Embed Size (px)
Citation preview

Int J Clin Exp Pathol 2016;9(3):4073-4077www.ijcep.com /ISSN:1936-2625/IJCEP0020362
Case ReportEwing sarcoma/peripheral primitive neuroectodermal tumor of the kidney: report of two cases
Dan Nie1,2*, Yu Yang3*, Nana Zhang1,2, Yuan Qiu1,2, Jianfeng You1,2, Michael A McNutt1, Hua Wang1,2
1Department of Pathology, Peking University Health Science Center, Beijing, China; 2Department of Pathology, Peking University Third Hospital, Beijing, China; 3Department of Pathology, University of Texas Medical Branch, Galveston, Texas, USA. *Equal contributors.
Received November 23, 2015; Accepted January 25, 2016; Epub March 1, 2016; Published March 15, 2016
Abstract: Ewing sarcoma/peripheral primitive neuroectodermal tumor (ES/pPNET) arising in the kidney is very rare, and only a few cases have been reported. Here we present two cases of renal ES/pPNET with different prognosis. Both patients underwent radical nephrectomy. One patient had complex EWSR1 gene chromosome translocation, high Ki-67 proliferative index and died of metastatic disease 2 months after surgery. The other patient had conven-tional EWSR1 gene translocation, low Ki-67 proliferative index and is alive with no evidence of disease after 4 year follow-up.
Keywords: Kidney, Ewing sarcoma/peripheral primitive neuroectodermal tumor, immunohistochemistry, fluores-cence in situ hybridization
Introduction
Ewing sarcoma/peripheral primitive neuroecto-dermal tumor (ES/pPNET) is a small round cell sarcoma of presumed neuroectodermal origin which typically originates in bone or soft tissue. ES/pPNET is rare in the kidney [1], and gener-ally occurs in young adults and exhibits highly aggressive biological behavior [2]. Here we present two cases of renal ES/pPNET.
Materials and methods
Patient 1
A 27-year-old female presented with lumbar pain which radiated to the lower limbs. At pre-sentation, she had bloody urine and an aching sensation in her upper limbs. Ultrasound and CT scanning revealed a 17 × 17 × 10 cm3 solid-cystic right renal mass. The patient was clini-cally diagnosed as renal cancer and underwent a right radical nephrectomy. This tumor involved the upper part of kidney, was adherent to the liver and grossly measured 17 cm in greatest dimension. It was poorly-circumscribed and composed of solid and cystic areas. Microscopically, the tumor was composed of
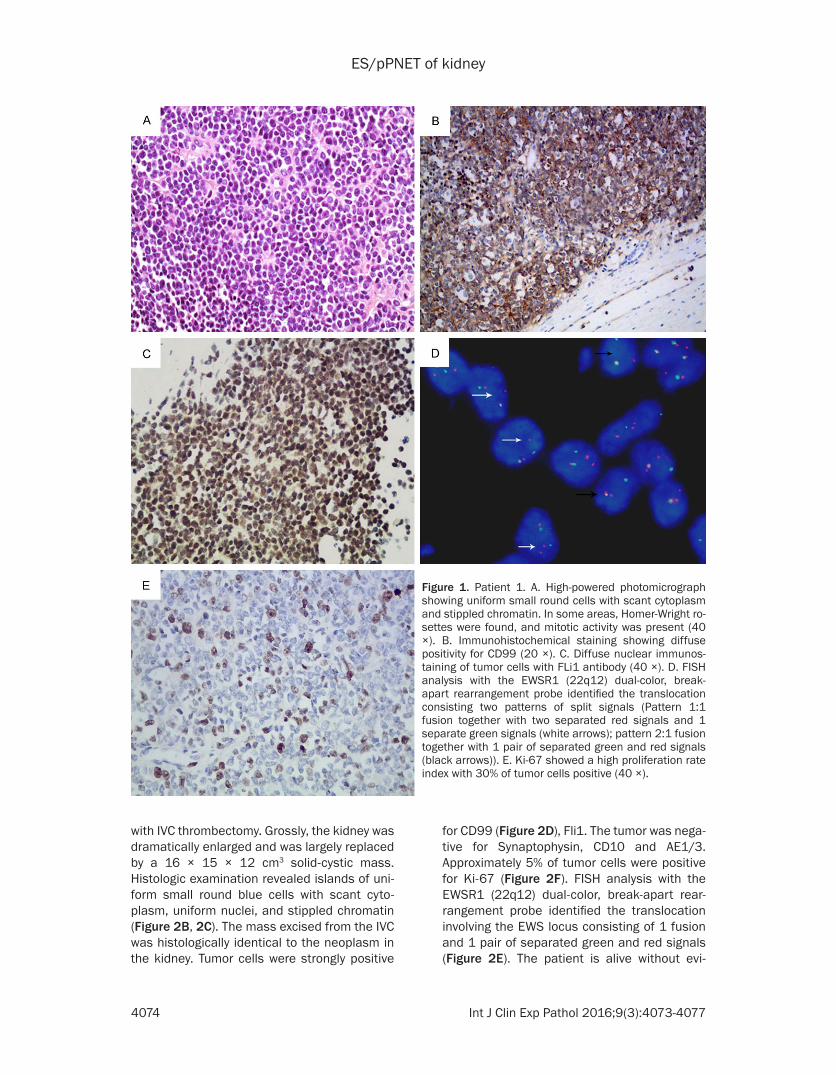
monomorphic small round cells. Homer-Wright rosettes and significant mitotic activity were present (Figure 1A). Immunohistochemical staining showed that tumor cells were positive for CD99 (Figure 1B), Synaptophysin, Chromo- granin A, NSE, Fli1 (Figure 1C) and S-100, and negative for LCA and AE1/3. Approximately 30% of tumor cells were positive for Ki-67 (Figure 1E). Fluorescence in situ hybridization (FISH) analysis showed rearrangement of the EWSR1 region in 22q12 consisting of 2 pat-terns of split signals: Sixty seven percent (67%) of tumor cells showed 1 fusion together with two separated red signals and 1 separate green signals, while 15% of tumor cells showed 1 fusion, together with 1 pair of separated green and red signals (Figure 1D). The patient died 2 months after surgery secondary to bone metastasis.
Patient 2
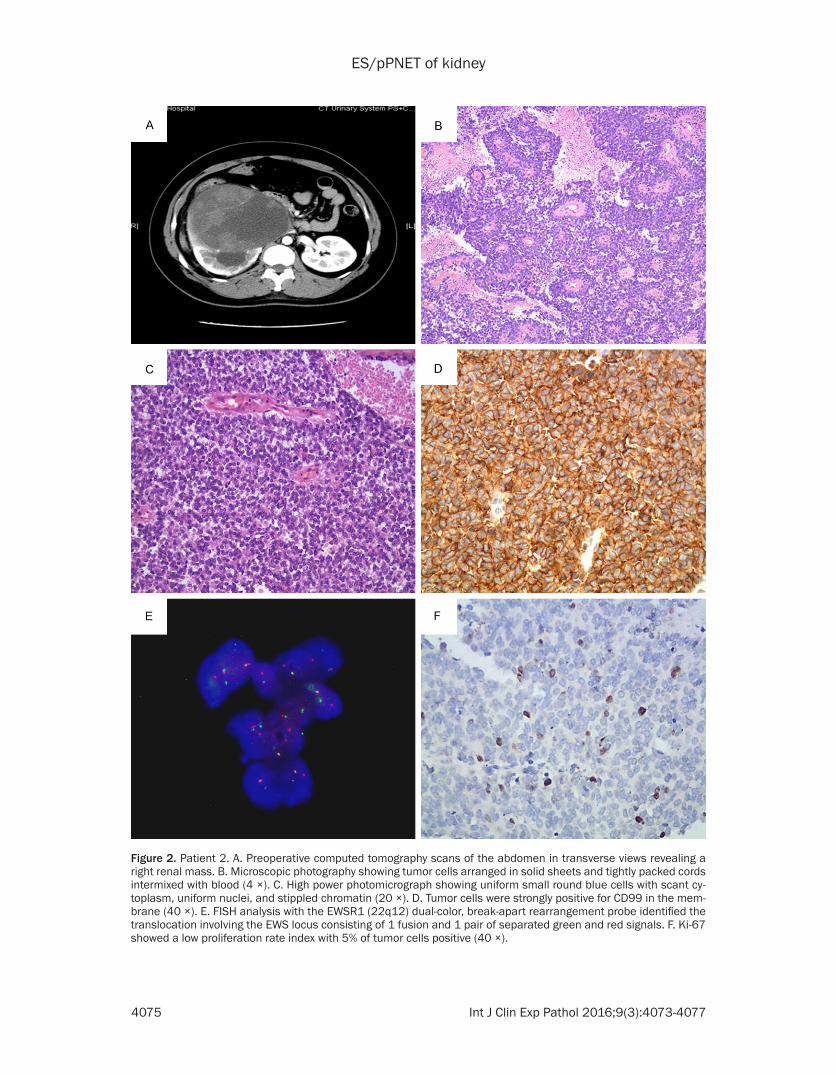
A 24-year-old female presented with right lum-bar pain which increased in severity upon move-ment. A CT scan revealed a 16 × 15 × 13 cm3 mass in the right kidney with tumor thrombus in the inferior vena cava (IVC) (Figure 2A). The patient underwent right radical nephrectomy
ES/pPNET of kidney
4074 Int J Clin Exp Pathol 2016;9(3):4073-4077
with IVC thrombectomy. Grossly, the kidney was dramatically enlarged and was largely replaced by a 16 × 15 × 12 cm3 solid-cystic mass. Histologic examination revealed islands of uni-form small round blue cells with scant cyto-plasm, uniform nuclei, and stippled chromatin (Figure 2B, 2C). The mass excised from the IVC was histologically identical to the neoplasm in the kidney. Tumor cells were strongly positive
for CD99 (Figure 2D), Fli1. The tumor was nega-tive for Synaptophysin, CD10 and AE1/3. Approximately 5% of tumor cells were positive for Ki-67 (Figure 2F). FISH analysis with the EWSR1 (22q12) dual-color, break-apart rear-rangement probe identified the translocation involving the EWS locus consisting of 1 fusion and 1 pair of separated green and red signals (Figure 2E). The patient is alive without evi-
Figure 1. Patient 1. A. High-powered photomicrograph showing uniform small round cells with scant cytoplasm and stippled chromatin. In some areas, Homer-Wright ro-settes were found, and mitotic activity was present (40 ×). B. Immunohistochemical staining showing diffuse positivity for CD99 (20 ×). C. Diffuse nuclear immunos-taining of tumor cells with FLi1 antibody (40 ×). D. FISH analysis with the EWSR1 (22q12) dual-color, break-apart rearrangement probe identified the translocation consisting two patterns of split signals (Pattern 1:1 fusion together with two separated red signals and 1 separate green signals (white arrows); pattern 2:1 fusion together with 1 pair of separated green and red signals (black arrows)). E. Ki-67 showed a high proliferation rate index with 30% of tumor cells positive (40 ×).
ES/pPNET of kidney
4075 Int J Clin Exp Pathol 2016;9(3):4073-4077
Figure 2. Patient 2. A. Preoperative computed tomography scans of the abdomen in transverse views revealing a right renal mass. B. Microscopic photography showing tumor cells arranged in solid sheets and tightly packed cords intermixed with blood (4 ×). C. High power photomicrograph showing uniform small round blue cells with scant cy-toplasm, uniform nuclei, and stippled chromatin (20 ×). D. Tumor cells were strongly positive for CD99 in the mem-brane (40 ×). E. FISH analysis with the EWSR1 (22q12) dual-color, break-apart rearrangement probe identified the translocation involving the EWS locus consisting of 1 fusion and 1 pair of separated green and red signals. F. Ki-67 showed a low proliferation rate index with 5% of tumor cells positive (40 ×).

ES/pPNET of kidney
4076 Int J Clin Exp Pathol 2016;9(3):4073-4077
dence of recurrence after 4 years follow-up after diagnosis.
Discussion
Renal ES/pPNET is usually not identified at an early stage because of the rapid growth of this neoplasm and its deep location. In both of these cases, the renal masses were very large at the time of discovery, and both cases were clinically misdiagnosed as renal cell carcinoma [3, 4].
The differential diagnosis of ES/pPNET in the kidney is broad and includes small cell neuro-endocrine carcinoma, lymphoma, desmoplas-tic small round cell tumor, neuroblastoma, synovial sarcoma, neuroepithelial tumor, and Wilm’s tumor. There is considerable morpho-logic and immunohistochemical overlap among these tumors [4], and accurate diagnosis of ES/pPNET must incorporate several different diag-nostic modalities [5]. Morphologic findings and immunohistochemistry are critical in ES/pPNET diagnosis, as they may be used to exclude many neoplasms from the differential diagno-sis at the outset. CD99 and Fli1 are the primary positive markers for diagnosis of ES/pPNET, but can also be positive in variety of non-ES/pPNET including Wilm’s tumor, vascular malig-nancies, lymphoblastic lymphoma, and neuro-endocrine tumors which may confound the diagnosis. Cytogenetics thus plays a critical role in the diagnosis of this poorly differentiat-ed neoplasm. EWSR1 gene rearrangements on chromosome 22 have been suggested as a useful tool for confirming ES/pPNET [6-8]. However, t (11;22) can also be seen in desmo-plastic small round cell tumor and rhabdomyo-sarcoma [9, 10]. Nonetheless, in the context of appropriate histologic findings and immunohis-tochemical profile, the diagnosis of ES/pPNET can be made with certainly.
It is of interest that our FISH study demonstrat-ed two patterns of split signals using FISH with the EWSR1 break-apart rearrangement probe in patient 1 (Figure 1D), in contrast to patient 2 (Figure 2E) where only one pattern of split sig-nals (consisting of 1 fusion and 1 pair of sepa-rated green and red signals) was found. This phenomenon has not previously been described in ES/pPNET. This intriguing observation indi-cates that there is another translocation within -500 kb flanking the 5’ side of the EWSR1 gene
(22q12), in addition to the well-known location of the EWSR1 gene translocation. This complex chromosome translocation suggests that the tumor may have dynamic change in the genome resulting in genomic instability and acquire more capabilities for tumor growth and pro-gression. Whether this phenomenon is associ-ated with high tumor cell proliferation index and poor prognosis in this patient warrants further study.
Renal ES/pPNET with IVC tumor thrombus is very rare [11]. To date, data on surgical out-come and prognosis after radical nephrectomy and thrombectomy are sparse. In this report, the patient 2 is still alive without evidence of recurrence after a 4 year follow-up. Although this follow-up period is limited, it suggests IVC tumor thrombus in renal ES/pPNET is not asso-ciated with survival after aggressive surgical resection. The proliferation index determined with Ki-67 is used widely as a significant inde-pendent prognostic marker in a variety of malig-nancies including ES/PNETs [12], and high per-centages of Ki-67-positive tumor cells correlate with tumor progression and unfavorable clinical outcome. In this report, Ki-67-positive tumor cells in patient 1 (30%) are much higher than that in patient 2 (5%), which is consistent with the significantly poorer prognosis in this patient (case 1).
In summary, we have presented two rare cases of primary renal ES/pPNET with different prog-nosis. Both patients underwent nephrectomy. One patient died of metastatic disease 2 months after surgery and the other is alive with no evidence of disease after 4 year follow-up.
Acknowledgements
This work was supported by the National Natural Science Foundation of China (Grant No. 81272945) and the Beijing Natural Science Foundation of China (Grant No. 7122100).
Disclosure of conflict of interest
None.
Address correspondence to: Dr. Hua Wang, De- partment of Pathology, Peking University Health Science Center; Department of Pathology, Peking University Third Hospital, Beijing 100191, China. Tel: 86-10-82805489; E-mail: [email protected]
ES/pPNET of kidney
4077 Int J Clin Exp Pathol 2016;9(3):4073-4077
References
[1] Castro EC and Parwani AV. Ewing sarcoma/primitive neuroectodermal tumor of the kid-ney: two unusual presentations of a rare tu-mor. Case Rep Med 2012; 2012: 190581.
[2] Rowe RG, Thomas DG, Schuetze SM, Hafez KS, Lawlor ER, Chugh R. Ewing sarcoma of the kid-ney: case series and literature review of an of-ten overlooked entity in the diagnosis of pri-mary renal tumors. Urology 2013; 81: 347-353.
[3] Bing Z, Zhang P, Tomaszewski JE, Maclennan GT. Primary Ewing sarcoma/primitive neuroec-todermal tumor of the kidney. J Urol 2009; 181: 1341-1342.
[4] Karpate A, Menon S, Basak R, Yuvaraja TB, Tongaonkar HB, Desai SB. Ewing sarcoma/primitive neuroectodermal tumor of the kid-ney: clinicopathologic analysis of 34 cases. Ann Diagn Pathol 2012; 16: 267-274.
[5] Saxena R, Sait S, Mhawech-Fauceglia P. Ewing sarcoma/primitive neuroectodermal tumor of the kidney: a case report. Diagnosed by immu-nohistochemistry and molecular analysis. Ann Diagn Pathol 2006; 10: 363-366.
[6] Kang SH, Perle MA, Nonaka D, Zhu H, Chan W, Yang GC. Primary Ewing sarcoma/PNET of the kidney: fine-needle aspiration, histology, and dual color break apart FISH assay. Diagn Cyto-pathol 2007; 35: 353-357.
[7] Bridge RS, Rajaram V, Dehner LP, Pfeifer JD, Perry A. Molecular diagnosis of Ewing sarco-ma/primitive neuroectodermal tumor in rou-tinely processed tissue: a comparison of two FISH strategies and RT-PCR in malignant round cell tumors. Mod Pathol 2006; 19: 1-8.
[8] Yang Y, Zhang L, Wei Y, Wang H, Xiong W, Chen Z, Hes O, Zheng J. Detection of EWSR1 translo-cation with nuclear extraction-based fluores-cence in situ hybridization for diagnosis of Ew-ing’s sarcoma/primitive neuroectodermal tumor. Anal Quant Cytol Histol 2007; 29: 221-230.
[9] Wang LL, Perlman EJ, Vujanic GM, Zuppan C, Brundler MA, Cheung CR, Calicchio ML, Dubois S, Cendron M, Murata-Collins JL, Wenger GD, Strzelecki D, Barr FG, Collins T, Perez-Atayde AR, Kozakewich H. Desmoplastic small round cell tumor of the kidney in childhood. Am J Surg Pathol 2007; 31: 576-584.
[10] Thorner P, Squire J, Chilton-MacNeil S, Marra-no P, Bayani J, Malkin D, Greenberg M, Lo-renzana A, Zielenska M. Is the EWS/FLI-1 fu-sion transcript specific for Ewing sarcoma and peripheral primitive neuroectodermal tumor? A report of four cases showing this transcript in a wider range of tumor types. Am J Pathol 1996; 148: 1125-1138.
[11] Fergany AF, Dhar N, Budd GT, Skacel M, Garcia JA. Primary extraosseous Ewing sarcoma of the kidney with level III inferior vena cava thrombus. Clin Genitourin Cancer 2009; 7: E95-E97.
[12] Grotzer MA, Geoerger B, Janss AJ, Zhao H, Rorke LB, Phillips PC. Prognostic significance of Ki-67 (MIB-1) proliferation index in child-hood primitive neuroectodermal tumors of the central nervous system. Med Pediatr Oncol 2001; 36: 268-273.





























