Embed Size (px)
Citation preview
Central JSM Neurosurgery and Spine
Cite this article: Lücke S, Kinzel A, Schreiber L, Petridis AK (2014) Anterior Cervical Uncoforaminotomy performed with Piezosurgery Technical Note. JSM Neurosurg Spine 2(6): 1048.
*Corresponding authorAthanasios K. Petridis, Wedau Kliniken, Sana Konzern, Department of Neurological Surgery, Zu den Rehwiesen 9,47055 Duisburg, Germany, Tel: +49-203-7332425; Email:
Submitted: 29 November 2014
Accepted: 23 December 2014
Published: 30 December 2014
Copyright© 2014 Lücke et al.
OPEN ACCESS
Case Report
Anterior Cervical Uncoforaminotomy performed with Piezosurgery Technical NoteSebastian Lücke1,2, Adrian Kinzel1, Lutz Schreiber1 and Athanasios K. Petridis1*1Department of Neurosurgery, Teaching Hospital of the University Essen-Duisburg, Germany2Department of Neurosurgery University Hospital Bochum, Germany
Abstract
The microsurgical anterior foraminotomy is a well-established treatment of cervical radiculopathy in cases of cervical disc herniation and spondylotic foraminal stenosis. The risk of injuring vertebral artery because of the proximity to the uncovertebral joint, which is resected with the drill is not insignificant.
PIEZOsurgery is known to reduce the risk of soft tissue damage in fields of maxillo-facial / ENT surgery, because it selectively cuts mineralized structures. The use of PIEZOsurgery is widespread in paediatric neurosurgery, but until now there are only a few studies about dorsal spine procedures and none about anterior approaches to the cervical spine published.
We report our experience of ventral approaches to the cervical spine with this innovative ultrasonic osteotomy tool. With selective cutting of mineralized structures and a good visualisation, dissection along the nerval and vascular structures could be performed without damage.
In our opinion the use of the PIEZOsurgery osteotomy gives the surgeon a safe possibility to perform the uncoforaminotomy and to decompress the cervical root. The PIEZOsurgery tool will allow surgeons, to perform this surgery with lower risk of damage soft tissues or the vertebral artery.
INTRODUCTIONSurgical decompression of nerval and vascular structures
bears a significant risk of damaging them. The anterolateral approach to the cervical spine is an elegant operation with obvious risk to lesion the vertebral artery. Since the description of Jho [1-3] several authors have published advantages of this less invasive technic [4-6]. Excellent clinical results and preservation of the motional segment, resulting in avoidance of adjacent level morbidity were compared with the challenge of the procedure and the routine exposure of the vertebral artery. The use of rotating instruments (high speed drills) may lead to undesirable complications in less experienced hands.
In our neurosurgical department the anterior uncoforaminotomy is used as standard operation for cervical radiculopathy as is the anterior cervical discectomy and fusion (ACDF) and disc prosthesis since 2003. The osteotomy with
PIEZOsurgery (was just introduced in our department) allows a selective cut of mineralized structures, which leads to increased safety, especially in preserving nerval structures as documented in facial nerve decompression [4]. A recent study of Grauvogel [2] describes the potential of PIEZOsurgery to replace the rotating drill in bone cutting for internal auditory canal(IAC) opening in acoustic neuroma surgery.
The aim of the present work was to test the applicability of the PIEZOsurgery medical device in microsurgical anterior foraminotomy. We report our first experience with the first three cases.
MATERIAL AND METHODSWe used the PIEZOSURGERY medical device (Mectron®
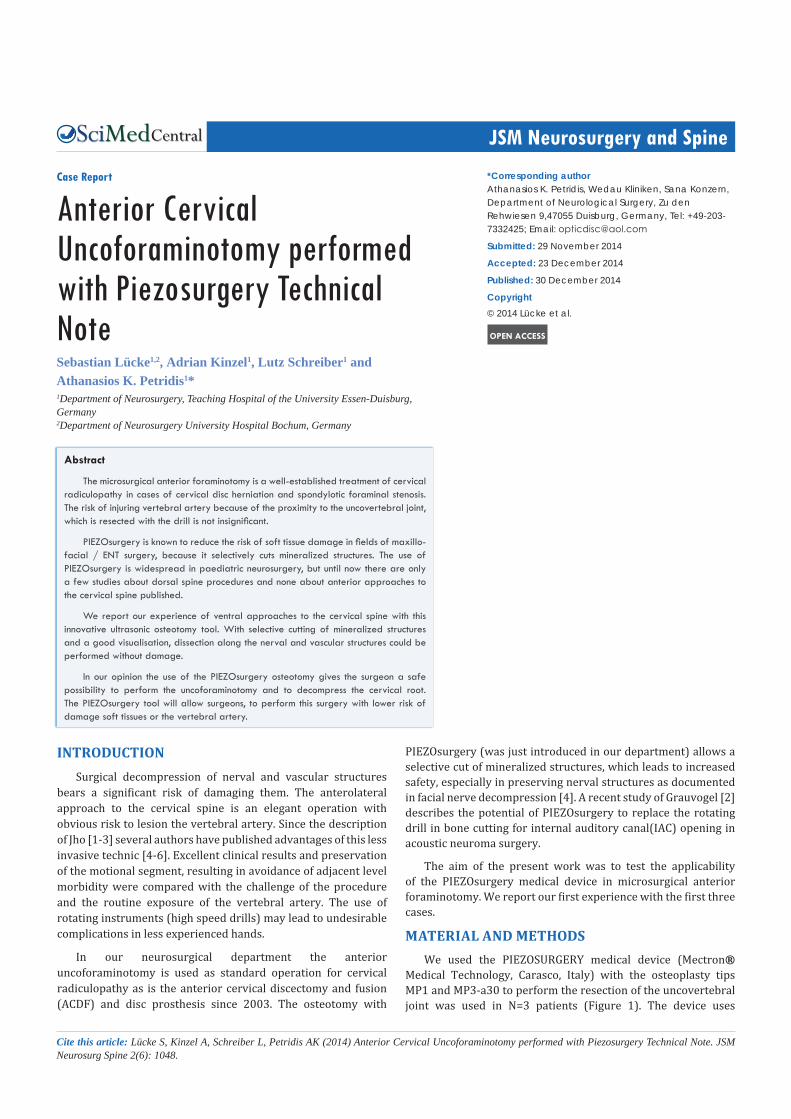
Medical Technology, Carasco, Italy) with the osteoplasty tips MP1 and MP3-a30 to perform the resection of the uncovertebral joint was used in N=3 patients (Figure 1). The device uses
Central
Lücke et al. (2014)Email:
JSM Neurosurg Spine 2(6): 1048 (2014) 2/3
low frequency ultrasonic waves (24-36KHz) to generate micromovements with amplitude of about 40micrometres [3,7-13]. Intraoperative irrigation cools down the tip and the bone surface and furthermore it improves visualisation.
In all three cases we used the standard ventral approach to the cervical spine under the ZEISS® Pentero operating microscope with the patient in supine position.
RESULTSThe resection of the uncinate process up to the posterior
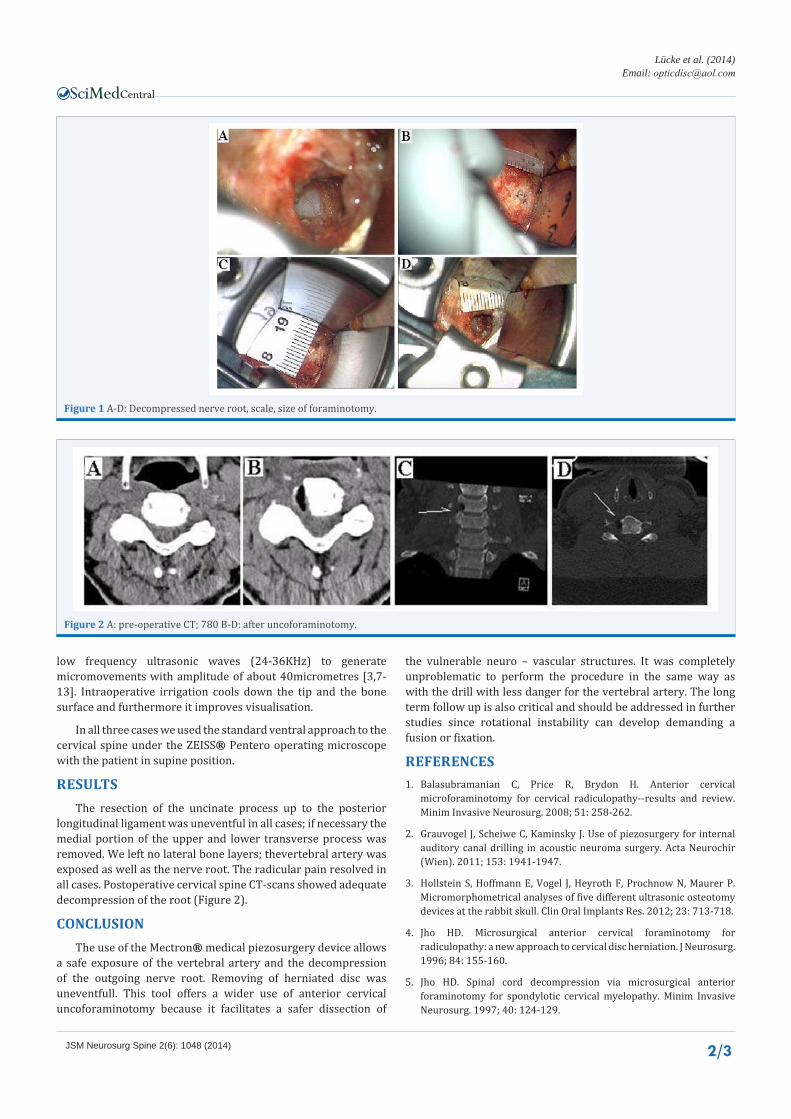
longitudinal ligament was uneventful in all cases; if necessary the medial portion of the upper and lower transverse process was removed. We left no lateral bone layers; thevertebral artery was exposed as well as the nerve root. The radicular pain resolved in all cases. Postoperative cervical spine CT-scans showed adequate decompression of the root (Figure 2).
CONCLUSIONThe use of the Mectron® medical piezosurgery device allows
a safe exposure of the vertebral artery and the decompression of the outgoing nerve root. Removing of herniated disc was uneventfull. This tool offers a wider use of anterior cervical uncoforaminotomy because it facilitates a safer dissection of
the vulnerable neuro – vascular structures. It was completely unproblematic to perform the procedure in the same way as with the drill with less danger for the vertebral artery. The long term follow up is also critical and should be addressed in further studies since rotational instability can develop demanding a fusion or fixation.
REFERENCES1. Balasubramanian C, Price R, Brydon H. Anterior cervical
microforaminotomy for cervical radiculopathy--results and review. Minim Invasive Neurosurg. 2008; 51: 258-262.
2. Grauvogel J, Scheiwe C, Kaminsky J. Use of piezosurgery for internal auditory canal drilling in acoustic neuroma surgery. Acta Neurochir (Wien). 2011; 153: 1941-1947.
3. Hollstein S, Hoffmann E, Vogel J, Heyroth F, Prochnow N, Maurer P. Micromorphometrical analyses of five different ultrasonic osteotomy devices at the rabbit skull. Clin Oral Implants Res. 2012; 23: 713-718.
4. Jho HD. Microsurgical anterior cervical foraminotomy for radiculopathy: a new approach to cervical disc herniation. J Neurosurg. 1996; 84: 155-160.
5. Jho HD. Spinal cord decompression via microsurgical anterior foraminotomy for spondylotic cervical myelopathy. Minim Invasive Neurosurg. 1997; 40: 124-129.
Figure 1 A-D: Decompressed nerve root, scale, size of foraminotomy.
Figure 2 A: pre-operative CT; 780 B-D: after uncoforaminotomy.

Central
Lücke et al. (2014)Email:
JSM Neurosurg Spine 2(6): 1048 (2014) 3/3
Lücke S, Kinzel A, Schreiber L, Petridis AK (2014) Anterior Cervical Uncoforaminotomy performed with Piezosurgery Technical Note. JSM Neurosurg Spine 2(6): 1048.
Cite this article
6. Jho HD, Ha HG. Anterolateral approach for cervical spinal cord tumors via an anterior microforaminotomy: technical note. Minim Invasive Neurosurg. 1999; 42: 1-5.
7. Lambrecht JT. [Intraoral piezo-surgery]. Schweiz Monatsschr Zahnmed. 2004; 114: 28-36.
8. Maurer P, Kriwalsky MS, Block Veras R, Brandt J, Heiss C. [Light microscopic examination of rabbit skulls following conventional and Piezosurgery osteotomy]. Biomed Tech (Berl). 2007; 52: 351-355.
9. Pechlivanis I, Brenke C, Scholz M, Engelhardt M, Harders A, Schmieder K. Treatment of degenerative cervical disc disease with uncoforaminotomy--intermediate clinical outcome. Minim Invasive Neurosurg. 2008; 51: 211-217.
10. Rashad A, Kaiser A, Prochnow N, Schmitz I, Hoffmann E, Maurer P. Heat production during different ultrasonic and conventional osteotomy preparations for dental implants. Clin Oral Implants Res. 2011; 22: 1361-1365.
11. Salami A, Dellepiane M, Mora R. A novel approach to facial nerve decompression: use of Piezosurgery. Acta Otolaryngol. 2008; 128: 530-533.
12. Vercellotti T. Piezoelectric surgery in implantology: a case report--a new piezoelectric ridge expansion technique. Int J Periodontics Restorative Dent. 2000; 20: 358-365.
13. Vercellotti T. Technological characteristics and clinical indications of piezoelectric bone surgery. Minerva Stomatol. 2004; 53: 207-214.