Embed Size (px)
Citation preview

Case of Spinal TumorComplicating Pregnancy
Presentor : Dr. Deepmala
Designation : Fellow in HRP and Perinatology
Hospital : Fernandez Hospital, Hyderabad
Date of Presentation : 12.04.2011


Contents of this presentation
Approach to Paraplegia / Backache
Case Details
Discussion:
– Spinal Tumor
– Subacute combined degeneration of cord
– Muscular dystrophy

Approach To Paraplegia
Definition: Paralysis of lower part of the body,
commonly affecting both legs and often
internal organs below waist

Level of lesion
Upper Motor Neuron Lesion
Lower Motor Neuron Lesion

Spinal Cord

Spinal Reflex Arc

UMN -LMN


UMN Lesions Causing ParaplegiaSPINAL LESIONS (common)
SPINAL CORD COMPRESSION
– Pott’s disease
– Disc prolapse
– Fracture
– Tumors
– Epidural abscess,
– Cervical spondylosis
VASCULAR
– Hemorrhage
– Infarction

SPINAL LESIONS (common)
SYSTEMIC DEGENERATION OF TRACTS
– Multiple sclerosis
– Sub acute combined degeneration of cord
INFECTION
– Transverse myelitis
– Neurosyphilis

CEREBRAL LESIONS (uncommon)
– Thrombosis of superior sagital sinus
– Tumor of falx-cerebri
– Hydrocephalus
UMN Lesions Causing Paraplegia

LMN Lesions Causing Paraplegia
Anterior horn cells : Poliomyelitis, Motor
neuron disease
Peripheral nerve : Peripheral neuropathy
Neuromuscular junction : Myasthenia gravis
Muscles : Muscular dystrophies

UMN Vs LMN Lesion

UMN-Spinal Cord Lesions
Intramedullary
Extramedullary, intradural


How to Differentiate Clinically?
Extramedullary Intramedullary
Root pain common rare
UMN signs early late
Sensory deficit
Contralateral loss of pain/temp;
ipsilateral loss of proprioception
Dissociated sensory loss

Approach to Backache - (Causes)
Degenerative : Musculoligamentous, facet joint,
osteoporosis
Trauma
Tumour : Intra / extradural, pathological fracture
Infection : Pyogenic, TB, discitis, osteomyelitis
Inflammatory
Vascular : Aortic aneurysm

Diagnostic triage Includes
– History
– Examination
– Investigation
Aids differentiation between :
Simple backache
Nerve root pain
Serious pathology
Tumour/Infection/Central disc prolapse

Simple Backache
Presentation : 20 – 55 yr age
Lumbosacral region : Buttocks and thighs
Mechanical pain : Varies with physical activity
and time
Patient well
Prognosis : 90 % recover

Nerve Root (Radicular) Pain
Unilateral leg pain worse than LBP
Radiation to foot or toes
Radicular Sx or signs : Straight leg raising / Sensory
disturbance / Motor weakness / Reflex changes
Prognosis : 50% carries good prognosis

Warning Signs of Serious Pathology
Age of onset : < 20 and > 55 years
Constant unremitting progressive pain
Thoracic radicular pain
Systemically unwell, weight loss
Drug abuse, HIV
Structural deformity
Significant trauma

Backache - Inflammatory Disorders
Gradual onset before 40 years
Marked morning stiffness
Persisting limitation of spinal motion
Peripheral arthritis
Iritis, psoriasis, colitis, urethritis
Family history

Cauda Equina Syndrome : Central Disc Prolapse
Bilateral leg pain
Saddle anaesthesia
Bilateral foot
weakness
Bil. loss of ankle reflex
Loss of anal tone
Urinary incontinence

Case Details
Mrs X, 25 yrs
Married since FEB 2012
Nonconsanguinous marriage
G2A1,39 Wks; Referred in view of paraparesis (6th Nov)
Obstetric history:
G1- Missed miscarriage @ 8 wks,2012 spontaneous
expulsion
G2- Present pregnancy, Spontaneous conception

Case Details
First Trimester – Folic acid
Second Trimester – Iron, calcium supplements;
Fetal anomaly scan (TIFFA) – Normal
Third Trimester – Fetal wellbeing scan Normal
– Two doses Tetanus toxoid √, Hematinics√

Symptoms
Low backache since 1 year; gradual onset ; slowly
worsening
Difficulty in walking- fourth month of pregnancy
Difficulty in sitting ,getting up & turning in bed
Gradual onset, slowly progressing

Symptoms
Initially walking with support of wall / staircase;
Since 15 days restricted activity, almost
bedridden,(only going to washroom with walker
and support of an attendant)
No h/s of upperlimb weakness, cranial nerve
palsies or bowel-bladder involvement

Case Details
Past history: Nil
Family history:
Parents HTN and DM
Muscular Dystrophy-Father and Paternal
cousins
Two of her brother had tuberculosis

Clinical Findings
Obese lady BMI=39, comfortable in supine
Pedal oedema++, U/A-Trace
PR-90/min,BP-120/70 mm Hg
RS- Air entry bilaterally equal, CVS-S1,S2+
P/A –Uterus Term, relaxed,
– Presentation: Cephalic 4/5, Fetal Heart Sound+

Motor Examination of lower limbs
Exam RT LL LT LL
Bulk N N
Tone (Proximal/Distal) N/Flaccid N/Flaccid
Power 1/5 3/5
Knee jerk Brisk Brisk
Ankle jerk ++ ++
Plantar jerk Upgoing Upgoing

Other Neurological Findings
Patchy sensory loss in lower limbs- touch,pain,
position sense;?level
Motor and sensory: Both Upper limbs normal
Higher functions N, All Cranial Nerve N
No Cerebellar signs/meningeal signs
Spine normal

Differential Diagnosis
Myeloradiculopathy
Subacute combined degeneration of
spinal cord
Muscular dystrophy

Initial Investigations
Hb- 10 gm/dl
Blood group: O Positive
TSH- 1.26
HIV & HBsAg- Nonreactive
OGTT- 79/123/98 @ 20 wks
TIFFA,Fetal wellbeing scan- Normal

Lab Investigations
Lab Parameters 31/10 6/11
Hb / WBC 13.5/9800 13.5/11,100
PLT 2.14 1.63
LFT /RFT N N
CUE /U-C N N
Vit B12 - 201
CPK - 174
LDH - 353
ESR - 84

Multidisciplinary Care
Obstetrician, Physician, Anaesthetist, Neurophysician and
Neurosurgeon

MRI DORSAL SPINE with Screening of Cervical Spine
Well defined, regular, Space occupying lesion (2.2
x1.01 cm ) iso-intense(Gray matter ) all sequences
Intradural, extramedullary between D2/D3
Subtle cord edema
Possibly Schwannoma / Meningioma

MRI Images

Delivery Details
Elective LSCS with Thoracic( T1-3)
Laminectomy and Excision of intradural
Meningioma under GA on 9/11/13
Girl , 3.5 kg ,(8/9/9)
HPE- Meningioma
(Meningiotheliomatous/Transitional type)

Post Op Period
Inj Ceftriaxone, Amikacin, LMWH X 3 Days
Regular-Physiotherapy
Suture removal on 10th pod –Wound Healthy
Power in lower limbs improved by 20%
Discharged on 10th Day, Hb- 11.7

Summary
25 yr old primi presented with gradual onset, slowly
worsening symptoms of LBA and paraparesis with
patchy sensory involvement, few UMN signs, no
bowel/bladder or cranial nerve involvement; MRI
concluded extramedullary, intradural tumor,
resected at LSCS, HPE confirmed meningioma; post
op gradual recovery in progress

Spinal Cord Tumors
Extradural
Secondary carcinomaPrimary sarcomaReticulosisChordomaNeurinomaMeningioma
Extramedullary NeurinomaMeningiomaEpidermoid
Intramedullary EpendymomaAstrocytomaAngioma
Intradural

Meninges of the Spinal Cord

Meninges of the spinal cord

Spinal Meningioma
Peak age: 40- 70YR
Female:Male= 4: 1
Intradural- 90%
Extradural- 5%
Both- 5%
Less Frequent compared to intracranial(7-12% of all Meningioma)
Multiple meningioma-Rare
Thoracic 82 %
Cervical 15 %
Lumbar 3 %
Lateral 68%
Posterior 18%
Anterior 15%

Genetic Component
Complete / Partial Loss of Chr 22
Abnormality - Cancer related
gene1p,9q,10q,17q
? Dependence on Sex Hormone

M/C Symptoms
@compression
/onset@surgery
Local /Radicular Pain 42 % 53%
Motor deficit 33 % 92%
Sensory deficit 25 % 61%
Sphincter disturbances 50%

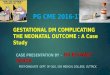
An intradural enhancing meningioma , the ventrally located tumor has produced cord compression and with displacement of the thoracic cord to the right side. Calcified nature of the tumor is identified on sagittal
T2 wtd. image as an area of dark signal intensity (yellow arrow in B) and confirmed by CT imaging as an area of high attenuation density.

Treatment
Rx: resection by safest route
Total resection including
dural attachment and/or
cauterization of the
adjacent dura
Subtotal resection has much
higher risk of recurrence
Deficits often dramatically
reversible

Meningioma
Nest of tumor cells
Abundant cytoplasm
Bland oval nuclei
Occasional
Psammoma bodies

Subacute Combined Degeneration of Spinal Cord
Causes of B12 deficiency
– GI malabsorption
• pernicious anemia (lack of intrinsic factor)
• post-gastrectomy
• Crohn disease
• Celiac disease
– Nutritional – Vegetarian

SACD : Pathophysiology
B12 Deficiency
– Accumulated methylmalonic acid cause
myelin toxicity
– Upregulation of tumor necrosis factor and
downregulation of epidermal growth factor
Nitrous oxide
Susceptible patients, B12 is inactivated

SACD: Pathology
Loss of myelin in the spinal cord white matter
tracts:
– Dorsal columns ( vibration,jt position,fine
touch)
– Lateral columns( pain,temperature)
– Ventral columns(pressure,crude touch)

SACD: Clinical Findings
Insidious subacute onset
– parasthesias, sensory ataxia, hyperreflexia,
and + Babinski
Severe disability in weeks to months
Symmetric;progresses distal to proximal
INV: Megaloblastic anemia; low B12

SACD : Imaging Findings
MRI: high T2 signal intensity involving the
cervical and/or thoracic spinal cord
– Dorsal, lateral and ventral white matter
Cord diameter-normal
No Gd enhancement

SACD: Imaging Findings

SACD: Treatment
B12 supplementation
Cannot recover lost axons
Avoid nitrous oxide anesthesia

Muscular Dystrophy
Group of genetic disorders
Characterized by progressive loss of muscle
integrity; wasting; weakness
Degeneration and regeneration of muscle fibers
(in contrast with static or structural
myopathies)

Muscular Dystrophy- Association
Covers all muscular dystrophies and
myopathies
Multisystem diseases : ALS or Friedreich’s
Ataxia

Dystrophinopathy
Disorders involving dystrophin
Dystrophin: large gene on the X-chromosome
– ubiquitous in the human body
Two most common and severe dystrophy
Duchenne MD and Becker MD

Duchenne’s Muscular Dystrophy
X-linked recessive disorder
Deficiency of protein dystrophin in muscles
Symptoms start in childhood
Become severe in adolescence
Death occurs by age 20 years

Becker Muscular Dystrophy
Same gene affected as Duchenne MD
Disorder of function or decreased amount of
dystrophin rather than absence of the protein
Slowly progressive form
Muscle biopsy, immunostaining for dystrophin:
patchy staining

Myotonic Muscular Dystrophy (Steinert’s disease)
Presentation: adult; multi-system involvt
Primarily distal and facial weakness
Facial features
– frontal balding in men, ptosis, low-set ears,
dysarthria, swan neck,
Myotonia: worse in cold weather, > 20 yr

Myotonic Muscular Dystrophy
Heart: conduction block : Evaluate syncope
Smooth muscle: Constipation, problems with childbirth,
BP lability
Brain: Learning disabilities
Ophthalmology: Cataracts
Endocrine: Insulin resistance, hypothyroidism, testicular
atrophy