Embed Size (px)
Citation preview
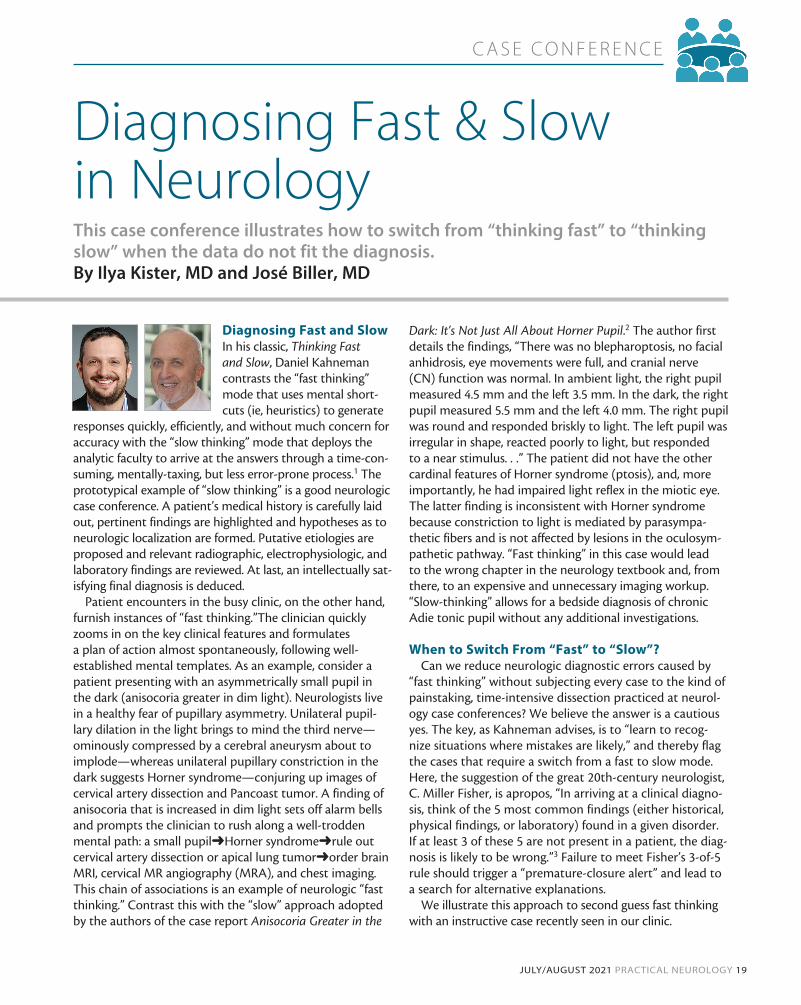
C A S E C O N F E R E N C E
JULY/AUGUST 2021 PRACTICAL NEUROLOGY 19
Diagnosing Fast and Slow In his classic, Thinking Fast and Slow, Daniel Kahneman contrasts the “fast thinking” mode that uses mental short-cuts (ie, heuristics) to generate
responses quickly, efficiently, and without much concern for accuracy with the “slow thinking” mode that deploys the analytic faculty to arrive at the answers through a time-con-suming, mentally-taxing, but less error-prone process.1 The prototypical example of “slow thinking” is a good neurologic case conference. A patient’s medical history is carefully laid out, pertinent findings are highlighted and hypotheses as to neurologic localization are formed. Putative etiologies are proposed and relevant radiographic, electrophysiologic, and laboratory findings are reviewed. At last, an intellectually sat-isfying final diagnosis is deduced.
Patient encounters in the busy clinic, on the other hand, furnish instances of “fast thinking.”The clinician quickly zooms in on the key clinical features and formulates a plan of action almost spontaneously, following well-established mental templates. As an example, consider a patient presenting with an asymmetrically small pupil in the dark (anisocoria greater in dim light). Neurologists live in a healthy fear of pupillary asymmetry. Unilateral pupil-lary dilation in the light brings to mind the third nerve—ominously compressed by a cerebral aneurysm about to implode—whereas unilateral pupillary constriction in the dark suggests Horner syndrome—conjuring up images of cervical artery dissection and Pancoast tumor. A finding of anisocoria that is increased in dim light sets off alarm bells and prompts the clinician to rush along a well-trodden mental path: a small pupil➜Horner syndrome➜rule out cervical artery dissection or apical lung tumor➜order brain MRI, cervical MR angiography (MRA), and chest imaging. This chain of associations is an example of neurologic “fast thinking.” Contrast this with the “slow” approach adopted by the authors of the case report Anisocoria Greater in the
Dark: It’s Not Just All About Horner Pupil.2 The author first details the findings, “There was no blepharoptosis, no facial anhidrosis, eye movements were full, and cranial nerve (CN) function was normal. In ambient light, the right pupil measured 4.5 mm and the left 3.5 mm. In the dark, the right pupil measured 5.5 mm and the left 4.0 mm. The right pupil was round and responded briskly to light. The left pupil was irregular in shape, reacted poorly to light, but responded to a near stimulus. . .” The patient did not have the other cardinal features of Horner syndrome (ptosis), and, more importantly, he had impaired light reflex in the miotic eye. The latter finding is inconsistent with Horner syndrome because constriction to light is mediated by parasympa-thetic fibers and is not affected by lesions in the oculosym-pathetic pathway. “Fast thinking” in this case would lead to the wrong chapter in the neurology textbook and, from there, to an expensive and unnecessary imaging workup. “Slow-thinking” allows for a bedside diagnosis of chronic Adie tonic pupil without any additional investigations.
When to Switch From “Fast” to “Slow”?Can we reduce neurologic diagnostic errors caused by
“fast thinking” without subjecting every case to the kind of painstaking, time-intensive dissection practiced at neurol-ogy case conferences? We believe the answer is a cautious yes. The key, as Kahneman advises, is to “learn to recog-nize situations where mistakes are likely,” and thereby flag the cases that require a switch from a fast to slow mode. Here, the suggestion of the great 20th-century neurologist, C. Miller Fisher, is apropos, “In arriving at a clinical diagno-sis, think of the 5 most common findings (either historical, physical findings, or laboratory) found in a given disorder. If at least 3 of these 5 are not present in a patient, the diag-nosis is likely to be wrong.”3 Failure to meet Fisher’s 3-of-5 rule should trigger a “premature-closure alert” and lead to a search for alternative explanations.
We illustrate this approach to second guess fast thinking with an instructive case recently seen in our clinic.
Diagnosing Fast & Slow in NeurologyThis case conference illustrates how to switch from “thinking fast” to “thinking slow” when the data do not fit the diagnosis.By Ilya Kister, MD and José Biller, MD
C A S E C O N F E R E N C E
20 PRACTICAL NEUROLOGY JULY/AUGUST 2021
Fever, Bilateral Headache, and Jaw Pain
The patient’s clinical history is briefly reviewed here. To hear the patient relate their history, view Video 1 at https://practical-neurology.com/videos/fever-bilateral-headache-and-jaw-pain.
Clinical History and PresentationMr CE is age 52 with a medical history relevant for arterial
hypertension, chronic obstructive pulmonary disease (COPD), obesity, dyslipidemia, obstructive sleep apnea, and cigarette smoking. He developed low-grade fever, pain, and hypersen-sitivity to touch on both temples for several months. He also reported jaw pain, especially on chewing. Mr CE was seen sev-eral times in the emergency department for these symptoms over the course of several months and was repeatedly diag-nosed with acute sinusitis. Antibiotics did not ameliorate his symptoms. After several months, he acutely lost vision in the left eye. At the time of presentation to the neurology clinic, Mr CE’s visual acuity was 20/25 on the left eye and finger counting on the right eye. A right relative afferent pupillary defect (RAPD) was present (Figure 1; Video 2: https://practical-neuro-logy.com/videos/pupillary-examination.)
Diagnostic TestingReview of Mr CE’s laboratory results showed elevated eryth-
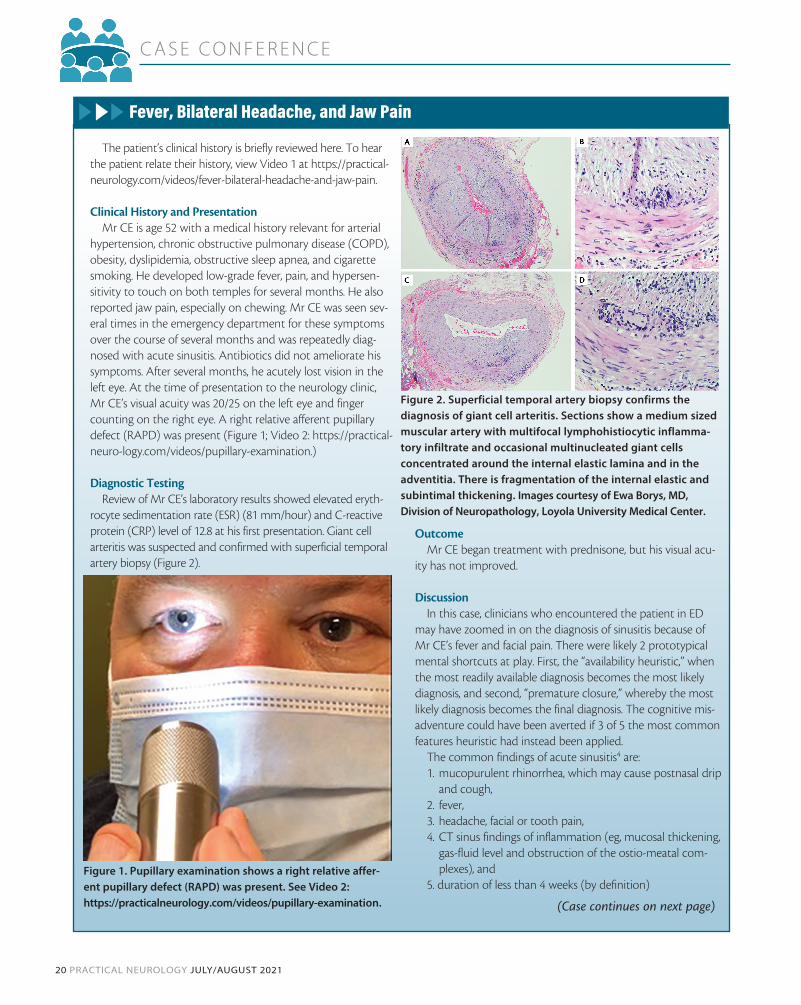
rocyte sedimentation rate (ESR) (81 mm/hour) and C-reactive protein (CRP) level of 12.8 at his first presentation. Giant cell arteritis was suspected and confirmed with superficial temporal artery biopsy (Figure 2).
OutcomeMr CE began treatment with prednisone, but his visual acu-
ity has not improved.
DiscussionIn this case, clinicians who encountered the patient in ED
may have zoomed in on the diagnosis of sinusitis because of Mr CE’s fever and facial pain. There were likely 2 prototypical mental shortcuts at play. First, the “availability heuristic,” when the most readily available diagnosis becomes the most likely diagnosis, and second, “premature closure,” whereby the most likely diagnosis becomes the final diagnosis. The cognitive mis-adventure could have been averted if 3 of 5 the most common features heuristic had instead been applied.
The common findings of acute sinusitis4 are: 1. mucopurulent rhinorrhea, which may cause postnasal drip
and cough,2. fever,3. headache, facial or tooth pain,4. CT sinus findings of inflammation (eg, mucosal thickening,
gas-fluid level and obstruction of the ostio-meatal com-plexes), and
5. duration of less than 4 weeks (by definition)
(Case continues on next page)
Figure 1. Pupillary examination shows a right relative affer-ent pupillary defect (RAPD) was present. See Video 2: https://practicalneurology.com/videos/pupillary-examination.
Figure 2. Superficial temporal artery biopsy confirms thediagnosis of giant cell arteritis. Sections show a medium sizedmuscular artery with multifocal lymphohistiocytic inflamma-tory infiltrate and occasional multinucleated giant cellsconcentrated around the internal elastic lamina and in theadventitia. There is fragmentation of the internal elastic andsubintimal thickening. Images courtesy of Ewa Borys, MD, Division of Neuropathology, Loyola University Medical Center.

C A S E C O N F E R E N C E
JULY/AUGUST 2021 PRACTICAL NEUROLOGY 21
Putting Fisher’s 3-of-5 Rule into PracticeTo make this approach practical for the fast-paced clini-
cal setting we have compiled the 5 most common findings for 100 of the most common and important diagnoses in neurology in the book Top 100 Diagnoses in Neurology: Core Features, Synopses, Illustrations and Questions for Rapid Review and Retention.5 This compilation allows clinicians to quickly cross-check the findings of a particular case against the most common features of the suspected neurologic
diagnosis and see if Fisher’s 3-of-5 rule is satisfied. In the forthcoming columns, we hope to demonstrate the utility of this approach using illustrative cases from our practice. n
1. Kahneman, D. Thinking, Fast and Slow. Farrar, Straus and Giroux; 1st edition:2011.2. Witsberger E, Mansukhani SA, Chen JJ, Bhatti MT. Pearls & Oy-sters: Anisocoria Greater in the Dark: It’s Not Just All
About Horner Pupil. Neurology. 2021;96(15):719-722.3. Caplan LR. Fisher’s rules. Arch Neurol. 1982;39(7):389-390.4. Evans KL. Diagnosis and management of sinusitis. BMJ. 1994;309(6966):1415-1422.5. Kister I, Biller J. Top 100 Diagnoses in Neurology: Core Features, Synopses, Illustrations and Questions for Rapid Review and
Retention. Wolters Kluwer:2021.
Ilya Kister, MDNew York UniversityLangone Medical CenterDepartment of NeurologyNew York, NY
José Biller, MDChair, Department of Neurology Loyola University ChicagoStritch School of Medicine Loyola University Medical Center Maywood, IL
DisclosuresJB reports no disclosure IK has disclosures at practicalneurology.com
Case Report (continued)
Comparison of these cardinal features with Mr CE’s presenta-tion shows that, at most, 2 of 5 features were present: fever and facial pain, although localization of head pain to the temporal region would be quite unusual for sinusitis. The absence of nasal discharge or cough would also be highly uncharacteristic of sinus-itis, as is the presence of jaw pain on chewing, or jaw claudication, which may have been confused with tooth pain. Finally, symp-tom duration of months is inconsistent with acute sinusitis. This analysis shows acute sinusitis to be a highly unlikely diagnostic possibility. Alternative diagnoses should be sought after. If none are forthcoming, it would be wise to avoid affixing any diagnostic labels and refer this patient with temporal pain and fever for additional consultations and specialized investigations.