Embed Size (px)
Citation preview
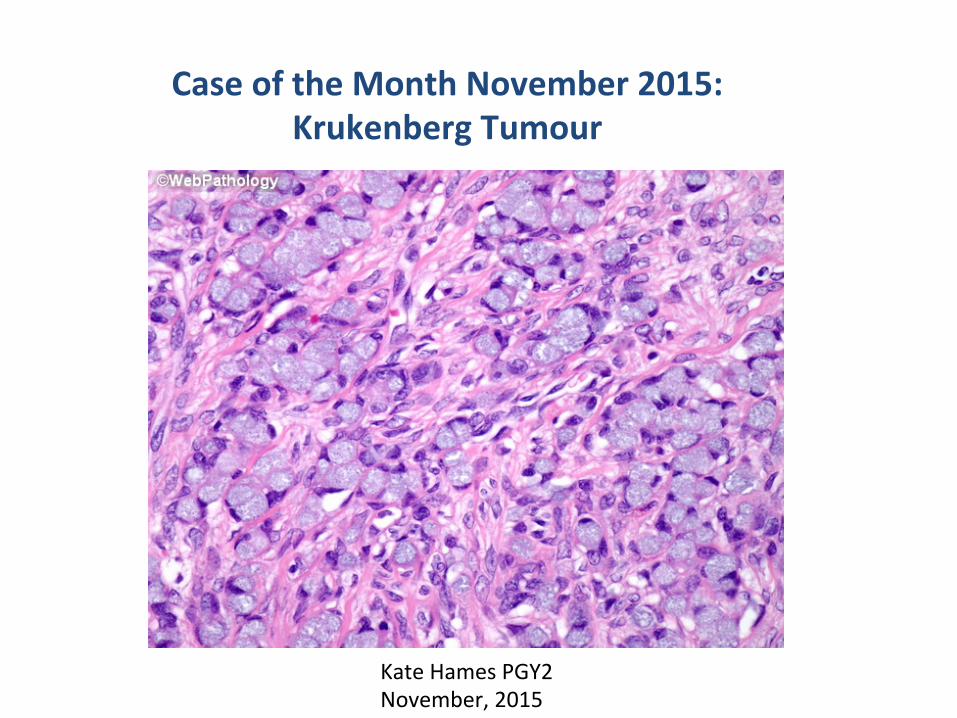
Case of the Month November 2015: Krukenberg Tumour
Kate Hames PGY2 November, 2015

Case Report
70 year-‐old female presents with a 6 month history of severe worsening heartburn, consApaAon, and vague lower abdominal and pelvic pain. Vitals: Non febrile HR 80 BP 145/95 CBC: Normal Liver enzymes: Normal Lipase: Normal
Physical Exam: Mild epigastric tenderness NegaAve Murphy’s Mild tenderness in RLQ and LLQ DRE negaAve
Past Medical Hx: Remote history of bladder tumour resecAon. Previous smoker, quit 10 years ago

Ø DiagnosMc Imaging: CT and Ultrasound
InvesMgaMons
Ø Gastroscopy and Colonoscopy
Ø Biopsy and Pathology

Axial image demonstraMng thickened gastric wall
InvesMgaMons: CT

CT axial image of bilateral adnexal masses

Coronal reformats of adnexal masses

SagiTal Reformats of adnexal masses

Ø Abnormal thickening of the gastric body wall with mucosal enhancement.
Ø Abnormal stranding of the fat planes within the gastrohepaAc ligament as well as inferior to the gastric body.
Ø Extensive omental nodularity beneath anterior abdominal wall in keeping with omental metastases.
Ø Moderate volume of pelvic free fluid. Ø Large heterogenous enhancing mass in the right adnexa suspicious for a solid right ovarian mass. Similar appearing mass in the leW adnexa.
CT imaging findings
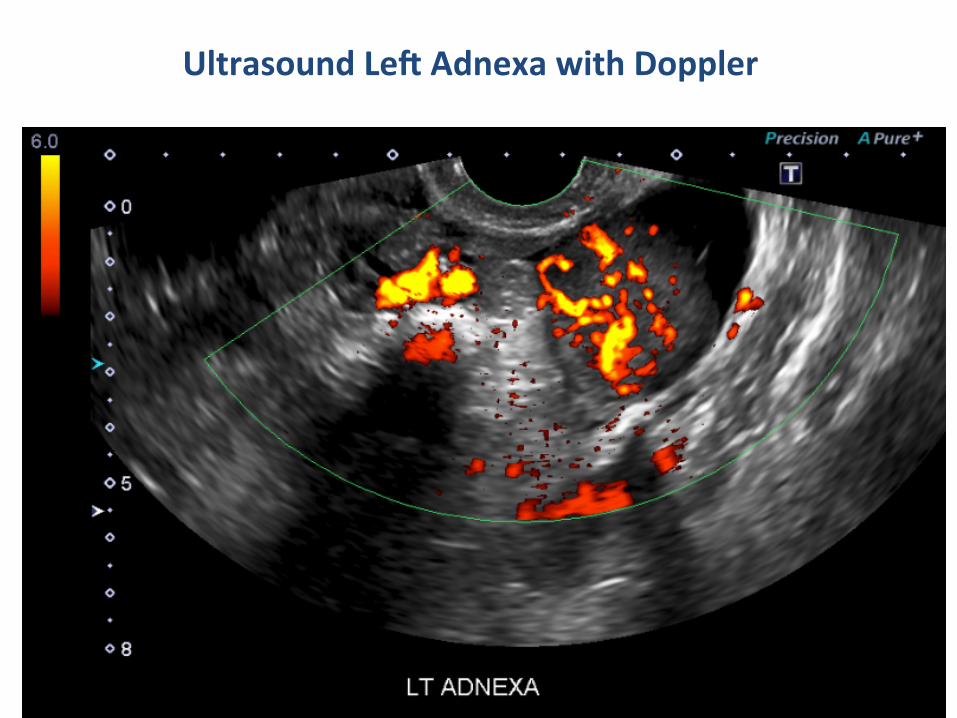
Ultrasound LeW Adnexa with Doppler
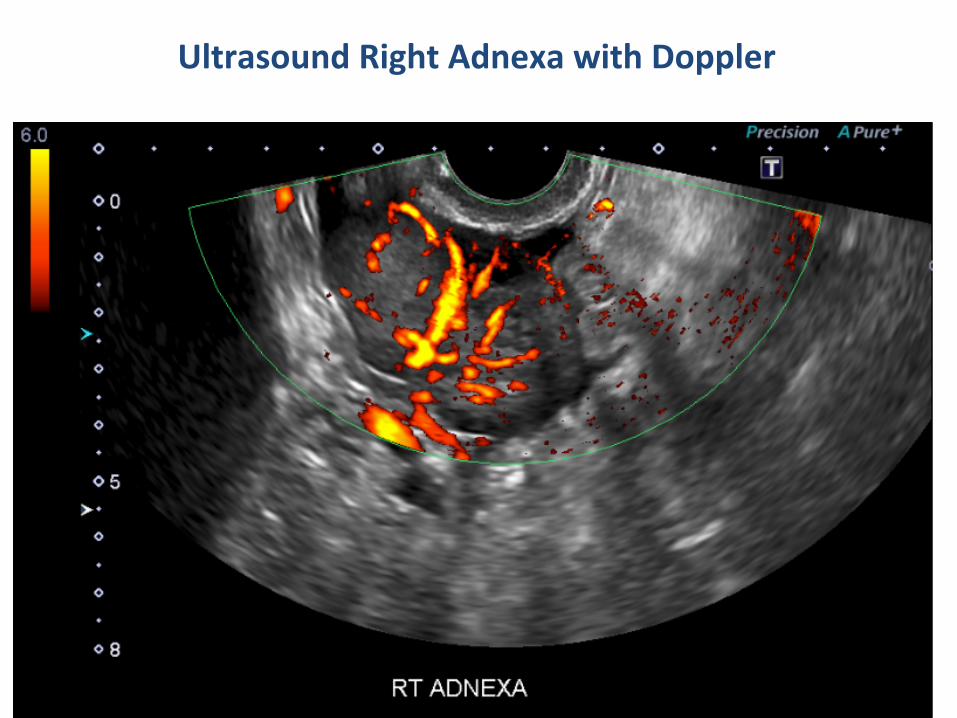
Ultrasound Right Adnexa with Doppler

Ø The uterus is anteverted and atrophic. Normal endometrium. Ø Right adnexal lobulated mass measuring 5.4 x 3.2 cm with associated hypervascularity.
Ø LeW adnexal lobulated mass measuring 4.4 x 3.2 cm with associated hypervascularity.
Ø Free fluid within the pelvis.
Ultrasound Findings
InvesMgaMons ConMnued
Gastroscopy demonstrated severe gastriAs along the lesser curve from the mid body to the GE juncAon. A visible tumour extended from the distal esophagus to the lesser curvature just proximal to the antrum. There was marked liniAs plasAca. Colonoscopy was unremarkable aside from diverAculi.
Biopsies from the first endoscopy showed poorly differenMated adenocarcinoma of the stomach. The second biopsy demonstrated small foci of signet ring cell carcinoma.
Pathology confirmed metastaMc HER2-‐neu negaMve gastric cancer.

Diagnosis:
In the context of signet ring cell gastric carcinoma, the bilateral adnexal masses are favoured to be bilateral ovarian metastases in keeping with Krukenberg tumour.

Krukenberg Tumor
Ø “Signet ring” subtype of metastaMc ovarian tumor, also known as carcinoma mucocellulare.
Ø The most common primary tumours are stomach and colon, followed by breast, lung, and contralateral ovarian tumour
Epidemiology
Ø Krukenberg tumors are 5-‐10% of all ovarian tumors, and up to 50% of all metastaAc ovarian tumours
Pathology
Ø Histology demonstrates mucin-‐secreAng “signet ring” cells; the cells typically originate from the stomach, followed by colorectal, breast, lung, contralateral ovarian carcinoma, pancreas, and cholangiocarcinoma
Jung et al 2002

Webpathology.com
Nests and clusters of signet ring cells filled with basophilic mucin seen infiltraAng spindled stroma
Pathology: Signet Ring Cells

DiagnosMc Imaging CharacterisMcs of Krukenberg Tumour
CT: Ovarian masses may be mixed cysAc-‐solid or primarily solid, and may be indisAnguishable from primary ovarian carcinoma. Krukenberg tumor may be suspected if there are addiMonal gastric or colonic lesions idenMfied. Ultrasound: Findings are typically bilateral solid ovarian masses with well-‐defined margins. A characterisAc feature for Krukenberg tumor includes an irregular hyper-‐echoic solid paTern and “moth-‐eaten like cyst formaMon” (Radiopaedia).
Jung SE et al, Radiographics 2002
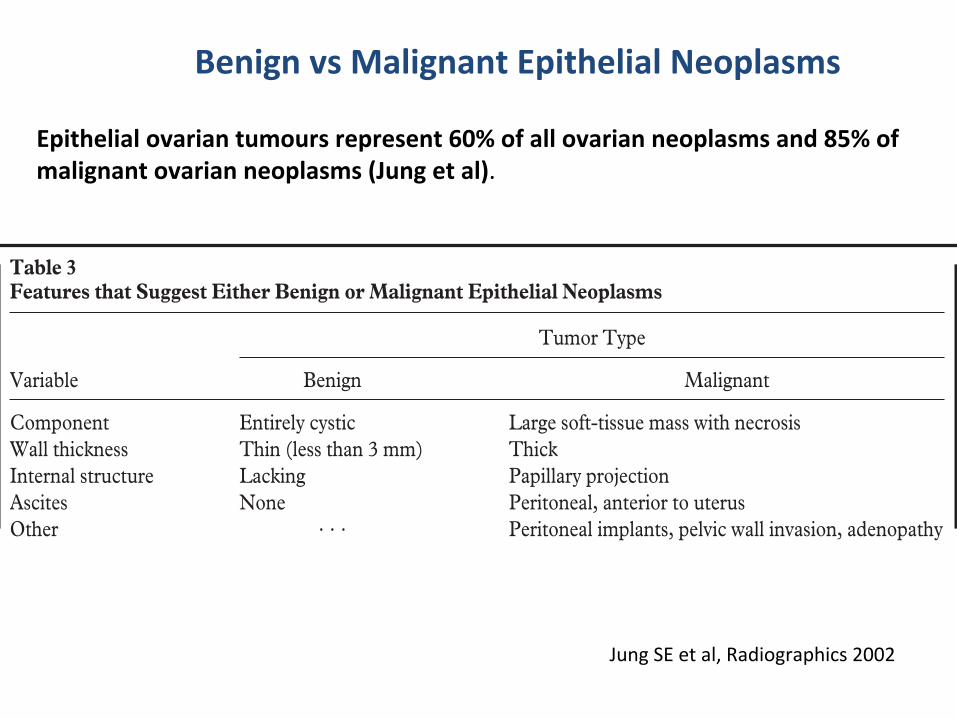
Benign vs Malignant Epithelial Neoplasms
Epithelial ovarian tumours represent 60% of all ovarian neoplasms and 85% of malignant ovarian neoplasms (Jung et al).
(10). Exceptionally large benign neoplasms occurare occasionally seen and are more likely to re-main clinically silent as they grow (11). Epithelialtumors with low malignant potential demonstrate
more proliferation of papillary projections than dobenign cystadenomas (Fig 6) and are often seenin younger patients (14,15). Epithelial tumors
Figure 5. Ruptured mucinous cystadenocarci-noma in a 36-year-old woman. (a) Sagittal turbospin-echo T1-weighted MR image (repetitiontime msec/echo time msec ! 464/14) shows alarge, multilocular mass with heterogeneous highsignal intensity but with variable signal intensityin the locules. (b) On an axial turbo spin-echoT2-weighted MR image (4,511/132), the massdemonstrates high signal intensity, and there aremultiple locules with a honeycomb appearance.The tumor wall is disrupted by spillage of themucinous material (arrows). (c) Gadolinium-enhanced fat-suppressed turbo spin-echo T1-weighted MR image (782/14) demonstratesmarked enhancement of the tumor wall andsepta.
Table 3Features that Suggest Either Benign or Malignant Epithelial Neoplasms
Variable
Tumor Type
Benign Malignant
Component Entirely cystic Large soft-tissue mass with necrosisWall thickness Thin (less than 3 mm) ThickInternal structure Lacking Papillary projectionAscites None Peritoneal, anterior to uterusOther . . . Peritoneal implants, pelvic wall invasion, adenopathy
RG f Volume 22 ● Number 6 Jung et al 1309
Radio
Gra
phic
s

Treatment and Prognosis
Ø Treatment varies widely depending on primary tumour, extent of metastases, invasion of nearby organs, and overall baseline health of the paAent.
Ø Many paAents receive chemotherapy; some receive
radiaAon; some may receive surgery for the primary tumour and/or debulking surgery.
Ø Prognosis also varies widely depending on the primary
tumour and extent of metastases.
Case report conclusion
Ø Our paAent was diagnosed with metastaAc HER2-‐neu negaAve signet ring cell carcinoma with Krukenberg ovarian tumour metastases.
Ø She received six cycles of ECF/X chemotherapy and now conAnues on Capecitabine.
Ø She was not a candidate for radiaAon therapy and has not undergone surgery.
Ø She is now 1 month post-‐chemo and progress reports indicate she is declining in health but sAll living at home with her husband.
Ø Follow up imaging post-‐chemo is sAll pending.

References
Al-‐Agha OM, Nicastri AD et al. An in-‐depth look at Krukenberg tumor. Arch pathol Lab Med 2006; 130: 1725-‐1730. Cho KC, Gold BM. Computed tomography of Krukenberg tumors. AJR Am J Roentgenol. 1985;145: 285-‐8. Goel A, Weerakkody Y et al. Krukenberg tumour. Radiopaedia.org 2015. Ha HK, Baek SY et al. Kruenberg’s tumor of the ovary: MR imaging features. AJR 1995; 164:1435-‐1439. Jung SE, Lee JM et al. CT and MR imaging of ovarian tumors with emphasis on differenAal diagnosis. RadioGraphics 2002; 22:1305-‐1325.





























