Embed Size (px)
Citation preview

Case of the Season
By Mayank Goyal, Raju Sharma, and Manorama Berry
A 5-YEAR-OLD male child presented with pro- gressively increasing jaundice for the last 3
months and a recently noticed firm lump in the epigastrium. There was history of jaundice 1 year ago, which subsided spontaneously over 3 weeks. No investigations of the previous episode were available.
On examination, the child was emaciated and jaundiced. A firm, well-defined lump was palpable in the epigastrium; the lump was inseparable from the liver. Mild splenomegaly was also present. There was no evidence of ascites.
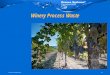
Fig 1. An isoechoic bulge in the left lobe of liver is seen. There is no distinct margin with normal liver.
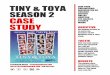
Fig 3. Chest radiograph reveals bilateral interstitial pat- tern.
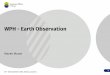
Laboratory investigations revealed serum biliru- bin of 3.5 mg%, alkaline phosphatase of 400 iU (normal up to 250 IU), and mildly elevated serum glutamate oxaloacetate transaminase (SGOT) and serum glutamate pyruvate transaminase (SGPT). Ultrasonography (Fig 1) showed an isoechoic bulge in the left lobe of liver; its margin from the normal liver could not be appreciated. There was no central scar or calcification. Hepatic veins and portal vein radicals did not reveal any abnormality. Intrahe- patic biliary radicals (IHBR) were not dilated. The caudate lobe was hypertrophied. Mild splen 0- megaly was seen. Computed tomography (CT) scan (Fig 2) confirmed the above-mentioned find- ings. The mass was isodense before and after intravenous contrast, and a routine chest radiograph at the time is shown (Fig 3).
Fig 2. The same region shows an isodense mass with no distinct margin with the normal liver, The caudate lobe is hypertrophied (~).
From the Department of Radiodiagnosis, All India Institute of Medical Sciences, New Delhi, India.
Address reprint requests to Raju Sharma, MD, Department of Radiodiagnosis, All India Institute of Medical Sciences, New Delhi 110 029, India.
Copyright © 1997 by W.B. Saunders Company 0037-198X/97/3203-000255.00/0
Seminars in Roentgenology, Vot XXXII, No 3 (July), 1997: pp 147-149 147

148 GOYAL, SHARMA, AND BERRY
DIAGNOSIS
Langerhans' Ceil Histiocytosis With Sclerosing Cholangitis [SC] Causing Secondary Biliary Cirrhosis
Subsequently, CT scan of the chest (Fig 4) was performed, which confirmed the presence of bilateral interstitial lung disease. Radiograph of the skull (Fig 5) showed multiple well-defined lytic lesions with a beveled edge confirming the diagnosis of Langerhans' cell histiocytosis (LCH). Liver biopsy showed evidence of bili- ary cirrhosis secondary to sclerosing cholangitis
(SC). SC is a relatively infrequent cause of jaundice in
a child. However, up to 15% to 24% of SC in children is caused by LCH.1,2 The clinical presenta- tion of this case with jaundice and epigastric lump is unusual. However, the lump that is part of the left lobe of liver is isoechoic and isodense on ultrasonog- raphy and CT scan, respectively; it has no distinct margin, is not reaching up to the porta hepatis, and the IHBR are not dilated. There is significant hypertrophy of the caudate lobe. In addition, sple- nomega!y is present. This should lead one to suspect a hypertrophied left lobe caused by cirrho- sis rather than a mass.
LCH is high in the differential diagnosis for a child with bilateral interstitial pattern seen in the chest radiograph who is otherwise free of symp- toms referable to the chest. Although there is no
Fig 4. CT scan of chest confirms presence of bilateral interstitial lung disease.
Fig 5. Skull radiograph shows multiple well-defined lytic lesions.
characteristic imaging finding that suggests the diagnosis of SC, the history of self-remitting jaun- dice, absence of dilated IHBR, and the known association between LCH and SC are helpful features. Laboratory parameters may be inconclu- sive owing to coexistence of obstructive and nonob- structive jaundice.
LCH represents a single nosologic entity that covers a range of disorders (including Letterer- Siwe, Hand-Schuller-Christian, and eosinophilic granuloma) characterized by abnormal prolifera- tion of histiocytes that form giant cells normally found in the phagocytic system of the skin, esopha- gus, vagina, and buccal mucosa. Liver involvement is common in disseminated LCH (representing 40% to 60% of cases), most often affecting chil- dren under 2 years of age. Histopathological fea- tures of liver involvement have been staged in four phases: (1) infiltration of the portal tract by histio- cytes, (2) a granulomatous phase, (3) a xanthoma- tous phase, and (4) a late fibrous phase leading to cirrhosis. 3
This case would represent the last stage of liver involvement. The prognosis for these patients is extremely poor with liver transplantation being the only viable option. 3

CASE OF THE SEASON 149
REFERENCES
1. Sisto A, Feldman P, Garel L, et al: Primary sclerosing gitis in children. J Pediatr 124:49-56, 1994 cholangitis: Study of five cases and review of literature. 3. Zandi R Panis Y, Debray D, et al: Pediatric liver transplan- Pediatrics 80:918-923, 1987 ration for Langerhans' cell histiocytosis. Hepatology 21:129:
2. Debray D, Periente D, Urvoas E, et al: Sclerosing cholan- 133, 1995