Embed Size (px)
Citation preview

Case Analysis I- Lecture 9
Liana Al-Labadi, O.D.

If you hear hoof beats, think horses—not
zebras

CC: Dr. I see a black curtain over my
eyes

“Dr. I See All Black” Frequency: Constantly (all the time, everyday) @ D&N Onset: Suddenly10 days ago, but has noticed it more
over the past 2 days Location: Both eyes Duration: Lasts for a short time but I feel it’s there all
the time Associated Factors:
Blurry vision A lot of headaches
Relief: Headaches get better with parcetamol but I still see a
black curtain Severity:
The blacking out is pretty bad, I just can’t stand it anymore. The headaches are there all the time.

DIFFERENTIAL DIAGNOSIS????

“Dr. I See All Black” Migraine DES / Keratitis/ Blepharitis/ Iritis /AACG Vitreous detachment /Retinal break Angiospasm/ vasospasm Optic disc drusen/ Orbital tumor Papilledema ON / MS/ SLE Embolic/ Carotid emboli / Cardiac emboli IV drug use Hypoperfusion Coagulation disorders /Inflammatory arteritis Carotid stenosis /Ophthalmic artery stenosis Cardiac failure or arrhythmia Increased blood viscosity Intraocular hemorrhage Intracranial tumor Psychogenic

POH: (+) Near sightedness Negative for asthenopia, surgery, pain, & flashes Negative for AMD, DR, Cats & Glc (+) DIPL-?????? (+) Trauma- 14 years ago?????
LEE: 6 months ago (unknown doctor)- Status normal FOH: Negative for AMD, DR, Glc, Cat LPE: Does not remember PMH:
(+) stress (+) ENT (+) Respiratory Negative for HTN/DM/Cancer/Neuro
FMH: (+) HTN- Father; (+) DM- Parents; Migraines- Parents MED: None Allg: NKDA; No seasonal allergies SH: Reading Occupation: Student No alcohol consumption ; (+) smoking- Argeeleh
“Dr. I See All Black”

Entrance Testing: DVA (c):
OD: 20/50 PH: ??????????? OS: 20/30 PH: ???????????
Motility: S&F OD, OS Pupils: 4mm/4mm RRL OD, OS; No APD Confrontations:
OD: Slight inferior constriction OS: Full
“Dr. I See All Black”

Additional Tests: Lensometry:
OD: -3.75 -0.50x 153 OS: -3.75 -0.50x 153
Manifest Refraction: OD: -4.00 -0.50x 165 VA: “All black” OS: -3.75 -0.50x 153 VA: “All black”
“Dr. I See All Black”

SLE: L/L: trace MGD OD, OS Conj: No injection OD, OS K: Clear OD, OS Iris: Flat & brown OD, OS AC: No cell & no flare/ D&Q OD, OS Lens: Clear OD, OS
IOP (TA): ??????????
“Dr. I See All Black”

“Dr. I See All Black”

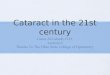
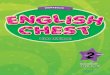
“Dr. I See All Black” DFE:
CDR: 0.15 round OD, OS NRR: 360˚ optic nerve swelling/elevation OD, OS
Blurry disc margins OD, OS Superior flame-shaped heme OD Inferior flame-shaped heme OS
Macula: Flat OD, OS Posterior Pole: Flat OD, OS Vessels:
Dilated & tortuous OD, OS Periphery: ????

“Dr. I See All Black” Differential Diagnosis:
Papilledema Retinal Vein Occlusion Optic Neuritis/Papillitis Ischemic Optic Neuropathy Compressive Optic Neuropathy Infiltrative Optic Neuropathy Systemic etiology:
Sarcoid Leukemia

“Dr. I See All Black” Assessment:
Bilateral optic never disc edema Unknown etiology Sx of TVO + Headaches + DIPL
Plan:Pt education on condition Refer for CT scanRefer patient for neurological work-upPt education on importance of follow-up with
neurology appointment

“Dr. I See All Black” F/U Visit:
Patient was told it was “benign” Began oral medications

“Dr. I See All Black” Assessment:
Bilateral Papilledema
Plan:RTC in 2 months for DFE + Visual Field

Papilledema-Definition Optic disc swelling produced by increased
intracranial pressure

Papilledema-Symptoms Symptoms:
Episodes of transient, often bilateral visual loss Lasting seconds
Symptoms precipitated after rising from a lying or sitting position (altering intracranial pressure)
Headache Double vision Nausea Vomiting Tinnitis Decrease in visual acuity (rare)
Mild decrease in VA can occur in an acute setting if there is macular disturbance
Visual field defects & severe loss of central vision Occur only with chronic papilledema

Papilledema-Signs Critical Signs:
Bilaterally swollen, hyperemic discs Early papilledema- disc swelling may be asymmetric
NFL edema causing blurring of the disc margin and often obscuring the blood vessels
Other Signs: Papillary pr peripapillary retinal hemorrhages Loss of venous pulsation
20% of the normal population do not have venous pulsation
Dilated, tortuous retinal veins Normal pupillary response Normal color vision Enlarged blind spot

Papilledema-Signs Signs of chronic papilledema:
Any hemorrhages or cotton-wool spots resolve Disc hyperemia disappears The disc becomes gray in color Narrowing of the peripapillary retinal vessels Optociliary shunt vessels may develop on the disc Loss of color vision, VA, VF defects (especially inferionasally)
may also occur

“Dr. I See All Black”

Papilledema Differential Diagnosis
Other Differential Diagnosis: Pseudopapilledema
Not true disc swelling Vessels overlying the disc are not obscured The disc is not hyperemic The surrounding NFL is normal Spontaneous venous pulsation is often present
Secondary to optic disc drusen or congenitally anomalous disc Hypertensive optic neuropathy
Optic nerve disc swelling caused by extremely high blood pressure
Narrowed arterioles A/V crossing changes Heme with or with out CWS in the peripheral retina and
posterior pole

Papilledema Differential Diagnosis Other Differential Diagnosis:
Orbital optic nerve tumors: Unilateral disc swelling May have proptosis
Amiodarone toxicity Patient present with acute visual loss and disc edema
Diabetic papillopathy: Benign disc edema in one or both eyes of a diabetic
patient Telagectasia of BVs and NV of the disc may occur
Thyroid-related optic neuropathy:

Papilledema Etiology Primary & metastatic intracranial tumora Hydrocephalus Pseudotumor cerebri (PTC) Subdural & epidural hematomas Subarachnoid hemorrhage
These patients have severe headaches Arteriovenous malformation Brain abscess- often produces high fever Meningitis
Fever, stiff neck, headache Encephalitis Cerebral venous sinus thrombosis

Papilledema Work-Up History & physical examination
Including blood pressure measurement Ocular examination
Pupils, color vision, DFE, VF Emergency MRI with MRV (magnetic
resonance venography) of the head CT scan may be done if MRI is not available
emergently Lumbar puncture with CSF analysis and
opening pressure measurement Done if MRI/MRV or CT scan results are normal

Papilledema Treament Treatment
Directed at the underlying cause of the increased intracranial pressure

Pseudotumor Cerebri (PTC) AKA Idiopathic Intracranial Hypertension (IIH) A syndrome in which patients present with
symptoms and signs of elevated intracranial pressure The nature of which may be idiopathic or due to
various causative factors Diagnosis of exclusion
Need to eliminate all other possible etiologies

Pseudotumor Cerebri (PTC) Symptoms:
Headaches Between 90% and 98% of patients with IIH present with
headache TVO
Transient episodes of visual loss- typically lasting seconds Percipitated by changes in posture
Double vision Tinnitis Nausea Vomitting Occurs predominantly in obese women of childbearing
age (20 to 44 years) “Fat 40 disease” Some studies suggest that excess weight in the abdominal
area causes a chain reaction from increased intra-abdominal pressure, eventually leading to increased intra-cranial venous pressure

Pseudotumor Cerebri (PTC) Critical Signs:
Papilledema due to increases intracranial pressure Bilateral papilledema is a hallmark sign of the disease
Negative MRI/MRV of the brain MRV added to evaluate the venous system of the brain and to
rule out a sinus thrombosis that is usually missed with an MRI. Without this information, the patient with a sinus thrombosis
could be misdiagnosed with the more benign PTC Increased opening pressure on lumbar puncture with
normal CSF composition Opening pressure exceeds 250mm of water
Other Signs: Unilateral or bilateral 6th nerve palsy with no other
neurological signs

Pseudotumor Cerebri (PTC) Differential Diagnosis:
Same as Papilledema- refer to previous slides

Pseudotumor Cerebri (PTC) Associated Factors:
Obesity “Fat 40” Significant weight gain Pregnancy Medications:
Oral contraceptives Tetracyclines Nalidixic acid Cyclosporine Vitmain A (>100,000 U/day) Systemic steroid withdrawl
http://www.revoptom.com/content/d/cornea/c/15325/

Pseudotumor Cerebri (PTC) Work-Up:
History: Specifically inquire about weight gain & medications
Ocular Exam: Pupils, EOMs, color vision & optic nerve evaluation Visual field test- very important for following up patients
Systemic Exam: Measure blood pressure & temperature Thorough blood work with CBC to R/O infectious
etiologies MRI/MRV of orbit and brain
Must be done immediately Need to R/O a space-occupying lesion
If normal refer for neuro-ophthalmic evaluation, including a lumbar puncture, to rule out other causes of papilledema & to determine the CSF opening pressure

Pseudotumor Cerebri (PTC) Treatment:
PTC may be a self-limited process. Treatment is indicated in the following situations:
Severe, intractable headaches Evidence of progressive decrease in visual acuity or visual
field loss Some ophthalmologists suggest treating all patients with
papilledema Method of treatment:
Wight loss- if overweight or recent increase in weight – 1st line tx
Acetazolomide (Diamox) Use with caution in sulfa-allergic patients Can decrease CSF production by 50%
Discontinuation of any causative medication If method of treatment unsuccessful
Consider systemic steroids Optic nerve sheathing surgery if reduced VA Neurosurgical shunt if headaches are a prominent symptom

Pseudotumor Cerebri (PTC)
Prognosis: Typically good if the underlying condition is
addressed promptly Follow-Up:
If acute: Monitor every 3 months in the absence of visual field loss
If chronic: Initially follow-up every 3-4 weeks to monitor visual
acuity and visual field loss then every 3 months
Patient education: Educate patients that papilledema can lead to optic
atrophy & irreversible vision damage if left untreated