Embed Size (px)
DESCRIPTION
just a dermatology case report
Citation preview

Drug-induced Acneiform Eruption due to Diet PillsSita Anindita, Arif Widiatmoko
Dermatology And Venereology Department, Medical Faculty Universitas BrawijayaDr. Saiful Anwar General Hospital
Malang, IndonesiaEmail:[email protected]
Abstract:Introduction:. Acneiform eruption is a group of dermatoses characterised by papules, pustules, nodules, cysts, or papulopustules resembling acne that clinically lacks comedones. The report describes a case of acneiform eruption in a young woman that showed significant improvements following several acne treatment regiments.Case Reporta 21 year-old young woman presented complaints of severe, pus-filled multiple small bumps resembling acne that had quickly covered her face and neck. Careful history taking revealed that the patient was a long-term consumer of diet pills. Further examinations combined with anamnesis established the diagnosis of drug-induced acneiform eruptions, specifically due to fad diet pills. A treatment regiment consisting of oral doxycycline 100 mg 2x1, a topical gel containing benzoyl peroxide 5% and clindamycin phosphate 1.2%, a topical lotion containing 70% alcohol, propylene glycol, zinc oxide, precipitated sulphur 6%, resorcinol 15%, and camphor to be used twice or three times daily, acne facial wash, and an SPF 30 sunscreen lotion as well as cessation of diet pill consumption had successfully improved her conditions. Subsequent therapy removed the antibiotic and benzoyl peroxide still resulted in marked improvements, reaching a stable state with some residual symptomatology. Discussion The diagnosis of was based on anamnesis, clinical manifestation and histopathologic findings relevant to acneiform eruptions. The significant alleviation of symptoms following the treatment as well as cessation of triggering factor underlined the importance of proper diagnosis and management for patients with persistent dermatologic conditions. Keywords: acneiform eruption, drug-induced, diet pills

INTRODUCTION
Acneiform eruptions are a group of dermatoses that resemble acne
vulgaris. Lesions may consist of papules, nodules, pustules, papulopustules, or
cysts that lack comedones, contrasting this disorder from acne vulgaris. Being a
group of dermatoses, acneiform eruptions can appear due to infections, hormonal
or metabolic abnormalities, genetic disorders, and drug reactions. As the name
indicates, acneiform eruptions present with acnelike lesions. However, the lack of
comedones is a distinguishing factor. The lesions may localise outside of the area
in which acne vulgaris occurs. Acneiform eruptions can also be distinguished
from acne vulgaris by a history of sudden onset, monotonous lesion morphology,
and eruption development at an age outside the range typical of acne vulgaris. In
the case of drug-induced acneiform eruptions, the eruption resolves with
discontinuation of the medication 1.
A prominent dermatology textbook had listed steroid folliculitis, drug-
induced acne, occupational acne and chloracne, epidermal growth factor receptor
inhibitor-associated eruption, gram negative folliculitis, radiation acne, tropical
acne, acne aestivalis, pseudoacne of the nasal crease, and apert syndrome amongst
the possible entities 2, whereas other sources had included nevus comedonicus,
eruptive hair cysts, tuberous sclerosis 3, 4, amineptine acne, eosinophilic pustular
folliculitis, Malassezia folliculitis, coccidioidomycosis, secondary syphilis 5, 6,
sporotrichosis, rosacea, and perioral dermatitis 1.
The differential diagnoses of acneiform eruptions may include but not
limited to: acne vulgaris, allergic contact dermatitis, and drug eruptions 1.
Therefore, to establish the diagnosis, careful history taking and dermatological
examinations ought to be performed.
The laboratory studies for acneiform eruptions vary greatly, reflecting the
wide variety of diseases. This can include skin biopsies, cultures and sensitivities,
serologic tests, and empiric trials of drug withdrawal. Having emphasised that, the
treatment varies with the particular disease suspected and consists of a wide range

of methods, including excision, laser ablation, topical/oral antibiotics, topical/oral
retinoids, and drug withdrawal.

CASE REPORT
A 21 year-old young woman visited the dermatovenereology outpatient
clinic of Saiful Anwar General Hospital (RSSA) on the 25th of February 2016
complaining of severe, pus-filled multiple small bumps resembling acne that had
quickly covered her face since the day before the visit. It started to develop two
days ago after she took an over-the-counter cold medication that contained
phenylpropanolamine hydrochloride, chlorpheniramine maleate, and paracetamol.
When asked, she revealed that her acne-like condition had actually persisted for
three years. However, since the last month the disorder had significantly worsened
until acne-like lesions covered the whole facial surface area. The patient denied
consuming any drugs — either orally or topically — except a regiment of fad diet
pills, which she had been consuming for the past 7 months until then. Last year,
the patient visited a dermatovenereologist as a result of the same complaint. She
received oral clindamycin and topical desoxymethasone, which she consumed
without showing any significant improvements. Therefore, she decided to stop the
usage. She noticed that her lesions worsened during her menstrual period. Both of
her parents had also suffered from severe, untreated acne-like conditions.
General physical examination revealed that she was compos mentis, looked
generally well, blood pressure 120/90, pulse rate 68 times per minute, respiratory
rate 18 times per minute, and the body temperature was 37.0°C. There were no
sign of anaemia, cyanotis, icterus, hyperemia and secret on conjunctiva and there
were no enlargement of lymphnodes. The heart and lungs were within normal
limits and there were no abnormalities on abdominal examination. Her extremities
were also within normal limit and there was no edema.
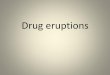
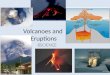
Dermatological examination showed multiple small pustules 0.1 cm in
diameter with erythematous base. Some joined to form multiple plaques. The
lesions were localised on the face and neck, evenly distributed. No comedones or
hyperkeratotic plugs were observed (Figures 1-4).

Figure 1. Multiple pustules Ø 0.1 cm with erythematous base with some joined to form
multiple plaques, localised on the face and neck, evenly distributed. No comedones were
observed (frontal view)
Figure 2. Multiple pustules Ø 0.1 cm with erythematous base with some joined to form multiple plaques, localised on the face and
neck, evenly distributed. No comedones were observed (lateral view)
Figure 3. Multiple pustules Ø 0.1 cm with erythematous base with some joined to form
multiple plaques, localised on the face and neck, evenly distributed. No comedones were
observed (lateral view)
Figure 4. Lesion on the neck area

Microscopic examination of a sample taken from the lesion revealed mixed
inflammatory inflitrates and debris among oedematous cells, suggesting
conspicuous superficial dermal inflammation. Neither bacteria, mites, hyphae, nor
keratotic plugs were observed (Figure 5).
Figure 5. Microscopic examination of a lesion sample revealed mixed inflammatory inflitrates and debris among oedematous cells, suggesting conspicuous superficial dermal inflammation. Neither
bacteria, mites, hyphae, nor keratotic plugs were observed
The patient was diagnosed as having an acneiform eruptions and therefore
prescribed oral Doxycycline 100 mg to be taken twice daily, a topical gel
containing benzoyl peroxide 5% and clindamycin phosphate 1.2%, a topical lotion
containing 70% alcohol, propylene glycol, zinc oxide, precipitated sulphur 6%,
resorcinol 15%, and camphor to be used twice or three times daily, acne facial
wash, and an SPF 30 sunscreen lotion. The patient was educated and informed to
use all the medications properly and accordingly, at the same time discontinuing
the diet pills that she had been routinely taking. She was then asked to return for a
follow-up visit on the 1st of March 2016.
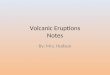
Coming for her first follow-up visit on the 1st of March 2016, the patient
reported significant improvements on her previous complaints. The pus had been
disappearing to almost none, whilst the skin redness had started to fade. The
medications given on the first visit were all almost finished, as she had been using
them as previously instructed. Dermatological examinations revealed significant
improvements on the acneiform eruptions localised on the face and the neck.

What remained from the past lesions were multiple erythematous plaque with
unclear definition. The size varied from 1-10 cm, with and without papules and
pustules on top Figures 6 - 9 .
Figure 6.. First follow-up visit revealed significant improvements on the acneiform
eruptions (Frontal View)
Figure 7. First follow-up visit revealed significant improvements on the acneiform
eruptions (Lateral View)
Figure 8. Another lateral view of the lesion
improvement
Figure 9. The remaining of the lesions on the
neck

A slight change in therapeutic regiments was therefore given.
Discontinuing the oral antibiotic and topical benzoyl peroxide courses, she would
then had to only apply topical Clindamycin phosphate 1.2% gel twice daily,
continuing the a topical therapy of a lotion containing 70% alcohol, propylene
glycol, zinc oxide, precipitated sulphur 6%, resorcinol 15%, albeit only once at
night times, and acne facial wash.
Figure 10. Further improvements on the second follow-up visit (Frontal View)
Figure 11. Further improvements on the second follow-up visit (Lateral View)
Figure 12. Further improvements on the second follow-up visit (Lateral View)

The patient came again for the final follow-up visit on the 4th of March 2016,
complimenting the progress of her improvements. Dermatological examination
was performed and revealing localised lesions on the face, which consisted of
erythematous plaque with several various sized papules and pustules (Figures 10-
12). The same therapy as the previous visit which consisted of topical
clindamycin phosphate 1.2% gel twice daily, lotion containing 70% alcohol,
propylene glycol, zinc oxide, precipitated sulphur 6%, resorcinol 15%, once at
night times, and acne facial wash was therefore given.

DISCUSSION
Acneiform eruptions are a group of dermatoses that resemble acne vulgaris.
Lesions may consist of papules, nodules, pustules, papulopustules, or cysts that
lack comedones, contrasting this disorder from acne vulgaris 2. The patient visited
the dermatovenereology outpatient clinic of Saiful Anwar General Hospital
(RSSA) on the 25th of February 2016 complaining of severe, pus-filled multiple
small bumps resembling acne covered her face. Dermatological examination
showed multiple small pustules 0.1 cm in diameter with erythematous base. Some
joined to form multiple plaques. The lesions were localised on the face and neck,
evenly distributed. No comedones or hyperkeratotic plugs were observed.
Therefore, the patient was diagnosed as having acneiform eruptions.
Being a group of dermatoses, acneiform eruptions can appear due to
infections, hormonal or metabolic abnormalities, genetic disorders, and drug
reactions. Steroid folliculitis appeared after systemic glucocorticoids or
corticotropin administration and observed as monomorphous small pustules and
red papules located predominantly on the trunk and extremities, with less
involvement of the face. Topical or inhaled corticosteroids may cause an
acneiform eruption of the area of skin under which the topical preparation is
applied or in around the nose or mouth in the case of inhaled steroids. The
eruption usually resolves after discontinuation of the steroid and, in addition, may
respond to the usual treatments of acne vulgaris such as topical retinoids and
antibiotics 2, 7. This does not match the history taking from the patient which
claimed that she hand not been taking medications. The dermatological
examinations also did not match the aforementioned description of the lesions.
Therefore, the acneiform eruption in this patient is not due to steroid folliculitis.
Occupational acne and chloracne are induced by industrial compounds
encountered in the workplace, which may include coal tar derivatives, insoluble
cutting oils, and chlorinated hydrocarbons (chlornaphtalenes, chlordiphenyls, and
chlordiphenyloxides) 2. Exposure to halogenated aromatic hydrocarbon
compounds, such as chlorinated dioxins and dibenzofurans, by inhalation,

ingestion, or direct contact of contaminated compounds or foods induces a
cutaneous eruption of polymorphous comedones and cysts referred to as
chloracne. Other associated skin findings may include xerosis and pigmentary
changes. Internal changes involving the ophthalmic, nervous, and hepatic systems
may also occur, and some chloracnegens can be oncogenic. Treatment is difficult
because chloracne may persist for years, even without further exposure 1, 8. This
does not match the history taking from the patient, as she had not been exposed to
the industrial chemicals. The dermatological examinations also did not match the
aforementioned description of the lesions as her condition lacked comedones and
cysts.
Gram-negative folliculitis sometimes occurs in individuals with pre-
existing acne vulgaris, which receives long-term oral antibiotics treatments,
especially the tetracyclines. It may appear as either papulopustules concentrated
around the nose or as deep-seated nodules. Enterobacter, Klebsiella, or
Escherichia may be revealed in papulo-pustular lesions, while Proteus is more
dominant in the nodules. Antibiotics against Gram-negative bacteria may be
employed as a treatment approach. Oral isotretinoin for 4 to 5 months have been
proven beneficial for recalcitrant cases. Sometimes, an oral cephalosporin in
combination with isotretinoin may be given for 2 weeks 2, 9. The patient had not
been receiving a long-term antimicrobial therapy. The microscopic examination of
a sample taken from her lesions also revealed no Gram-negative bacteria.
Ionising radiation and UV radiation may trigger acneiform eruptions, with
comedo-like papular lesions. These hyperkeratotic plugs are resistant to
extraction. When the radiation such as UV is extensive, a yellow, atrophic plaque
studded with large, open comedones may form, also known as Favre-Raucochot
syndrome, solar comedones, senile comedones, nodular cutaneous elastosis with
cysts and comedones, and nodular elastoidosis with cysts and comedones. These
lesions are commonly distributed symmetrically on the temporal and periorbitas
areas. Oral or topical retinoids acoompanied with extraction are the treatment
choices. Sometimes, tropical climates or extremely hot occupational environments
produced acneiform eruption so-called tropical acne. The multiple lesions are

deep, large, inflammatory nodules with several draining areas not unlike acne
conglobata distributed chiefly on the trunk and buttocks. The treatment is by
removing the patient to a cooler environment and systemic antibiotics for
secondary coagulase-positive staphylococci infection that almost always ensues 2,
10, 11. Again, despite the fact that the patient lived in a tropical country, her
dermatological examinations did not match the lesion description. Not only that
the lesions are distributed evenly on her face and neck, the manifestation also
lacked comedones.
Acne aestivalis occurs due to the effect of UV radiation, primarily
ulatraviolet A. It is mainly developed in women aged 20-30 years old. Pseudoacne
of the nasal crease develops as acneiform red papules within the nasal crease
along with milia. On the other hand, a condition called Apert syndrome is an
autosomal dominant disorder with acrocephalosyndactyly. Perioral dermatitis is
an inflammatory and chronic papulopustular and vesicular eruptions on the
perioral area, whilst Malassezia folliculitis is caused by overgrowth of Malassezia
yeasts 11. Unlike acne vulgaris, it is pruritic, does not contain comedones, and
responds to empiric antifungal therapy rather than antibiotics. Diagnosis is
typically made clinically, although the yeast and hyphae can be observed in
biopsy specimens in the widened follicular ostia along with keratinous material,
and occasionally, rupture of the follicular wall may occur. Patients may be treated
with topical leave-on, wash-off, or systemic antifungal therapy 12. Nevus
comedonicus (NC) is an infrequent developmental anomaly manifesting as
aggregated open comedones. It consists of dilated follicular or eccrine orifices
plugged with keratin. It may be solitary, congenital, or, less frequently, can occur
later in life as a result of occupational exposure. Treatment of NC is generally
surgical, through excision or carbon dioxide laser ablation of the involved skin.
Medical therapy with topical retinoids may be of some benefit 13. However, both
the history taking and the dermatological examination suggested that the patient
did not suffer from these conditions. Moreover, hyphae were not found upon
microscopic examination.

The eruptive vellus hair cysts manifest as flesh-colored papules found
usually on the face, chest, neck, thighs, groin, buttocks, and axillae and
representing vellus hair follicle anomaly, which may be hereditary.
Histopathological examinations reveal a mid dermal epithelial cyst that contains
vellus hairs and keratinous material. These may regress spontaneously, forming a
connection to the epidermis, or degrade with a resultant foreign body
granulomatous formation. Treatment is often difficult. Incision and drainage of
individual lesions carries the risk of subsequent scarring, and modalities such as
carbon dioxide laser ablation are difficult to use over large surface areas. Topical
retinoids and 12% lactic acid preparations have proven useful in some instances 14,
15. The patient did not show vellus hair anomaly. Therefore, her condition must be
caused by another aetiology.
Eosinophilic pustular folliculitis (EPF) is a condition thought to be an
allergic hypersensitivity that appears as a recurrent pruritic papulopustular
eruption on the face, trunk, and extremities. Three main types exist, (1) infantile
form, (2) HIV associated, and (3) classic Ofuji disease in immunocompetent
patients, typically Japanese patients. Patients may also demonstrate blood
eosinophilia and leukocytosis. Treatment modalities and results vary greatly, but
include topical and systemic corticosteroids, oral antibiotics, dapsone, isotretinoin,
and pulsed ultraviolet phototherapy (PUVA). Indomethacin is the choice for
classic Ofuji disease 16. This almost matched the patient's history taking and
dermatological examinations. However, the lesions were localised only on the
face and the neck areas.
Secondary syphilis may produce papulopustules and nodules, some
crusted, may occur on the face, trunk, and extremities. The causative agent, the
spirochete Treponema pallidum, may be easily observed in biopsy specimens with
the Warthin-Starry stain. In addition, serologic tests and the presence of
spirochetes on darkfield microscopy may reveal the diagnosis 6. Sporothrix
schenckii, the responsible agent of sporotrichosis, commonly induces a
lymphocutaneous reaction, but it can also produce a persistent fixed localized
cutaneous papulonodular eruption that may involve the face. The organism can be

demonstrated histologically, by peripheral blood smear, and by fungal culture 17.
Cutaneous coccidioidomycosis usually caused by inhalation and dissemination
of Coccidioides immitis, may rarely occur by primary inoculation and appear as
papulopustules, nodules, or plaques that can eventually ulcerate and crust 18.
Despite the fact that no further tests were employed to eliminate these differential
causes, it is highly unlikely that the patient suffered from either condition. Both
conditions should also come with other sign and symptoms, which were negative
in the patient.
Rosacea appears similarly to acne vulgaris with papulopustules on the
face, but in addition, patients may also have facial flushing and telangiectasias.
Four subtypes of rosacea exist: (1) erythematotelangiectatic, (2) papulopustular,
(3) phymatous, and (4) ocular. Rosaea is more common in the white population
and in women in the third and fourth decades of life. Men, however, more
commonly develop sebaceous hyperplasia of the nose, known as rhinophyma.
Although the definitive etiology is unknown, weather extremes, hot or spicy
foods, alcohol, and Demodex folliculorum mites can trigger and exacerbate this
condition. Acne rosacea has also been associated with the ingestion of a high-dose
vitamin B6 supplement. Treatment primarily includes skin barrier sunscreens and
topical antibiotics such as metronidazole, retinoids, and oral tetracyclines 2. Signs
of rosacea were absent in this patient. There was no telangiectasia, Demodex
finding, amongst other things. Therefore, this cause could be easily excluded.
Perioral dermatitis is mainly observed in the young, white, female
population as papulopustules with erythematous base. The condition has an
unclear aetiology. The eruption is predominantly perioral in location,
characteristically sparing the vermilion border of the lip, but it may also include
the perinasal and periorbital areas. Periocular dermatitis is a variant of this
condition and affects the skin around the eyes. The eruption is thought to be a
variant of rosacea, as biopsies show changes similar to those of rosacea. Therapy
typically includes cessation of topical steroids or other offending agents and
topical anti-inflammatory treatments such as topical metronidazole, topical
pimecrolimus cream, azelaic acid, as well as oral anti-inflammatory dose

antibiotics such as doxycycline 1, 2. This definitely not the condition suffered by
the patient as her lesions were spread widely over her face and neck. Therefore,
another cause should be considered.
Epidermal growth factor receptor inhibitors (EGFR inhibitors) are used
mainly to treat non-small cell lung cancer, colorectal cancer, and breast cancer.
They include gefitinib, cetuximab, erlotinib, and trastuzumab. The lesions due to
EGFR inhibitors appear as perifollicular papulopustular eruption distributed on
the face and upper torso. This occurs in up to 86% patients. Interestingly, the
presence and severity of the lesion correlate with a positive treatment response.
Therefore, without eruption, dosing may not be enough or the tumour is
unresponsive to the therapy 2, 19, 20. The patient did not suffer from cancer nor
currently taking any EGFR inhibitors. Therefore, this cause could be easily
excluded.
Drug-induced acne is a condition not dissimilar to steroid folliculitis and
may be caused by halogenated compounds containing bromides or iodides
commonly found in cold and asthma medication. Kelp that presents in many fad
diet pills, and other vitamin-mineral combinations are also amongst the most
common cause in young women 2, 21, 22. Chemicals that contain iodides, bromides,
and other halogens can also induce an acneiform eruption similar to that of steroid
acne; however, the iodide-induced eruption may be more extreme. Antibiotics
may induce an acute generalized pustular eruption. Penicillins and macrolides are
the greatest offenders. Patients usually are febrile with leukocytosis, and the
eruption does not usually involve comedones. Other implicated antibiotics include
co-trimoxazole, doxycycline, ofloxacin, and chloramphenicol. Other types of
medications can also produce an acnelike eruption, including corticotropin,
nystatin, isoniazid, itraconazole, hydroxychloroquine, naproxen, mercury,
amineptine 23, the antipsychotics olanzapine and lithium, chemotherapy drugs, and
epidermal growth factor receptor inhibitors (EGFR inhibitors) 1, 8, 24. History taking
matched the description for drug-induced acneiform eruptions. The patient had
been using fad diet pills for a prolonged period, and cessation of consumption did
help improve her lesions. Dermatological examinations also revealed relevant

findings, with pustular eruption localised on face and neck without the presence of
comedones. Therefore, it could be deducted that the patient's condition was due to
the kelp-containing fad diet pills consumption.
The goals of pharmacotherapy in acneiform eruptions are to reduce
inflammation, eliminate infection if present, reduce morbidity, and prevent
complications 1, 8, 21. In case of acneiform eruptions due to fungal infections,
antifungals can be used. The use of topical agents has few adverse effects besides
an allergic reaction to the active agent or inactive component. The mechanism of
action usually involves the inhibition of pathways (eg, enzyme, substrate,
transport) that are necessary for sterol and/or cell membrane synthesis, or the
permeability of the cell membrane (polyenes) of the fungal cell is altered. For this
purpose, ciclopirox, econazole, or ketoconazole are especially useful 12. As the
patient did not suffer from fungal infection, antifungal treatments were not
included within the treatment regiments.
Because the aetiology and the pathogenesis of acneiform eruptions have
not been fully elucidated, no established treatment schemes exist. A number of
options have been tried with various results; however, no controlled treatment
trials have been performed for this condition. Oral indomethacin consistently
appears to be most beneficial, at least in the classic form of the eosinophilic
pustular folliculitis. First generation antihistamines such as cyproheptadine and
hydroxyzine may alleviate itching in some HIV-associated cases of eosinophilic
pustular folliculitis. For nocturnal pruritus, sedating forms may be more effective 16. The patient suffered no eosinophilic pustular folliculitis, so oral indomethacin
usage would have no benefit. She also complained no itching, therefore,
antihistamine drugs were not given.
Empiric antimicrobial therapy must be comprehensive and should cover
all likely pathogens in the context of this clinical setting. Antibiotic treatments for
rosacea include tetracyclines and metronidazole. Dapsone is used in the treatment
of eosinophilic pustular folliculitis 16, 25. Conversely, stopping antibiotic usage is
the first thing that needs to be expedited in drug-induced varieties 2. Retinoid-like
agents such as topical tretinoin stimulate cellular retinoid receptors and help

normalize keratinocyte differentiation and are comedolytic. In addition, they have
anti-inflammatory properties. Oral isotretinoin also reduces sebum production in
the skin. Last but not least, acne products such as benzoyl peroxide, azelaic acid,
salicylic acid, and other concoctions can be used for the treatment of mild to
moderate acneiform eruptions. These agents may have antibacterial and
comedolytic properties. In severe cases, the agents may be used as an adjunct in
therapeutic regimens. As this is relevant, for the first visit the patient was
prescribed oral Doxycycline 100 mg to be taken twice daily, a topical gel
containing benzoyl peroxide 5% and clindamycin phosphate 1.2%, a topical lotion
containing 70% alcohol, propylene glycol, zinc oxide, precipitated sulphur 6%,
resorcinol 15%, and camphor to be used twice or three times daily, acne facial
wash, and an SPF 30 sunscreen lotion. On the follow-up visit, the patient reported
significant improvements on her previous complaints. A slight change in
therapeutic regiments was therefore given. Discontinuing the oral antibiotic and
topical benzoyl peroxide courses, she would then had to only apply topical
Clindamycin phosphate 1.2% gel twice daily, continuing the a topical therapy of a
lotion containing 70% alcohol, propylene glycol, zinc oxide, precipitated sulphur
6%, resorcinol 15%, albeit only once at night times, and acne facial wash. On the
final follow-up visit on the 4th of March 2016, the patient complimented the
progress of her improvements. Dermatological examination was performed and
revealing localised lesions on the face, which consisted of erythematous plaque
with several various sized papules and pustules. Therefore, the same therapy as
the previous visit which consisted of topical clindamycin phosphate 1.2% gel
twice daily, lotion containing 70% alcohol, propylene glycol, zinc oxide,
precipitated sulphur 6%, resorcinol 15%, once at night times, and acne facial wash
was given.

SUMMARY
A case of a 21 year-old young woman visiting the dermatovenereology outpatient
clinic of Saiful Anwar General Hospital (RSSA) with complaints of severe, pus-
filled multiple small bumps resembling acne that had quickly covered her face had
been reported. Careful history taking, physical examination, dermatological
examination, and microscopic examinations had established the diagnosis of drug-
induced acneiform eruptions, specifically due to fad diet pills. A treatment
regiment consisting of oral doxycycline 100 mg 2x1, a topical gel containing
benzoyl peroxide 5% and clindamycin phosphate 1.2%, a topical lotion containing
70% alcohol, propylene glycol, zinc oxide, precipitated sulphur 6%, resorcinol
15%, and camphor to be used twice or three times daily, acne facial wash, and an
SPF 30 sunscreen lotion as well as cessation of diet pill consumption had
successfully improved her conditions. Subsequent therapy removed the antibiotic
and benzoyl peroxide still resulted in marked improvements.

REFERENCES
1. Dessinioti C, Antoniou C, Katsambas A. Acneiform eruptions. Clinics in dermatology. 2014;32(1):24-34.
2. Goldsmith L, Katz S, Gilchrest B, et al. Fitzpatrick's Dermatology in General Medicine. New York: McGraw-Hill Education / Medical 2012.
3. Józwiak S, Schwartz RA, Janniger CK, et al. Skin lesions in children with tuberous sclerosis complex: their prevalence, natural course, and diagnostic significance. International Journal of Dermatology. 1998;37(12):911-917.
4. Song MG, Park KB, Lee ES. Resurfacing of Facial Angiofibromas in Tuberous Sclerosis Patients Using CO2 Laser with Flashscanner. Dermatologic Surgery. 1999;25(12):970-973.
5. Harden D, Keeling JH. PApular and nodular lesions of the scalp, face, and neck. Archives of Dermatology. 1997;133(8):1027-1028.
6. Dourmishev LA, Dourmishev AL. Syphilis: uncommon presentations in adults. Clinics in dermatology. 2005;23(6):555-564.
7. Fung MA, Berger TG. A Prospective Study of Acute-Onset Steroid Acne Associated with Administration of Intravenous Corticosteroids. Dermatology. 2000;200(1):43-44.
8. Anforth R, Liu M, Nguyen B, et al. Acneiform eruptions: A common cutaneous toxicity of the MEK inhibitor trametinib. Australasian Journal of Dermatology. 2014;55(4):250-254.
9. Laureano AC, Schwartz RA, Cohen PJ. Facial bacterial infections: Folliculitis. Clinics in dermatology. 2014;32(6):711-714.
10. Hubiche T, Sibaud V. Localized acne induced by radiation therapy. Dermatology online journal. 2014;20(2).
11. Park MY. Acneiform eruptions. 프로그램북 ( 구 초록집). 2012;64(2):196-197.
12. Durdu M, Güran M, Ilkit M. Epidemiological characteristics of Malassezia folliculitis and use of the May-Grünwald-Giemsa stain to diagnose the infection. Diagnostic microbiology and infectious disease. 2013;76(4):450-457.
13. Yadav P, Mendiratta V, Rana S, et al. Nevus comedonicus syndrome. Indian journal of dermatology. 2015;60(4):421.
14. Patel U, Terushkin V, Fischer M, et al. Eruptive vellus hair cysts. Dermatology online journal. 2012;18(12).
15. Haritha K, Parthasaradhi A, Jalu J. Eruptive vellus hair cyst. Indian Journal of Paediatric Dermatology. 2016;17(1):76.
16. Kim BW, Lee JH, Won CH, et al. Eosinophilic Pustular Folliculitis: Association with Long-Term Immunosuppressant Use in a Solid Organ Transplant Recipient. Annals of dermatology. 2014;26(4):520-521.
17. Rodrigues AM, De Hoog S, De Camargo ZP. Emergence of pathogenicity in the Sporothrix schenckii complex. Medical mycology. 2013;51(4):405-412.

18. Salas-Alanis JC, Cepeda-Valdes R, Bonifaz A. Primary cutaneous coccidioidomycosis: incidental finding. Journal of Clinical & Experimental Dermatology Research. 2012;2012.
19. Nakahara T, Moroi Y, Takayama K, et al. changes in sebum levels and the development of acneiform rash in patients with non–small cell lung cancer after treatment with egFr inhibitors. OncoTargets and therapy. 2015;8:259.
20. Stintzing S, Heinemann V. Author's reply to:“Prognostic value of cetuximab related skintoxicity in metastatic colorectal cancer patients and its correlation with parameters of the EGFR signal transduction pathway: Results from a randomized trial of the GERMAN AIO CRC Study Group”. International Journal of Cancer. 2013;132(7):1719-1720.
21. Gollnick HP, Zouboulis CC. Not all acne is acne vulgaris. Dtsch Arztebl Int. 2014;111(17):301-312.
22. Kazandjieva JS, Tsankov NK. Drug-Induced Acne. In Zouboulis CC, Katsambas DA, Kligman MA, (Eds). Pathogenesis and Treatment of Acne and Rosacea. Berlin, Heidelberg: Springer Berlin Heidelberg 2014:251-257.
23. Vexiau P, Gourmel B, Castot A, et al. Severe acne due to chronic amineptine overdose. Archives of Dermatological Research.282(2):103-107.
24. Baselga J, Gómez P, Greil R, et al. Randomized phase II study of the anti–epidermal growth factor receptor monoclonal antibody cetuximab with cisplatin versus cisplatin alone in patients with metastatic triple-negative breast cancer. Journal of clinical oncology. 2013;31(20):2586-2592.
25. Culp B, Scheinfeld N. Rosacea: A Review. Pharmacy and Therapeutics. 2009;34(1):38-45.