Embed Size (px)
Citation preview

Case Report
Case of extreme growth deceleration after burns
Cheryl Bline a, Maggie L. Dylewski b, Daniel N. Driscoll c,Gennadiy Fuzaylov d,*aDepartment of Anesthesia, Critical Care and Pain Medicine, Massachusetts General Hospital, Boston, MA 012114,
United Statesb Shriners Hospital for Children, Boston, MA 02114, United StatescHarvard Medical School, Massachusetts General Hospital, Boston, MA 012114, United StatesdHarvard Medical School, Department Anesthesia, Critical Care and Pain Medicine, Massachusetts General Hospital,
55 Fruit Street, Gray/Jackson 409, Boston, MA 012114, United States
b u r n s 4 0 ( 2 0 1 4 ) e 1 5 – e 1 7
a r t i c l e i n f o
Article history:
Accepted 23 September 2013
Keywords:
Growth deceleration
Burns
Abuse
a b s t r a c t
Studies have demonstrated deceleration in both weight and height following burns in
children. It is expected patients will display catch up growth and return to normal weight
within three years but continued height deficiency may remain in cases of severe burns.
We describe a case of severe growth retardation of 8 years old orphan child from Ukraine
who suffered of burn less than 40% of total body surface area when he was a 3 years of life.
His case was complicated by domestic abuse, neglect and limited medical care. He initially
presented to the United States for surgical care of his contractures but his treatment quickly
focused on his profound growth retardation. Despite aggressive nutritional supplementa-
tion and evaluation he did not demonstrate any weight gain.
Published by Elsevier Ltd and ISBI
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: www.elsevier.com/locate/burns
1. Introduction
Significant hypermetabolic injuries that occur during child-
hood can have significant effect on growth deceleration [1,2].
One example of a hypermetabolic injury is a burn. While
treatments may vary between locations, there is no difference
in the degree of metabolic alteration in patients who have
early excision and grafting of affected areas compared to
patients who have conservative therapy with the application
of antimicrobial ointments initially [3]. Studies have demon-
strated an initial deceleration in both height and weight with
burns [1,2,4]. Growth deceleration is more pronounced in
patients with severe burns and catch up growth has been
displayed in both height and weight regardless of burn
severity [1,2]. Weight returns to normal within 3 years
* Corresponding author. Tel.: +1 617 643 3416; fax: +1 617 726 9697.E-mail addresses: [email protected], [email protected]
Abbreviation: HIV, human immunodeficiency virus.0305-4179/$36.00. Published by Elsevier Ltd and ISBIhttp://dx.doi.org/10.1016/j.burns.2013.09.013
post-burn but continued deficiency in height may remain in
patients with severe burn [2]. Patients with severe burns can
develop vitamin D deficiency that will result in decreased bone
mineral density and may affect bone growth [2,5]. Various
treatments have been suggested including vitamin D supple-
mentation, recombinant growth hormone and oxandrolone
[5–7]. Available studies evaluate patients who are in proximity
to their burn and who have received initial care in the United
States. We explore a case of a young Ukrainian male orphan
who is remote from his initial injury.
2. Case description
This report describes the medical course of an 8-year-old boy
who was brought to the United States from Ukraine for
(G. Fuzaylov).

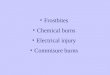
Fig. 1 – Photo before (Panel A) and after (Panel B) treatment.
Table 1 – Longitudinal calorie, weight, and pre-albumindata.
Calorie intakekcal/day (kcal/kg)
Weight kg(z-score)
Pre-albumin(mg/dL)
Admission – 13.0 (�8.1) 12
1 month 2079 (160)* 13.6 (�7.6) 19
2 month 1944 (150)* 13.3 (�8.0)
3 month 1900 (146)** 13.8 (�7.4)
4 month 2100 (162)** 13.4 (�8.0)
b u r n s 4 0 ( 2 0 1 4 ) e 1 5 – e 1 7e16
evaluation of severe burn contractures. Although his past
medical history is vague, between the ages of 2–3 years, this
patient suffered a flame burn to his face, chest, trunk, and
partial extremities while living at home with his biological
parents. It is estimated that the original burn covered less than
40% of his total body surface area was primarily full thickness.
Reports from social services in Ukraine, as well as dialog from
the patient suggest that his parents neglected his acute injury
and he endured domestic physical and emotional abuse. The
patient was eventually intercepted by Social Services and
placed in an orphanage.
Approximately five years after his burn and one year after
his placement in the orphanage, he was brought to the United
States for treatment at a pediatric burn hospital. His primary
diagnoses included burn scar contractures and malnutrition
(Fig. 1). The right elbow and bilateral knees were severely
contracted and the left arm was adhered to his chest and
abdomen. He was wasted, stunted and non-weight bearing.
An oral examination revealed multiple dental carries of the
primary teeth with visible odontogenic infections. Outside of
his physical, nutritional limitations, remaining components of
the physical exam were unremarkable.
Admission weight (13 kg), height (109 cm) and BMI (10.9)
were below the 5th percentile on the Center for Disease
Control age specific growth charts. Bone density, assessed
using dual energy X-ray absorptiometry indicated severe
osteopenia at the lumbar spine (z-score = �3.2). The prealbu-
min level (12 mg/dL) was also depressed. Complete blood
count, electrolytes and liver function tests were all within
normal limits. He tested negative for HIV and intestinal
parasite.
The child’s significant malnutrition delayed surgical
reconstruction until nutritional status was restored. An
aggressive treatment plan, consisting of oral intake coupled
with enteral nutrition support via a nasogastric feeding tube
was devised.
Protein and energy goals were titrated to support weight
gain and restore visceral proteins. Initially protein require-
ments were estimated to be 2–3 g/kg and the caloric goal was
1400 kcal per day, calculated using the dietary reference intake
value plus an additional 500 kcal. Multivitamin, calcium,
vitamin D and an anabolic steroid supplements were also
provided.
The patient tolerated enteral tube feedings and an oral diet.
Total caloric intake exceeded the initial goal by 35–50%
throughout admission (Table 1).
Visceral protein status normalized after 1 month of
aggressive nutrition support (Table 1). However, despite
aggressive nutrition therapy, significant weight gain was
never achieved (Table 1).
Surgical treatment, which consisted of releasing his left
arm from his chest, release of contractures in his other
extremities and skin grafting of open areas, was completed
without complications. He received daily physical therapy for
assistance with range of motion in all four extremities and
weight bearing activities. After 60 days, he was discharged
from the hospital.
As an outpatient, he continued aggressive physical and
nutritional therapy. He also received dental rehabilitation that
included of the removal of the infected primary teeth. Dietary
analyses revealed that his caloric intake was maintained at
approximately 1900–2100 kcal per day (Table 1). Celiac disease,
other intestinal malabsorption disorders, and hyperthyroid-
ism were all ruled out. Despite sustained and substantial
caloric intake and no clear evidence of a malabsorption
disorder, the patient failed to gain weight.
3. Discussion
The bodies of literature that discuss growth deceleration
and burns specifically discuss cases in which the children
are treated for acute burns with follow-up for several years
[1–4]. This is a unique case in which the child did not
present for aggressive treatment for several years after his
burn. Studies have yet to be completed to examine if there is
a time frame in which a child may be able to display catch
up growth. It is possible that the severity of this child’s
nutritional deficit and the duration of the deficit may have
long-lasting repercussions on his ability to achieve a normal
weight.
The ability to bear weight has also been important. Studies
have demonstrated reduction in linear growth in all burns
with a return toward normal once activity is resumed [2].
Demineralization has been demonstrated and can affect the
integrity of the child’s long bones. The severity of this patient’s
contractures, particularly in his lower extremities, prevented
weight-bearing activity. His total body surface area of his burn
did not fall in the category of a severe burn but several years of

b u r n s 4 0 ( 2 0 1 4 ) e 1 5 – e 1 7 e17
limited weight bearing may have resulted in permanent linear
growth retardation. His ability to regain length now that he is
participating in physical therapy with weight bearing will be
determined over the following years, but if his failure to gain
weight is any indication, he likely will have long-lasting height
deficiency.
Another factor that may have contributed to this child’s
dramatic growth deceleration is his social situation. Children
from abused and neglected households without serious illness
or injury can display growth delay [8]. The combination of
growth deceleration from years of abuse and neglect com-
bined with serious injury may have combined in this case.
In conclusion, it is expected that children with burns will
have a deceleration in height and weight growth with most
demonstrating catch up growth. It is uncommon for children
to present remote from their initial injury, but this could have
long-lasting effects on the ability to regain lost height and
weight despite aggressive nutrition supplementation and
physical therapy.
Funding source
No funding was received for this project.
Financial disclosure
Authors have no financial relationships relevant to this article
to disclose.
Conflict of interest
The authors declare that they have no conflict of interest.
r e f e r e n c e s
[1] Rutan RL, Herndon DN. Growth delay in postburn pediatricpatient. Arch Surg 1990;125:392–5.
[2] Prelack K, Dwyer J, Dallal G, Rand WM, Yu YM, Kehayias JJ,et al. Growth deceleration and restoration after serious burninjury. J Burn Care Res 2007;28:262–8.
[3] Rutan TC, Herndon DN, Van Osten T, Abston S. Metabolicrate alterations in early excision and grafting versusconservative treatment. J Trauma 1986;26:140–2.
[4] Childs C, Hall T, Davenport PJ, Little RA. Dietary intake andchanges in body weight in burned children. Burns1990;16(6):418–22.
[5] Klein GL, Langman CB, Herndon DN. Vitamin D depletionfollowing burn injury in children: a possible factor in post-burn osteopenia. J Trauma 2002;52:346–50.
[6] Aili Low JF, Barrow RE, Mittendorfer B, Jeschke MG, ChinkesDL, Herndon DN. The effect of short-term growth hormonetreatment on growth and energy expenditure in burnedchildren. Burns 2001;27:447–52.
[7] Murphy KD, Thomas S, Mlcak RP, Chinkes DL, Klein GL,Herndon DN. Effects of long-term oxandroloneadministration in severely burned children. Surgery2004;136:219–24.
[8] Olivan G. Catch-up growth assessment in long-termphysically neglected and emotionally abused preschool agemale children. Child Abuse Neglect 2003;27:103–8.