is secondary totrauma, tuberculosis or other infections and ju-venile, rheumatoid arthritis [1]. Congenital fu-sion of vertebrae most commonly involves cer-vical regions [4,5]. The surgical fusion of 2 ver-tebrae is known as spondylodesis or spondylo-syndesis fusion of thoracic vertebrae can presentclinical signs like, congentials- colosis, shorten-ing of trunk with scoliosis or lordosis in olderchildren [6]. The spinal fusion may cause re-stricted movements, premature degenerativechanges and associated neurological deficits[5,7]. The symptoms may vary according to theextent and level of vertebral fusion.
While teaching the students, during normalclasses we adminstred a specimen of fusionbetween the typical thoracic vertebrae from theOsteology section of Anatomy department ofSaveetha Medical College, Thandalam. The fea-tures of the fused typical thoracic vertebrae wereanalysed and the specimen was photographedfrom anterior, posterior, right lateral, left lateraland superior aspect. The measurements of thefused vertebral specimen were taken with thehelp of digital vernier calliper. The parametersmeasured were heights of fused vertebralbodies, diameter and intervertebral foramen.
CASE REPORT
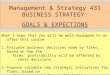
cic vertebrae. The features and measurementsof the fused vertebra are given in Table 1 andshown in Fig. 1-5. The table 2 indicates variousmeasurements of typical fused thoracic verte-brae,Fusion of three typical thoracic vertebrae: Thebodies of typical thoracic vertebrae werepartially fused on right side and partially fusedon left side. The pedicle, laminae articularprocesses, and spinous processes were unfused(Fig. 1-5).
OBSERVATIONSThe study details of a fused three typical thora-
Fig. 1: Posterior viewof fused vertebrae.
Fig. 2: Anterior viewof fused vertebrae.
Fig. 3: Left lateral viewof fused vertebrae.
Fig. 4: Right lateral viewof fused vertebrae.
Fig. 5: Superiorview of fused
vertebrae.
T3-T4 Fusion: The height of fused vertebralbodies was 3.6 cm on right side and 3.5 cm onleft side. The intervertebral foramen weremeasured 1.2 cm on right side and 0.9 cm onleft side (Table 1).

Int J Anat Res 2017, 5(2.3):3923-26. ISSN 2321-4287 3925
Nivedha Viswanathan, Ayesha Parveen et al. FUSION OF TYPICAL THORACIC VERTEBRAE: A CASE REPORT.
Table 1: Showing the measurements of fused typicalthoracic vertebrae.
S.no Feature T3-T4 T4-T5
PF- Right side PF- Right side
PF-Left side PF- Left side2 Pedicles UF UF3 Laminae UF UF4 Articular processes UF UF5 Spinous processes UF UF6 Vertebral foramen REGULAR REGULAR
Right -Oblique, 1.2; Right-Arcuate, 1.3;Left -Arcuate, 0.9 Left -Oblique, 1.0
1Vertebral bodies Height
[(Right +Left )/2]
7 Intervertebral foramen
Note: CF: Complete fusion, PF: Partial fusion,UF: Unfused,
T4-T5 Fusion: The height of fused vertebralbodies was 3.9 cm on right side and 4.1 cm onleft side. The intervertebral foramen measured1.3cm on right side and 1.0 cm on left side (Tab.2)Table 2: Various parameters of different parts of thoracicvertebrae.
Transverse 2.4cm 2.7cm Antero-posterior 1.4cm 1.5cm
On right side
S.No view Upper
vertebra Lower
vertebra
1 Body 1.3cm 1.6cmAntero-posterior
Parts of vertebra
3 Vertebral for amen 0.8
On left side 0.8
2 Spinal canal Transverse 1.9cm 1.8cm
time of organogenesis. The non segmentationof the primitive sclerotome is the causes for thefusion of vertebrae called block vertebrae orfused vertebrae. Congential fusion arecharacterised by absence of the intervertebraldisc. Or its replacement by radio opaque linethe wasp- waist appearance, smooth intervertebralforamina, a single spinous process for twovertebral bodies and maintenance of vertebralbody height on x-ray examination [10]. Blockvertebrae results in disturbance in posturalbiomechancics causing degenerative changesand disc prolapsed at the adjoining segmentsin advance age [5]. Fusion between the typicalthoracic vertebrae and lumbar vertebrae werereported by vadgaouear et al. which can causelow back pain [3]. early diagnosis of theseanomalies will be helpful in documenting thechange due to an injury, ageing or progressionof a degenerative process and also motivatesthe patients to change their life styles to lead anormal life [7].In the congenitally fused vertebrae, the anterio-posterior diameter of the vertebrae is decreasedand the individual measumerents of the twovertebraes bodies height is equal to the twofused vertebraes height including the inter-ver-tebral disc.Vertebral synostosis is the hallmark of KFS, atraid of short neck mobility [1]. Acquired fusionof vertebrae may be subsequently shorting ofthe trunk. The thoracic vertebrae and the inter-vening disc along with ribs help in maintain theshape and length of the thorax.Fusion of the vertebrae and the absence of thedisc will narrow the thorax that can lead torespiratory distress. Asphyxiating thoracicdystrophy is caused by narrow thorax and shortribs [11, 12] congenital block vertebrae may beassociated with other systematic anomalies thatincludes abnormal spinal curvatures scoliosis,etc , sprengels deformity, hemivertebrae,platybasia, basilar impression, spina bifida, clibfeet, anomalies involving kidney and the ribs(cervical rib)cleft palate, respiratory problems,deafness or hearing impairment and cardiacanomalies [6,13] various syndromes associa-tions of vertebral fusion are segmentationsyndrome with laryngeal malformations,VACTERL (s) (vertebral, Anal, Cardiovascular,
DISCUSSION
The vertebral column develops from pairedsomites, each composed of a dermatome,myotome, and sclerotome. They arise initiallyin cervical region, [4th week] increasing innumber craniocaudally. In the 5th week, thesclerotome cells of the somites lose theiradherence and migrate to the vertebral centrum,neural process and costal processes. Eachthoracic neural process gives rise to a cartilagi-nous pedicle, transverse process and lamina.The ossification centre arises, one for thecentrum and one for the neural process, theirtiming is idiosyncratic starting in the 4th monthat T10 and L1 centra and C2 and T1 neuralprocess and spreading up and down the column[8]. Radiologically , three types of vertebralfusion have been described, single fusedcervical segment seen in 25% of patientsmultiple contiguous fused segments seen in 25%patients and multiple non –contiguous fusedseen in 50% patients[9].The segmentation of the vertebrae occurs at the

Int J Anat Res 2017, 5(2.3):3923-26. ISSN 2321-4287 3926
Nivedha Viswanathan, Ayesha Parveen et al. FUSION OF TYPICAL THORACIC VERTEBRAE: A CASE REPORT.
Tracheo –oesophageal, renal and limbabnormalities), Mullerian duct aplasia, Renalaplasia, Cervico – thoracic somite dysplasia),diabetic embryopathy, trisomy 18, joubert,jarcho-levin syndrome, etc [14].Pathological causes of fusion of vertebrae arefibro – dysplasia progressive juvenile rheuma-toid arthritis etc [15]. The differentiation andresegmentation of vertebrae occurs at the timeof organogenesis. It explains the association ofvertebral synostosis with cardiac, renal,musculoskeletal and neural abnormalities [16].
CONCLUSION
Thoracic vertebral fusion usually results due tocongenital or acquired causes and vertebralfusion can be helpful feature for identification.The study has provided additional informationof the anatomy and morphology of thoracicvertebral fusion and their embryological basisand clinical significance. These details are clini-cally important as they might be associated with,neurological and musculoskeletal abnormalities.
[4]. Seaver LH, Boyd E. Spondyloc arpotar salsynost osissyndrome and cervical instability. PubmedAm J MedGenet, 2000;91(5):340-344.
[5]. Soni P, Sharma V, Sengupta J. Cervical vertebralanomalies- incidental findings on lateralcephalograms. The Angle Orthodontist,2008;78(1):176-180.
[6]. Fernandes T, Costa C. Klippel-Feil syndrome withother associated anomalies in a medieval Portugeseskeleton (13th – 15th century). J Anat.,2007;211:681-685.
[7]. Shankar VV and Roopa R Kulkarni. Block vertebra,Fusion of axis with the third cervical vertebra- acase report. International Journal of AnatomicalVariation, 2011;4:15-16.
[8]. Brookes M, Zietman A. Clinical Embryology. USA:Library of Congress; 1998: 293.
[9]. Johansen JG, mccartyDJ, Haughton VM. Retrosomaticclefts: computed tomographic appearance. Radiol-ogy, 1983;148:447-448.
[10]. Brown MW, Templeton AW, Hodges FJ III. The inci-dence of acquired and congenital fusion in the cer-vical spine. Am J Radiology, 1964;92:1255-1259.
[11]. Bhargava S. Radiological Differential Diagnosis. 1stedition, Jaypee Brothers, New Delhi, 2005:528.
[12]. Thomas D, Kulkarni BG. A case of fusion of thoracicvertebra. Journal of Ayurveda and Holistic Medi-cine, 2013;1(5):23-26.
[13]. Batra S, Ahuja S. Congenital Scoliosis: Managementand future directions. ActaorthopedicaBelgica,2008;74:147-160.
[14]. Victor’s Notes. Cranial and vertebral anomalies.Dev 9(1) updated by May 13, 2010.
[15]. Clarke RA, Catalan G, Diwan AD, Kearsley JH. Het-erogeneity in Klippel-Feil syndrome: a new classifi-cation. Paediatric Radiology, 1998;28:967-974.
[16]. Kulkarni V, Ramesh BR. A spectrum of vertebral synos-tosis. International Journal of Basic and AppliedMedical Sciences, 2012;2(2):71-77.
Conflicts of Interests: None
REFERENCES
[1]. Erdil H, Yildiz N, Cimen M. Congenital fusionof cer-vical vertebrae and its clinicalsignificance. Jour-nal of Anatomical Society ofIndia, 2003;52(2):125-127.
[2]. Wazir S, Mahajan A. Fusion of axis with third cervi-cal vertebra-a case report. Indian J FundamentalApplied Sciences, 2011;1(4):164-166.
[3]. Kulkarni V, Ramesh BR. A spectrum of vertebralsynostosis. International Journal of Basic and Ap-plied Medical Sciences, 2012;2(2):71-77.
How to cite this article:Nivedha Viswanathan, Ayesha Parveen, Yuvaraj Maria Francis,Priya Dharshini gowthaman. A. FUSION OF TYPICAL THORACICVERTEBRAE: A CASE REPORT. Int J Anat Res 2017;5(2.3):3923-3926. DOI: 10.16965/ijar.2017.219