Embed Size (px)
Citation preview

Case ReportCardiac Arrest after Local Anaesthetic Toxicity ina Paediatric Patient
Liana Maria Torres de Arauacutejo Azi Diego Grimaldi Figueroa and Ana Ameacutelia Souza Simas
Edgard Santos Professor University Hospital Federal University of Bahia Salvador BA Brazil
Correspondence should be addressed to Liana Maria Torres de Araujo Azi lianaaraujoufbabr
Received 27 August 2016 Accepted 10 October 2016
Academic Editor Kuang-I Cheng
Copyright copy 2016 Liana Maria Torres de Araujo Azi et al This is an open access article distributed under the Creative CommonsAttribution License which permits unrestricted use distribution and reproduction in any medium provided the original work isproperly cited
We report a case of a paediatric patient undergoing urological procedure in which a possible inadvertent intravascular orintraosseous injection of bupivacaine with adrenaline in usual doses caused subsequent cardiac arrest completely reversed afteradministration of 20 intravenous lipid emulsion Early diagnosis of local anaesthetics toxicity and adequate cardiovascularresuscitation manoeuvres contribute to the favourable outcome
1 Introduction
The caudal block is a procedure often used as a comple-mentary method of analgesia in paediatric surgery Possiblecomplications of the procedure include intravascular sub-arachnoid or intraosseous injections all with catastrophicconsequences for patients Intravascular injection occurs inabout 13 to 10000 caudal blocks [1]
Overdose toxicity of local anaesthetics has long beenknown but its therapy has gained a new ally with the use oflipid emulsions in their treatment [2]
Acceptable theories by which lipid therapy reverses localanaesthetic cardiotoxicity are the ldquolipid sinkrdquo (increasing theclearance of the local anaesthetic from cardiac tissue) and theinhibition of myocardial fatty acid oxidation by the phospho-lipid [2]
Consent was obtained from the patient for publication ofthis case
2 Case Presentation
A 6-year-old male child 22 kg with congenital glaucoma(using Timolol drops for three years) was posted for hypospa-dias repair Uneventful general anaesthesia (GA) inductionwith fentanyl 100mcg Propofol 60mg and Rocuronium15mg occurred and he was intubated with a 55 cuffedVolume-controlledmechanical ventilation (TV=200mLand
RR = 18 rpm PEEP = 5 cmH2O O260 in 16 sevoflurane)
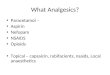
was started and a caudal block in lateral position wasperformed without difficulty with 12mL of 05 bupivacainewith epinephrine (lack of resistance technique) after negativeaspiration for blood or CSF After supine position the patientimmediately presented hypotension (BP = 60 times 32mmHg)and cardiac rhythm of ventricular tachycardia with pulse(HR = 176 bpm) Amiodarone hydrochloride 50mg andepinephrine 20mcg reverted the rhythm to sinus (HR =148 bpm BP = 80 times 45mmHg) FiO
2was raised to 100
Local anaesthetic intoxication was hypothesized and lipidemulsion was requested About two minutes later the patienthad cardiac arrest (pulseless ventricular tachycardia inter-spersed with ventricular fibrillation) and cardiopulmonaryresuscitation was initiated Amiodarone 50mg + epinephrine40mcg was given and a three-time one-minute intravenousbolus injection of 20 lipid emulsion 10mLsdotkgminus1 was givenwith prompt reversion to sinus rhythmThen an intravenousinfusion of 20 lipid emulsion at 025mLsdotkgminus1sdotminminus1 wasadministered in the next 30 minutes Surgery was cancelled
The patient also had two new cardiac arrests in pulselesselectrical activity about four and nine minutes later from theprevious reversal treated with effective cardiac resuscitationand 40mcg bolus of adrenaline Adrenaline infusion at doses01ndash04mcgsdotkgminus1sdotminminus1 was begun Thereafter the patienthad no further episodes of arrests Left femoral artery was
Hindawi Publishing CorporationCase Reports in AnesthesiologyVolume 2016 Article ID 7826280 3 pageshttpdxdoiorg10115520167826280
2 Case Reports in Anesthesiology
30hours
3days
VT
with
pul
se B
P=60times32
mm
Hg
HR=176
bpm
Sinu
s rhy
thm
BP=80times45
mm
Hg
HR=148
bpm
VT
with
out p
ulse
inte
rspe
rsed
with
VF
Disc
harg
ed h
ome
Extu
batio
n w
ithou
t seq
uela
e
Pulse
less
elec
tric
al ac
tivity
ECG
Pulse
less
elec
tric
al ac
tivity
ECG
2998400 1
9984001998400
4998400
9998400
30998400
Amiodarone 50mg +
Amiodarone 50mg +
epinefrine 20mcg
epinefrine 40mcg +
20 ILE 1mLmiddotkgminus1
20 ILE 1mLmiddotkgminus1
20 ILE 1mLmiddotkgminus1
Epinefrine 40mcg
20 ILE 0 25 mLmiddot
Epinefrine 40mcg + epinefrine 01ndash04mcgmiddot
kgminus1middotminminus1
kgminus1middotminminus1
Caud
al b
lock
12
mL05
b
upiv
acai
ne w
ith ep
inep
hrin
e
Figure 1
punctured and urinary catheterization for diuresis monitor-ing was done Blood gas analysis showed pH = 709 pO
2
= 86mmHg pCO2= 46mmHg HCO
3= 14mEqL BE =
minus158 and Sat = 93 Despite respiratory acidosis lactateconcentration was nearly normal (17mmolsdotLminus1) He wastransferred to the Intensive Care Unit and the adrenaline wasturned off after 5 hours of its onset (Figure 1) As perfusionimproved respiratory acidosis disappeared blood lactate leveldecreased to 08mmolsdotLminus1The patient was kept sedated untilnormalization of pulmonary and tissue perfusion parametersComputed tomography of the brain showed no brain damageHe was extubated without sequelae thirty hours after theepisode and was discharged home three days later Formalconsent for publication was obtained from patientrsquos mother
3 Discussion
Local anaesthetic toxicity has been reported with almost allkind of regional blocks including peripheral blockades [3]and caudal blocks [4] The caudal block is the most easilylearned of all regional anaesthetic techniques It has relativelylow risk of complications and a high rate of success Atesting dose can be used to exclude intravascular injectionand althoughdesirable it is not commonly performed bymostanaesthesiologists In this case the ease of injection was usedas a parameter for correct placement The choice of a longer-acting amide LA such as bupivacaine improves analgesiaafter surgery but its cardiotoxicity limits its use [5] Additionof vasoconstrictors such as epinephrine can dramaticallyslow its absorption improving its safety and prolonging the
anaesthesia [1] In this case the limit dose (3mgsdotkgminus1) was notachieved and the typical description of progressive biphasicsymptoms affecting first the CNS and then CVS [6] was notseen as he was sedated and curarized
Beta blockade with Timolol drops before surgery mayhave difficult cardiac arrest reversion and it could also justifythe increasing necessities of adrenaline to maintain hemo-dynamic stable status
Intravenous lipid emulsion is a method for rescue forcardiovascular collapse after an inadvertent intravenousinjection of local anaesthetics [7] In cardiac arrest caused bybupivacaine intoxication first-line rescue with epinephrineand epinephrine + intravenous lipid emulsion (ILE)wasmoreeffective with regard to survival [8] There are several casereports of successful resuscitation after cardiovascular col-lapse in the adult population but examples in children arescarce and this case seems to be the second one showingfeatures of ventilationperfusion (VP) mismatch after ILEin child [4] The doses used in this case followed the ASRAPracticeAdvisory [9 10] and resulted in a complete stop of thearrests about 20 minutes after the beginning of its infusion
If ventilation or perfusion is unstable a ventilationperfu-sion (VQ) mismatch can occur It can be caused by bloodshunting for example during atelectasis or by dead space inthe lungs for example with a pulmonary embolism hypo-volemia or on postarrest period in an intubated and well-ventilated patient Gas analysis just after cardiac recoveryshowed respiratory acidosis due to VQ mismatch Inad-equate pulmonary perfusion (yet) to adequately ventilatedareas of the lung impairs gas exchange and leads to hypoxia
Case Reports in Anesthesiology 3
[11] FiO2was set to 100 to target SaO
2to 90ndash94 in the
postcardiac arrest periodDespite the fact that it would have resulted in the same
consequences (subsequently pulseless electrical activity car-diac arrest) defibrillation using 2 Joulessdotkgminus1 would be moresuitable than amiodarone as the first choice for treatmentof the second cardiac arrest Induced hypothermia was notperformed according to PALS guideline [12]
This case is remarkable because due to the rapid onsetof cardiac symptoms intraosseous injection cannot be ruledout Appropriate conduction of the case favoured a postarrestperiod without complications
Ethical Approval
The responsible institutional review board of our institutiongave permission to publish this report
Disclosure
This report was previously presented in part at theMedicallyChallenging Case poster presentation at the ASA AnnualMeeting 2013
Competing Interests
All the authors declare that there is no conflict of interestsregarding this publication
References
[1] E Giaufre ldquoCaudal anesthesia in childrenrdquoCahAnesthesiol vol43 no 3 pp 281ndash286 1995
[2] S Ciechanowicz and V Patil ldquoLipid emulsion for local anes-thetic systemic toxicityrdquo Anesthesiology Research and Practicevol 2012 Article ID 131784 11 pages 2012
[3] I Kamel G Trehan and R Barnette ldquoIntralipid therapy forinadvertent peripheral nervous system blockade resulting fromlocal anesthetic overdoserdquo Case Reports in Anesthesiology vol2015 Article ID 486543 3 pages 2015
[4] U Shenoy J Paul and D Antony ldquoLipid resuscitation in pedia-tric patientsmdashneed for cautionrdquo Paediatric Anaesthesia vol 24no 3 pp 332ndash334 2014
[5] P-A Lonnqvist and N S Morton ldquoPostoperative analgesia ininfants and childrenrdquo British Journal of Anaesthesia vol 95 no1 pp 59ndash68 2005
[6] M F Mulroy ldquoSystemic toxicity and cardiotoxicity from localanesthetics incidence and preventivemeasuresrdquoRegional Anes-thesia and Pain Medicine vol 27 no 6 pp 556ndash561 2002
[7] M S Ozcan andGWeinberg ldquoUpdate on the use of lipid emul-sions in local anesthetic systemic toxicity a focus on differen-tial efficacy and lipid emulsion as part of advanced cardiac lifesupportrdquo International Anesthesiology Clinics vol 49 no 4 pp91ndash103 2011
[8] J Mauch O M Jurado N Spielmann R Bettschart-Wolfens-berger and M Weiss ldquoResuscitation strategies from bupiva-caine-induced cardiac arrestrdquo Paediatric Anaesthesia vol 22no 2 pp 124ndash129 2012
[9] J M Neal C M Bernards J F Butterworth et al ldquoASRApractice advisory on local anesthetic systemic toxicityrdquoRegionalAnesthesia and Pain Medicine vol 35 no 2 pp 152ndash161 2010
[10] J M Neal M F Mulroy and G L Weinberg ldquoAmericanSociety of Regional Anesthesia and Pain Medicine checklistfor managing local anesthetic systemic toxicity 2012 versionrdquoRegional Anesthesia and Pain Medicine vol 37 no 1 pp 16ndash182012
[11] F A Donoso S D Arriagada R F Dıaz and R P Cruces ldquoVen-tilation strategies in the child with severe hypoxemic respir-atory failurerdquoGacetaMedica deMexico vol 151 no 1 pp 75ndash842015
[12] M E Kleinman A R De Caen L Chameides et al ldquoSpecialreportmdashpediatric basic and advanced life support 2010 interna-tional consensus on cardiopulmonary resuscitation and emer-gency cardiovascular care science with treatment recommenda-tionsrdquo Pediatrics vol 126 no 5 pp e1261ndashe1318 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Case Reports in Anesthesiology
30hours
3days
VT
with
pul
se B
P=60times32
mm
Hg
HR=176
bpm
Sinu
s rhy
thm
BP=80times45
mm
Hg
HR=148
bpm
VT
with
out p
ulse
inte
rspe
rsed
with
VF
Disc
harg
ed h
ome
Extu
batio
n w
ithou
t seq
uela
e
Pulse
less
elec
tric
al ac
tivity
ECG
Pulse
less
elec
tric
al ac
tivity
ECG
2998400 1
9984001998400
4998400
9998400
30998400
Amiodarone 50mg +
Amiodarone 50mg +
epinefrine 20mcg
epinefrine 40mcg +
20 ILE 1mLmiddotkgminus1
20 ILE 1mLmiddotkgminus1
20 ILE 1mLmiddotkgminus1
Epinefrine 40mcg
20 ILE 0 25 mLmiddot
Epinefrine 40mcg + epinefrine 01ndash04mcgmiddot
kgminus1middotminminus1
kgminus1middotminminus1
Caud
al b
lock
12
mL05
b
upiv
acai
ne w
ith ep
inep
hrin
e
Figure 1
punctured and urinary catheterization for diuresis monitor-ing was done Blood gas analysis showed pH = 709 pO
2
= 86mmHg pCO2= 46mmHg HCO
3= 14mEqL BE =
minus158 and Sat = 93 Despite respiratory acidosis lactateconcentration was nearly normal (17mmolsdotLminus1) He wastransferred to the Intensive Care Unit and the adrenaline wasturned off after 5 hours of its onset (Figure 1) As perfusionimproved respiratory acidosis disappeared blood lactate leveldecreased to 08mmolsdotLminus1The patient was kept sedated untilnormalization of pulmonary and tissue perfusion parametersComputed tomography of the brain showed no brain damageHe was extubated without sequelae thirty hours after theepisode and was discharged home three days later Formalconsent for publication was obtained from patientrsquos mother
3 Discussion
Local anaesthetic toxicity has been reported with almost allkind of regional blocks including peripheral blockades [3]and caudal blocks [4] The caudal block is the most easilylearned of all regional anaesthetic techniques It has relativelylow risk of complications and a high rate of success Atesting dose can be used to exclude intravascular injectionand althoughdesirable it is not commonly performed bymostanaesthesiologists In this case the ease of injection was usedas a parameter for correct placement The choice of a longer-acting amide LA such as bupivacaine improves analgesiaafter surgery but its cardiotoxicity limits its use [5] Additionof vasoconstrictors such as epinephrine can dramaticallyslow its absorption improving its safety and prolonging the
anaesthesia [1] In this case the limit dose (3mgsdotkgminus1) was notachieved and the typical description of progressive biphasicsymptoms affecting first the CNS and then CVS [6] was notseen as he was sedated and curarized
Beta blockade with Timolol drops before surgery mayhave difficult cardiac arrest reversion and it could also justifythe increasing necessities of adrenaline to maintain hemo-dynamic stable status
Intravenous lipid emulsion is a method for rescue forcardiovascular collapse after an inadvertent intravenousinjection of local anaesthetics [7] In cardiac arrest caused bybupivacaine intoxication first-line rescue with epinephrineand epinephrine + intravenous lipid emulsion (ILE)wasmoreeffective with regard to survival [8] There are several casereports of successful resuscitation after cardiovascular col-lapse in the adult population but examples in children arescarce and this case seems to be the second one showingfeatures of ventilationperfusion (VP) mismatch after ILEin child [4] The doses used in this case followed the ASRAPracticeAdvisory [9 10] and resulted in a complete stop of thearrests about 20 minutes after the beginning of its infusion
If ventilation or perfusion is unstable a ventilationperfu-sion (VQ) mismatch can occur It can be caused by bloodshunting for example during atelectasis or by dead space inthe lungs for example with a pulmonary embolism hypo-volemia or on postarrest period in an intubated and well-ventilated patient Gas analysis just after cardiac recoveryshowed respiratory acidosis due to VQ mismatch Inad-equate pulmonary perfusion (yet) to adequately ventilatedareas of the lung impairs gas exchange and leads to hypoxia
Case Reports in Anesthesiology 3
[11] FiO2was set to 100 to target SaO
2to 90ndash94 in the
postcardiac arrest periodDespite the fact that it would have resulted in the same
consequences (subsequently pulseless electrical activity car-diac arrest) defibrillation using 2 Joulessdotkgminus1 would be moresuitable than amiodarone as the first choice for treatmentof the second cardiac arrest Induced hypothermia was notperformed according to PALS guideline [12]
This case is remarkable because due to the rapid onsetof cardiac symptoms intraosseous injection cannot be ruledout Appropriate conduction of the case favoured a postarrestperiod without complications
Ethical Approval
The responsible institutional review board of our institutiongave permission to publish this report
Disclosure
This report was previously presented in part at theMedicallyChallenging Case poster presentation at the ASA AnnualMeeting 2013
Competing Interests
All the authors declare that there is no conflict of interestsregarding this publication
References
[1] E Giaufre ldquoCaudal anesthesia in childrenrdquoCahAnesthesiol vol43 no 3 pp 281ndash286 1995
[2] S Ciechanowicz and V Patil ldquoLipid emulsion for local anes-thetic systemic toxicityrdquo Anesthesiology Research and Practicevol 2012 Article ID 131784 11 pages 2012
[3] I Kamel G Trehan and R Barnette ldquoIntralipid therapy forinadvertent peripheral nervous system blockade resulting fromlocal anesthetic overdoserdquo Case Reports in Anesthesiology vol2015 Article ID 486543 3 pages 2015
[4] U Shenoy J Paul and D Antony ldquoLipid resuscitation in pedia-tric patientsmdashneed for cautionrdquo Paediatric Anaesthesia vol 24no 3 pp 332ndash334 2014
[5] P-A Lonnqvist and N S Morton ldquoPostoperative analgesia ininfants and childrenrdquo British Journal of Anaesthesia vol 95 no1 pp 59ndash68 2005
[6] M F Mulroy ldquoSystemic toxicity and cardiotoxicity from localanesthetics incidence and preventivemeasuresrdquoRegional Anes-thesia and Pain Medicine vol 27 no 6 pp 556ndash561 2002
[7] M S Ozcan andGWeinberg ldquoUpdate on the use of lipid emul-sions in local anesthetic systemic toxicity a focus on differen-tial efficacy and lipid emulsion as part of advanced cardiac lifesupportrdquo International Anesthesiology Clinics vol 49 no 4 pp91ndash103 2011
[8] J Mauch O M Jurado N Spielmann R Bettschart-Wolfens-berger and M Weiss ldquoResuscitation strategies from bupiva-caine-induced cardiac arrestrdquo Paediatric Anaesthesia vol 22no 2 pp 124ndash129 2012
[9] J M Neal C M Bernards J F Butterworth et al ldquoASRApractice advisory on local anesthetic systemic toxicityrdquoRegionalAnesthesia and Pain Medicine vol 35 no 2 pp 152ndash161 2010
[10] J M Neal M F Mulroy and G L Weinberg ldquoAmericanSociety of Regional Anesthesia and Pain Medicine checklistfor managing local anesthetic systemic toxicity 2012 versionrdquoRegional Anesthesia and Pain Medicine vol 37 no 1 pp 16ndash182012
[11] F A Donoso S D Arriagada R F Dıaz and R P Cruces ldquoVen-tilation strategies in the child with severe hypoxemic respir-atory failurerdquoGacetaMedica deMexico vol 151 no 1 pp 75ndash842015
[12] M E Kleinman A R De Caen L Chameides et al ldquoSpecialreportmdashpediatric basic and advanced life support 2010 interna-tional consensus on cardiopulmonary resuscitation and emer-gency cardiovascular care science with treatment recommenda-tionsrdquo Pediatrics vol 126 no 5 pp e1261ndashe1318 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Case Reports in Anesthesiology 3
[11] FiO2was set to 100 to target SaO
2to 90ndash94 in the
postcardiac arrest periodDespite the fact that it would have resulted in the same
consequences (subsequently pulseless electrical activity car-diac arrest) defibrillation using 2 Joulessdotkgminus1 would be moresuitable than amiodarone as the first choice for treatmentof the second cardiac arrest Induced hypothermia was notperformed according to PALS guideline [12]
This case is remarkable because due to the rapid onsetof cardiac symptoms intraosseous injection cannot be ruledout Appropriate conduction of the case favoured a postarrestperiod without complications
Ethical Approval
The responsible institutional review board of our institutiongave permission to publish this report
Disclosure
This report was previously presented in part at theMedicallyChallenging Case poster presentation at the ASA AnnualMeeting 2013
Competing Interests
All the authors declare that there is no conflict of interestsregarding this publication
References
[1] E Giaufre ldquoCaudal anesthesia in childrenrdquoCahAnesthesiol vol43 no 3 pp 281ndash286 1995
[2] S Ciechanowicz and V Patil ldquoLipid emulsion for local anes-thetic systemic toxicityrdquo Anesthesiology Research and Practicevol 2012 Article ID 131784 11 pages 2012
[3] I Kamel G Trehan and R Barnette ldquoIntralipid therapy forinadvertent peripheral nervous system blockade resulting fromlocal anesthetic overdoserdquo Case Reports in Anesthesiology vol2015 Article ID 486543 3 pages 2015
[4] U Shenoy J Paul and D Antony ldquoLipid resuscitation in pedia-tric patientsmdashneed for cautionrdquo Paediatric Anaesthesia vol 24no 3 pp 332ndash334 2014
[5] P-A Lonnqvist and N S Morton ldquoPostoperative analgesia ininfants and childrenrdquo British Journal of Anaesthesia vol 95 no1 pp 59ndash68 2005
[6] M F Mulroy ldquoSystemic toxicity and cardiotoxicity from localanesthetics incidence and preventivemeasuresrdquoRegional Anes-thesia and Pain Medicine vol 27 no 6 pp 556ndash561 2002
[7] M S Ozcan andGWeinberg ldquoUpdate on the use of lipid emul-sions in local anesthetic systemic toxicity a focus on differen-tial efficacy and lipid emulsion as part of advanced cardiac lifesupportrdquo International Anesthesiology Clinics vol 49 no 4 pp91ndash103 2011
[8] J Mauch O M Jurado N Spielmann R Bettschart-Wolfens-berger and M Weiss ldquoResuscitation strategies from bupiva-caine-induced cardiac arrestrdquo Paediatric Anaesthesia vol 22no 2 pp 124ndash129 2012
[9] J M Neal C M Bernards J F Butterworth et al ldquoASRApractice advisory on local anesthetic systemic toxicityrdquoRegionalAnesthesia and Pain Medicine vol 35 no 2 pp 152ndash161 2010
[10] J M Neal M F Mulroy and G L Weinberg ldquoAmericanSociety of Regional Anesthesia and Pain Medicine checklistfor managing local anesthetic systemic toxicity 2012 versionrdquoRegional Anesthesia and Pain Medicine vol 37 no 1 pp 16ndash182012
[11] F A Donoso S D Arriagada R F Dıaz and R P Cruces ldquoVen-tilation strategies in the child with severe hypoxemic respir-atory failurerdquoGacetaMedica deMexico vol 151 no 1 pp 75ndash842015
[12] M E Kleinman A R De Caen L Chameides et al ldquoSpecialreportmdashpediatric basic and advanced life support 2010 interna-tional consensus on cardiopulmonary resuscitation and emer-gency cardiovascular care science with treatment recommenda-tionsrdquo Pediatrics vol 126 no 5 pp e1261ndashe1318 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom