Embed Size (px)
Citation preview

Case PresentationA 47-year-old Taiwanese male without significant past medical history presented with complaints of dizziness, decreased urination and diarrhea. On exam he was noted to be markedly orthostatic. The abdomen was slightly distended. After voiding, foley catheterization returned approximately one liter of residual urine. Laboratory evaluation was remarkable for hyponatremia. The patient was admitted for intravenous hydration with a presumptive diagnosis of dehydration secondary to gastroenteritis.
Despite aggressive fluid resuscitation his orthostasis did not resolve. He could not tolerate sitting up for more than a few minutes as his systolic blood pressure would acutely drop to 50-60mm Hg. He also exhibited dry skin, dry mouth, dry eyes, blurry vision and poor heart rate variability. An extensive evaluation for causes of autonomic insufficiency did not reveal adrenal insufficiency, paraneoplastic syndrome, myasthenia gravis, Parkinson’s or cancer. A ganglionic acetylcholine receptor antibody test for autoimmune autonomic ganglionopathy was negative. Given the patient’s extensive negative evaluation and his constellation of symptoms consistent with autonomic failure, a diagnosis of autoimmune autonomic ganglionopathy was made. No benefit was noted after treatment with fludrocortisone and midodrine hydrochloride. Plasmapheresis and intravenous immunoglobin (IVIG) was initiated and the patient had significant symptomatic improvement.
DiscussionAutoimmune autonomic ganglionopathy (AAG) is a type of autonomic insufficiency that includes both parasympathetic and sympathetic dysfunction and is thought to have an immunologic basis. It may occur after a viral illness or with cancer, most commonly non-small cell lung cancer. AAG usually develops subacutely over days to weeks. Characteristic clinical features include gastrointestinal dysmotility and an abnormal pupillary response to light and accommodation. Serologic testing may be positive for an autonomic ganglionic acetylcholine receptor antibody, but a negative result does not exclude the diagnosis. Treatment is supportive and fludrocortisone and midodrine hydrochloride help with orthostatic hypotension. There is no definitive course-modifying treatment. Recovery after plasma exchange and IVIG therapy has been reported. Spontaneous recovery may also occur.
ConclusionsReview of this case may help practitioners recognize this rare form of autonomic insufficiency.
AUTONOMIC NERVOUS SYSTEMAUTOIMMUNE AUTONOMICGANGLIONOPATHY (AAG)
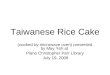
Figure 1 - Anatomy of the Autonomic Nervous System
AUTONOMIC NERVOUS SYSTEM (ANS)
• Controls involuntary or “autonomic” functions of the body• Typically divided into three components
1. Sympathetic (Craniosacral)2. Parasympathetic (Thoracolumbar)3. Enteric
• Signals from spinal autonomic neurons synapse with ganglionic neurons
• Ganglionic neurons send axons to innervate target organs (Figure 1)
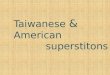
• Nicotinic acetylcholine receptors (AChR) are the same in sympathetic and parasympathetic ganglia (Figure 2)
• Pentameric transmembrane complex (2 alpha ,3 beta subunits)• Ligand-gated ion channel• Fast synaptic transmission• Immunologically distinct from AChR at the neuromuscular
junction
Figure 2 – Nicotinic AChR a)Muscle AChR b) Ganglionic AChR c) Transmembrane AChR receptor, antibodies recognize extracellular alpha subunits (Reproduced from Vernino, S., Winston, N. Autoimmune autonomic ganglionopathy. Front Neurol Neurosci. (26) 85-93, 2009.)
Background• AAG first described by Young et al. in 1969• Auto-antibodies to the ganglionic AChR identified 10 years ago• AAG is a distinct disorder but may share many clinical features with other types of autoimmune disorders that affect the ANS (paraneoplastic, acute inflammatory demyelinating polyradiculopathy (Guillain-Barre), diabetic autonomic neuropathy)• AAG is an acquired neurological disorder characterized by diffuse autonomic failure Sympathetic (orthostatic hypotension, anhidrosis) Parasympathetic (dry eyes and mouth, fixed pupils, bladder and sexual dysfunction) Enteric (ileus, colic, diarrhea, and constipation)• Key distinction: AAG spares somatic nerve function Pathophysiology• Alpha-3 subunit of the AChR is the target in AAG• AAG is an antibody mediated disorder caused by reversible disruption of fast synaptic transmission in autonomic ganglia Clinical Presentation• Mean age 52 years (22-82) with slight female predominance (60-65%)• Acute and subacute AAG can affect children, although they are uniformly seronegative for ganglionic AChR antibodies)• Typically presents in previously healthy individual• May follow viral prodrome (upper respiratory or gastroenteritis) = 60% cases No specific association, but Epstein-Barr virus most commonly reported• Constellation of tonic pupils with gastrointestinal dysmotility (70%) in the setting of severe orthostatic hypotension(70%) is suggestive of AAG• Most common presentation is severe and subacute (66% cases)• 25% patients report neuropathic symptoms (tingling distal extremities) but sensory and nerve conduction studies are normal Diagnosis• AAG diagnosed on clinical grounds after excluding other etiologies• Up to 50% of patients with acute or subacute AAG have high antibody levels• High antibody levels correlate with severe phenotype and rapid onset• High antibody levels are specific for AAG and not found in other neurological disorders• Sensitivity of the antibody is only around 50%• Patients may be seronegative Autoimmune mechanism still postulated due to clinical similarity to seropositive AAG Some seronegative patients respond to immunomodulatory treatments• Cerebrospinal fluid analysis may show modest elevation in protein Treatment• Decrease in antibody levels is associated with improvement• Typically not diagnosed for many months after patient presents
• AAG is rare• Similarity with other forms of autonomic failure• Lack of routine diagnostic tools
• Initial treatment is largely symptomatic (volume expansion, fludrocortisone, erythropoietin, midodrine, lower extremity support hose, bowel and bladder management, supplemental moisture agents for dry eyes and mouth, pyridostigmine or other cholinesterase inhibitors)• In severe cases immunomodulatory treatment (corticosteroids, plasma exchange, intravenous immunoglobulin as well immunosuppression with azathioprine, mycophenolate mofetil or rituximab)• Long-term management needs to be tailored to the individual patient.
Summary Points
1) AAG is a severe, potentially treatable, form of antibody-mediated autonomic failure.
2) AAG manifests as gastrointestinal dysmotility, abnormal pupillary light response, bladder dysfunction, sicca complex, anhidrosis and orthostatic hypotension.3) Ganglionic AChR antibodies are very specific for AAG and levels correlate with disease severity.4)There are no proven therapies, but immunomodulatory treatments (plasma exchange, intravenous immunoglobulin and immunosupressants) can be considered for severe cases.
REFERENCES:1) Vernino, S, et al. Autonomic ganglia, acetylcholine receptor antibodies, and autoimmune gangliopathy. Autonomic Neuroscience: Basic and Clinical. 146 (2009) 3-7.2) Vernino, S, Winston, N. Autoimmune autonomic ganglionopathy. Front Neurol Neurosci. (26) 85-93, 2009.3) Iodice, V, et al. Immunotherapy for autoimmune autonomic ganglionopathy. Autonomic Neuroscience:Basic and Clinical. (146) 22-25, 2009.4) Vernino, S. Antibody testing as a diagnostic tool in autonomic disorders. Clin Auton Res. (19) 13-19, 2009.5) Vernino, S, et al. Autonomic ganglia: Target and novel therapeutic tool. Neurology. 70(20) 1926-1932, 2008.6) Schroeder, C, et al. Plasma exchange for primary autoimmune autonomic failure. New England Journal of Medicine. 353:1585-1590, 2005.7) Harrison's Principles of Internal Medicine, 17th edition. Fauci, A, et al. McGraw-Hill Companies, Inc. 2008.8) Adams and Victor’s Neurology, 9th edition. Samuels, M.A. McGraw-Hill Companies, Inc. 2009.
SCHOOL of MEDICINEDEPARTMENT of INTERNAL MEDICINE