Embed Size (px)
Citation preview

Thorax (1956), 11, 36.
A CASE OF BRONCHIAL ADENOMA WITH LIVERMETASTASIS
BY
PRISCILLA KINCAID-SMITH AND JEAN-JACQUES BROSSY
From the Departments of Pathology and Surgery, Hammersmith Hospital (Postgraduate Medical School ofLondon)
(RECEIVED FOR PUBLICATION AUGUST 19, 1955)
Distant metastases from bronchial " adenomas "are sufficiently uncommon to warrant reporting apatient in whom a liver metastasis after apparentlysuccessful treatment of a bronchial adenomacaused diagnostic difficulties.
CASE REPORTA shorthand-typist, then aged 58, was first seen in
February, 1948, complaining that three months pre-viously she had caught a cold which had "gone intoher chest" and persisted, with the development of acough productive of sputum which had latterly beenblood-streaked.
Clinical examination suggested some collapse at theright lung base, and radiography of the chest confirmedthat this involved mainly the middle lobe. Atbronchoscopy a large polypoid tumour was found inthe right main bronchus, just above the middle lobarand apical lower segmental orifices. A biopsy speci-men was reported as bronchial adenoma. A rightmiddle and lower lobectomy was performed (March,1948). Convalescence after this operation was smooth.At a routine follow-up visit in September, 1954, the
patient reported having had intermittent diarrhoea for10 weeks, the stools being watery, without blood orslime. She had also suffered flatulence associated withcolicky rumblings in the upper abdomen. There wasno history of dyspepsia, pain, or weight loss.
Palpation of the abdomen showed a mobile, smooth,rounded tumour about 10 cm. in diameter projectingfrom under the left costal margin near the midline.It moved freely on respiration and could be pushedfrom side to side of the abdomen. There was no asso-ciated tenderness or pain.A few rales were audible over the right lung, and
the trachea was slightly displaced to the right, but airentry on both sides of the chest was good and radio-graphy confirmed the absence of gross disease in thechest.A barium meal and enema showed that the stomach
and colon were displaced by but not attached to themass, which appeared to be in a more posterior plane.An intravenous pyelogram showed that the left kidneywas displaced downwards, but the caliceal pattern wasnormal.
Our presumptive pre-operative diagnosis was of apancreatic cyst, but at laparotomy (through a leftupper paramedian incision) a cystic mass was found,10 cm. in diameter, in the lower edge of the left lobeof the liver. This was thought to be a simple cystof the liver, and easily excised with a thin rim of livertissue. There were no other tumours in the liver, andthe stomach, transverse colon, and gall bladderappeared normal. The hepato-gastric omentum wasabnormally large and lax. This and the unusualmobility of the tumour clearly enabled it to projectbehind the stomach and give the radiological appear-ance of a retroperitoneal mass.The patient was fit and well when last seen in March,
1955, aged 65.
MORBID ANATOMYBRONCHIAL ADENOMA.-This was excised in 1948.
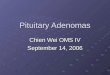
The right middle lobe bronchus forked into medialand lateral branches 15 mm. below its origin. Themain tumour mass was in the medial branch of themiddle lobe bronchus. It measured 11 mm. in dia-,meter and extended over a length of approximately35 mm. Tumour was also present in the lumen ofthe main middle lobe bronchus and its lateral branch.The main tumour mass had invaded the surroundinglung through the wall of the bronchus, and extendedalong the branches of the medial bronchus. The wholemiddle lobe was collapsed. The tumour tissue wassoft, friable, and homogeneous. It was buff-colouredand showed no macroscopic haemorrhage or necrosis.
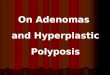
Histology.-The tumour (Fig. 2) consisted of uni-form polyhedral cells 15-20 It in diameter withgranular pale eosinophilic cytoplasm and oval orspherical vesicular nuclei. Very occasional mitoseswere observed.The arrangement of cells in most areas was into
small regular groups 20-50 cells across. These wereseparated by a delicate stroma rich in vascular chan-nels. In other areas sheets and columns of cellswere less regularly permeated by a similar delicatevascular stroma. Within a bronchial lumen in onearea there was a definite papillary pattern.From the tumour in the medial branch of the middle
lobe bronchus the surrounding lung was extensively
copyright. on D
ecember 24, 2020 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.11.1.36 on 1 M
arch 1956. Dow
nloaded from

invaded. Active destruction of cartilage and invasionof lymphatics was observed. In addition distantbronchioles and alveoli contained small groups ofliving tumour cells quite separate from the maintumour. A diagnosis of carcinoid type of bronchialadenoma was made.
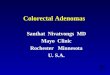
THE LIVER TUMOUR.-This was excised in 1954. Ex-ternally this was a smooth oval apparently cystic mass(Fig. 3) measuring 111 x 100 x 65 mm. and weighing500 g. The upper half of the tumour was covered bya 2-3 mm. shell of liver tissue. The lower surfaceshowed "sugar-icing" thickening of the peritoneum.On section a fibrous capsule 0.5-1 mm. thick sur-
rounded the tumour. In the fresh state the latter wasextraordinarily soft, resembling semi-solid gelatine. Ithad a spongy appearance due to the presence of abun-dant large and small haemorrhagic areas. The tumourtissue was buff coloured. No areas of necrosis werepresent.
Histology.-The microscopical appearance (Fig. 4)was very similar to that of the primary bronchialadenoma removed six years previously. In the solidareas the cells were uniformly arranged in small groupsseparated by delicate vascular stroma. In other areaslarge irregular cystic spaces containing blood or lymphseparated the cell groups.The tumour cells were of the same uniform poly-
hedral type described above. The only significantdifference was the relative frequency of mitoses whichwere approximately one per high power field (0.05sq. mm.). The dense collagenous capsule was invaded
I w I
0 cM.
.4
MIDDLE LOBEBRONCHUS
LATERALSEGMENT
5
MEDIALSEGMENINVADEDBYTUMOUR
FIG. 1.-Photograph of right middle lobe in section.
FIG. 2.-Photomicrograph obronchial adenoma showingtumour growth in the lumenof a bronchus and in thesurrounding lung paren-chyma ( x 90).
w - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - wcopyright.
on Decem
ber 24, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.11.1.36 on 1 March 1956. D
ownloaded from

at several points. In addition a few scattered groupsof infiltrating tumour cells were present in the adacentliver tissue outside the capsule.
This tumour was diagnosed as a metastatic depositfrom the carcinoid bronchial adenoma removed sixyears previously.
METHODSSections from both primary and secondary tumour
were stained by the diazo method for argentaffin cellgranules (Pearse, 1953) and by the periodic-acid-Schiffmethod for mucin. Both methods gave negativeresults.
DIscussIoNIn spite of the invasive character and the occur-
rence of local lymph node and distant metastasesin tumours of the type described above, it is gener-ally agreed that there is every justification forplacing them in a separate category from the morecommon bronchial carcinomas. Ah.
The natural history of the so-called "bronchialadenomas" is strikingly different from that ofcarcinomas. The adenomas are most commonin the 30-40 age group (Foster-Carter, 1941;Liebow, 1952) and in the majority the dura-tion of symptoms is as long as five yearsbefore diagnosis (Foster-Carter, 1941). These -features, together with an almost equal sex inci- C m. sdence (Foster-Carter, 1941; Liebow, 1952), slug-gish growth, and rare metastases, contrast stronglvwith those of bronchial carcinoma.
FIG. 3.-Macroscopic appear-XFICm-wJ ance of the liver "cyst"
54 ~ '. i.~~i on section. A small tag4 ~~~~~~~~~~~~~~~~~~~~~~~ofnormal liver tissue is
0% tJ 4% 4 ,4. . seen on the right side.%'.
_~~~~~~~~~~~~~~4 . 4*4
% ' N. , I.4 Poomcorahok ~~ascinfo h ie
,,,-~~~~~~~~~~~~~~~~~~~~U -e tumur Te ppar
JA.P.~~~~~~~~~~~~~~~~~~~~~~~~~acsaetos facri
404W.;? ~ ~ ~ ~ ~ ni tp o umu-4V ~ (x90)
copyright. on D
ecember 24, 2020 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.11.1.36 on 1 M
arch 1956. Dow
nloaded from

BRONCHIAL ADENOMA WITH LIVER METASTASIS
STRUCTURAL TYPES.-The descriptive termscarcinoid and cylindroma have been widely appliedto the two main histological types of bronchialadenoma. Liebow (1952) states that 85% are ofthe carcinoid type and 15% of the cylindroid.The carcinoid type owes its name to the striking
similarity between these tumours and the argentaf-finoma (carcinoid) of the intestine. The descrip-tion given above covers most of the classicalfeatures of this type. The arrangement is notacinar but in groups of cells separated by delicatehighly vascular stroma. A pseudo-acinar picturemay be produced by the survival of a ring of cellsaround a vessel.The choice of the name cylindroma is perhaps
less fortunate than that of carcinoid. The classicalarrangement here is that of branching tubularepithelial structures frequently with a double lining.The rather irregular acini are lined by small,deeply staining cells, more variable in size andshape than in the carcinoid type. Microscopicallythe tumour appears more invasive than the carci-noid, and mucin secretion is frequently seen.
Mitoses are rare in both types but more frequentin the cylindromas. Haemorrhagic areas are morecommon in the carcinoid, and necrosis very rarelyoccurs in either histological type.
In addition to these two main types of bronchialadenoma minor variations in the histological pic-ture may occur. Tumours may be composedalmost entirely of " oncocytes." Like the onco-cytic (Hurthle) thyroid adenomas and salivarytumours the cells in this type have a large amountof opaque eosinophilic cytoplasm and a densenuclear chromatin. Their arrangement is usuallysimilar to that seen in carcinoids, but oncocyticareas may occur in either type. A further varia-tion usually seen in the cylindroma has beencalled muco-epidermoid (Liebow, 1952) because ofthe presence of mixed mucous and squamousareas.NOMENCLATURE AND HISTOGENESIS.-The name
bronchial adenoma is so widely accepted for thisgroup of tumours that we think it should beretained in spite of their malignant potentialities.
Willis (1953) regards bronchial adenomas asanalogous to the pleomorphic (mixed) salivarytumours and considers that they arise from themucous glands of the bronchial wall. He does notsubdivide them into histological types. Womackand Graham (1938) consider them to be tumoursof mixed developmental origin on the basis ofareas of bone cartilage and mucous glands withinthem. Willis (1953) and others (Doty, 1951 ; VanHazel, Holinger, and Jensik, 1949; Moersch, Tin-
ney, and McDonald, 1945) consider that the bonearises from stromal metaplasia and the cartilageand glands from invasion of bronchial wall struc-tures. Womack and Graham (1938) group allbronchial adenomas together as mixed tumours oflung. Holley (1946), Goldman (1949), and Doty(1951) have all used the term " mixed tumour " forthe non-carcinoid (cylindroma) group of bronchialadenomas. Van Hazel and others (1949) use thename "adenoma" for the carcinoid type aloneand cylindroma for the residue.
Because of this confusion in nomenclature itseems to us desirable to employ a purely descrip-tive classification such as that of Liebow (1952).He divides bronchial adenomas into the twocharacteristic patterns carcinoid and cylindroid(cylindroma), and recognizes the occurrence ofoncocytoid and muco-epidermoid variants withinthese two groups. This avoids the use of theterms " mixed tumour " and " adenoma " to whichdifferent meanings have been applied by differentauthors.
BEHAVIOUR OF DIFFERENT TYPEs.-The justifica-tion for subdividing bronchial adenomas dependson the differences in behaviour and thus in prog-nosis in the two types. It appears that the dataat present available are insufficient for an accurateassessment of the liability of the types of bronchialadenoma to invade and metastasize (Liebow, 1952).It will be difficult to obtain this information untila standard nomenclature is adopted.As recently as 1941 Foster-Carter stated that
distant metastases from these tumours were un-known. To-day, however, their occurrence is wellrecognized (Mallory, 1938; Adams, Steiner, andBloch, 1942; Anderson, 1943; Laff and Neu-buerger, 1944; Holley, 1946; Van Hazel andothers, 1949; Liebow, 1952). Locally the cylin-droma shows a more invasive microscopic picturethan the carcinoid, more frequently invading carti-lage and vessels (Liebow, 1952). Several authorsregard cylindromas as probably more malignantthan carcinoids (Laff and Neubuerger, 1944; VanHazel and others, 1949; Goldman, 1949). It isworthy of note that few distant metastases fromcylindromas have been reported (Van Hazel andothers, 1949; Liebow, 1952). In most reportedcases of haematogenous spread the tumour hasbeen of the carcinoid type. This apparent discrep-ancy may be due to the relative infrequency ofcylindromas, which constitute only some 15% of allbronchial adenomas (Liebow, 1952).The tumour in our case clearly falls within the
carcinoid group. We were unable to demonstrate
39
copyright. on D
ecember 24, 2020 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.11.1.36 on 1 M
arch 1956. Dow
nloaded from

PRISCILLA KINCAID-SMITH atd JEAN-JACQLIES BROSSY
argentaffin granLules in the tumour. These were
reported in one case by Holley (1946).In 1943 Anderson reported the first macroscopic
metastasis from a bronchial adenoma. This was
a 2 cm. nodule in the liver, and no other metastaseswere found at the necropsy. Several other authorshave reported liver metastases (Adams and others,1942; Laff and Neubuerger, 1944; Holley, 1946:Graham, 1949). Gordon (1949) had a case very
similar to ours in which a tumour removed fromthe left lobe of the liver was found to be identicalwith a bronchial adenoma removed previously.The time interval is not stated.
In oLir case six and a half years elapsed betweenlobectomy for the bronchial adenoma and thesymptoms which led to the discovery of an
abdominal tumotir. The metastatic deposit was
histologically very similar to the bronchial tumour.The length of history and well-formed capsulearound the liver tumour indicate that growth was
very slow. At the time of removal, however,mitoses were undoubtedly more numerous in themetastasis than in the primary tumour. This is ofinterest in view of reports of the progression ofbronchial adenomas to frank carcinomas (Bigger,1945; Alexander, 1945: Cheek and Muirhead,1948: Goldman, 1949: Abbott, 1949; Umiker andStorey, 1952: Price Thomas, 1954). Willis (1953)discusses two cases in which the diagnosis laybetween an adenoma and a carcinoma. lt is pos-
sible that malignant transition 'may account inpart for the rarity of necropsy accotunts ofbronchial adenoma in the days before broncho-scopy became a routine method of investigation.
SUMMARYA case of adenoma of the bronchus is presented,
in which a metastasis appeared in the liver sixyears after excision of the original tumour bylobectomy. The common origin of both tumoursis demonstrated histologically, and the experiencesof other authors with distant metastases in thesetumours are briefly reviewed. A plea is made forsimplification and standardization of nomenclature.
We thank Mr. W. P. Cleland and Mr. R. H. Franklinfor permission to publish this case. and ProfessorC. V. Harrison for his helpful advice. The histo-logical material was prepared by Mr. J. G. Griffin andphotographed by Miss R. Klein.
REFERENCESAbbott, 0. (1949). J. thtorac. Surg., 18, 156.Adams, W. E.. Steiner, P. E., and Bloch, R. G. (1942). Snrgery,
11. 503.Alexander, J. (1945). J. thorac. Surg.. 14, 122.Anderson, W. M. (1943). Ibid.. 12, 351.Bigger, 1. A. (1945). Ibid., 14. 120.Cheek. J. H., and Muirhead, E. E. (1948). Arch. Palth. (Chli(ago).
46. 529.Doty. R. D. (1951). J. thorac. Sairg., 21. 349.Foster-Carter. A. F. (1941). Quart. J. Ailed.. 10. 139.Goldman. A. (1949). J. thorac. Surg., 18, 137.Gordon, J. (1949). Ibid., 18. 158.Graham, E. (1949). Ibid., 18. 155.Holley, S. W. (1946). Afilit. Strg.. 99. 528.Laff, H. I., and Neubuerger, K. T. (1944). Arch. OtolarYng.
(Chicago), 40, 487.Liebow. A. A. (1952). Tumnors of the Lower Respiratory- Tract.
Atlas of Tumor Pathology. Section V. Fascicle 17. ArmedForces Institute of Pathology. Washington.
Mallory, T. B. (1938). New Engl. J. Mled., 218. 391.Moersch. H. J., Tinney, W. S., and McDonald, J. R. (1945). Siarg.
Gynec. Obstet., 81. 551.Pearse, A. G. E. (1953). Histocheiristry. Theoretical a(nd Appiied.
p. 477. Churchill, London.Thomas. C. P. (1954). Lancer. 1. 1.Umiker, W., and Storey, C. F. (1952). J. thorac. Stirg.. 24. 420.Van Hazel. W.. Holinger, P. H., and Jensik, R. J. (1949). gDis.
ChJest. 16. 146.Willis. R. A. (1953). Pathology of T..no0rs, 2nd ed. Butterworth.
London.Womack. N. A.. and Graham. E. A. (1938). Arch. Path. (Chicago).
26. 165.
40
copyright. on D
ecember 24, 2020 by guest. P
rotected byhttp://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.11.1.36 on 1 M
arch 1956. Dow
nloaded from