Embed Size (px)
Citation preview
Case presentationCase presentationMr K Ntombela, 44 year old gentlemanReferred from CJM hosp, and presented to Grey’s Hospital on 6th
February 2003 with a bicytopenia Hb 2,2 and platelet count of 34. On arrival to CJM the patient was actively bleeding, and it was decided to transfuse him with 2 units of packed red cells and platelets, with no response
Main complaint: 4 day history of sudden onset epistaxis followed more recently by haematemesis (dark red blood)In addition reports bleeding from the gums with easy bruising tendencies.No other bleeding diasthesis reportedNo history of trauma, toxin ingestion, or any other haematologicaldisorders, including family hxDescribes one other similar episode last year March 2002. Managed by a private GP who transfused 2 units of packed cells, with no history of further investigations or follow-up thereafter.
Systemic enquiry
CVS- Fatigue, dyspnoea grade II,No orthopnea or PND
Neurological- painful paraesthesia’s soles of feet dizziness (non-vertiginous)
No other significant past medical or surgical historyMedications- no previous ingestion of anti-inflammatory’s,
anticoagulants etc.Family history-nilEthic origin-Zulu(KZN)

On examinationGenerally
Well lookingNo active bleeding
Pallor ++
Not jaundicedOral thrush notedLymphadenopathy (<1cm)
-posterior cervical triangle
-axillary
Petechial Haemorrhages noticed on the gums, hard palate, tongue and forearms bilaterally
Bruises noticed over the anterior aspect of both foreams
Vitals:
BP122/51 Pulse 68, regular, good volume
RR 28bpm Temp 36.8 C
CardiovascularNormotensiveNot in Failure, no features of infective endocarditisS1 and S2 present and normal
Short ESM at LPSB grade 2/6- probably in keeping with a a flow murmurRespiratory:NAD (including no hilar lymphadenopathy)
Abdominal
No liver or spleen palpatedNo features of liver failureNo abdominal lymphadenopathyPR: malaena
Peripheries
Nails-no koilonychiaBruises of varying sizes over arms and lower limbsNo bony tenderness? Kaposi’s sarcoma lesion over anterior tibial surface LHS

Special investigationsSpecial investigationsBloods
FBC 31/1 06/2 14/2 16/2 22/2
HB 2,2 5,4 3,4 6,0 8,3WCC 23,5 12.3 7,3 7,0 11,3Platelets 34 9 13 3,0 5,0Corr retics 4,95RPI 1,9
Smear showed target red cells with assoc anisocytosis. Unfortunately no comment was made on platelets.
•U & E: Na 129 K2,3 Cl 101 HCo3 U 4,7 Cr 132
•INR 0,85
•PTT 20,1(p) 29,7(c)
•Bleeding time : prolonged
•Blood cultures: negative
•Malaria smear: negative

•Urine dipstix: trace blood, 1+leuco’s and 1+blood
•BMA: inadequate spp
•BMT: showed hypercellularity,all the haemopoeitic elements are seen. Good maturation noticed in the myeloid and erythroid series. Megakaryocytes are increased in number. Some have dysmorhic morphology with micro-megakaryocytes and hyperchromatic nuclei. There is no increase in reticulin fibrosis and no abnormal infiltrate. Granulomas not noticed.
Findings suggestive of ITP
•RVD status – positivetotal lymphocytes 800CD4 count not available yet
ManagementManagement
Patient was initially commenced on haematinics (pregamal, Vit B12), with 2 units of packed red cells and 5 units of pooled platelets being transfused. Subsequent repeat bloods and the patients clinical condition remained unchanged (platelets dropped to 5), suggesting an immune process in place. On confirmation of the diagnosis of ITP via BMT, oral prednisone 60mg dly was initiated with once again no clinical and biochemical improvement.
Dr Asmal (haematologist) at ALH was contacted on 24/2 and it was decided in view of the marked thrombocytopenia which was not responding to oral steroids and the patients RVD positive status, a splenectomy be considered as a next step.
Patient is currently being managed further at KEH.
ConclusionConclusion
Here we have a 44 year old gentleman who suddenly developed a bleeding diasthesis, following which relevant work-up confirmed an idiopathic thrombocytopenic purpura. As to the underlying predisposing factor, we felt that the most likely precipitant was his retroviral positive status, which brings us to the core of our discussion today: HIV and its effects it has on the haematological system.

ImmuneDrugs
Idiopathic
Non-immuneProstehesisSepsis/DICVasculitis
Excess destruction
Normal marrow
Production defect
Abnormal MarrowAplasia
Haem d/o
Normal spleen
Normal marrowLiver disease
TumourCongestive splenomegaly
Abnormal marrowLeukaemiaLymphomaHaem d/o
Splenomegaly
THROMBOCYTOPENIA

HAEMATOLOGY AND HIVHAEMATOLOGY AND HIV
Haematological effects are common in HIV infection.
The severity of its effects increases in advanced diseaseHaematological influences may be due to: HAART, opportunistic infections, malignancy or HIV infection itself.These may range from deviation in one cell line to a pancytopenia.
Bone Marrow
Usually displays a decreased cellularity and myelodysplasiaDecreased CD34 and Progenitor cellsIncrease cytokines TGF, TNF-alpha, IFN-gamma, IL-1Drug inducedInfections

Red blood cells
Anaemia is the most common abnormality in HIV infection. There is a disproportionate decrease in reticulocytes. Usually a normocytic normochromic anaemia manifests. A positive coombs tests may be present in 18-100% of patients. Of interest,a persistently low haemoglobin is predictive of a poor outcome.
Causes:
- Nutritional-Decrease in Vitamin B12 commonly, rarely folate- Opportunistic infections- TB, CMV- AZT- Hereditary syndromes- Pure red cell aplasia’s- Cytokine induced suppresion- Clinically significant haemolysis (rare)
Treatment:
1) Fe deficiency-ferrous sulphate2) Periodic packed cell transfusion3) Erythropoeitin4) IV immunoglobulins for Parvovirus B-19 related anaemia
White blood cells
- Neutropenia tends to occur with a decreased haemoglobin, howeverneutrophils may be increased in bacterial infections.
- Lymphopenia occurs due to the progressive decrease in CD4 countsAetiology:
1) Myelosuppression-HIV-Infections-Drugs (AZT/Bactrim/Acyclovir)
2) Peripheral destruction
Management
• Antibiotics if pyrexialGM-CSF which enhances HIV replication in monocytes and enhances
AZT antiretroviral effect
• G-CSF which partially corrects bacteriacidal defect

Thrombocytes
Thrombocytopenia is a common initial finding in HIV infection. The incidence increases with advancing disease. It is mainly of an immune basis, as opposed to anaemia and leucopenia which are mainly due to decreased haematopoesis.
Aetiology
1) Immune mediated destructionSimilar to ITP with a severe decrease in platelets and abundance ofmegakaryocytes in the bone marrow.
2) Decrease production3)TTP –usually seen in advanced HIV4)Sepsis/DIC5)Drugs
Treatment
- Spontaneous resolution in 10-20%.- AZT often improves the platelet count.- Steroids, however relapse is common with tapering- Splenectomy - IV Ig-rapid response of transient duration- Anti-D preparation-useful I refractory ITP
IMMUNE THROMBOCYTOPENIC PURPURAIMMUNE THROMBOCYTOPENIC PURPURA
ITP is an auto-immune disorder characterised by a low platelet count and muco-cutaneous bleeding. The incidence is 100/1million per year and half of these are children. This disorder occurs three times more commonly in females than males.
Classification1)Primary vs Secondary2)Acute vs Chronic (>6 months)
Adult onset and child onset ITP are strikingly different, with the acute form occuring in children and the chronic in adults.

NormalCoagulation time
Normal
Prolonged Bleeding time
Prolonged
ShortPlatelet survival (t)
Very short
Hyperplasia not present unless active bleeding
Bone marrowNormoblastic & myeloid hyperplasia
Same if purpura excessive
LeucocytesLeucocytosis
Normochromic with reticulocytosis
AnaemiaNormocytic normochromic
Larger bizzare platelets
MorphologyNormal
40000-200000Platelet count5000-20000
CHRONICACUTE
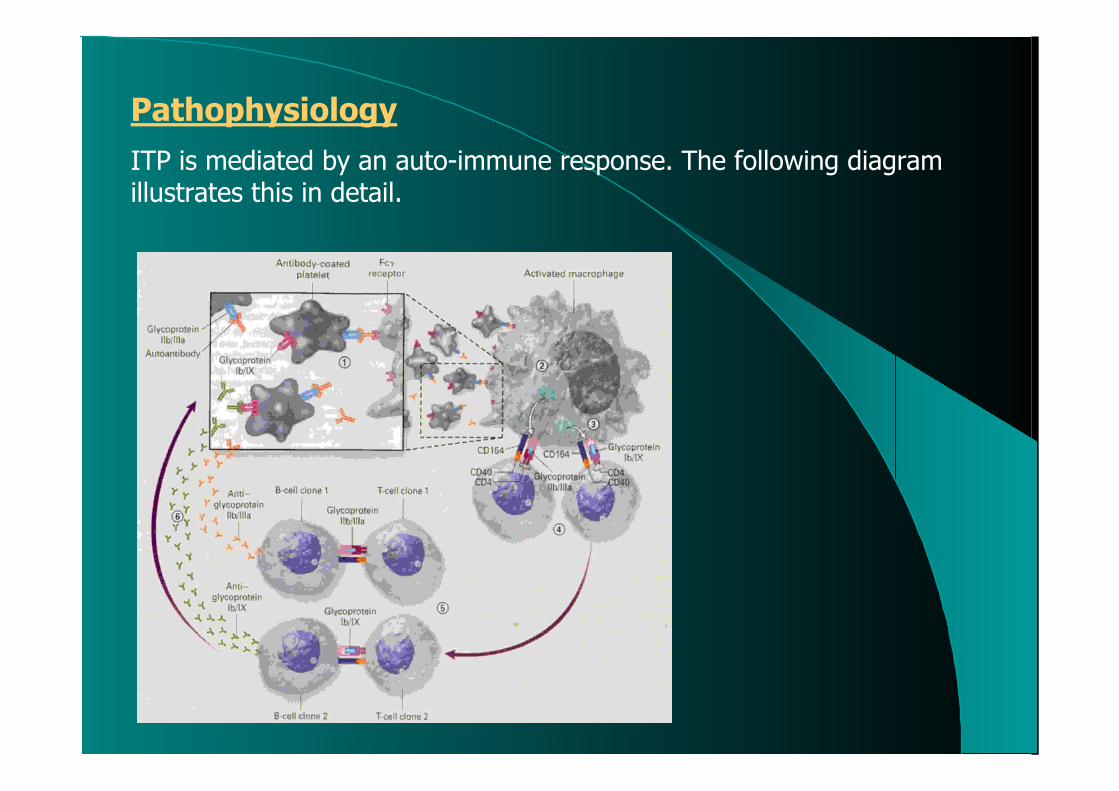
PathophysiologyITP is mediated by an auto-immune response. The following diagram illustrates this in detail.
Diagnosis
The diagnosis is mainly one of exclusion. Secondary causes which need to be excluded include SLE, Anti-phospholipid syndrome, immunodeficiency states, lymphoproliferative disorders, infection with HIV and hepatitis C virus and therapy with drugs such as quinidine and heparin.A few patients have concurrent auto-immune haemolytic anaemia, neutropenia or both which carry a less favourable prognosis.History and examination are important in excluding secondary causes and in distinguishing acute from chronic forms. Marked splenomegaly should trigger consideration of an alternative diagnosis. Apart from the thrombocytopenia the blood count should be normal. If abnormal it should be readily explained, for eg. anaemia due to epistaxis. A peripheral blood smear is required to rule out other haematolgic disorders like pseudothrombocytopenia, or inherited giant platelet syndromes. Large immature platelets are often seen. Much controversy surrounds the need for bone marrow studies in diagnosing ITP. According to the American Society of Haematology a bone marrow examination is not required if the presentation is typical but is appropriate before splenectomy is performed.

Some indications for a bone marrow investigation are:- Patients with atypical features for eg. those with additional cytopenias- Patients without a brisk response to therapy- Children, to rule out acute leukaemias- Atypical cases such as those with lassitude, protracted fever, bone orjoint pain, unexplained macrocytosis or neutropenia.

ManagementManagement
HaemorrhagePlatelet tx
IV IgPrednisone
30,000-50,000Prednisone orno treatment
Active BleedingIV Ig
PrednisoneSplenectomy
Splnectomy
<30,000
Spenectomy Gradual discontinuationof therapy or contmedical therapy
>30,000
Medical thereapyPrednisone/Danazol/
Dapsone
<30,000platelets
< 30,000 plateletsPrednisone
Anti-d Ig
30,000-50,000Prednisone orno treatment
>50,000 plateletsNo Rx

Advances in the management of HIV patients with ITP Advances in the management of HIV patients with ITP
Given that ITP occurs in as many as 40% of patients infected with HIV, much research and publications have been made regarding the bestmanagement of these patients
1) HAART- According to a study done in Virginia in 2000, showed that these drugs are effective in improving platelet counts, enhancing CD4 counts and reducing HIV loads
2) Interferon-Alpha-study conducted at University of California portrayed that a low dose continuous therapy of IFN resulted in a meaningful increases in platelet counts
3) Immune globulin IV according to study in Scotland showed a definite increase in platelet count and was beneficial. It seems to have a particular role in HIV patients suffering from Parvovirus B19,or measles infection, or patients with auto-immune disease.
4) Splenectomy has proved effective in the course of HIV infection prior to the onset of symptomatic AIDS.

SummarySummary
In summary, our case discussion serves as a mere example in which the HIV virus may affect the haematological system. It therefore should always be borne in mind when faced with any haematological disorder, in the South African context in particular.
Of interest, in our experience here at Grey’s Hospital, we have witnessed numerous cases of HIV patients presenting with a range of haematological disturbances, most of which have been mentioned here today.
ReferencesReferences
1) The New England Journal of Medicine, Vol 346, March 28,2002, no.13, Medical Progress: Immune Thrombocytopenic Purpura
2) Harrison’s Principles of Internal Medicine Volume I, 14th Edition
3) The Southern African Journal of HIV Medicine, July 2002 pg 37-38, The Haematology of HIV infection
4) Colour Atlas and Textbook of Haematology, 2nd Edition, William R.Platt
5) Internet: Abstract articles - Pubmed



























![[Msd07]mapping cjm](https://img.pdfslide.us/doc/110x75/55ab7ad21a28abd1418b478f/msd07mapping-cjm.jpg)