Embed Size (px)
Citation preview

CASE Approach to Patients with Prolonged Fever
Sirichai Wiwatrojanagul, M.D., M.Sc.
Division of Infectious Disease
Department of Medicine
Maharat Nakhon Ratchasima Hospital

Approach to fever
• History • Age
• Occupation
• Place of origin, Travel history
• Consumption of unpasteurized dairy products
• STI risk
• Family history
• Contact pulmonary tuberculosis
• Family members has an illness
• Drugs • Immunosuppressive drugs
• Previous antibiotics
• Host (underlying disease)• Immunodeficiency
• Post splenectomy
• Diabetes mellitus
• Cirrhosis
• CKD
• ...

Approach to fever
Onset of Fever
Week 0 1 2 3 4
Acute Fever
Prolonged fever
Prolonged fever
Classic FUO
Visit
VisitVisit
Visit
Visit +investigation VisitVisit +/-investigation

How to differentiate the cause of fever in clinical practice
• Clinical Presentation
• Host
• Exposure / Epidemiology

Clinical Presentation
• Fever with specific organ/system involvement
• Fever with multi-organs/system involvement
• Fever without specific organ/system involvement
• Typical manifestation of a common disease
• Atypical manifestation of a common disease
• Typical manifestation of a uncommon disease
• Atypical manifestation of a uncommon disease

Host
• Infection in the Elderly (>65 year)
• Infection in Neutropenia
• Infection in Cirrhosis
• Infection in Diabetes Mellitus
• Infection in Thalassemia patients
• Infection in SLE, RA
• Infection in Transplant recipients
• Fever in the returned traveler
• Fever of unknown origin

Host
• Steroid: CMI deficiency and Phagocytic dysfunction• CMI deficiency -> Listeria monocytogenes, Nocardia spp, TB/NTM, Mould,
dimorphic fungi, C. neoforman, toxoplasma gondii
• Phagocytic dysfunction -> S. aureus, P. aeruginosa, zygomycetes
• DM: Phagocytic dysfunction • Phagocytic dysfunction -> S. aureus, P. aeruginosa, zygomycetes
• Iron overload : L. monocytogenes, e.coli, V. vulnificus, A. hydrophila, Y. enterocolitica, zygomycetes
• Splenectomy: Encapsulated -> S. pneumonia, H. influenza, N. menigitidis, C. canimorsus, C.cynodegmi

Exposure / Epidemiology
• Race
• Domicile, Region
• Career
• Hobby
• Immunization
• Travel

No Localizing sign & symptoms
Prolonged FeverLocalizing symptoms▪ CNS ▪ GI ▪ CVS ▪ GU ▪ Skin ▪ LN▪ Respiratory ▪ Bone & joint ▪ Hemato
Laboratory▪ CBC ▪ LFT ▪ Bun/Cr ▪ UA ▪ Hemoculture▪ ESR/CRP
Review history ▪ Occupation/recreation ▪ Habitat ▪ Travel ▪ Animal contact ▪ Contact with ill person ▪ Medications
No diagnosis ! FUO

Prolonged Fever
Localized infections
• CNS -> Meningitis, Brain mass• CVS -> IE, Aortitis/Aneurism• Respi -> Pneumonia, Effusion• GI -> Intraabdominal infection• Bone&Joint -> Spodylodiscitis• Lymphadenopathy• Skin lesion• KUB• Hemato
Non- Localized infections
• Fever of unknown origin• Infection
• Autoimmune
• Tumor
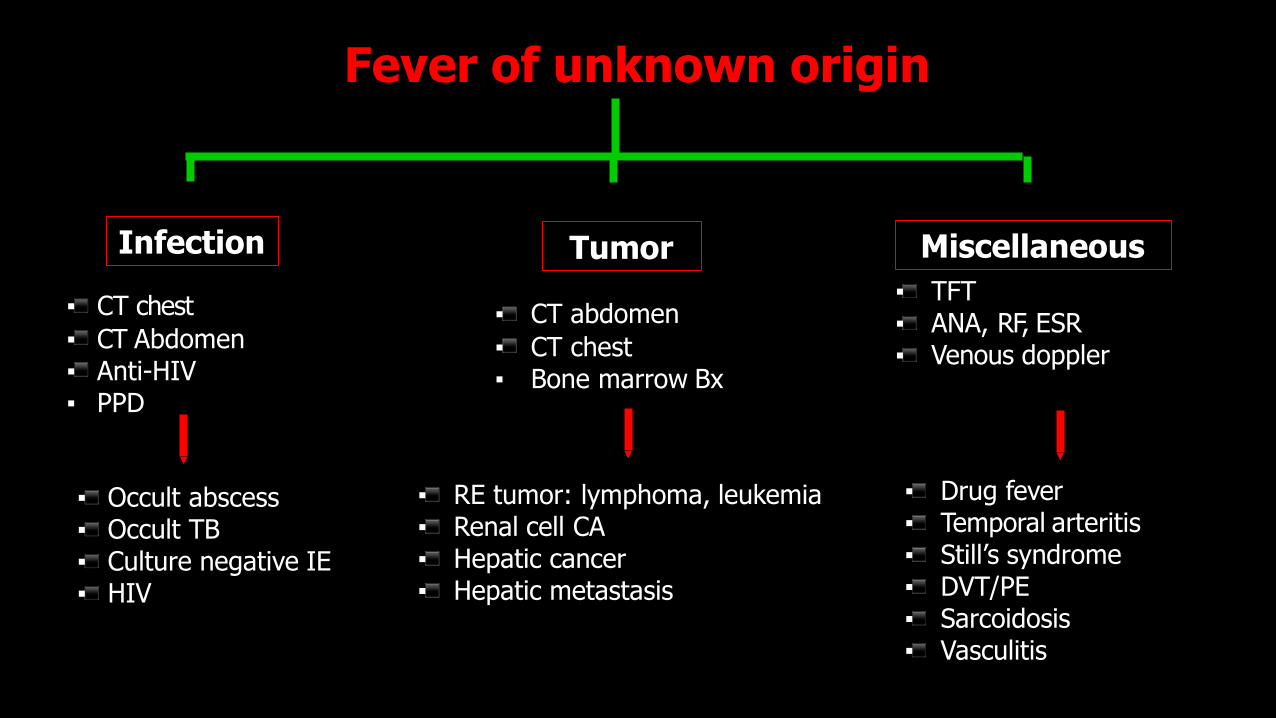
Fever of unknown origin
Infection Tumor Miscellaneous
▪ CT chest
▪ CT Abdomen▪ Anti-HIV▪ PPD
▪ Occult abscess▪ Occult TB▪ Culture negative IE▪ HIV
▪ CT abdomen
▪ CT chest▪ Bone marrow Bx
▪ RE tumor: lymphoma, leukemia▪ Renal cell CA▪ Hepatic cancer▪ Hepatic metastasis
▪ TFT▪ ANA, RF, ESR▪ Venous doppler
▪ Drug fever▪ Temporal arteritis▪ Still’s syndrome▪ DVT/PE▪ Sarcoidosis▪ Vasculitis

Clinical Evaluation of Fever of unknown origin• History :Comprehensive History is cornerstone
• Physical Examination : Repeated PE
• Laboratory Investigation : Noninvasive test ; CBC, UA, chemistry, culture, serology, BM study
• Imaging Studies : U/S, CT scanning
• Invasive Diagnostic Procedures : Histopathology ; excisional biopsy, needle biopsy or laparotomy
• Therapeutic Trials

Classic Nosocomial Neutropenic HIV-related
Definition >38°C 3 wk., > 3 visits or 3 d in hospital (Durack & street 1991)
>38°C, 3 d, not present or incubating on admission
>38oC, 3 days, negative cultures after 48 hrs. with ANC
>38°C,< 3 d for inpatients, outpatient > 4 wk. HIV infection confirmed
Patient location
Community, clinic or hospital
Acute care hospital Hospital or clinic Community, clinic or hospital
Leading causes
Infections, inflammatory conditions, cancer, undiagnosed, habitual hyperthermia
Nosocomial infections, postoperative complications, drug fever C. difficileinfection, thrombophlebitis
Majority due to infections, but cause documented in only 40–60% (Aspergillus spp., Candida spp.)
(HIV primary infection), typical & atypical mycobacteria, CMV, lymphoma, toxoplasmosis, cryptococcosis
History emphasis
Travel, contacts, animal and insect exposure, medications, immunizations, family history, cardiac valve disorder
Operations and procedures, devices, anatomic considerations, drug treatment
Stage of chemotherapy, drugs administered, immunosuppressive disorder, Skin folds, IV sites, lungs, perianal area
Drugs, exposures, risk factors, travel contacts, stage of infection Mouth, sinuses, skin, lymph nodes, eyes, lungs perianal area
Classification of the four subtypes of FUO

CASE1: ชายไทยคู ่อาย ุ47ปี อาชพีคร ูจ.นครราชสมีา
• CC: กอ้นโตขึน้ตามตัว มา 1 เดอืน
4 เดอืนกอ่น สงัเกตวา่มไีขต้ า่ๆ โดยเฉพาะชว่งค า่ ไมม่อีาการผดิปตอิยา่งอืน่รว่มดว้ย
3 เดอืนกอ่น ยังมไีข ้รว่มกับสงัเกตวา่มกีอ้นทีค่อ 2 ขา้งโตมากขึน้ กอ้นแข็ง ไมม่อีาการปวด มเีบือ่อาหารและน ้าหนักลดลง (จาก 86 เหลอื66 กโิลกรัมในชว่ง3เดอืน)ไมม่ไีอเรือ้รัง ไมม่อีาการอืน่ผดิปกติ
2 เดอืนกอ่น ยังคงมไีข ้รว่มกับกอ้นโตเพิม่ขึน้ทีบ่รเิวณขาหนบีทัง้สองขา้ง แข็ง ไมเ่จ็บ กอ้นทีบ่รเิวณคอยังมขีนาดเทา่ๆ เดมิ ผูป่้วยซือ้ยาหมอ้มาตม้กนิอยู ่1 เดอืน สงัเกตวา่กอ้นยบุลงแตไ่มห่มด
1 เดอืนกอ่น ไขส้งูขึน้หลังหยดุยาหมอ้ รว่มกับกอ้นโตมากขึน้ จงึไปพบทีร่พช. และสง่ตัวตอ่มารักษาตอ่ รพ.มหาราช นครราชสมีา

CASE1: ชายไทยคู ่อาย ุ47ปี อาชพีคร ูภมูลิ าเนาจ.นครราชสมีา
Physical examination
• T 38.6 c, BP 116/75 mmHg, HR 120/min, RR 16/min
• GA: Good consciousness, moderately pale, no jaundice, no dyspnea & tachypnea
• HEENT: no thyroid gland enlargement
• CVS & RS: unremarkable
• Abdomen: soft, no distension, no tenderness, no hepatosplenomegaly, no ascites, normal bowel sound
• Nervous system: no neurological deficit
Lymphatic system :
• Cervical-> Bilateral matted LN, the largest node was 5 cm in diameter firm consistency, not tender, movable
• Axillar -> Bilateral multiple matted LN, 3 cm in diameter of 4-5 nodes each side firm consistency, not tender, movable
• Inguinal -> Bilateral multiple matted LN, 3 cm in diameter of 4-5 nodes each sidefirm consistency, not tender, movable

CASE1: ชายไทยคู ่อาย ุ47ปี อาชพีคร ูภมูลิ าเนาจ.นครราชสมีา
Problem List
• Prolonged fever with Generalized lymphadenopathy for 4 months
• Significant weight loss (20 kg in 3 months)
• Anemia
Investigation
• CBC: Hb7.4 g/dL, Hct24.2%, MCV 82 fL, WBC 7,480/mm3(N 75.4%, L 14.3%, M 7.2%, Eo2.8%, B 0.3%), plt424,000/mm3
• Blood chemistry : BUN 12.1mg/dL, Cr 1.0mg/dL,Na 137 mmol/L, K 3.9 mmol/L, Cl95 mmol/L, HCO3 28 mmol/L
• LFT: TB 0.3 mg/dL, DB 0.16 mg/dL, AST 18 U/L, ALT 12 U/L, ALP 240U/L, Albumin 2.5 g/dL, Globulin 6.1 g/dL

Prolonged fever with Generalized lymphadenopathy
Key Factors in Evaluation• Age of patient • Location of lymphadenopathy • Systemic signs/symptoms • Presence/absence of
splenomegaly • Size, consistency, tenderness,
and fixation of LN• History of exposures • Drug history
•Aspirate LN: AFB, mAFB, G/S, Wright, culture
•LN Aspiration, biopsy and culture
Specific treatment
• HIV: -> TB/NTM, Dimorphic fungi, Crypto• Exposure-> Cat-> CSD• Systemic or Autoimmune -> Kikuchi Fujimoto disease• Rash/Arthritis-> Still's disease• IgG4-related disease

Case1: ชายไทยคู ่อาย ุ47ปี อาชพีคร ูภมูลิ าเนาจ.นครราชสมีา
• FNA: AFB+
• PCR: Positive for NTM
• Tissue C/S: M. abscessuscomplex
• H/C for mycobacterium : M. abscessus complex
• Anti-HIV – nonreactive
• Anti IFN Gamma Ab– positive
Adult-onset immunodeficiency with disseminated M. abscessus infection

Mycobacteria
Mycobacterium tuberculosis
complex (MTBC)Non-tuberculous mycobacteria (NTM)
M.tuberculosisM.africanumM.bovisM.canettiM.capraeM.microtiM.pinnipedii
RGMSGMNon-
culturable
M. fortuitum complexM. Chelonae complexM. abscessus complexM. smegmatis complex
M. lepraePhoto-chromo
gen
Scoto-chromo
gen
Non-chromo
gen
M. marinumM. kansasiiM. simiae
M. scrofulaceumM. gordonaeM. szulgai
MACM. haemophilumM. ulcerans

Baldwin SL et al. PLoS Negl Trop Dis. 2019;13(2): e0007083 Retrieved form Facebook : oneslide ID

Macrolide susceptibility pattern Number of drug and Preferred drugs
Mutational# Inducible¶ Initial phase Continuation phase
Susceptible Susceptible ⩾3
Parenteral (choose 1–2)
Amikacin
Imipenem (or Cefoxitin)
Tigecycline
Oral (choose 2)
Azithromycin (clarithromycin)§
Clofazimine
Linezolid
⩾2
Oral/inhaled (choose 2–3)
Azithromycin (clarithromycin)§
Clofazimine
Linezolid
Inhaled amikacin
Susceptible Resistant ⩾4
Parenteral (choose 2-3)
Amikacin
Imipenem (or Cefoxitin)
Tigecycline
Oral (choose 2-3)
Azithromycin (clarithromycin)§
Clofazimine
Linezolid
⩾2
Oral/inhaled (choose 2–3)
Azithromycin (clarithromycin)§
Clofazimine
Linezolid
Inhaled amikacin
Resistant Susceptible
Resistant Resistant
Treatment regimens for Mycobacterium abscessus complex
Daley CL, et al.. Treatment of nontuberculous mycobacterial pulmonary disease: an official ATS/ERS/ESCMID/IDSA clinical practice guideline. Clinical Infectious Diseases.2020 Aug 14;71(4):e1-36.
M. abscessus subsp. massiliense
M. abscessus subsp. abscessusM. abscessus subsp. bolletii
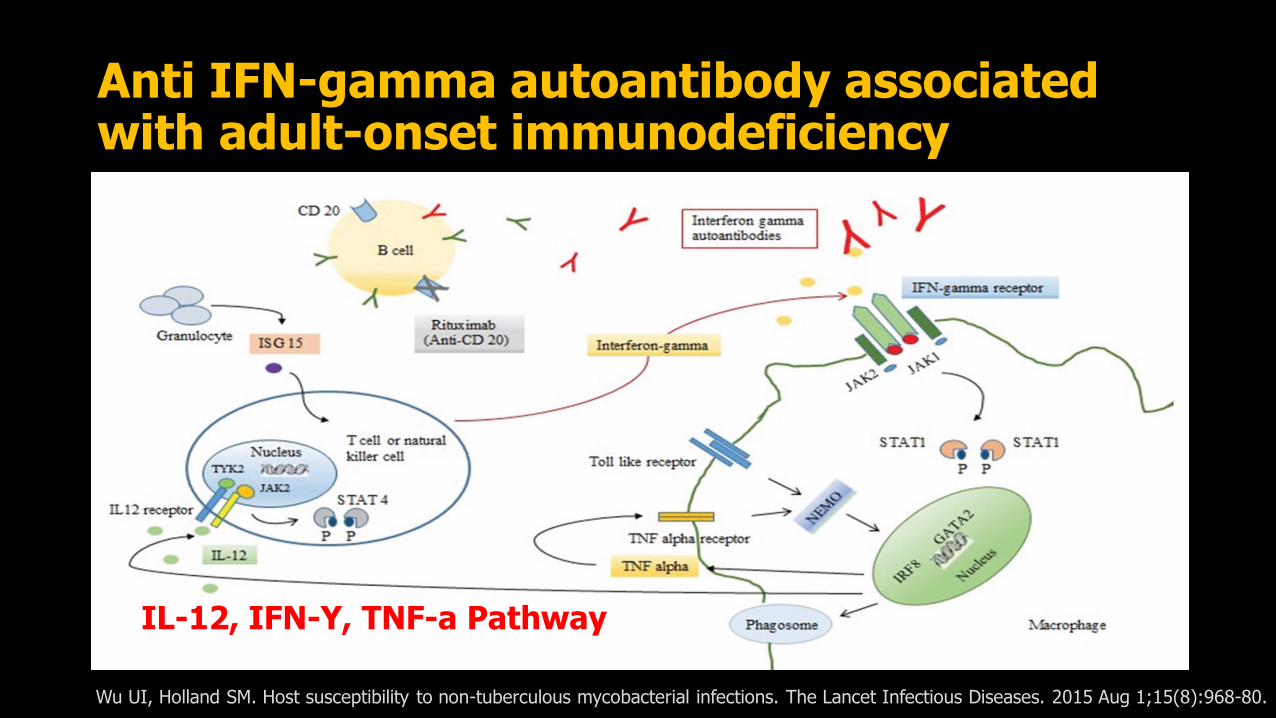
Anti IFN-gamma autoantibody associated with adult-onset immunodeficiency
IL-12, IFN-Y, TNF-a Pathway
Wu UI, Holland SM. Host susceptibility to non-tuberculous mycobacterial infections. The Lancet Infectious Diseases. 2015 Aug 1;15(8):968-80.

Chetchotisakd P, et al. Disseminated nontuberculous mycobacterial infection in patients who are not infected with HIV in Thailand. Clinical infectious diseases. 2007 Aug 15;45(4):421-7.

CASE2: หญิงอาย ุ68ปี อาชีพท านา ภูมิล าเนานครราชสีมา
• CC: ไขม้า 2 เดอืน
2 เดอืน มไีขส้งูๆต า่ๆ ทานพาราเชตแลว้ดขีึน้
1เดอืน เริม่ปวดบรเิวณกน้กบปวดตือ้ๆ เป็นมากเวลานอนหงายและขยับตวั
วันนีไ้มด่ขี ึน้ยงัมไีข ้และปวดกน้กบมากขึน้ และน ้าหนักลด 5กโิลกรัม (56->51)
-No Hx contact TB
-ไมไ่ดเ้ลีย้งสตัว์
Physical examination
• T 38.5 c, BP 140/86 mmHg, HR 100/min, RR 16/min
• GA: Good consciousness, no pale, no jaundice, no dyspnea & tachypnea
• HEENT: no thyroid gland enlargement
• CVS & RS: unremarkable
• Abdomen: soft, no distension, no tenderness, no hepatosplenomegaly, no ascites, normal bowel sound
• Tender at LS area
• Nervous system: no neurological deficit

CASE2: หญิงอาย ุ68ปี อาชีพท านา ภูมิล าเนานครราชสีมา
Investigation
• CBC: Hct30 WBC5700 Plt331000
• BUN/Cr LFT:normal
• ESR100
Problem list
• –> Prolonged fever with inflammatory back pain for 2 months
• Spondylodiscis• Etiology – TB/NTM, Pyogenic,
Brucellosis
• Investigation • MRI spine
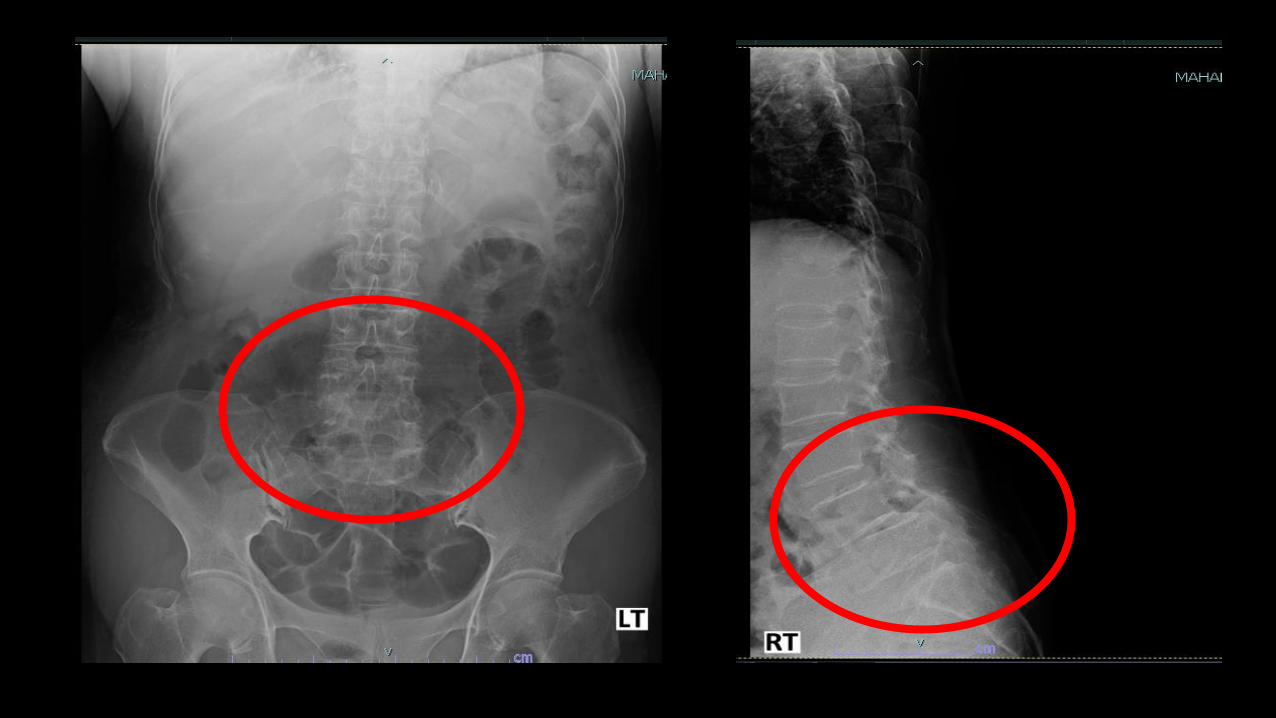


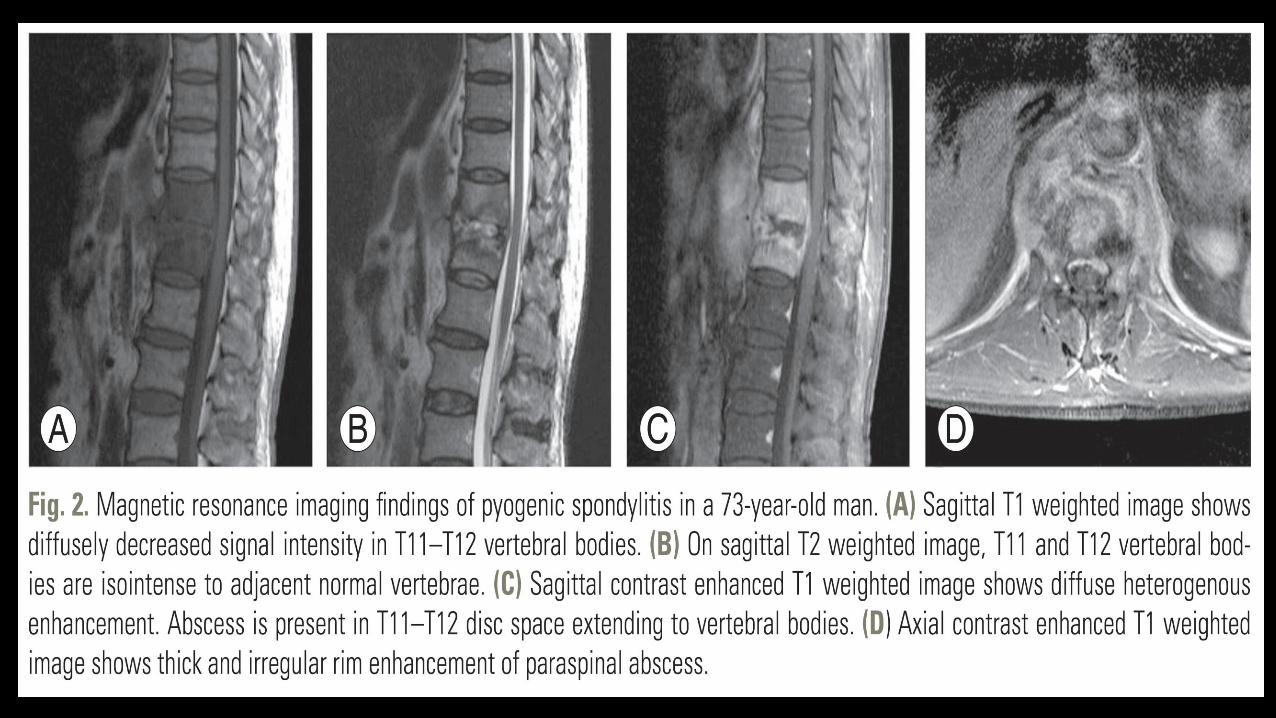
MRI finding: spondylodiscitis
1. Decrease signal intensity from disc and adjacent vertebral body on T1-weight image and loss of vertebral endplate
2. Increase signal intensity on T2-weight images ( due to edema)
3. Gadolinium enhancement of disc, vertebrae and surrounding soft tissue
Sign on MRI Sensitivity
1. Inflammation of soft tissue ( high T2
signal intensitiy and contrast uptake )98%
2. Disc enhancement ( contrast uptake ) 95%
3. High T2 signal intensity from the disc
or fluid-like signal93%
4. Loss of intradiscal space 84%
1+2, 2+3, 3+4, 1+3 หรอื 1+ destruction
of the vertebral endplates100%

Variable Pyogenic Tuberculous Brucellar
Commonly involved region Lumbar spine Thoracic spine Lumbosacral spine
Involvement of vertebral bodies
Involvement ≤2 vertebral bodies
Multiple body involvement or Skip lesion
Involvement ≤2 vertebral bodies
Degree of disc preservation Moderate to complete disc destruction
Normal to mild disc destruction (Late)
Moderate to complete disc destruction
Endplate destruction Anterior Anterior and posterior Anterior and superior“ Parrot-beak osteophyte”
Bony destruction more than half
Infrequent and mild to moderate
Frequent and more severe Infrequent and mild to moderate
Vertebral body enhancement pattern
Homogeneous Heterogeneous and focal Homogeneous
Epidural abscess Presence Presence , More common Presence
Paraspinal abscess and abscess wall
<2cm, Thick and irregular >2cm, Thin and smooth <2cm, Thick and irregular
Postcontrast paraspinalabnormal signal margin
Ill-defined Well defined Ill-defined
Abscess with postcontrastrim enhancement
Disc abscess Vertebral intraosseousabscess
Disc abscess

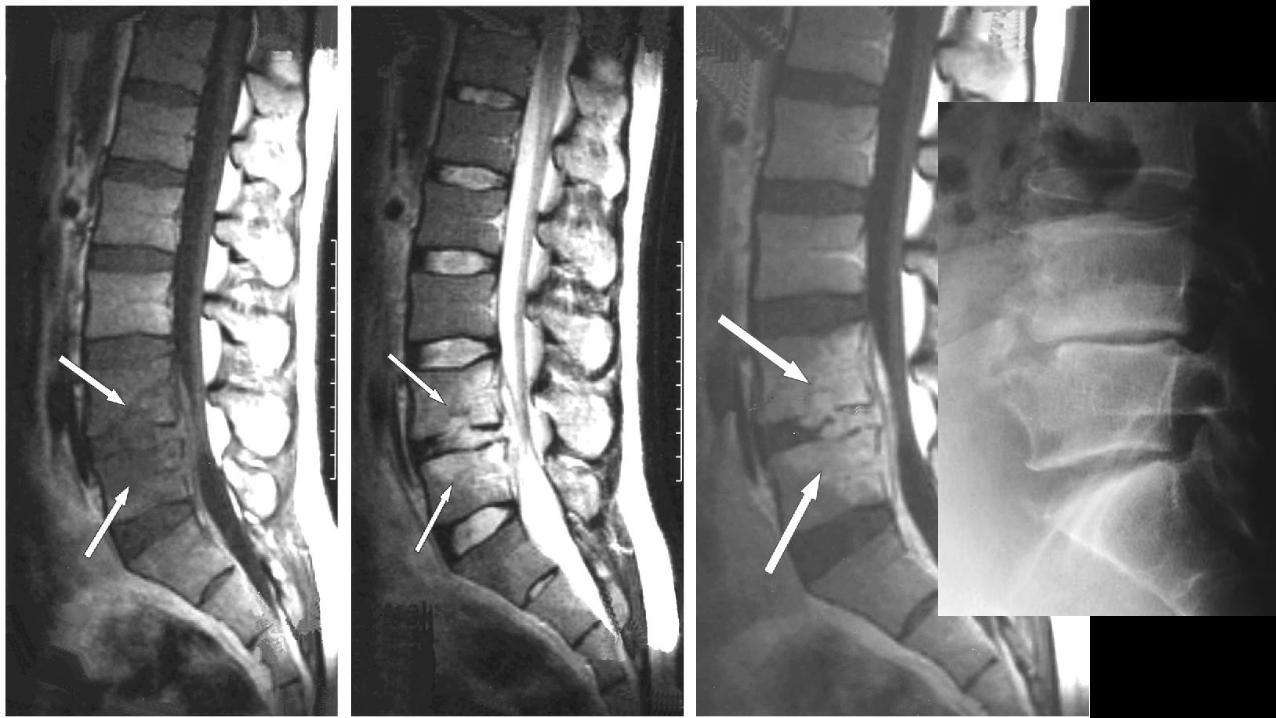


Dx: Brucellosis
• H/C : Brucella melitensis x II specimen
• Rx :
Non localized Doxycycline (6wks) + Gentamicin (7D)Doxycycline (6wks) + Rifampin (6wks)
Osteoarticular Doxycycline (3mo) + Gentamicin (7D) or Ciprofloxacin (3mo) + Rifampin (3mo)
Neurobrucellosis Doxycycline + Rifampin + CeftriaxoneUntil CSF become normal
Pregnant Woman TMP/SMX + Rifampin
B. melitensis -> GoatB. abortus -> CattleB. canis -> DogB. suis -> Pig
Diagnosis• Culture: Blood, BM• Non Culture- PCR- Serology
- Rose Bengal- Serum agglutination test (titer >1:160)- ELISA

CASE3: ชายไทยคู ่อาย ุ54ปี อาชพีขบัรถรับจา้ง ภมูลิ าเนาจ.นครราชสมีา
• CC: ไข ้1 เดอืน
• 1 เดอืนมไีขต้ า่ๆ ตลอดทัง้วนั กนิยาลดไขแ้ลว้อาการดขี ึน้ กนิไดล้ดลงอิม่เร็วขึน้ รูส้กึแน่นทอ้งหลังกนิอาหาร ไมม่คีลืน่ไส/้อาเจยีน ถา่ยอจุจาระปกต ิไมเ่คยเขา้ป่า/ลยุน ้า ไมไ่ดท้อ่งเทีย่งตา่งจังหวดั ไมเ่คยมปีระวตัคินในครอบครัว/คนใกลต้ัวเป็นวณัโรค
• 1 สปัดาหป์วดทอ้งดา้นขวาบน ไมม่รีา้วไปต าแหน่งอืน่ รว่มกับไขเ้ริม่สงูขึน้หนาวสัน่ จงึมาโรงพยาบาล
• Past Hx: Beta thalassemia, DM type2 (HbA1C 9)
• Personal Hx: กนิเหลา้ขาว 1-2 แบน/วนั สบูบหุรี ่20 pack-year

CASE3: ชายไทยคู ่อาย ุ54ปี อาชพีขบัรถรับจา้ง ภมูลิ าเนาจ.นครราชสมีา
• PE V/S BP 120/70 mmHg PR 80/min RR15 T 37.8˚c
• Thai man, good consciousness, pale, no jaundice
• HEENT: no pale conjunctivae, anicteric sclerae
• Heart : no murmur
• Lung : clear, no adventitious sound
• Abdomen : soft, mild tender at RUQ, no guarding, no rebound tenderness, liver 3 FB BRCM, liver span 12 cm, splenic dullness – positive, Fist test -positive
• Ext : no rash, no petechiae or ecchymosis, no pitting edema

Case3: ชายไทยคู ่อาย ุ54ปี อาชพีขบัรถรับจา้ง ภมูลิ าเนาจ.นครราชสมีา
Problem list
• Prolonged fever with RUQ pain with Hepatosplenomegaly and tender
• DM type2
• Beta Thalassemia
Investigation
• CBC: Hb 8.1 g/dL, Hct 24.5%, WBC 13,300 /mm
3 (N 83.1%, L
7.4%,band9.5%) Platelet 145,000 /mm
3
• BUN 20 mg/dL, Cr 1.1 mg/dL, Na 133, K 3.5, Cl 97, HCO3 22 mmol/L
• LFT: Alb 2.8, Glob 3.9 g/dl, TB 0.46, DB 0.27 mg/dL, AST 58, ALT 130, ALP210 U/L


Signs and symptoms of liver abscess
Clinical practice in gastroenterology. 2555; 278
Amoebic Pyogenic Melioidosis
Symptoms
- Fever 51-48 42-86 100
- Abdominal pain 86-100 52-58 44
- RUQ pain 47-60 45-48 24
- Dysentery 10-42 0-11 -
Signs
- Hepatomegaly 62-87 52-85 76
- Abdominal tenderness 33-77 35-62 47
- Jaundice 14-27 21-48 26
- Ascitis 9 10 -
- Peritonitis 11 10 -

Sonographic appearance of liver abscesses
Amoebic Pyogenic Melioidosis
Number
- Single 71-96 52-80 18
- Multiple 4-29 20-48 82
Site
- Right lobe 86-96 50-63 74
- Left lobe 4-9 8-31 6
- Both lobes 2-9 6-41 26
Characteristic
Hypoechoic round or oval, no septum
Hypo-,or isoechoic, multiloculated or
multiseptated
Multiloculated or multiseptated, cart-wheel or
swiss-cheese
Spleenic abscess - 6 56Clinical practice in gastroenterology. 2555; 278

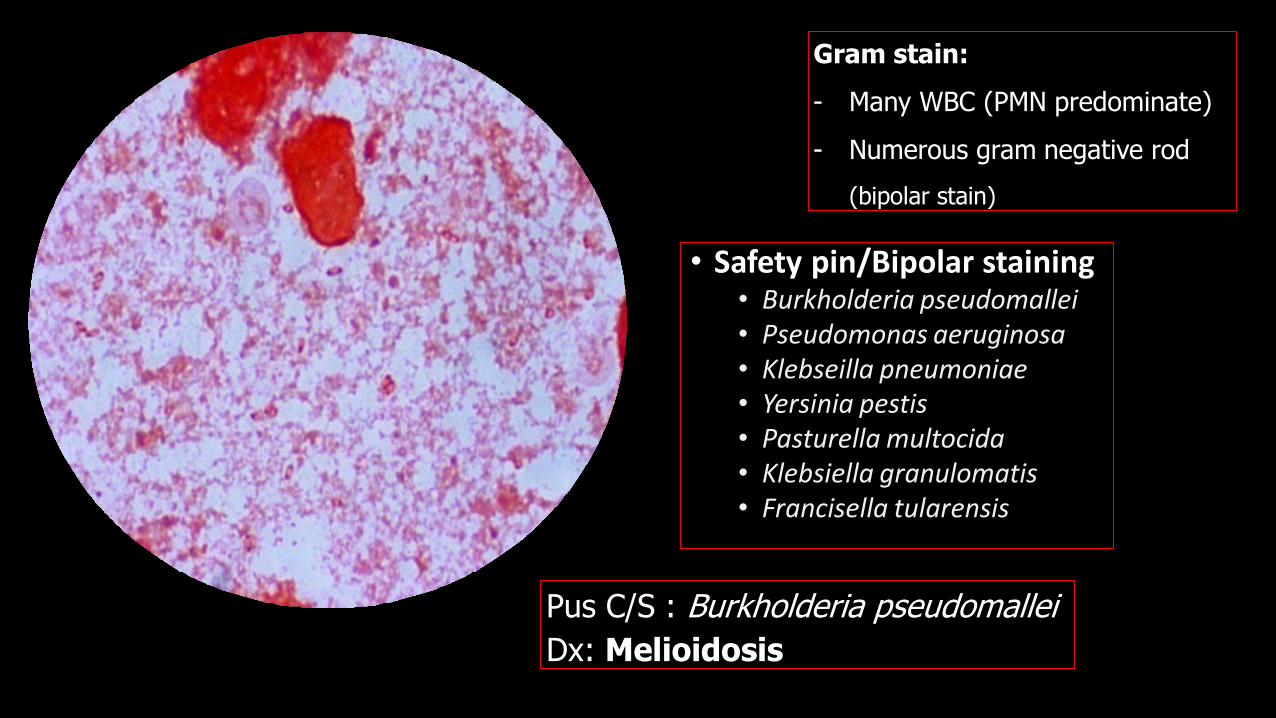
Gram stain:
- Many WBC (PMN predominate)
- Numerous gram negative rod
(bipolar stain)
Pus C/S : Burkholderia pseudomallei
Dx: Melioidosis
• Safety pin/Bipolar staining• Burkholderia pseudomallei• Pseudomonas aeruginosa• Klebseilla pneumoniae• Yersinia pestis• Pasturella multocida• Klebsiella granulomatis• Francisella tularensis

Melioidosis
• Gram-negative bacteria
• Burkholderia pseudomallei
• Mean incubation period 3-7
days in acute infection & 2-3
weeks to months or years in
chronic infection
Risk factor OR (95% CI )
Thalassemic disease 10.2 (3.5-30.8)
DM 5.9 (4.0-8.9)
Preexisting Renal disease 2.9(1.7-2.5)
DM with high soil & water exposure
8.5(5.5-13.1)
DM with Moderate soil & water exposure
5.6(1.7-18.6)
High soil & water exposure 3.3(1.8-6.3)
Moderate soil & water exposure
2.1(0.8-5.6)
Excessive alcohol consumption
Less prevalence in Thailand
Suputtamongkoletal B, et al, Risk factor for melioidosis. CID 1999;29.
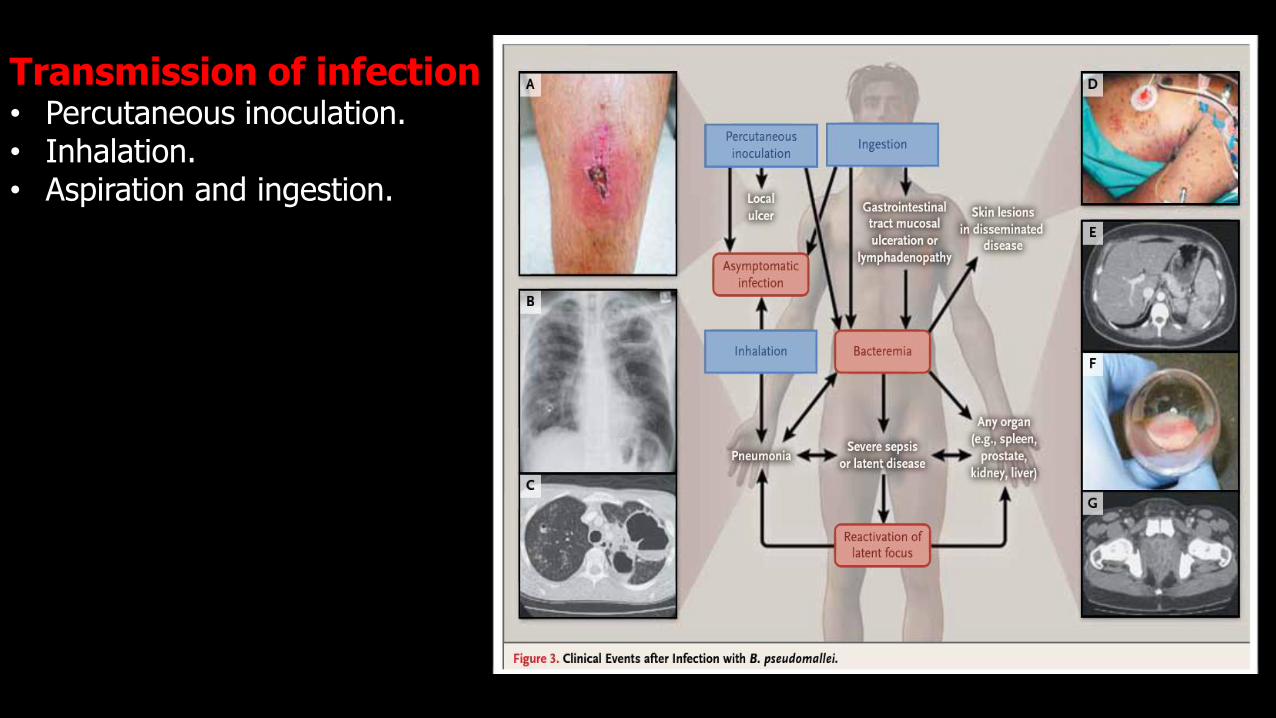
W. Joost Wiersinga, Melioidosis, NEJM,2012, 367;11
Transmission of infection• Percutaneous inoculation.• Inhalation.• Aspiration and ingestion.

Visceral organ involvement in melioidosis
Organs PatientsOne organ 57 (71%)
- Spleen 37
- Liver 16
- Kidney 4
Multi-organ 23 (29%)
- Liver and spleen 17
- Liver, spleen and kidney 3
- Spleen and kidney 2
- Liver and kidney 1
Wibulpolprasert B, et al, Visceral organ abscesses in melioidosis. J clin Ultrasound 1999; 29-34.
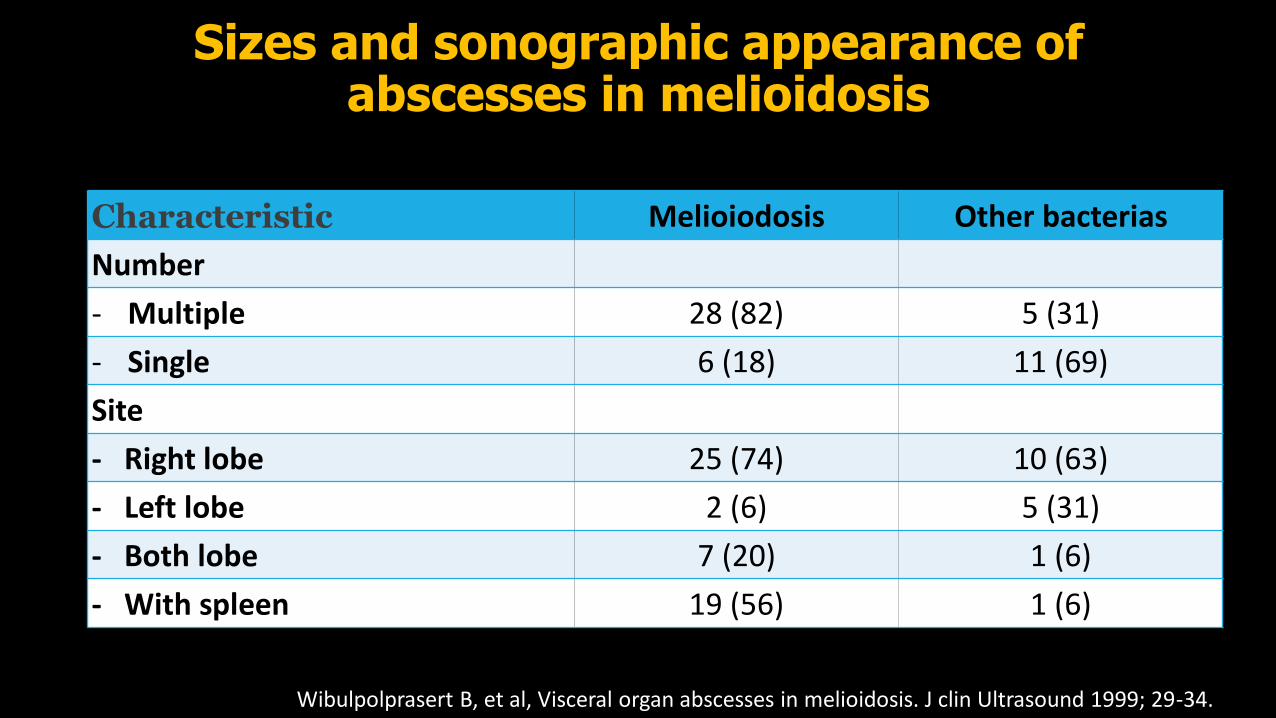
Sizes and sonographic appearance of abscesses in melioidosis
Wibulpolprasert B, et al, Visceral organ abscesses in melioidosis. J clin Ultrasound 1999; 29-34.
Characteristic Melioiodosis Other bacterias
Number
- Multiple 28 (82) 5 (31)
- Single 6 (18) 11 (69)
Site
- Right lobe 25 (74) 10 (63)
- Left lobe 2 (6) 5 (31)
- Both lobe 7 (20) 1 (6)
- With spleen 19 (56) 1 (6)

Sizes and sonographic appearance of abscesses in melioidosis
Wibulpolprasert B, et al, Visceral organ abscesses in melioidosis. J clin Ultrasound 1999; 29-34.
Site and size Appearance of lesion ( No. Patients)
Cystic Target-like Bull's eye Multiloculated
Splenic abscess
< 2cm. ( 54 Pts.) 1 37 3 15
>=2cm. ( 13 Pts.) 2 3 3 6
Liver abscess
<2cm. (21 Pts.) 0 13 4 5
>=2cm. (23 pts.) 0 0 1 21

Chest x-ray characteristic
Acute with bacteremian=55 (%)
Acute without bacteremian=50 (%)
Subacute/chronic bacteremian=31 (%)
Subacute/chronic
n=47 (%)
Infiltrations
Nodular 46 (84) 11 (22) 17 (55) 13 (28)
Alveolar 4 (7) 26 (52) 4 (13) 8 (17)
Mixed 2 (3.5) 9 (18) 8 (26) 23 (49)
Miscellaneous 3 (3.5) 4 (8) 2(6) 3 (6)
Distribution
One lobe 9 (17) 19 (38) 9 (29) 17 (36)
Multiple lobe 44 (80 ) 31 (62) 22 (71) 30(64)
Apical lesion 5 (9) 6 (12) 6 (19) 10 (21)

Treatment of melioidosisAntimicrobial drug Dose
Initial intensive therapy (at least 14 days)
Ceftazidime (120mg/kg/day) 2 gm iv q 8hr
Imipenem (50mg/kg/day) 1 gm iv q 8hr
Meropenem (75mg/kg/day) 1 gm iv q 8 hr
Amoxy/clav (160mg/kg/day of amoxy) 2.4 gm iv loading then 1.2gm iv q 4hr
Cefoperazone/sulbactam + Co-trimoxazone 25mg/kg/day(cefoperazone)+ 8mg/kg/day (TMP)
Eradication therapy (20 wks)
Co-trimoxazole (80TMP/400SMX)
BW > 60 kg 4tab oral q 12hr
BW 40-60 kg 3tab oral q 12hr
BW < 40 kg 2tab oral q 12hr
Co-trimoxazole+doxycycline : relapse 4% Add doxycycline(100) 1 tab oral q 12hr
Amoxy/clav : relapse 16% ( recommend in pregnancy) 60mg/kg/day(amoxy) + 15mg/kg/day(clavulanic)
Ciprofloxacin+azithromycin : relapse 22% Ciprofloxacin 500mg bid + azithromycin 500 mg oral od

Melioidosis
• Recurrent melioidosis
▪ 6% in the first year and 13% during 10 years
▪ Recurrent melioidosis
o 75% -> relapse (same strain)
o 25% -> re-infection (different strain)
▪ Risk factors
oMaintenance with ATB other than TMP/SMX
o Treatment duration < 8 weeks
o Bacteremia or disseminated infection form

klebsiella syndrome
• Klebsiella pneumoniae (K1 and K2 serotypes)
• Host factor : Diabetes mellitus (70-78 %)
• Clinical manifestations• Fever (93 %)• Right upper quadrant tenderness (71 %)• Nausea, vomiting, diarrhea, or abdominal
pain (38 %)• Leukocytosis (70 %)• Elevations in serum alanine and aspartate
aminotransferases (59 and 68 %)• Elevations in alkaline phosphatase (78 %)• Elevations in bilirubin (26 %)
Wang JH, et al. Primary liver abscess due to Klebsiella pneumoniae in Taiwan. Clinical Infectious Diseases. 1998 Jun 1;26(6):1434-8.Choby JE, et al. Hypervirulent Klebsiella pneumoniae–clinical and molecular perspectives. Journal of internal medicine. 2020 Mar;287(3):283-300.

CASE4: หญงิไทยคู ่อาย ุ74ปี ไมไ่ดป้ระกอบอาชพี ภมูลิ าเนา จ.นครราชสมีา
CC: เหนือ่ยมากขึน้ 1วนั• 1เดอืนกอ่น รูส้กึมไีขต้ า่ๆ เป็นตลอดทัง้วัน รว่มกบัมอีาการไอแหง้ๆ เล็กนอ้ย ไมม่อีาการผดิปกติ
• 2สปัดาหก์อ่น ยังมไีขต้ลอด ไอเริม่มเีสมหะ ไปตรวจที ่รพช แพทย์ใหน้อนโรงพยาบาลไดย้าเป็น Ceftriaxone และ Azithromycin
• 1วัน ขณะทีย่ังนอนโรงพยาบาล มไีขส้งูขึน้และหอบเหนือ่ยมากขึน้ จงึreferมา
• ไมม่โีรคประจ าตวั

CASE4: หญงิไทยคู ่อาย ุ74ปี ไมไ่ดป้ระกอบอาชพี ภมูลิ าเนา จ.นครราชสมีา• Vital sign : BP 95/60 mmHg PR 75 bpm BT 38.5 RR
• GA: A Thai middle-aged woman ,Alert
• HEENT: not conjuctivae, anicteric sclerae, LN can’t palpable
• Heart: apex at 5th ICS , impalpable apex , JVP not
• engorge, no heaving, no thrill, normal s1 s2, no Murmur
• Lung: trachea in midline normal breath sound, equally both lung , secretion sound both lung, Fine crepitation both lung, mass at right chest wall 2x3 cm with tender, redness , fluctuation
• Abdomen: normal distension, no superficial vein dilatation, normoactivebowel sound, soft , not tender , fluid thrill negative, liver span 10 cm
• Extremites: no pitting edema, no petechiae , no ecchymosis
• Neuro: grossly intact

CASE4: หญงิไทยคู ่อาย ุ74ปี ไมไ่ดป้ระกอบอาชพี ภมูลิ าเนา จ.นครราชสมีา
Problem list
• Progressive dyspnea for 3 day
• Mass at chest wall
• Hx of pneumonia
• Hx of breast mass

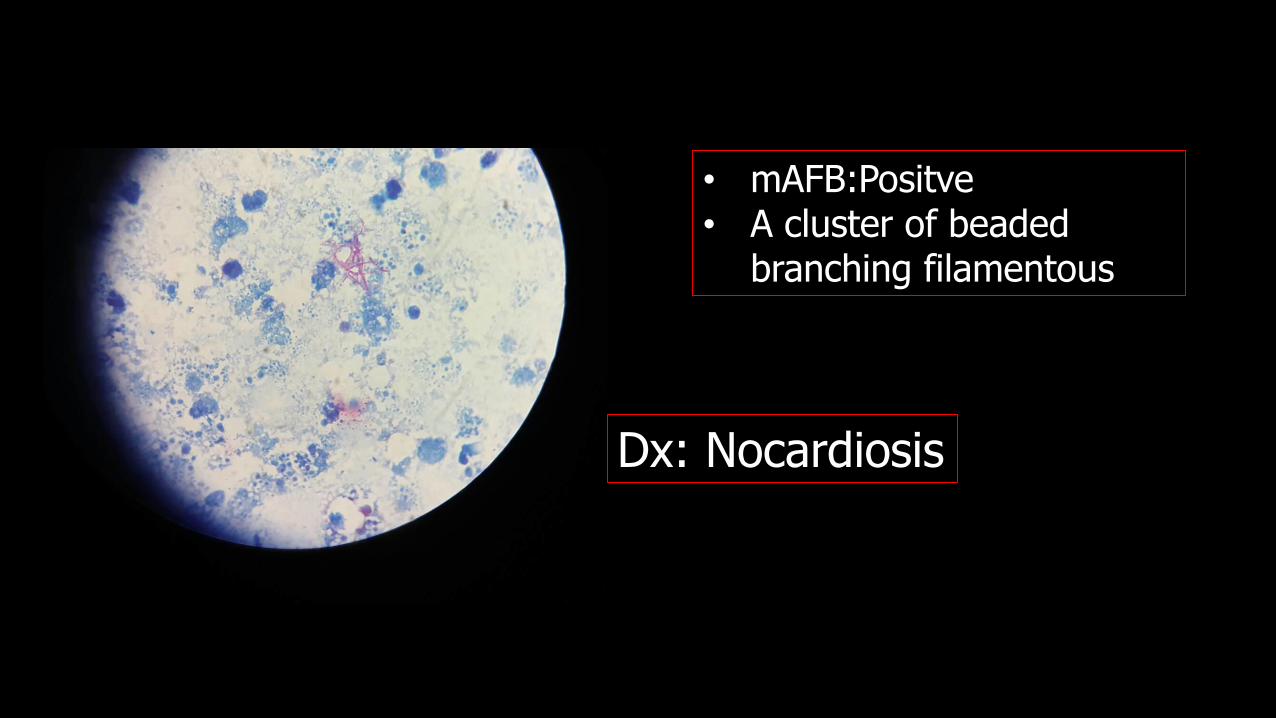
• mAFB:Positve• A cluster of beaded
branching filamentous
Dx: Nocardiosis

Nocardiosis
• Nocardia spp.
Clinical presentation
• Pulmonary nocardiosis
• Lymphocutaneous
• Disseminated nocardiosis
Risk factorUsually Immunosuppressive condition
• HIV (esp. CD4 < 100 cell/mm3)
• Solid organ/hematopoietic stem cell transplant
• Glucocorticoid / CMT therapy
• Chronic lung disease
• DM
Up to 1/3 of patient are immunocompetent


Non-severe infection
Isolated cutaneous infection TMP-SMX OR Minocycline (alternative regimen)
Non-severe mycetoma TMP-SMX +/- Dapsone
Mild or moderate pulmonary disease in immunocompetent hosts
TMP-SMX
Mild or moderate pulmonary disease in immunocompromised hosts
TMP-SMX
Severe infection
Severe mycetoma Imipenem +/- Amikacin
Severe pulmonary or disseminated disease (without CNS involvement)
TMP-SMX PLUS Amikacin (first-line regimen)ORImipenem PLUS Amikacin (alternative regimen)
Involvement of ≥2 sites in immunocompromisedhosts (without CNS involvement)
TMP-SMX PLUS Amikacin (first-line regimen)ORImipenem PLUS Amikacin (alternative regimen)
Isolated CNS disease TMP-SMX PLUS Imipenem
CNS disease with multiorgan involvement (ie, at least one other site)
TMP-SMX PLUS Imipenem PLUS Amikacin
Life-threatening disease TMP-SMX PLUS Imipenem PLUS Amikacin

Rx: Nocardiosis
Switch to oral therapy• Start after induction phase (usually 3rd -6th week)
• Based upon a susceptibility result
CNS not involvement
• Monotherapy
CNS involvement/multi-organ involvement/ immunocompromised
• 2 drug regimen(based upon susceptibility)
• TMX-SMX(10mg/kg/day)
• Minocycline (100mg twice daily)
• Amoxicillin-clavulanate (875 mg twice daily)
Duration
Immunocompetent
• Isolated cutaneous infection : 3-6 month
• Pulmonary involvement : 6-12 month
• CNS involvement : at least 1 year
Immunocompromised
• Isolated cutaneous infection : 6-12 month
• Other :at least 1 year

CASE5: หญงิไทยคู ่อาย ุ70ปี ไมไ่ดป้ระกอบอาชพี ภมูลิ าเนา จ.นครราชสมีา
• CC: ไข ้4 เดือนก่อนมารพ.• 4เดือนก่อน ไขต้ ่าๆ โดยเฉพาะช่วงค ่า ไมม่ีอาการผิดปกติอยา่งอื่น• 3เดือนก่อน ไขย้งัคงมีอยูต่ลอด ไปรกัษาคลนิิก ไดย้ามาทาน แตไ่มด่ีขึน้• 2เดือนยงัคงมีไข ้ไปตรวจที่รพช ไดน้อน รพ. ใหย้าฆา่เช่ือ นอนนาน1เดือน มีไขท้กุวนั อาการเทา่ๆเดิม จึงขอแพทยก์ลบับา้น
• วนันีไ้ขย้งัมีเหมือนๆเดิม แตรู่ส้กึเหน่ือยเพลยี น า้หนกัลด 58->45Kg/4เดือน จึงมารพ.
• No. U/D• ไมไ่ดเ้ลีย้งสตัว์

• Vital sign : BP 120/70 mmHg PR 90 bpm BT 38.5 RR
• GA: A Thai woman ,Alert
• HEENT: mild pale conjuctivae, anicteric sclerae, LN can’t palpable
• Heart: apex at 5th ICS , impalpable apex , JVP not
• engorge, no heaving, no thrill, normal s1 s2, no Murmur
• Lung: trachea in midline normal breath sound, equally both lung , secretion sound both lung, Fine crepitation both lung
• Abdomen: normal distension, no superficial vein dilatation, normoactivebowel sound, soft , not tender , fluid thrill negative, liver span 10 cm
• Extremites: no pitting edema, no petechiae , no ecchymosis
• Neuro: grossly intact
CASE5: หญงิไทยคู ่อาย ุ70ปี ไมไ่ดป้ระกอบอาชพี ภมูลิ าเนา จ.นครราชสมีา

• CBC: Hb9.6 g/dL, Hct29.2%, MCV 82 fL, WBC 4,780/mm3(N 75.4%, L 14.3%, M 7.2%, Eo2.8%, B 0.3%), plt424,000/mm3, MCV77, RDW17.5
• Blood chemistry : BUN 12.1mg/dL, Cr 1.0mg/dL,Na 137 mmol/L, K 2.9 mmol/L, Cl95 mmol/L, HCO328 mmol/L
• LFT: TB 0.3 mg/dL, DB 0.16 mg/dL, AST 118 U/L, ALT 12 U/L, ALP 112U/L, Albumin 3.1 g/dL, Globulin 5.4 g/dL
• TIBC 258, Serum iron 13
CASE5: หญงิไทยคู ่อาย ุ70ปี ไมไ่ดป้ระกอบอาชพี ภมูลิ าเนา จ.นครราชสมีา
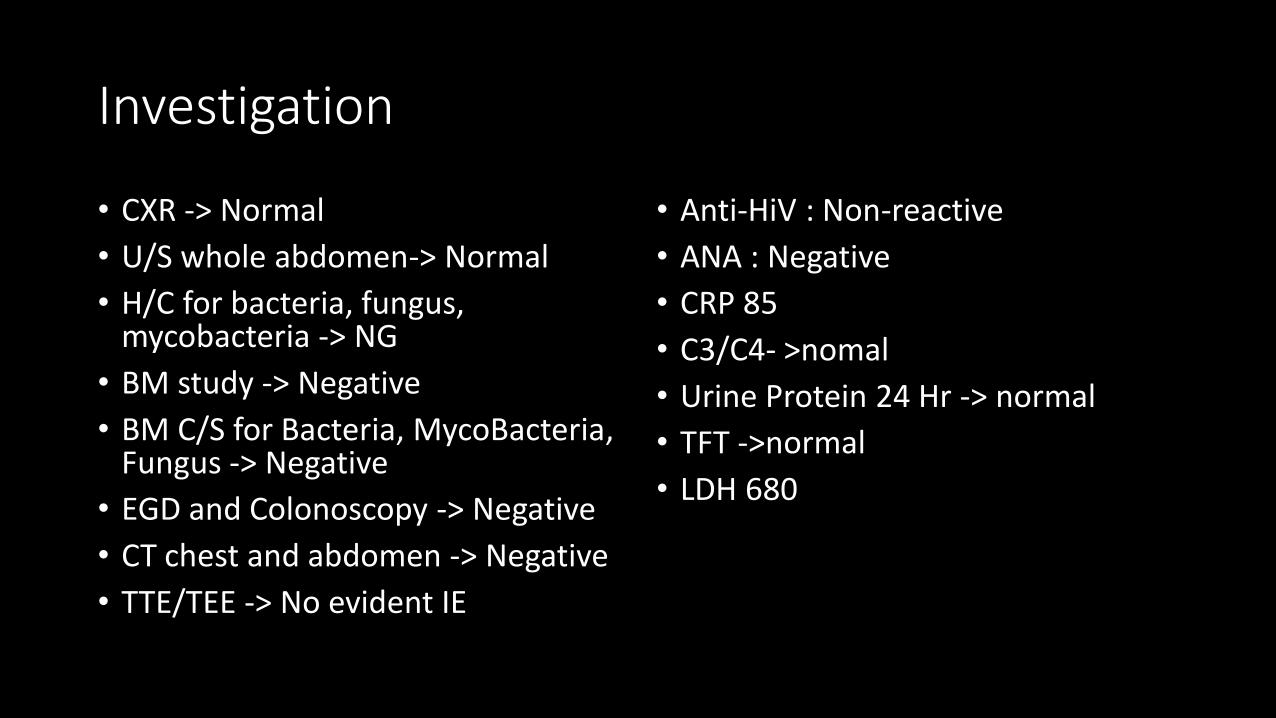
Investigation
• CXR -> Normal
• U/S whole abdomen-> Normal
• H/C for bacteria, fungus, mycobacteria -> NG
• BM study -> Negative
• BM C/S for Bacteria, MycoBacteria, Fungus -> Negative
• EGD and Colonoscopy -> Negative
• CT chest and abdomen -> Negative
• TTE/TEE -> No evident IE
• Anti-HiV : Non-reactive
• ANA : Negative
• CRP 85
• C3/C4- >nomal
• Urine Protein 24 Hr -> normal
• TFT ->normal
• LDH 680


Dx : Intravascular lymphoma
Clinical Presentation• Constitutional B symptoms
• Central nervous system (27 to 76 percent)
• Skin (15 to 39 percent)
• Laboratory studies• Elevated ESR, CRP, LDH
• Anemia
• Altered hepatic, renal, or thyroid function
•Diagnosis : Pathology

Case: ชาย 20ปี อาชีพนกัศึกษา จ.นครราชสีมา
• CC: ไข ้3สปัดาห์
• 3 สปัดาห ์ก่อนมารพ. ไขต้ ่าๆ ไมไ่อ ไมเ่หน่ือย ไมป่วดทอ้ง ถ่ายปกติ ไมม่ีปัสสาวะแสบขดั • 1 สปัดาห ์ก่อนมารพ. ไขส้งู เหน่ือยเวลาออกแรง นอนราบได ้ไมม่ีตื่นมาหอบเหน่ือย กลางคืน ไมบ่วม ไม ่ไอ ปัสสาวะอจุจาระปกติ
• Past history • ไมมี่โรคประจ าตวั• สบูบหุรี6่-10 มว้นตอ่วนั ดื่มสรุา 2-3 ครัง้ตอ่วนั • ไมมี่ประวตัิ ฉีดยาเสพติดเขา้เสน้• เลีย้งสนุขั และ แมว

Case: ชาย 20ปี อาชีพนกัศึกษา จ.นครราชสีมา
• Physical examination
• V/S: BT 38.9o C, RR 22/min, BP 110/70 mmHg, PR 120/min
• GA: A young Thai man, good consciousness
• HEENT: not pale conjunctivae, anicteric sclera, Multiple dental caries
• LN: can’t be palpated
• Heart: regualar, normal S1,S2, PSM at apex gr 3 radiate to axillary
• Lung: equal breath sound, no adventitious sound
• Abd: soft, not tender
• Ext: no edema, no Osler’s node, no Janeway’s lesion, no splinter hemorrhage

Case: ชาย 20ปี อาชีพนกัศึกษา จ.นครราชสีมา
Problem list
• Prolonged fever 3wks
• Progressive dyspnea 1 wks
• Mitral valve regurgitation
• Dental carries
Investigation for diagnosis
• Hemoculture ¾ bottles
• CXR
• EKG12lead
• Echo

Hemoculture: Streptococcus oralis * 3 bottle
Infective endocarditis
• Modified duke criteria (ESC 2016)
▪ Definite IE
o2 major
o1 major + 3 minor
o5 minor

Modified duke criteria (ESC 2016): major criteria
1. Positive hemoculture 2. Imaging
▪ Typical organisms*
- 2 bottles
▪ Echo: vegetation, abscess,
aneurysm, pseudoaneurysm,
fistula, perforation
▪ Organisms consistent with IE- 2 bottles (12 hr apart)- 3/3 or 3/4 bottles (first and last 1 hr apart)
▪ Cardiac CT: paravalvular lesions
▪ C. burnetti- 1 bottle or phase 1 IgG > 1:800
▪ 18 F-FDG PET/CT (Prosthesis
> 3m) or radiolabeled
leukocytes SPECT/CT
* Typical organisms: S. aureus, Viridans streptococci, Gr D Streptococci, HACEK
Community acquired Enterococci without primary foci

Modified duke criteria (ESC 2016): minor criteria
Criteria
1. Predisposing heart disease or IVDU
2. Fever >38.0 C
3. Vascular phenomenon (New: require imaging forconfirmation)
4. Immunologic phenomenon
5. Positive culture (not compatible with major criteria)

Vascular VS Immunologic phenomenon
Vascular phenomenon
• Major arterial emboli
▪ Septic pulmonary infarcts
▪ Mycotic aneurysm
▪ Intracranial hemorrhage
▪ Conjunctival hemorrhage
▪ Janeway’s lesion
Immunologic phenomenon
▪ Glomerulonephritis
▪ Osler’s node
▪ Roth’s spot
▪ Rheumatoid factor

Osler’s node Janway’s lesion
Splinter hemorrhage Roth’s spot

History/Exposure Possible disease
IVDU S. aureus
Dental caries Streptococcus Viridans Group
Hepatobiliary / colon Gr D Streptococcus
Inhalation/Ingestion/Contact with Goat, Sheep, Cattle, Cat
C. Burnetti
Contact with Goat, Sheep, CattleIngestion daily products
Brucellosis
Contact to swine, fish Erysipelothrix rhusiopathiae
Contact to cat, mammals Bartonella spp
Abdominal Surgery Fungus Esp. candida

Empirical ATB
ESC 2016
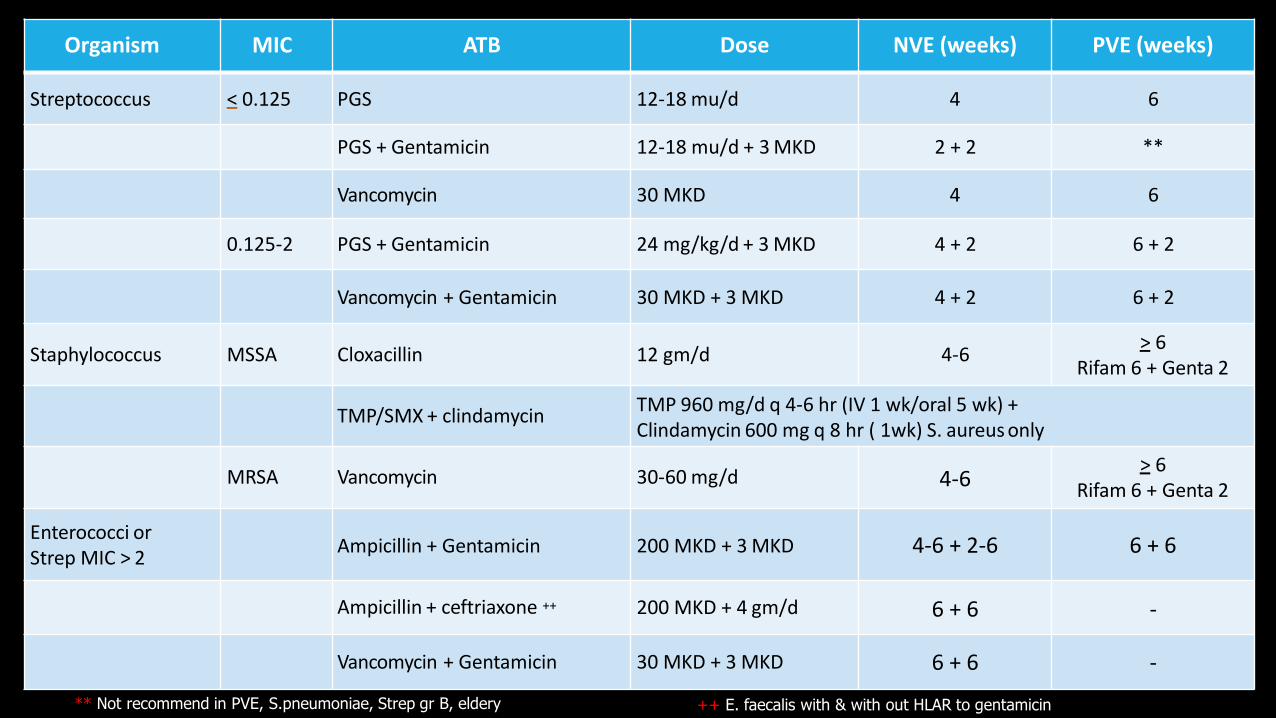
Organism MIC ATB Dose NVE (weeks) PVE (weeks)
Streptococcus < 0.125 PGS 12-18 mu/d 4 6
PGS + Gentamicin 12-18 mu/d + 3 MKD 2 + 2 **
Vancomycin 30 MKD 4 6
0.125-2 PGS + Gentamicin 24 mg/kg/d + 3 MKD 4 + 2 6 + 2
Vancomycin + Gentamicin 30 MKD + 3 MKD 4 + 2 6 + 2
Staphylococcus MSSA Cloxacillin 12 gm/d 4-6> 6
Rifam 6 + Genta 2
TMP/SMX + clindamycinTMP 960 mg/d q 4-6 hr (IV 1 wk/oral 5 wk) + Clindamycin 600 mg q 8 hr ( 1wk) S. aureus only
MRSA Vancomycin 30-60 mg/d 4-6> 6
Rifam 6 + Genta 2
Enterococci or Strep MIC > 2
Ampicillin + Gentamicin 200 MKD + 3 MKD 4-6 + 2-6 6 + 6
Ampicillin + ceftriaxone ++ 200 MKD + 4 gm/d 6 + 6 -
Vancomycin + Gentamicin 30 MKD + 3 MKD 6 + 6 -
** Not recommend in PVE, S.pneumoniae, Strep gr B, eldery ++ E. faecalis with & with out HLAR to gentamicin


No Localizing sign & symptoms
Prolonged FeverLocalizing symptoms▪ CNS ▪ GI ▪ CVS ▪ GU ▪ Skin ▪ LN▪ Respiratory ▪ Bone & joint ▪ Hemato
Laboratory▪ CBC ▪ LFT ▪ Bun/Cr ▪ UA ▪ Hemoculture▪ ESR/CRP
Review history ▪ Occupation/recreation ▪ Habitat ▪ Travel ▪ Animal contact ▪ Contact with ill person ▪ Medications
No diagnosis ! FUO

Fever of unknown origin
Infection Tumor Miscellaneous
▪ CT chest
▪ CT Abdomen▪ Anti-HIV▪ PPD
▪ Occult abscess▪ Occult TB▪ Culture negative IE▪ HIV
▪ CT abdomen
▪ CT chest▪ Bone marrow Bx
▪ RE tumor: lymphoma, leukemia▪ Renal cell CA▪ Hepatic cancer▪ Hepatic metastasis
▪ TFT▪ ANA, RF, ESR▪ Venous doppler
▪ Drug fever▪ Temporal arteritis▪ Still’s syndrome▪ DVT/PE▪ Sarcoidosis▪ Vasculitis